Looks like no one added any tags here yet for you.
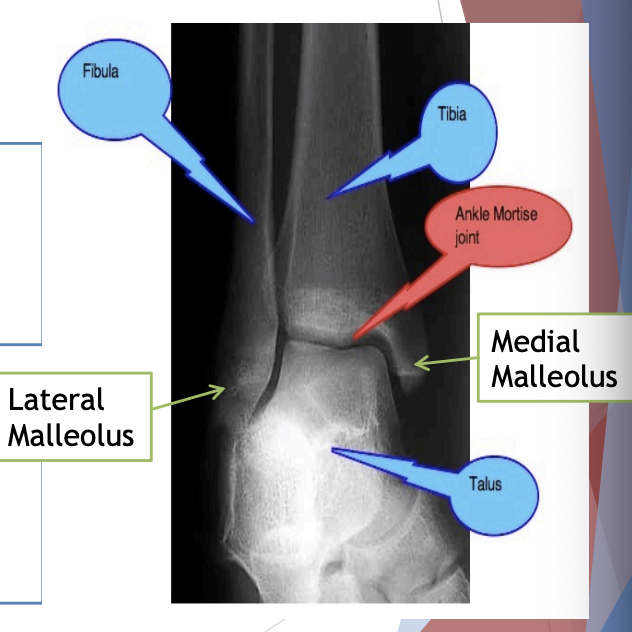
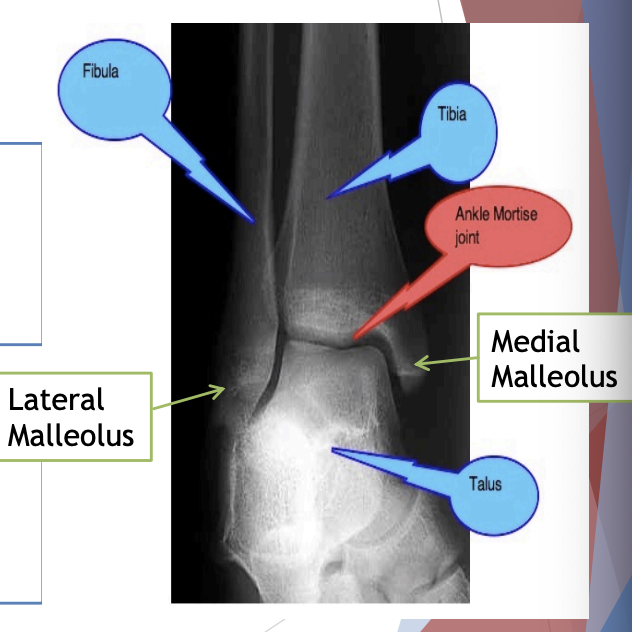
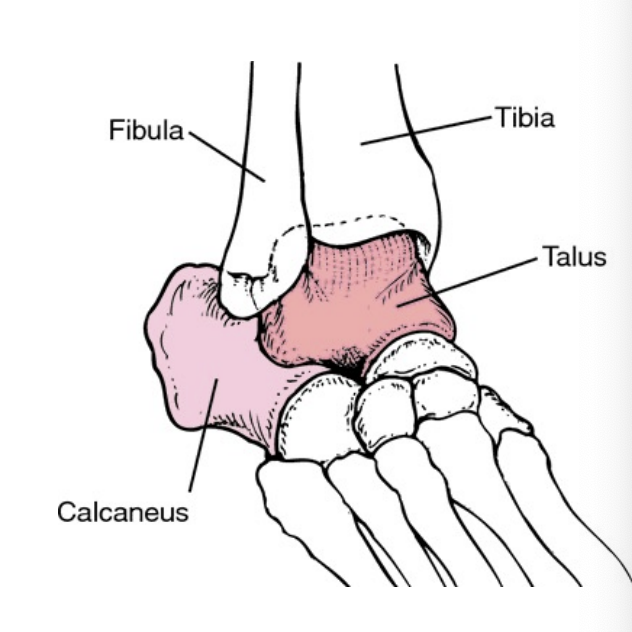
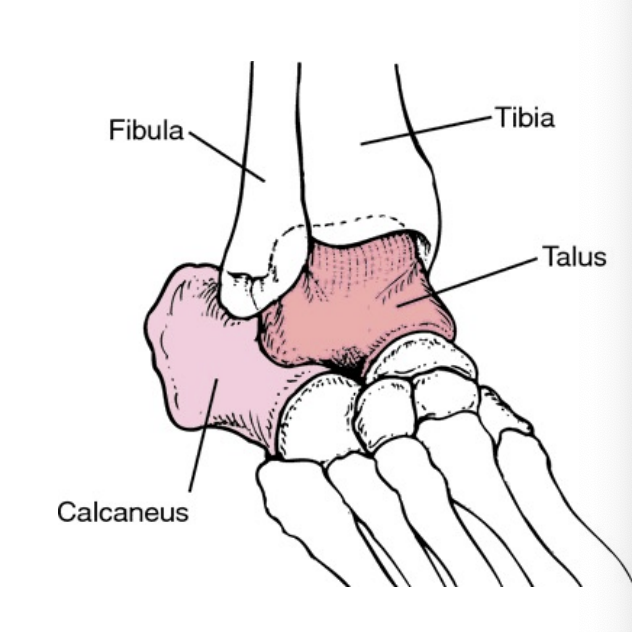
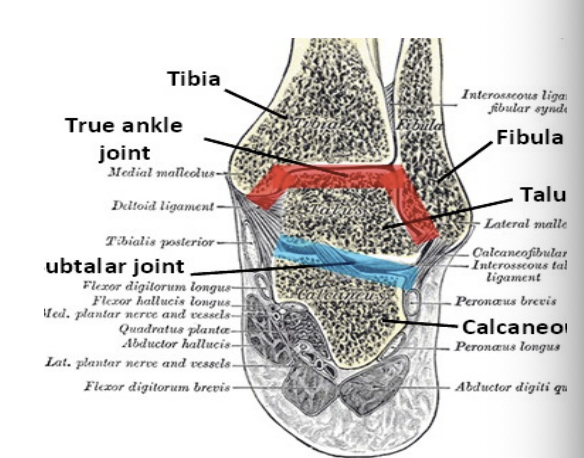
Tibia
Principal weight bearing bone of lower leg
Medial malleolus
Fibula
Long thin bone, lateral to tibia primarily for muscle attachment
Lateral malleolus
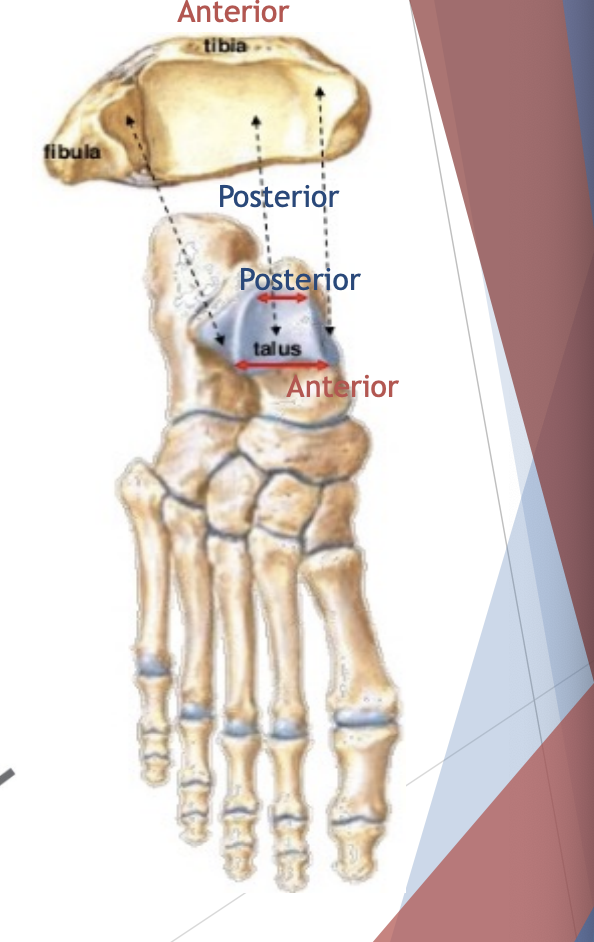
Talus
Rests on calcaneus
Main weight bearing bone of ankle joint
Talar dome (trochlea)
Calcaneus
Heel bone
Largest tarsal bone
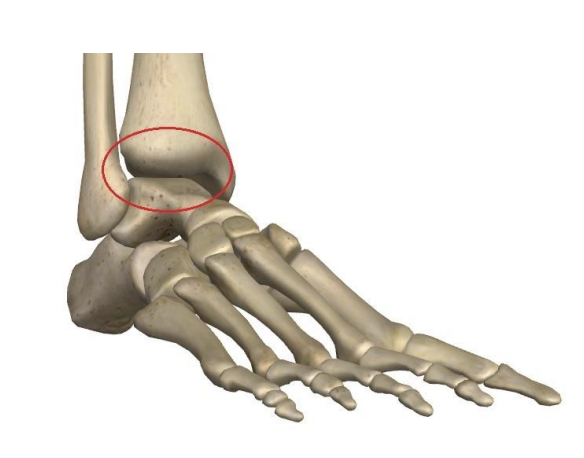
Talocrural joint
Formed between the distal tibia-fibula and the talus, and is commonly known as the ankle joint
Synovial and Hinge joint (flexion & extension) aka plantar flexion and dorsiflexion
Eversion and Inversion
A result of subtalar joint movement between talus and calcaneus as well as intertarsal joints.
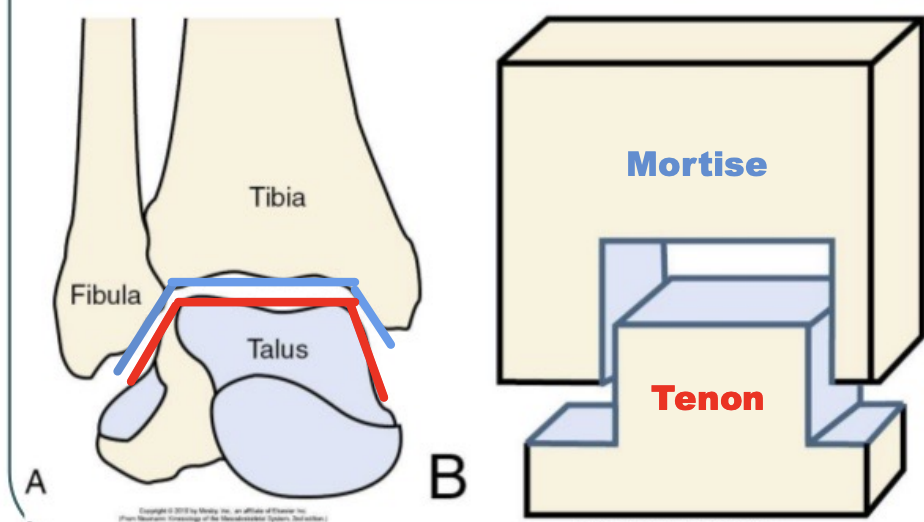
Distal Tibiofibular Joint
Ankle Mortise
