Immunity
the immune system’s capacity to protect individuals from disease by recognizing and eliminating potentially pathogenic agents
Immune response and the 2 types
complex series of physiological events that culminates in the destruction and elimination of these substances.
Non-Specific (innate)
`First defenses against pathogens regardless of the type of pathogen
Specific (adaptive)
Stronger defense against a specific pathogen(s) that takes longer to develop
inappropriate immune response
allergies, autoimmune diseases, rheumatoid arthritis, diabetes mellitus, multiple sclerosis, etc
Pathogen and the 4 types
any organism that has potential to cause disease
includes virus (smallest), bacterium (ex; salmonella or strep), fungi (ex; yeast infection, athletes foot) , parasites (ex; worm, ticks, flee, lice)
Physical and chemical barriers
First line of defense against pathogens. The epithelium has two components:
Skin: Epidermis (outer) layer and dermis (inner) layer
Mucous Membranes:
Continuous barrier with the skin
Viscous mucus (goblet cells): tries to trap pathogens
Acid (lysosomes): tightly regulates pH that allows acids to degrade pathogens
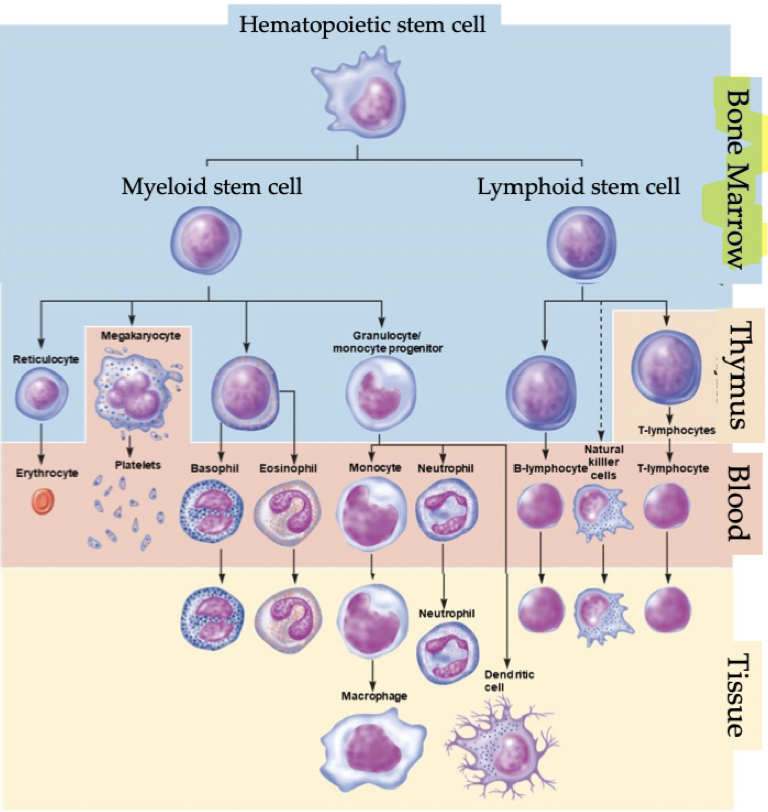
Leukocytes
white blood cells located in the blood stream and in other tissues. They are able to squeeze through pores in capillaries and migrate through tissues. There are 5 types:
The granulocytes: Eosinophils, Neutrophils, Basophils,
The agranulocytes: Monocytes, Lymphocytes
Haematopoiesis
Creation of new blood cells. Process begins with a multi-potential stem cell in the bone marrow of adults (or liver in fetus). Multi-potential stem cell can give rise to any and all blood cells; initial division into either
Myeloid cell creates a common myeloid progenitor (CMP) via Myelopoiesis
Lymphoid cell creates a common lymphoid progenitor (CLP) via Lymphopoiesis
Phagocytes
A type of leukocyte that engulfs foreign particles and microorganisms, thereby removing them from blood and tissue. Referred to as the pacman cell.
Secrete cytokines (cell signaling molecules)
Circulate the blood for 7-10 hours
Migrate to tissues for a few days
Increase in numbers during infections
Includes Neutrophils, Monocytes, Macrophages, Dendritic Cells, Eosinophils
Lymphocytes
type of leukocyte that provides the immune system with diversity, specificity, memory, and the ability to distinguish between self and non-self
Lymphocytes account for 20-40% of leukocytes. Leukocytes account for 99% of interstitial fluid cells.
