1 Study Me plz
1/123
Earn XP
Description and Tags
RADT100, RADT1020
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
124 Terms
How many bones are in the human body?
206
What is the general rule for lead markers on where they should be placed?
Laterally or anteriorly
Name all of the bones in the wrist (SLTPTTCH)
Scaphoid Lunate Triquetrum Pisiform Trapezium Trapezoid Capitate Hamate
What is the general kv used for upper limb (hands, wrist, finger)
50 to 60 kv
What is the kV and mAs used for a projection of the foot?
60 kV, 3.2 mAs
What is the kV and mAs used for a projection of the ankle
60 kV, 3.2 mAs to 4 mAs
What is the kV and mAs used for a projection of the tibfib
60 kV, 4-5 mAs
What is the kV and mAs used for a projection of the knee WITHOUT a grid?
60 kV, 5 mAs
What is the kV and mAs used for a projection of the knee WITH a grid?
70 kV, 8 mAs
What is the kV and mAs used for a projection of the distal femur?
70 kV, 8 mAs
What is the kV and mAs used for a projection of the proximal femur?
70 kV, 12.5 mAs
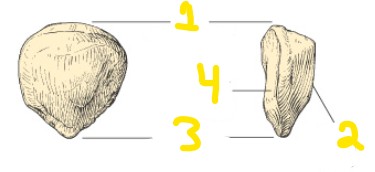
On this image of the patella, what does #3 represent?
Apex
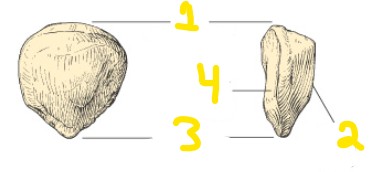
On the image of this patella, what does number 1 represent?
Base
A patient is being positioned for a AP oblique glenoid projection of their shoulder. They are in an RPO position. How much is the patient rotated?
35 to 45 degrees towards affected side
A patient with a hypersthenic body habitus is being positioned for a AP oblique projection of their shoulder. How much rotation should they have?
35 degrees
A patient is being positioned for an erect abdomen. What is the correct centering point?
2 inches above iliac crest
For an erect abdomen, why do we center 2 inches above the iliac crest?
to include diaphragm
What is the correct breathing technique for an AP erect abdomen?
end of expiration
What evaluation criteria effectively demonstrates proper positioning for an PA oblique hand projection?
midshafts of metacarpals should not overlap, some overlap of distal heads of third, fourth and fifth metacarpals but no overlap of distal second and third metacarpals should occur
A PA oblique projection of the hand is seen with the metacarpals overlapping. What is this an indication of?
over rotation
What is the correct centering point for a PA oblique projection of the shoulder? (Scapular Y)
scapulohumeral joint (2 inches below AC joint)
What is the correct evaluation criteria for a PA oblique Y view of the shoulder?
body of scapula seen on end without rib superimposition. The acromion and coracoid processes should appear as nearly symmetric upper limbs of the “Y”. The humeral head should appear superimposed over the base of the “Y” if the humerus is not dislocated.
During a Tangential Supraspinatus outlet view of the Shoulder (Neer method), what is the CR angle and centering point?
10 to 15 degree caudal angle. Centered posteriorly to pass through superior margin of humeral head which is located approximately 1 inch superior to medial aspect of scapular spine
What body position best demonstrates intraperitoneal when imaging the abdomen?
left lateral decubitus
The left lateral decubitus position for an abdomen x-ray best demonstrates free _________???
intraperitoneal air in the area of the liver in the right upper abdomen away from the gastric bubble
A lateral decubitus position for an abdomen requires the centering point to be:
2 inches (5 cm) above the iliac crest
What is the correct breathing instructions for a lateral decub abdomen x-ray?
expiration
What is the correct evaluation criteria for a lateral decub abdomen projection?
air filled stomach and loops of bowel and air-fluid levels where present. Also include bilateral diaphragm
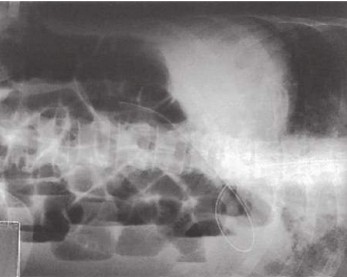
What is the patient position for this projection?
lateral recumbent (lying on left side)
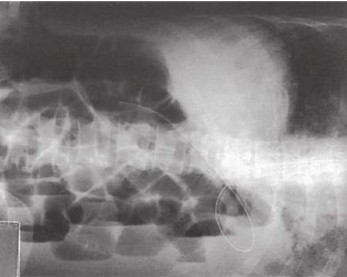
What is the correct centering point for this projection?