Articulations
Tibia & Fibula (ankle mortise)
Syndemosis (1-2 mm of movement)
Anterior and posterior inferior tibiofibular ligaments
Interosseous membrane
AITFL
Anterior-Inferior Tibiofibular Ligament
IM
Interosseous membrane
PITFL
Posterior-Inferior Tibiofibular ligament
TrTFL
Transverse Tibiofibular ligament
Talus(tendon)
Wider anteriorly- joint more stable in dorsiflexion
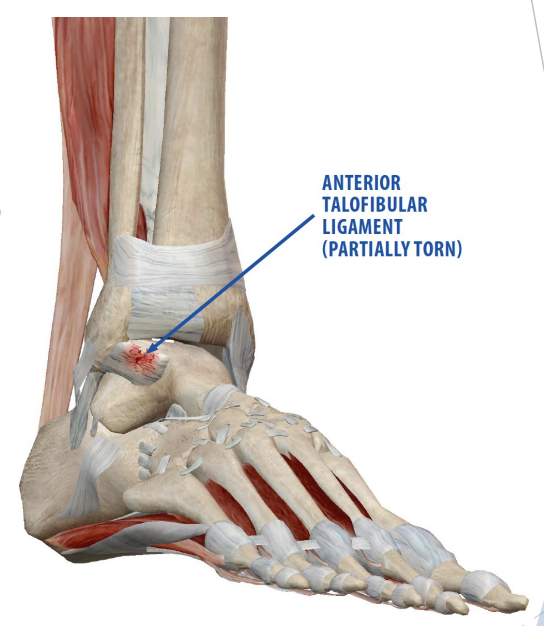
ATFL
Anterior talofibular ligament
PTFL
Posterior Talofibular ligament
CFL
Calcaneofibular ligament
Ankle Muscles (Anteriorly)
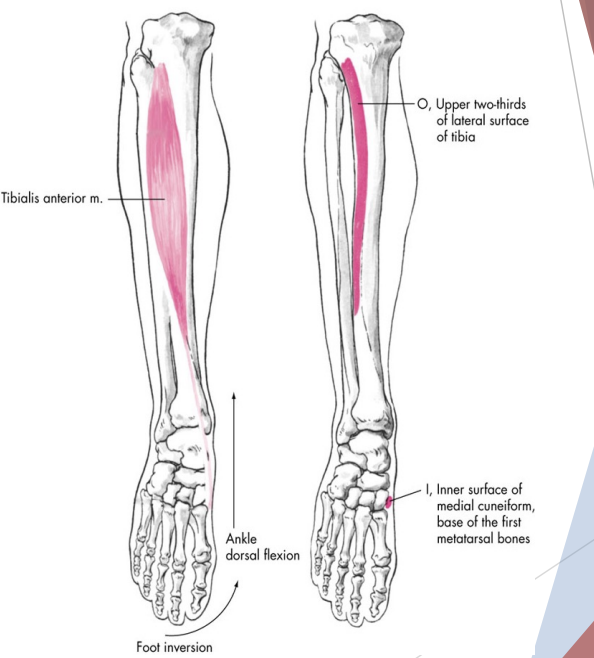
Tibialis Anterior
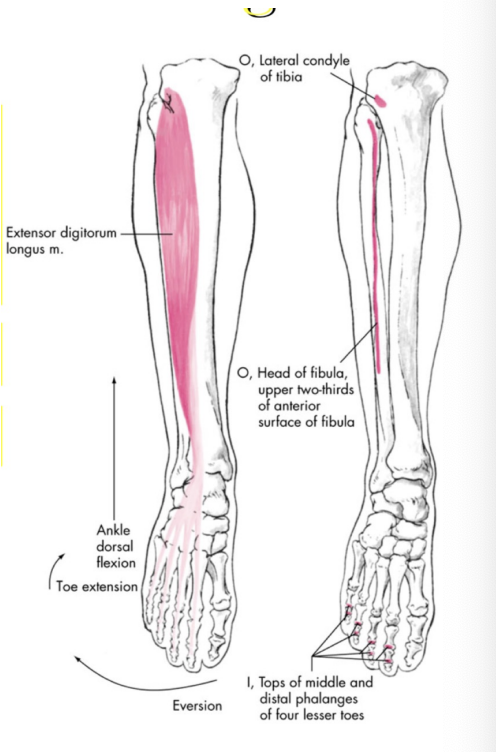
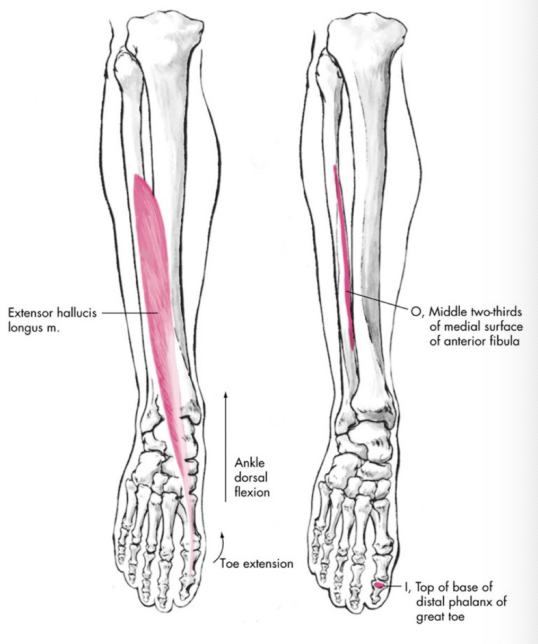
EHL & EDL
Dorsiflexion, inversion/flexion
Ankle Muscle (Posteriorly)
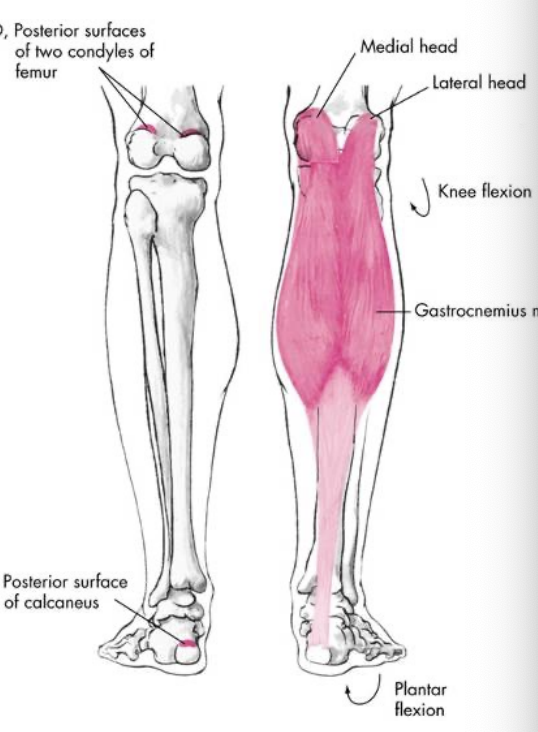
Gastrocnemius & soleus
Plantarflexion
Ankle Muscle (Posterior Medial)
Tibialis Posterior
FHL & FDL
Inversion, plantarflexion
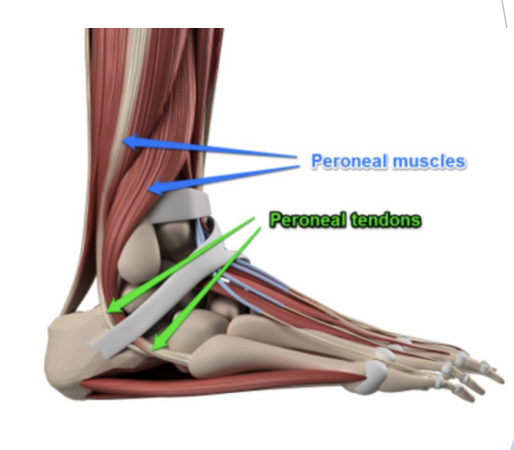
Ankle Muscle (Laterally)
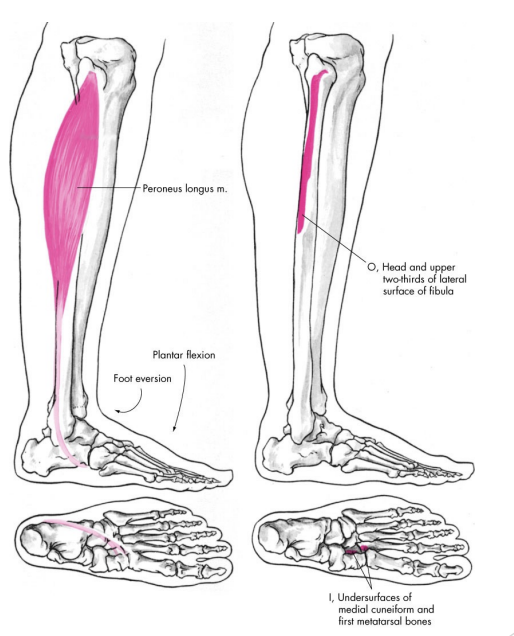