Includes B-Lymphocytes (B-Cells), T-Lymphocytes (T-Cells), Null Cells (Natural Killer Cells)
Lymphatic system
Central lymphoid tissue (primary): Site of lymphocyte production and maturation
In adults: bone marrow, thymus
In fetus: liver
Peripheral lymphoid tissues (secondary): Site of initiation of the adaptive immune response
Primary: lymph nodes, spleen
Secondary: Mucosae or mucosal-associated lymphoid tissues (MALTs)
Peyer's patch in the small intestine, tonsils, adenoids in throat and nose, appendix, lymph nodes
Roles of Peripheral Lymphoid Tissue
Filters bodily fluids
Removes potentially harmful material (pathogens from blood)
Stores leukocytes
Innate (Non-Specific) Immunity
Second line of defense (after physical and chemical barriers), recognize a pathogen but not specifically
Physical Barriers
Inflammation
Interferons
NK Cells
The complement system
Purpose to remove harmful agents, clean up the infection and help repair injured tissue
What is inflammation?
A non-specific rapid response via accumulation of proteins, fluids, and phagocytic cells in an area of tissues that has been injured or invaded by microorganisms
Induced by chemical mediators from invading pathogens, release by damaged cells, release by leukocytes, movement from blood to the infected tissue
Hallmark signs of inflammation: Heat, Pain, Redness and Swelling
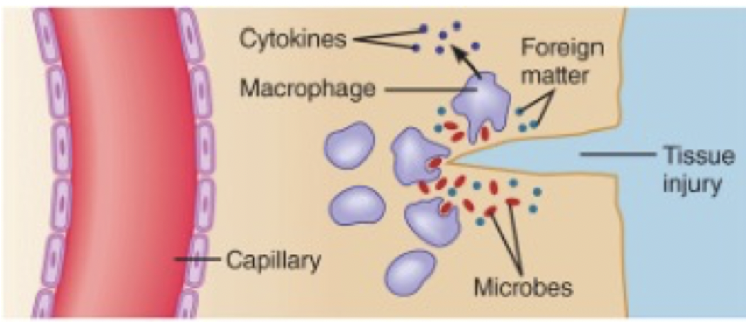
Steps of inflammation
Nearby macrophages engulf the debris and foreign matter
Nearby capillaries dilate and become more permeable to proteins and fluid
Foreign matter is contained
Additional Leukocytes migrate into the region
Recruited leukocytes continue to help clear the infection; phagocytosis
Step 1 of inflammation: Macrophages engulf foreign material
Macrophages are phagocytes that perform phagocytosis aka engulf foreign material.
They have receptors that detect pathogens (PRRs). The receptors grab a hold of bacteria & begin phagocytosis
They then release cytokines; Small signalling protein that signal other immune cells, which causes inflammation
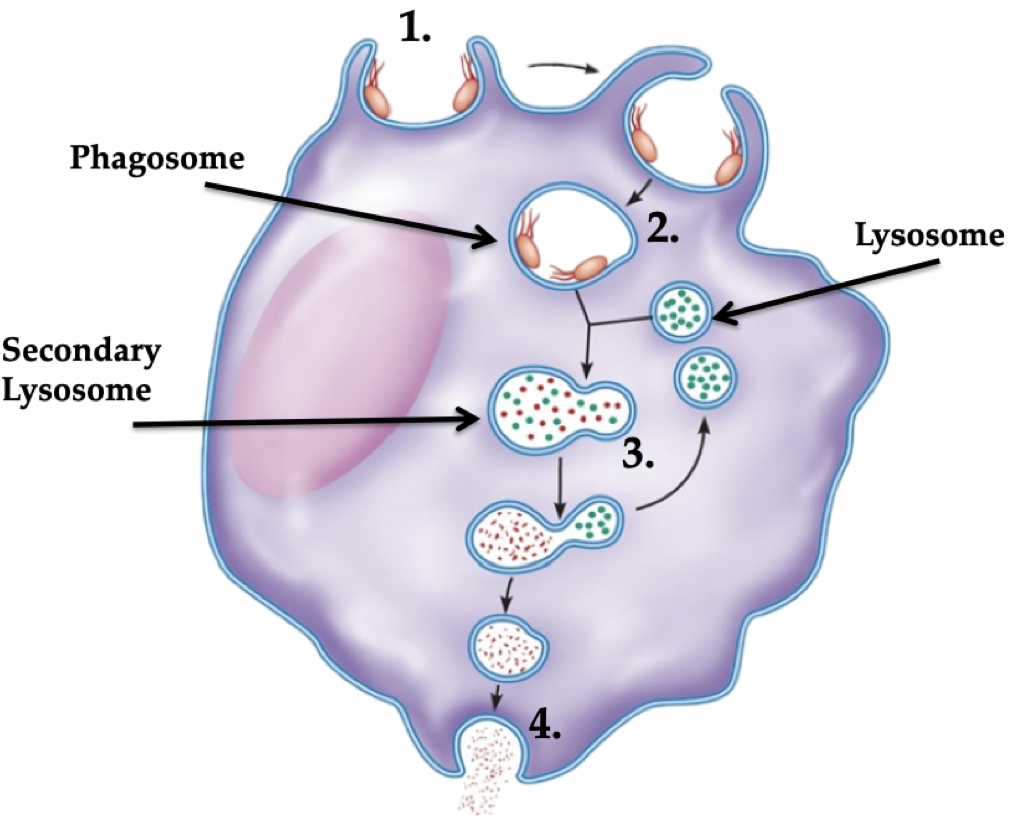
Steps of phagocytosis
Attachment: Bind to rough/irregular cell shapes using PRR receptors (not healthy cells)
Internalization: Fully surround bacteria and bring inside cell. Takes < .01 seconds!