2 inches (5 cm) above the iliac crest
A lateral C-spine x-ray needs to be taken on a patient in a c-spine collar, is hypersthentic and cannot move. The first image demonstrates C1 and doesn’t show below C6. How can a repeating image be improved by only adjusiting the CR angle?
5 degrees caudal
A lateral C-spine x-ray needs to be taken on a patient in a c-spine collar, is hypersthentic and cannot move. The first image demonstrates C1 and doesn’t show below C6. Without adjusting the CR angle, what can be done to improve the repeat image?
someone could apply traction on the arms/shoulders, and perform on exhalation
During a routine series of the hand, a patient is unable to hold still for an oblique image. What can be used to help, and what does this do?
use a radiolucent sponge as it helps provide an accurate degree of obliquity. Also causes the long axis of the fingers to be parallel to the IR. Joints are open and phalanges are not foreshortened
During an AP axial foot projection, the patient’s metatarsal bases are superimposed. What caused this?
lateral rotation of the foot
A patient requires a foot x-ray and they have a high longitudinal arch. Does this change how much rotation they need for an oblique image? If so, how much?
Should have 45 degree rotation
Someone enters the DI department with a low longitudinal arch. When positioning for the AP oblique image, how much should their foot be rotated?
30 degrees
During a lateral knee x-ray, the patient’s leg is externally rotated. How would the condyles appear on the image?
the medial condyle would be seen anterior to the lateral condyle
In the recovery room, a patient is getting a portable knee x-ray. After taking the cross table lateral image, the medial condyle can be seen anterior to the lateral condyle, and the fibular head has minimal superimposition of the tibia. What was wrong with this image?
the patient had their leg externally rotated
During a routine series of the knee, the lateral knee x-ray demonstrates the lateral condyle posterior to the medial condyle. How can this be fixed on an image?
internally rotate the patient’s leg
What is the patient position for an anterior oblique C-spine?
patient is erect with their arms by their sides, MSP is aligned to CR and midline to IR. patient’s head and body rotated 45 degrees. Chin is protracted to stop the mandible from superimposing the vertebrae, along with the chin being elevated to place AML parallel with the floor
A patient is postioned for an AP oblique ballcatchers hand projection. What is the correct centering point?
midpoint between both hands at the level of the fifth MCP joints
What is the clinical indication to perform an AP oblique Ballcatchers method hand projection?
rheumatoid arthritis
A correctly positioned AP oblique ball catchers hand projection demonstrates:
midshafts of second through fifth metacarpals and base of phalanges should not overlap; MCP joints should be open; no superimposition of the thumb and second digit should occur
How is the centering point for an AP elbow projection localized?
moving 2cm distal from the humeral condyles
The lateral position of the elbow requires flexion of 90 degrees in order to visualize:
the posterior fat pad and ensure proper positioning
The radial tuberosity faces ________ in a lateral view of the elbow
anteriorly
A lateral semi-axial radial head projection requires a ___ degree CR angulation
45
What are the two bony processes on the proximal ulna?
coronoid process and olecranon process
What is a condyle?
rounded protuberance at the end of a bone that forms an articulation
What is an epicondyle?
the eminence at the articular end of a bone that is located ABOVE a condyle
What is a “process”?
a projection or outgrowth of bone
What is a tubercle?
small rounded elevation or eminence of a bone
What is the topographical landmark for vertebra prominens?
C7-T1
What is the topographical landmark for the jugular notch?
T2-T3
What is the topographical landmark for the sternal angle?
T4-T5
What is the topographical landmark for the xiphoid process?
T9-T10
What is the topographical landmark for the inferior costal margin?
L2-L3
What is the topographical landmark for the iliac crest?
L4-L5 interspace
What is the topographical landmark for the ASIS?