Peroneus longus, brevis & tertius
Eversion
Tibialis Anterior
Dorsiflexion of ankle
Weak inversion of ankle
Extensor Digitorum Longus
Extensor of toes 2 through 5
Dorsiflexion of ankle
Eversion of foot
Extensor Hallucis Longus
Extension of 1st toe
Dorsiflexion of ankle
Weak inversion of ankle
Gastrocnemius
Plantarflexion of ankle
Flexion of ankle
Contraction of calf muscle
Crosses the knee joint
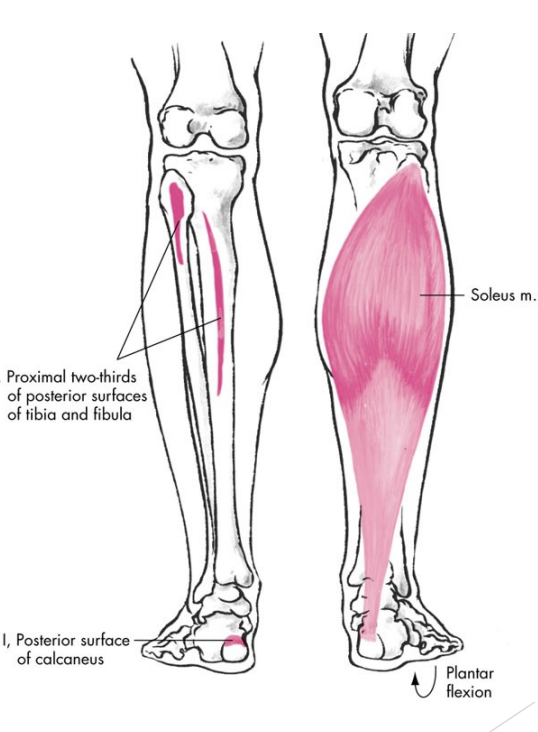
Soleus
Plantarflexion of ankle
Important for keeping us upright
Shares with achilles tendon
Doesn’t cross the knee joint
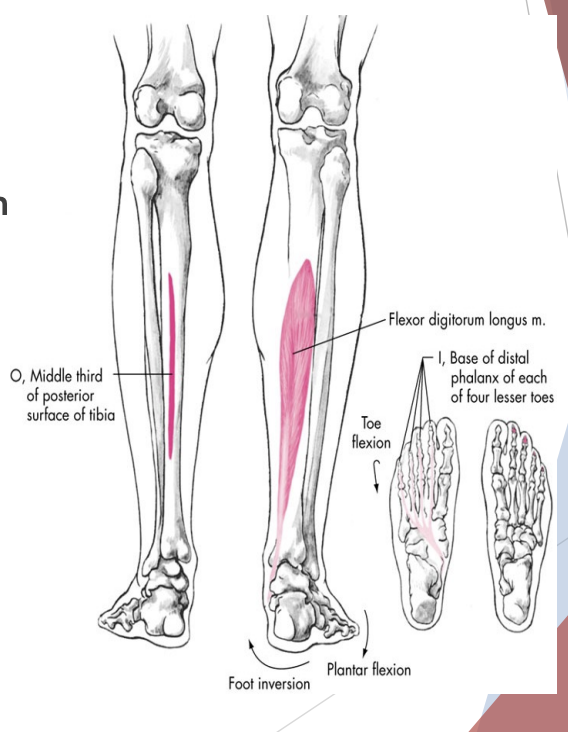
Flexion Digitorum Longus
Flexion of toes 2 through 5
Plantar flexion of ankle
Weak inversion of foot
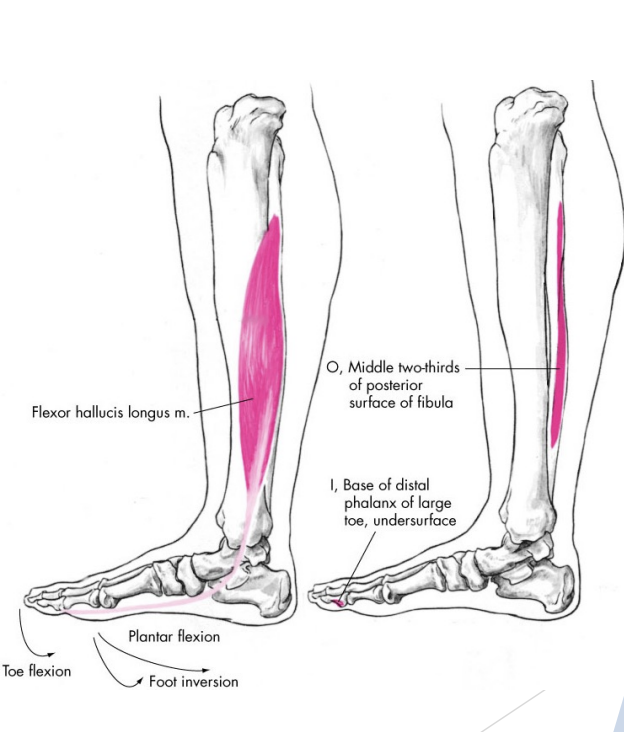
Flexor Hallucis Longus
Flexion of 1st toe
Plantar flexion of ankle
Weak inversion of ankle
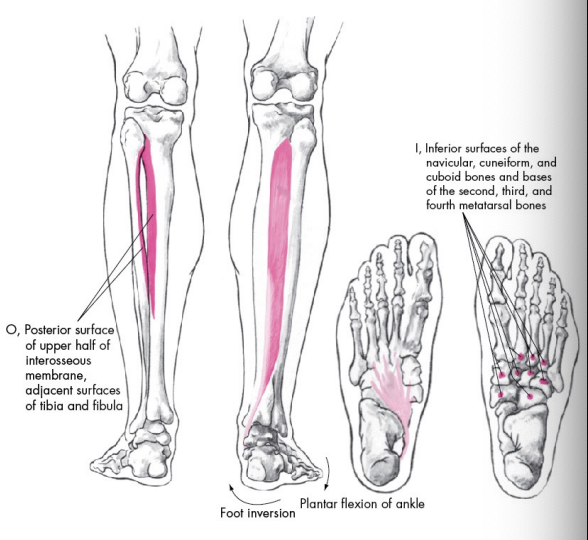
Tibialis Posterior
Inversion of foot
Plantar flexion of ankle
Crosses over to the medial side pulling it into the inverted side (inversion)