Phagosome: pathogen/foreign material inside a phagocyte
Degradation: Enzymes (lysosomes) breakdown pathogen
Phagosome + lysosome = secondary lysosome
Exocytosis: Eliminates harmless waste
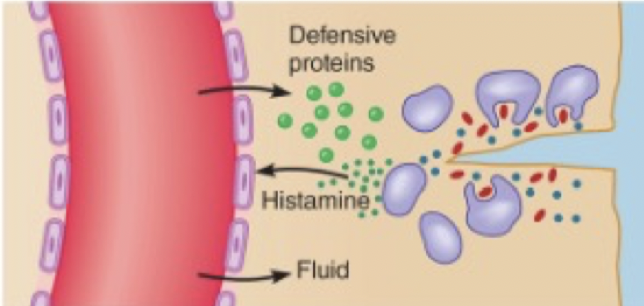
Step 2 of inflammation: Capillaries dilate & become more leaky
Local dilation of blood capillaries by histamine increase blood flow, which leads to warm and red skin
Causes gaps between endothelium cells for increased leakage of blood plasma
More blood flow and leakage leads to edema (swelling)
This causes an increase in pressure on nerves and leads to pain
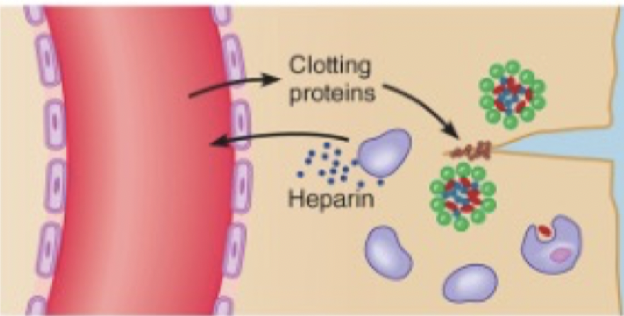
Step 3 of inflammation: Containment of Foreign Material
Need to reduce the spread of foreign material. Clotting factors are released from the blood and form a clot around bacteria
Heparin keeps area from clotting for a short period of time allowing entry of leukocytes
Step 4 of inflammation: Leukocyte Migration and Proliferation
Leukocytes (reinforcements) migrate to injury site. Other phagocytes that join the clean up effort
Bone marrow increases production of leukocytes because more are leaving to the site of injury
Adaptive (Specific) Immunity
Specificity, diversity, memory, self-tolerance. Specialized response initiated by an infection. Takes days to weeks after exposure to develop. Able to recognize specific pathogens and able to remember previous pathogens.
Humoral Immunity
Cell-Mediated Immunity
How do B and T cells identify pathogens?
Detect molecules called antigens: Unique proteins on foreign/damaged cells, like a fingerprint.
Antigens bind to antigen binding sites on lymphocytes that have specific shapes only!
What happens when antigens bind to T lymphocytes?
CD4 T cells help (ENHANCE activity) other cells by secreting Cytokines (helper T cells)
CD8 T cells kill the bad cell; a license to kill (cytotoxic T cells)
What happens when antigens bind to B lymphocytes?
