Diabetes Insipidus (DI) & Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
25 Terms
Diabetes Insipidus is
-Disorder of the posterior lobe of the pituitary gland
-Deficiency of ADH (vasopressin)
etiology of DI
-Head trauma
-Brain tumor
-Surgical ablation of pituitary gland
-Failure of renal tubules to respond to ADH
-CNS infections
-Tumors
CM of DI
-Dilute, water-like urine
-Specific gravity decreases 1.001-1.005
-Intense thirst
-2-10 L cold water
specific gravity for DI urine
1.001-1.005
patients are so _____ due to water loss so they tend to want ______
-thirsty
-2-10 L cold water
Diagnostics for DI
-Fluid deprivation test
-Desmopressin trial
-Plasma ADH levels
-Plasma urine and serum osmolality
-IV hypotonic fluid
What happens to UO with DI
-INCREASED
-urine is very DILUTE
Medical Management for DI
-Replace ADH
-Ensure adequate fluid replacement (hypotonic fluid)
-Identify and correct underlying intracranial pathology
Pharmacologic Management
-VP
-IM or intranasal route
-Thiazide diuretics : cause fluid retention due to compensation
*Nephrogenic classification:
-Ibuprofen, Indocin, aspirin, thiazide diuretics and mild salt depletion
for nephrogenic DI meaning the kidney tubules do not respond to ADH what do we give
-Ibuprofen
-Indocin
-aspirin
-thiazide diuretics
-mild salt depletion
SERUM SODIUM DI is
120
-sodium is low because of the diuresis and also can be diluted due to hypotonic fluid
Normal specific gravity of urine
1.005-1.030
Nursing Management
-Patient and family education
-Administer medication
-Vasopressin causes vasoconstriction: monitor for CORONARY ARTERY DISEASE
-Educate s/s of hyponatremia
-Medical alert bracelet
when giving vasopressin for DI you must monitor for
monitor for CORONARY ARTERY DISEASE
what should you give a patient who has DI
medical alert bracelet
SIADH
-TOO MMUCH ADH
SIADH etiology
-Non-endocrine in nature
-Bronchogenic carcinoma
-Severe pneumonia
-Pneumothorax
-Malignant tumors
-Disorders of CNS
-Head injury
-Brain surgery/tumor
-Infection
non-endocrine SIADH etiology
-Bronchogenic carcinoma
-Severe pneumonia
-Pneumothorax
SIADH patho
Excessive ADH secretion from the pituitary gland even in the face of subnormal serum osmolality
clinical manifestation of SIADH
-Concentrated urine
-Retention of fluids
-Sodium deficiency (dilutional hyponatremia)
Management of SIADH
-Elimination of underlying cause
-Restrict fluid intake
-Diuretics (LASIX)
-Fluid restriction if severe hyponatremia is present
what must you monitor for patients with DI and SIADH
-Close monitoring of I/O, daily weight
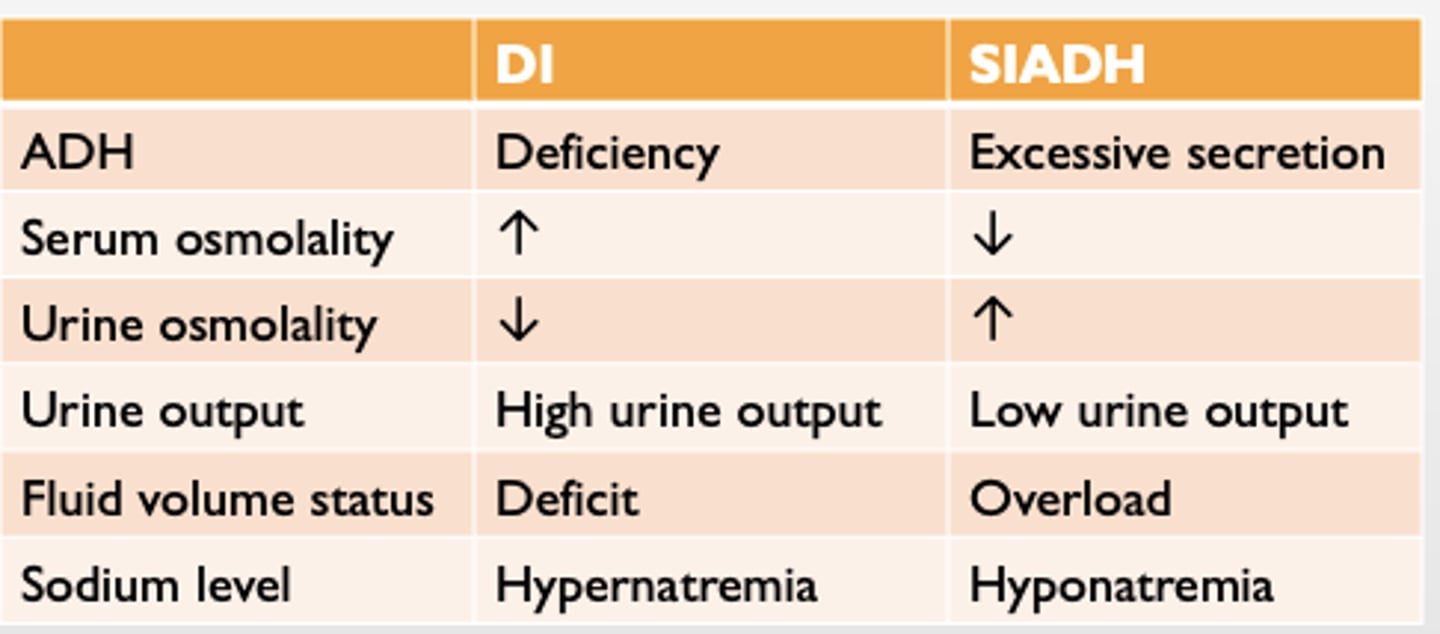
SIADH vs. DI
HYPONATREMIA CM
1. lethargy
2. confusion
3. Decreased reflexes
4. seizures
5. coma
6. respiratory system: shallow breathing
7. rapid HR
8. increased urinary output
*Most life-threatening*:
6. Cerebral edema
7. Increased intracranial pressure
8.sluggish pupils
hypernatremia
-change in MS
-confused
-decreased urine output