Peroneus (fibularis) longus
Eversion of foot
Plantar flexion of ankle
Tilt the sole of the foot away from the midline of the body and to extend the foot downward away from the body at the ankle.
Peroneus (fibularis) brevis
Eversion of foot
Plantar flexion of ankle
Receives innervation from the superficial peroneal nerve, and its arterial supply is by muscular branches of the peroneal artery
Muscles grouped by Plantar Flexion
Gastrocnemius
Soleus
Flexor digitorum longus
Flexor hallucis longus
Peroneus longus
Peroneus brevis
Plantaris
Tibialis anterior
Muscles grouped by Dorsiflexion
Tibialis anterior
Extensor digitorum longus
Extensor hallucis longus
Muscles grouped by Inversion
Tibialis posterior
Tibialis anterior
Flexor digitorum longus
Flexor hallucis longus
Muscles grouped by Eversion
Peroneus longus
Peroneus brevis
Extensor digitorum longus
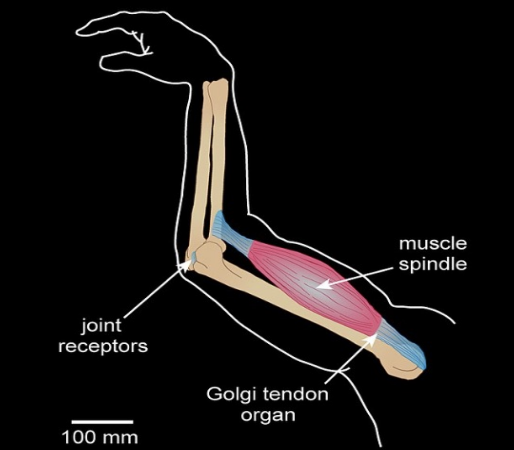
Proprioception
Sense of body position without the aid of vision
Kinaesthesia
Awareness of position and movement of body parts using proprioceptive sensory organs. Mediated by mechanosensory neurons in muscles, tendons and joints. Gives information on limb velocity, movement and loads on limbs. Feedback helps create overall picture of body position, movement, and acceleration
3 Basic types of proprioceptor neurons in vertebrates
Muscle Spindles
Golgi Tendons Organs
Mechanoreceptors
Muscle Spindles
Found in skeletal muscle fibres
Golgi Tendon Organs
At interface of muscles and tendons
Mechanoreceptors
Found in joint capsule surrounding synovial joints
Why do we care about proprioceptors and injury?
Proprioception and kinaesthesia can be interrupted/impaired following injury. What are the implications of this?
Ankle Assessment
History of current injury
Past history
Compare with uninjured extremity
Inspection/Observation
Range of Motion (ROM)
Ligament Test
Functional/Special tests
Palpation
Be systematic
Contusion
History: Traumatic bruise: direct blow
Symptoms: Pain, tenderness, Discolouration, Limp?