B cells can develop into …
plasma cells known as antibody-synthesizing factory and release antibodies into circulation
Memory cells where antibodies bind to antigens, marking them for destruction
Antibodies + 3 roles
Released by B lymphocytes into circulation. Antibodies bind to antigens in circulation, marking them for destruction. 3 roles:
Neutralize/block antigen (pathogen) activity
Clump pathogens into a big group (easier to clean up)
Enhance the activity of macrophages and other immune cells
Memory B and T cells
When activated by an antigen, B and T lymphocytes can create ‘clones’ called Memory B or T cells. If that same pathogen comes back, the body will be ready to quickly fight it off
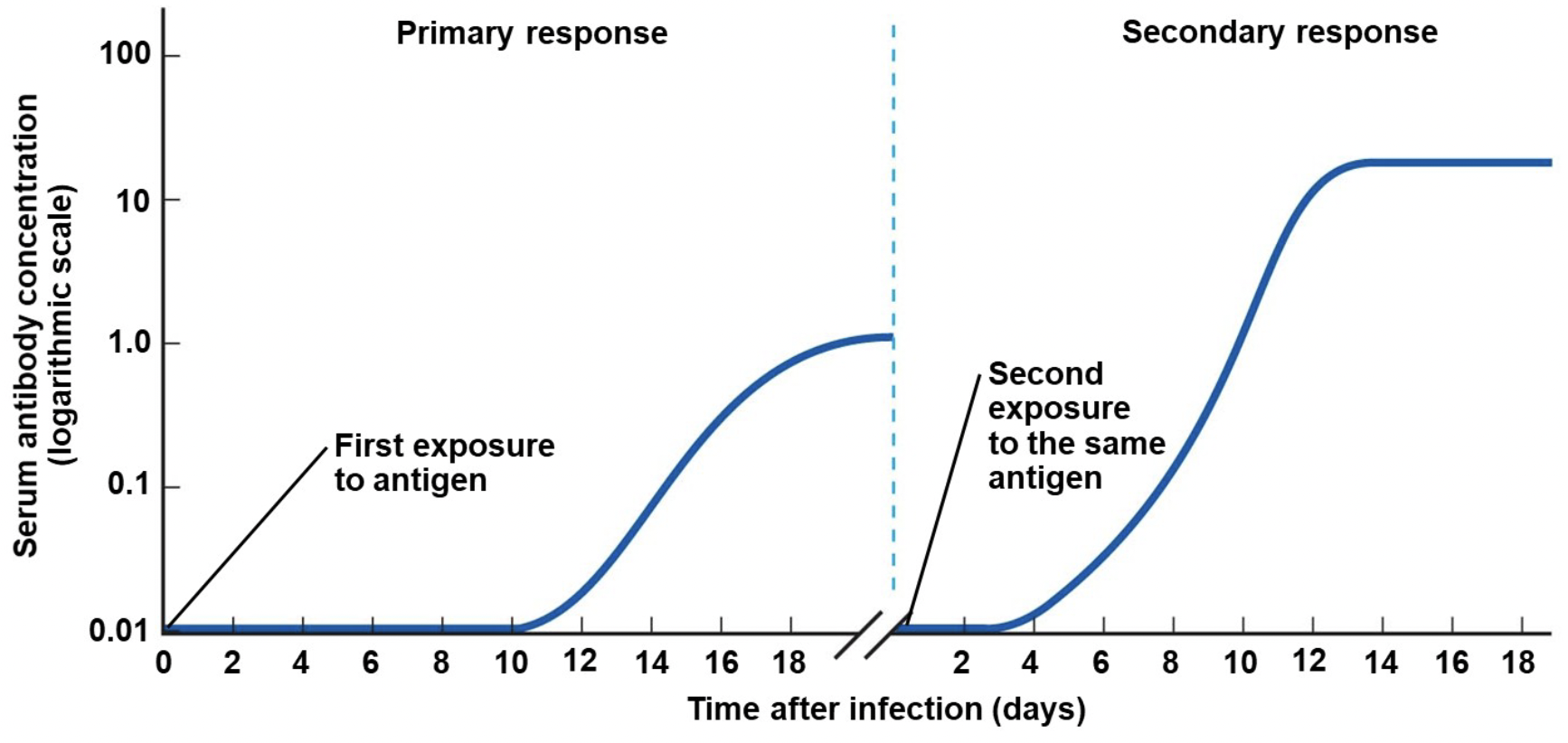
Primary vs secondary response
Primary response: first exposure to antigen
Secondary response: second exposure to the same antigen
Can take quite a long time to begin to make antibodies after first exposure (10-17 days), and you feel sick
After second exposure it only takes 2-7 days to fight off sickness
Vaccinations creation
Created by Edward Jenner with the invention of the smallpox vaccine in 1796-1798. He noticed that milkmaids that had been ill with cowpox appeared to be immune to smallpox. Cowpox is a similar, but far less aggressive version of smallpox. He predicted that deliberate inoculation with cowpox would protect people against smallpox.
Vaccination/immunization
Introduction of a safe form of a microorganism or a collection of its components (inoculum) that are not expected to cause disease into the body. Exposure to an antigen causes a slow, weak primary immune response and induces immunological memory.
Lymphocytes detect antigen and we start building immunity
When natural exposure occurs after vaccination, there is a fast and strong secondary immune response
Herd immunity
If a large portion of the population is vaccinated (protected), the rate of disease transmission is likely to be significantly lower than not protected
What are allergies
aka hypersensitivity reactions; Exaggerated immune response to environmental antigens called allergens
Pollen, dust, pet dander, types of food, bees, etc.
Some responses are more serious than others...
Life threatening = anaphylactic shock (widespread degranulation of mast cells causes bp to drop)
In low-grade reactions the main issue is usually vasodilation and capillary permeability
How does the immune system cause allergies
Excess production of specific antibodies by B cells, which bind to leukocytes (mast cells), which triggers degranulation
the release of histamine induces inflammation
anti-histamines prevent histamine from having the effect it normally has
Autoimmune disorders
An important feature of a healthy immune system is “self-tolerance”; Ability to recognize OWN cells vs. FOREIGN cells
This feature is dysfunctional in autoimmune disorders. Immune cells attack specific cells of the body
Multiple sclerosis
Immune system (T cell lymphocytes) attacks the myelin sheath on nerves of the central nervous system, so nerve Impulses traveling along nerves are interrupted or distorted.