S1-S2
What is the topographical landmark for the greater trochanter?
symphysis pubis
Using a left wrist as an example, describe SLTPTTCH going from right to left
Scaphoid lunate triquetrum pisiform trapezium trapezoid capitate hamate
How do you find the elbow joint in a lateral projection of the elbow? What do you palpate? (give answer in cm and inches)
palpate posterior surface of olecranon process and move 4cm medially (1.5 inch)
In a true lateral elbow, what are the 3 concentric arches demonstrated?
trochlear sulcus, trochlear notch of the ulna, and the double ridge (outer ridge or the capitulum and trochlea)
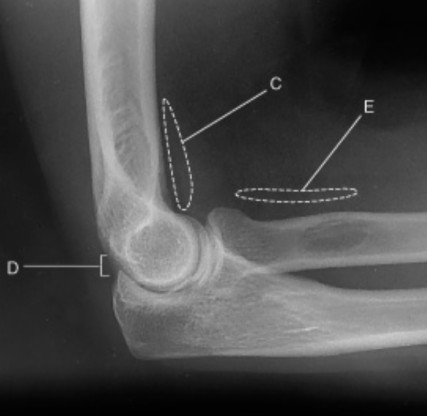
On this true lateral elbow projection, what does C represent?
anterior fat pad
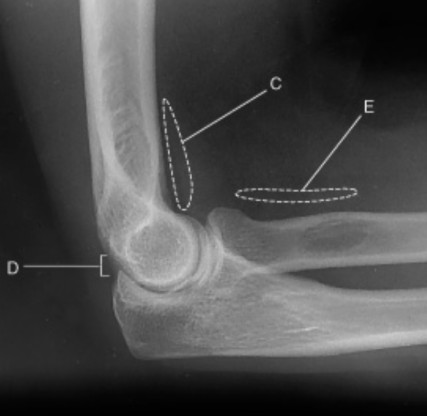
On this true lateral elbow projection, what does the teardrop shape represent?
anterior fat pad
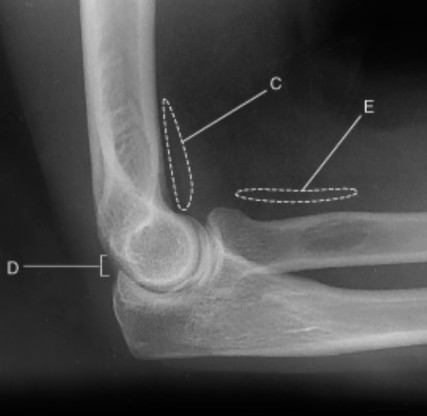
On this true lateral elbow, describe the appearance of C
anterior fat pad is teardrop shape
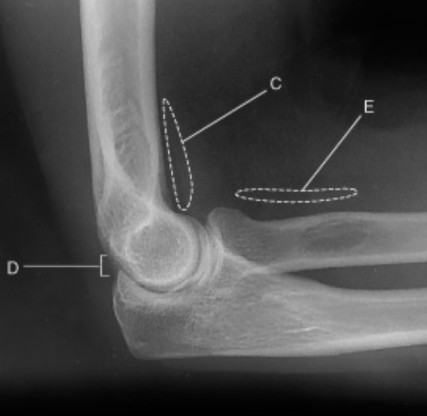
On this true lateral elbow projection, what does D represent?
posterior fat pad
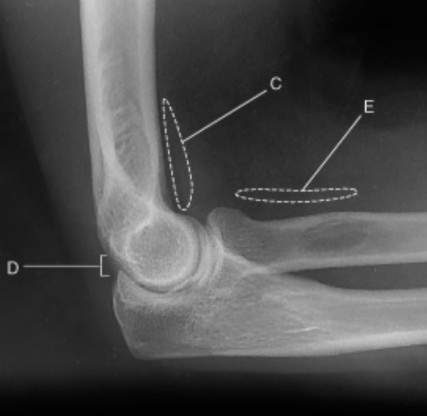
On this true lateral elbow projection, when does the posterior fat pad become visible?
only visible when there is pathology
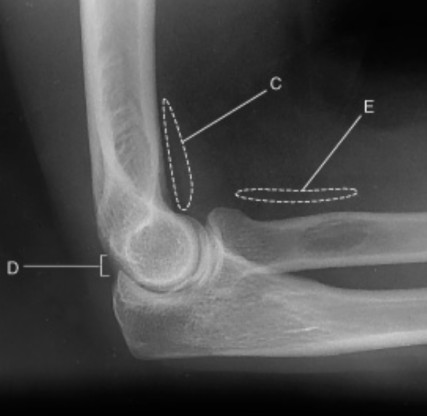
On this true lateral elbow projection, what does E represent?