Differential Diagnosis: Fracture, Body tenderness? Then X-Ray
Treatment: POLICE, Padding, Rehabilitation
Strain
Injury to tendon or muscle
History: Sudden Stretch (run, jump)
Symptoms: Pain, tenderness, may feel or hear a “snap”
Limp?(2nd or 3rd degree)
Treatment: POLICE, Tape or cast, ROM exercises, Physiotherapy
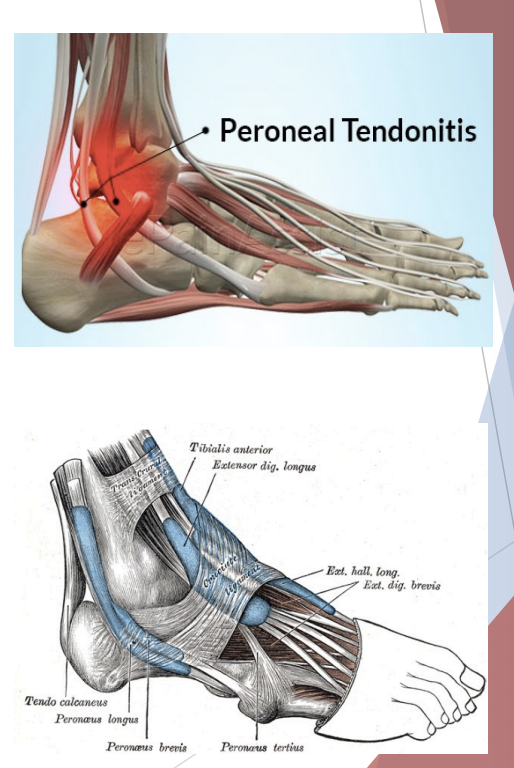
Tendinopathy
Tendonitis, Tendinosis or Tenosynvotis
History: acute strain or overuse
Symptoms: Those of acute strain?, Tenderness, Crepitus. Swelling/bogginess
Treatment: Complete tendon test(brace?), NSAID, Physio & ROM exercises, Tape, Slow return to exercise - graded
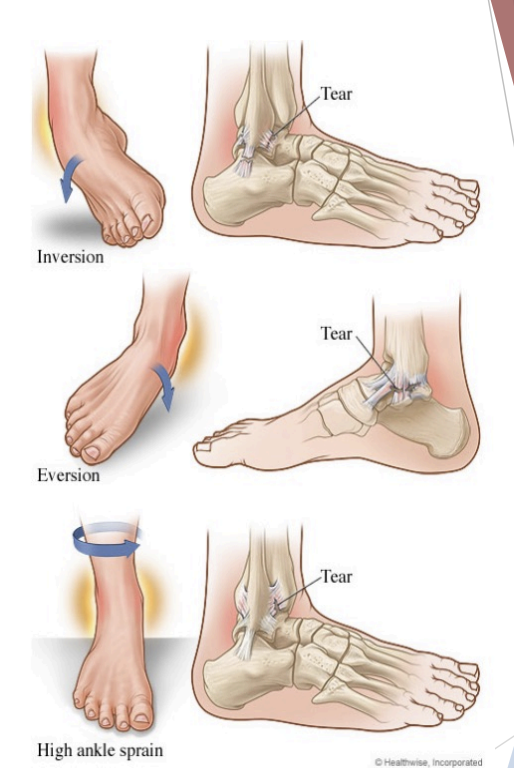
Sprain
Acute injury to ligament(s), very common, usually under-treated
Symptoms & disability for months
Most common in inversion(85%): usually in plantarflexion, ATFL
Less common in eversion(10%): usually forced eversion in dorsiflexed position, deltoid ligament
Dorsiflexion (Syndesmosis/”High ankle sprain”) sprains are rare
May destabilize mortise. AITFL damaged
Lateral (Inversion) Ankle Sprain
Has three degrees of tears in LCL
1st degree sprain
Partial tear of ligament(s)
Symptoms: Mild tenderness, pain, swelling
NO snap, no limp, no increased laxity
Treatment: POLICE, reduce predisposing factors
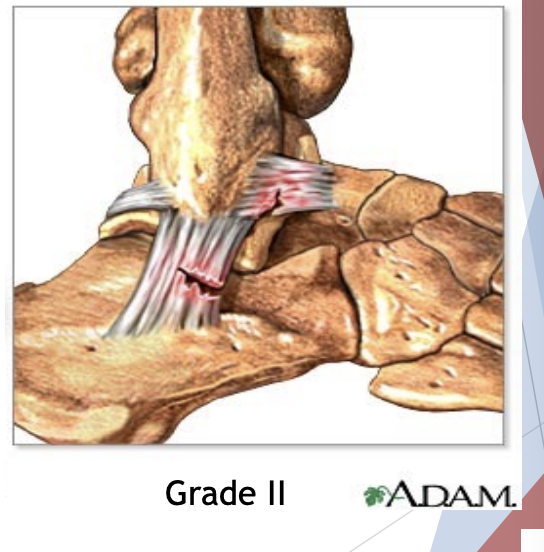
2nd degree sprain
Tear of ligament(s) - incomplete
Symptoms: Snap/pop, Pain, Tenderness, Swelling, Bruises, Limp, Resists inversion, increased laxity(has end-ponts)
Treatment: POLICE- 2 days rest, X-Ray?, Air cast, tape or plastar cast and NSAID
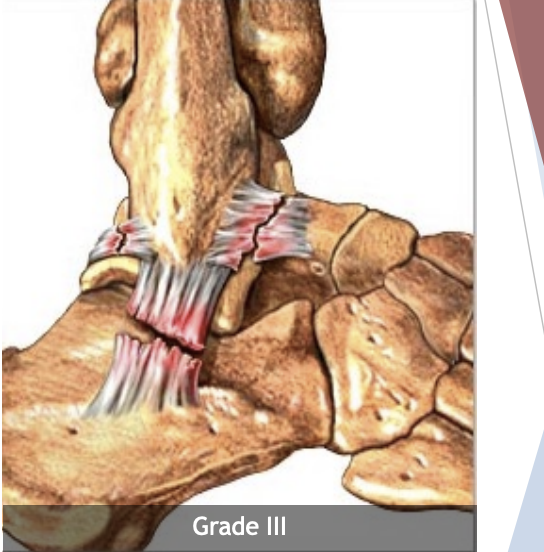
3rd degree sprain
Complete rupture of ligament(s)
Symptoms: Same as 2nd but more severe, Positive Anterior drawer test for inversion sprain, increased laxity, nor firm end point on talar tilt test, higher risk of fracture or dislocation
Treatment: Stabilize(NPO), get medical help, X-Ray, may need surgery, cast, Physio and rehab
Anterior Sprain Assessment Anterior Drawer Test
A quick way for your healthcare provider to diagnose a torn ACL. They'll move your lower leg to see if your ACL is holding your knee in place like it should. If your leg moves further than usual, you might have an ACL tear.