Symptoms:
Impaired Vision
Sensory Problems
Weakness in Limbs
Loss of Coordination
Speech Problems
Short Term Memory Loss
Fatigue
What is a possible explanation for multiple sclerosis?
Only specialized T cells are allowed in the brain and the blood-brain barrier controls T cell entry. An infection may change blood-brain barrier function and allows non-specialized T cells to enter brain tissue and attack myelin
Evidence: activated cytotoxic T cells are found in the cerebral spinal fluid of people with MS that are not found in healthy adults
Type 1 diabetes
Destruction of insulin-producing beta cells in pancreas leads to a lack of insulin which causes a whole plethora of problems.
People with T1D must regularly take insulin and regularly monitor their blood glucose.
What is a possible explanation for type 1 diabetes?
T cells wrongfully attack beta cells of the pancreas and destruction of beta cells = no more insulin.
Cause is not known but people with a certain type of major histocompatibility complex receptor (MHC) are prone to type 1 diabetes.
Normally, T cells identify antigens using MHCs type of receptor. Every cell in the body has an MHC and they tell T cells if the cell is a “Friend or Foe”. When a cell is infected, the MHC presents the antigen, telling the T cell “foe”. In type 1 diabetes, beta cells display a ‘friend’ MHC, but T cells misread it and break the cell down.