supinator fat stripe
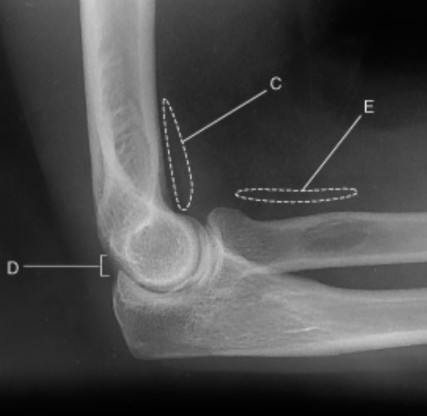
On this true lateral elbow projection, which fat pad is only demonstrated when there is pathology?
posterior fat pad
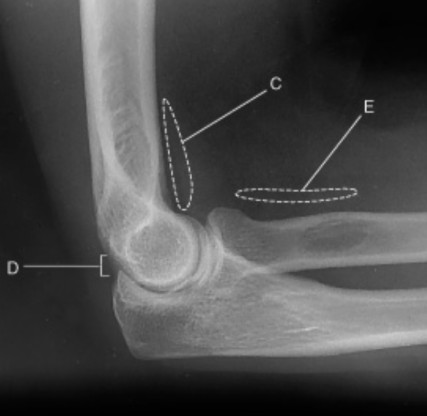
On this true lateral elbow projection, when is E commonly used for? Hint: used to d______
may be used to diagnose radial head or neck fractures

What does C represent in this foot image?
medial cuneiform

What does E-I represent in this image?
intermediate cuneiform, navicular cuneiform joint, navicular, talus, calcaneus

What does J-M represent in this foot image?
cuboid, lateral cuneiform, 5th metatarsal tuberosity, 5th metatarsal base, 4th tarsometatarsal joint
What is the correct CR angle used for an dorsoplantar projection of the foot?
10 degrees cephalic
A patient has a high arch and is being positioned for a dorsoplantar projection of the foot. What is the correct CR angulation?
15 degrees cephalic
What is the recommended amount of foot obliquity for a medial rotation oblique foot projection?
30 to 40 degrees
Why is a 40 degree foot obliquity recommended for an AP oblique projection of the foot?
to demonstrate tarsals and proximal metatarsals best relatively free of superimposition
What is the correct evaluation criteria for an AP oblique foot?
entire foot should be demonstrated from the distal phalanges to posterior calcaneus and proximal talus
How can you tell if a foot is correctly positioned for an AP oblique foot projection?
third through fifth metatarsals are free of superimposition, first and second metatarsal bases can be superimposed, sinus tarsi is open
What is the correct centering point for an AP oblique projection of the foot?
base of third metatarsal
What is the correct entering point for a mediolateral foot projection?
medial cuneiform (at the level of the base of the third metatarsal)
What is the evaluation criteria for a lateral foot projection?
entire foot demonstrated with 1 inch (2.5 cm) of distal tibfib. Heads of metatarsals are superimposed with the tuberosity of the fifth metatarsal base seen in profile
TRUE OR FALSE: the patient should carefully dorsiflex their foot if possible to assist in positioning for a lateral foot projection
TRUE
For an AP erect weight bearing feet projection, what is the correct CR angle and centering point?
15 degrees posteriorly to midpoint between feet at the level of the base of the metatarsals
What anatomy is demonstrated for an AP weight bearing foot projection?
bilateral feet from soft tissue surrounding phalanges to distal portion of talus
What is the correct centering point for a lateral WEIGHT BEARING foot projection?
level of base of third metatarsal
What anatomy is correctly demonstrated for a lateral WEIGHT bearing foot?