Ankle Sprain Assessment Talar Tilt Test
Assesses the lateral ankle ligaments for laxity, specifically calcaneofibular ligamentous laxity. The test is performed by stabilizing the distal leg in a neutral position while the examiner inverts the ankle. The degree of inversion is compared with the uninjured ankle.
Syndesmosis Sprain “High Ankle Sprain”
Forced dorsiflexion with external rotation
Tenderness between distal tibia & fibulae
Anterior ankle swelling
Patient walks on toes to avoid painful dorsiflexion
Positive side to side talar tilt test (widened mortise)
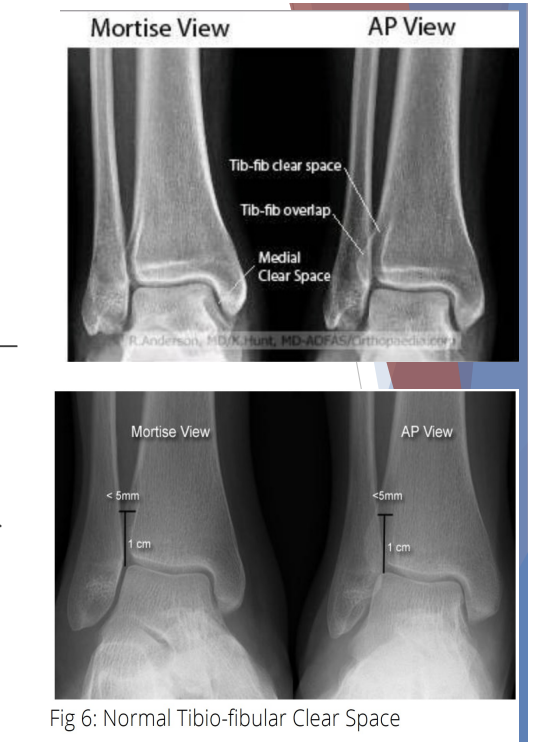
Sydesmosis Sprain “High Ankle Sprain” X-Ray Findings
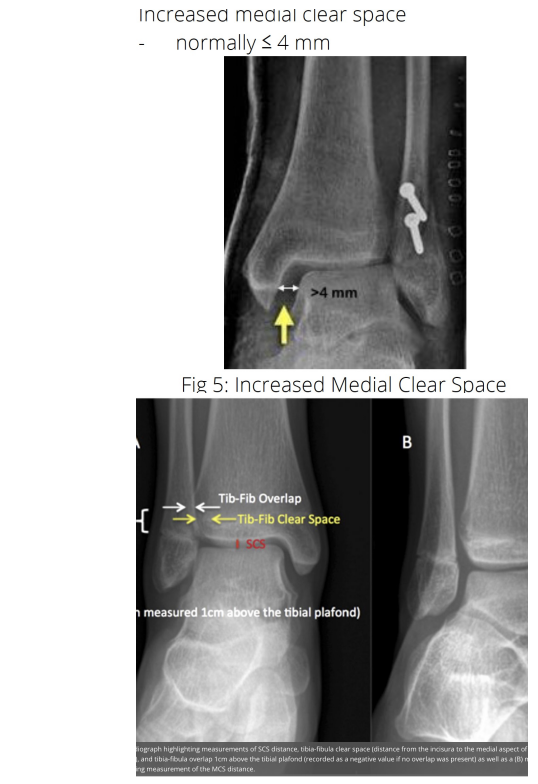
Increased tibiofibular (syndesmosis) clear space
Decreased tibiofibular overlap
Increased medial clear space
Ankle Sprain Complications
Recurrence (degrees)
Chronic instability (2nd/3rd)
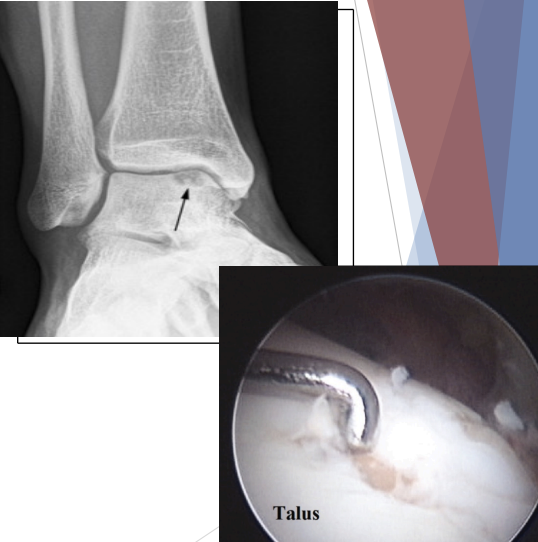
Fracture: Malleolus(tibia or fibula), Fibular shaft(spiral), Talus - osteochondral fracture
Dislocation
Subtalar joint injury
Temporary Loss of Proprioception
Periods of growth - adolescence
Significant changes in bodyweight/size
Increased flexibility - stretching
Fatigue
Vitamin B6 overdose
Alcohol consumption
Musculoskeletal injury
Concussion
CNS injury
Permanent Loss of Proprioception
Joint hyper-mobility
Viral Infection
Brain injuries, Parkinson, ALS
Assessing Proprioception
Joint Position Matching
Field Sobriety Test
Romberg Test
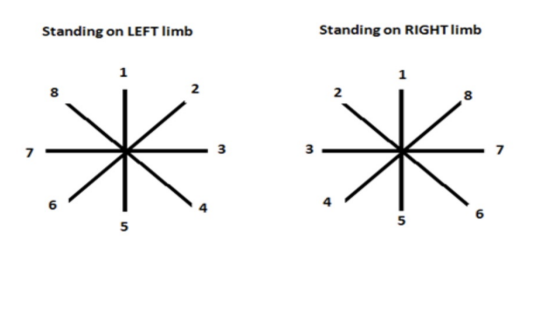
Y test or Star Excursion Balance Test
Star Excursion Balance Test (SEBT)
Dynamic balance test, requires strength, flexibility and proprioception. Using injured & uninjured leg to see balance & imperfections
Fractures
Evidence: History of severe trauma Deformity, Bony tenderness, Crepitus, difficultly weight bearing
Treatment: Recognize likelihood, Stabilize & Transport if suspicious, X-Ray, Reduction(may need surgery), Cast, Physio and Rehab
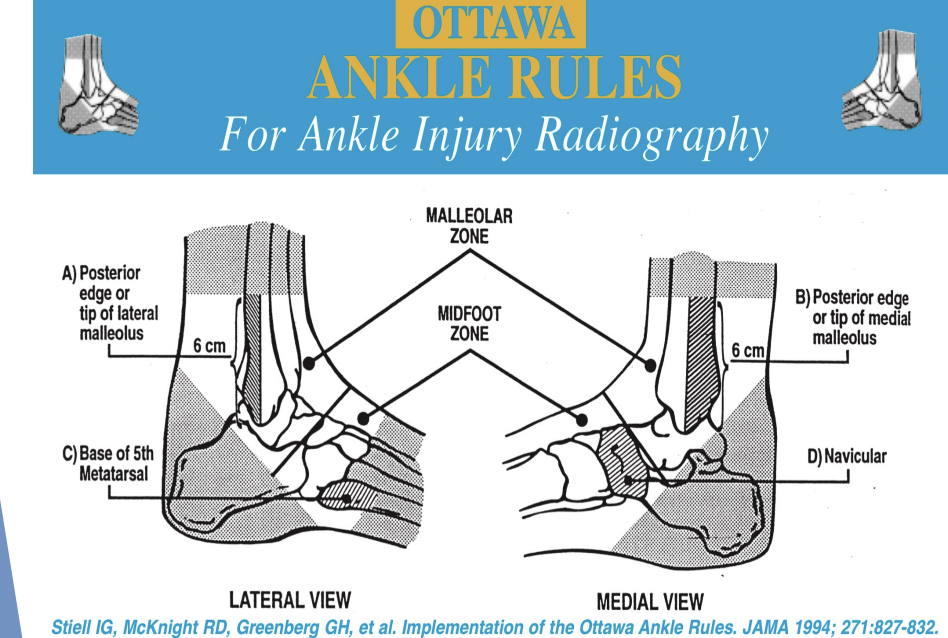
Ottawa Ankle Rules
Helps determine if x-ray needed
Ankle X-Rays needed if pain in malleolar area AND 1 of:
Pain over distal 6 cm inferior or posterior pile of med or lat malleolus
Inability to weight bear at all at time of injury
Inability to weight bear 4 steps at time of examination (ie. in hospital)
Foot X-Rays needed if pain in midfoot area AND 1 of:
Inability to bear weight at all at time of injury