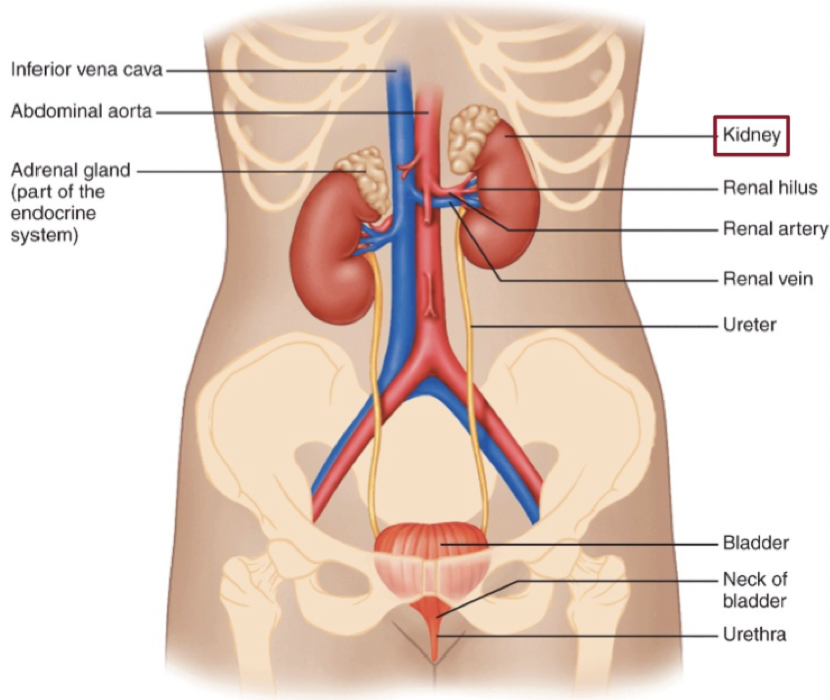
Anatomy of the renal system
We have two kidneys and two ureters, one bladder, one urethra
urethera is how we excrete
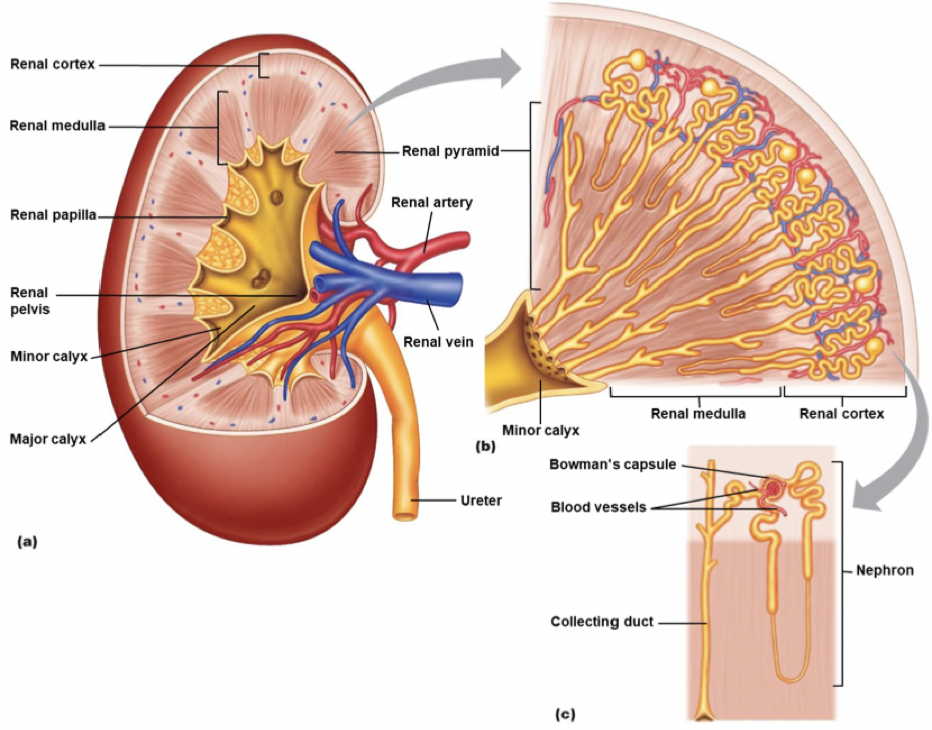
Anatomy of the kidney
Outer edge is renal cortex
Striated section is renal pyramids; part of medulla
Nephrons are the yellow pieces
Blue is veins
Red is arteries
Nephrons include blood vessels and bowmans capsule which make renal corpuscal
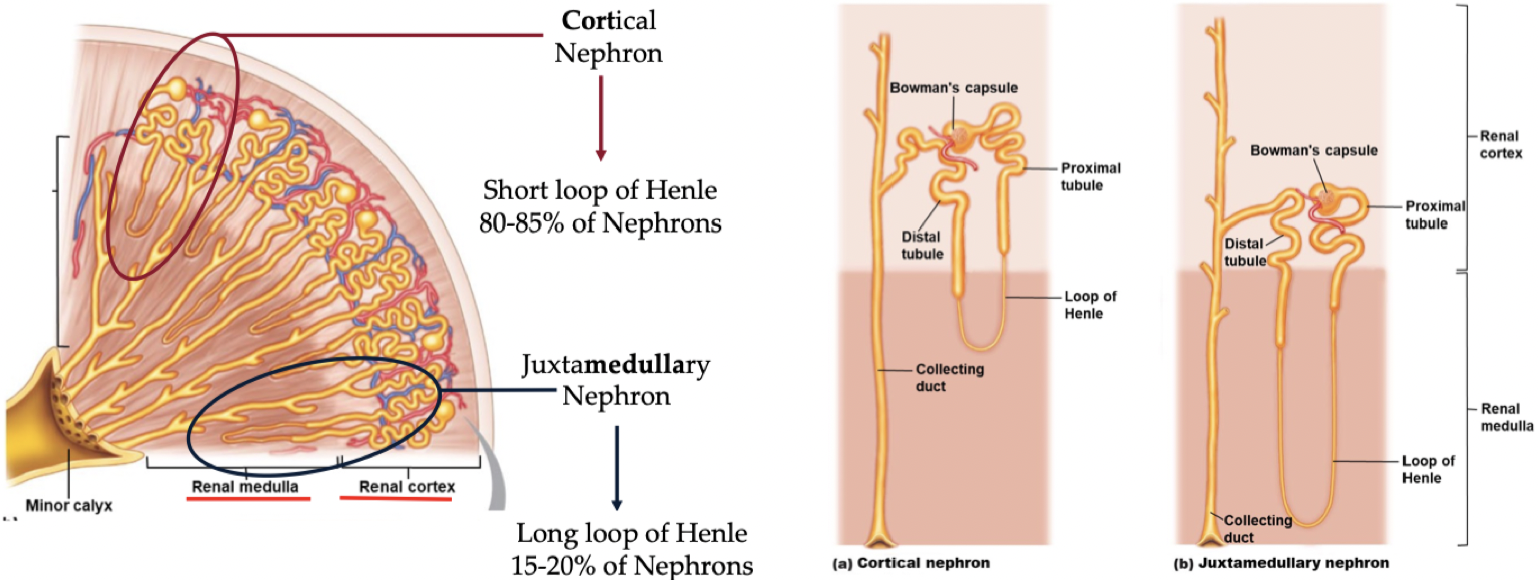
Types of nephrons
Juxtamedullary nephrons have a longer lop of henle that descend farther
Cortical nephrons are more common and have a short loop of henle
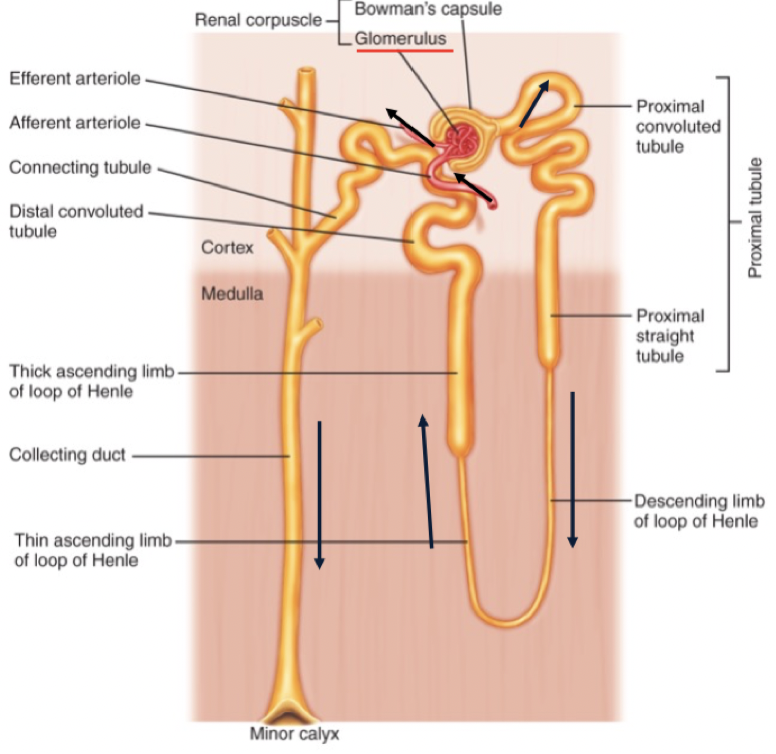
Juxtaglomerular Apparatus
Renal corpuscle/juxtaglomerular apparatus has two components; glomerulus and bowman’s capsule
Blood flows into kidney through arteries
Afferent artery delivers blood to Bowmans capsule
Filtrate; once it moves from the blood into the Bowmans capsule
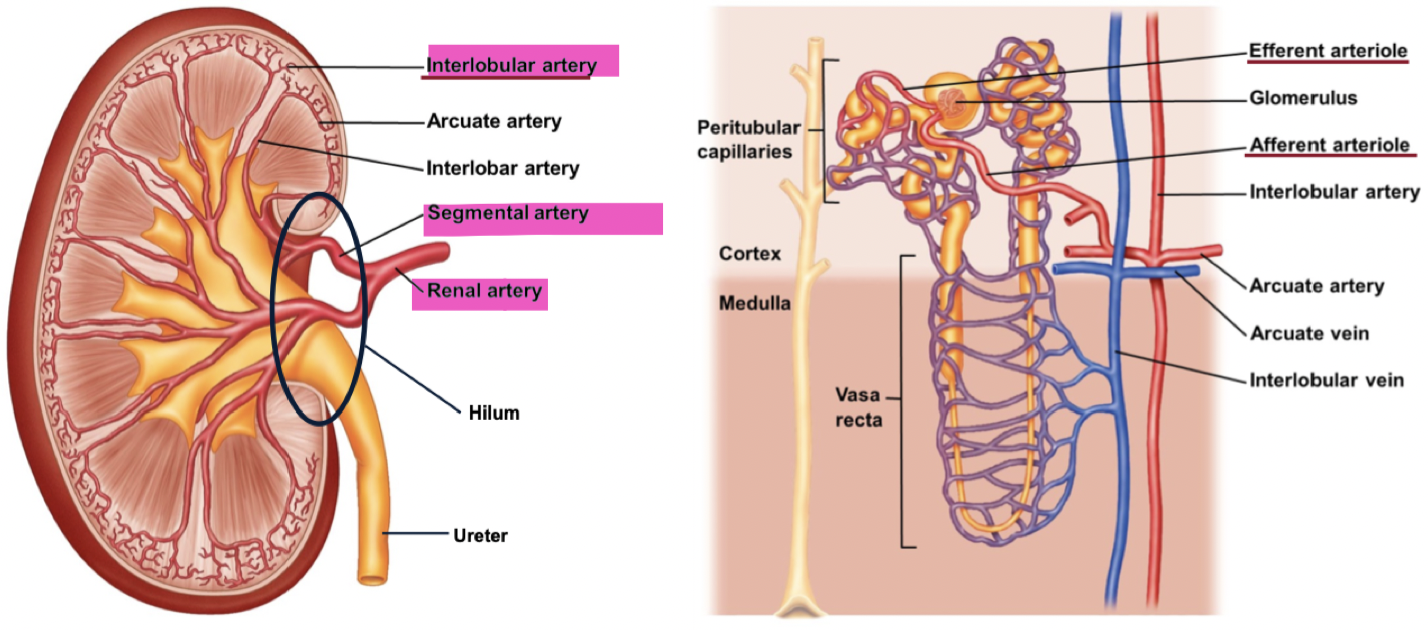
Blood supply to kidneys
Renal artery splits into segmental arteries, then interlobular arteries
Afferent arteriole brings blood to the glomerulus and the efferent arteriole carries blood away from the glomerulus
Peritubular capillary wrap around tubules
Increases surface area when they are wrapped around each other
Absorption and filtration allows us to stay at homeostasis
Blood enters through renal artery and comes out through the renal vein
Renal processes
Filtration: Removal of H2O, ions and molecules from the blood into the kidney filtrate
Tubular Reabsorption: Uptake of H2O, ions and molecules from the kidney filtrate back into the blood
Tubular Secretion and continued Reabsorption: Selective removal of substances from the blood into the kidney filtrate and the uptake of H20 from the kidney filtrate into the blood
Excretion: Elimination of solute and water from the body in the form of urine
Rate of excretion equation
Rate of Excretion = Filtration + Secretion - Reabsorption
Renal corpuscule
2 Major Components:
Glomerulus – blood supply, fed by afferent arteriole
Filters 20% of plasma volume that passes through
Bundled vessels increase surface area
Unfiltered blood leaves via efferent arteriole
Bowman’s Capsule – filtrate accepter
nutrients, vitamins, chemicals, and waste can cross the membrane to filter
proteins and cells can not
High pressure in glomerulus drives contents from the blood to Bowman’s capsule
Move from HIGH to LOW pressure
Passive process
Tubular Reabsorption
filtered solutes and water moving from the tubules into the plasma. Occurs in the proximal convoluted tubule (mass absorber) following filtration into Bowmans.