entire foot should be demonstrated along with 1 inch (2.5 cm) of distal tibfib. Distal fibula seen superimposed over posterior half of tibia, and plantar surfaces of heads of metatarsals should be superimposed if no rotation is present. The longitudinal arch of the foot must be demonstrated in its entirety

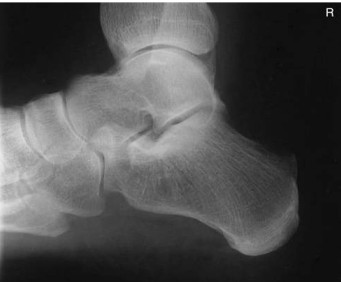
Name what anatomy is demonstrated in this projection of the foot
entire foot should be demonstrated along with 1 inch (2.5 cm) of distal tibfib. Distal fibula seen superimposed over posterior half of tibia, and plantar surfaces of heads of metatarsals should be superimposed if no rotation is present. The longitudinal arch of the foot must be demonstrated in its entirety
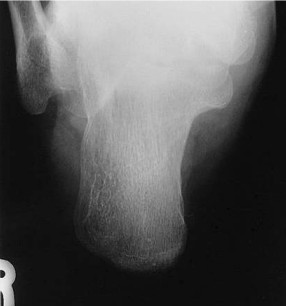
What is the correct CR angle and centering point for this projection?
CR 40 degrees cephalad from long axis of foot (40 degrees from vertical if long axis of foot is perpendicular to IR), CR to base of third metatarsal to emerge at a level just distal to lateral malleolus
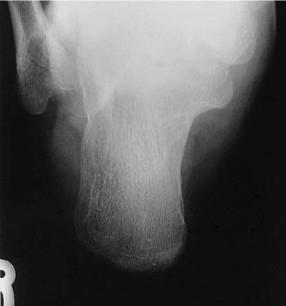
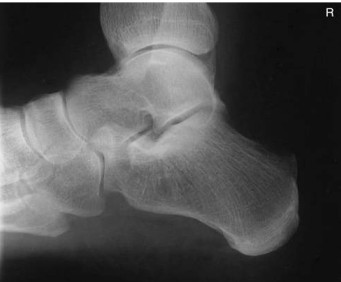
Discuss the correct anatomy demonstrated on this image
entire calcaneus should be seen from tuberosity posteriorly to talocalcaneal joint anteriorly
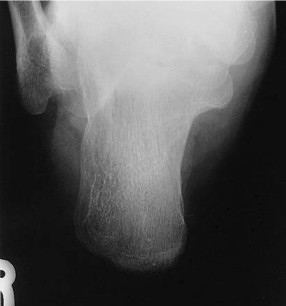
What is in profile on this image?
susentaculum tali is in profile medially
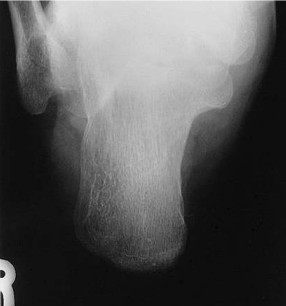
What indicates on this image that the CR angle was correct?
open talocalcaneal joint space
A patient is being positioned for a plantodorsal (axial) calcaneus projection. The long axis of the plantar surface of the foot is not perpendicular to the IR. How should the CR angle be changed?
increase CR angle
What is the correct centering point for this calcaneus projection?
1 inch (2.5 cm) inferior to medial malleolus
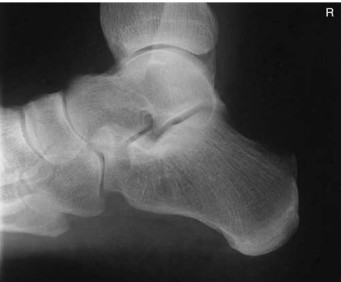
Should the foot be dorsiflexed or left in a neutral position for this mediolateral calcaneus projection?
Dorsiflex foot
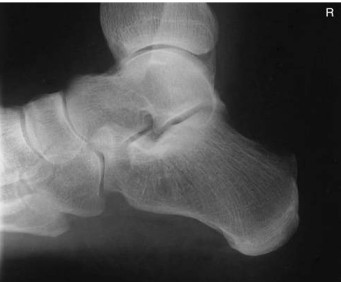
What anatomy is correctly demonstrated on this lateral calcaneus
calcaneus demonstrated in profile with talus and distal tibfib demonstrated superior and navicular and open joint space of the calcaneus and cuboid demonstrated distally
On this lateral calcaneus image, what indicates no rotation?
superimposed superior parts of the talus, open talocalcaneal joint, lateral malleolus superimposed over posterior half of the tibia and talus. Tarsal sinus and calcaneocuboid joint space should appear open
During an AP projection of the ankle, should the foot be dorsiflexed?
No have it remain in a neutral position

What is the correct evaluation criteria for an AP ankle projection?
distal one third of tibfib and lateral and medial malleoli, and talus and proximal half of metatarsals should be demonstrated