Inability to weight bear 4 steps at time of examination (ie. in hospital)
Tenderness along base of 5th metatarsal or navicular bone
Ankle Rehab
Activity Modification/ Controlled Weight Bearing
Range of Motion
Strengthening
Balance/ Proprioception
Running Progression
Return to Sport
Activity Modification/ Controlled Weight bearing
Partial or non weight bearing during initial healing period, may promote faster or stronger healing
If possible maintain partial weight bearing to help combat muscle atrophy, proprioceptive loss, decreased circulation, tendinitis
Range of Motion
ROM activities should be kept pain free
Minimize inversion and eversion initially
Towel assisted stretching into plantar and dorsiflexion
As pain decreases include inversion/eversion
Spelling alphabet with foot, towel pulls into inversion/eversion
Strengthening
Isometric exercises in all four ankle movement directions
Isotonic exercises into plantar and dorsiflexion
As pain free ROM increases, can add resistance to inversion and eversion exercises
Lighter resistance and higher reps (2 sets of 10 reps, progressing to 4 sets of 10 reps)
Balance/Proprioception
Initially seated rocker board plantar flexion/ dorsiflexion
Once pain free add seated rocker board inversion/eversion
Double leg stand eyes open, progress to single leg stand eyes open
Double leg stand eyes close, progress to single leg stand eyes close
Double and single leg exercises on Rocker, BOSU, mini trampoline, eyes open, eyes closed , perturbations
Running Progression
Pool Running
Walking
Running on mini ramp
Side to side hopping
Karaoke
Ladder work
Running on inside turf of track
Running on harder surface
Running figure eights (gradually making circles smaller)
Running and cutting
Sprinting
Sprinting with cutting
Return to Sport
Walking drills
Jogging drills
Running drills
Drills without contact
Drills with contact
Return to play
Criteria for return to sport
Full pain-free ROM?
May take 10 weeks to restore
Normal strength?
Strength loss may be avoided by early functional training
Normal proprioceptive function function?
How measure this?
Injured ligament healed?
May take at least 6 months
Use of tape or brace
Brace or tape should be used to prevent re-injury until rehabilitation program has been completed
Provided effective injury prevention in athletes with previous ankle injury, but not in uninjured players
Benefit most through proprioceptive stimulated
No effect on sprint and jump performance