Highly permeable tubule
Important molecules are reabsorbed back into blood (glucose, vitamins, amino acids, H2O, bicarbonate, K+)
Not well regulated
~70% of sodium and water in filtrate reabsorbe
Reabsorption occurs via diffusion and active transport
What are the reasons the proximal convoluted tubule has such high reabsorption?
Brush Border: Finger like projections increases surface area (increases conductance) in proximal convoluted tubule
Lots of Mitochondria: Make ATP for energy for lots of active transport
“Leaky” Epithelium: Allows molecules to flow across the membrane (no tight junctions)
Peritubular capillaries
capillary that wraps around the proximal distal tubule and reabsorb H2O and molecules that diffuse out of proximal convoluted tubule
Descending loop of Henle
Only permeable to H2O, so large amounts of H2O leave filtrate when osmotic gradient exists. No Na+, K+, Cl-, transport.
No transporter in the body for H2O
H2O moves down it’s osmotic gradient; high [H2O] to low [H2O]
Gradient created by the movement of solute (Na+, Cl-) from Ascending Loop of Henle into the Vasa Recta
Amount of solute transported is directly proportional to the amount H2O reabsorption
Ascending Loop of Henle
Impermeable to H2O. Actively pumps Na+, K+, Cl-, (co-transport) out of filtrate
Vasa recta
A capillary wrapping around the loop of henle that reabsorbs H2O, Na+ and Cl-
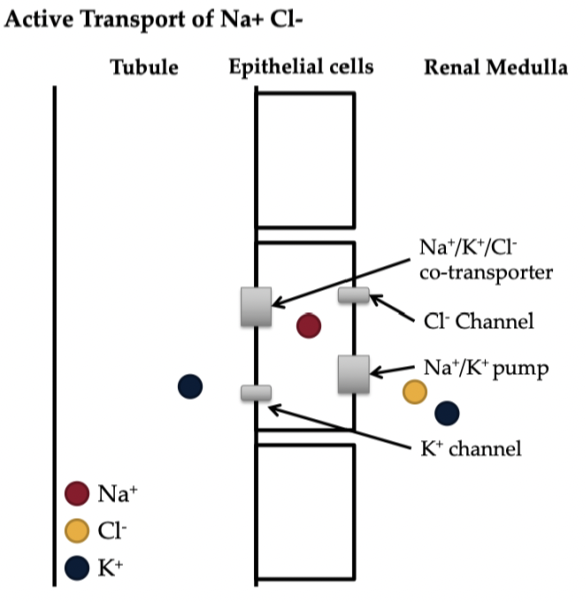
Active transport of Na+ Cl- from the ascending limb
Na+/K+/Cl- co-transporter moves ions out of tubule into epithelial cells
K+ diffuses through K+ channel back into tubule
Cl- diffuses into interstitial space through Cl- channel
Na+ pumped out of epithelial cells via Na +/K + pump
in total, more Na+ moves across epithelial cells than K+ creating an osmotic gradient
Distal convoluted tubule
Substances are secreted into the tubule from the blood via diffusion and active transport
Urea, ammonia, H+, K+, foreign substances (i.e. drugs)
Collecting ducts
as the remaining filtrate passes through the collecting ducts, H2O is reabsorbed
antidiuretic hormone
Collecting ducts reabsorb water only in response to antidiuretic hormone (ADH).
ADH is released by pituitary gland when water needs to be reabsorbed (i.e. sweating, low water intake, low blood pressure, etc.)
ADH release inhibited when water needs to be excreted (i.e. after drinking a big glass of water, high blood pressure)
ADH process
ADH stimulates receptor on collecting duct
ADH travels in the blood and moves to the interstitial space when it reaches the collecting duct and stimulates receptors on the outside wall of collecting duct
Causes aquaporin-2 to be present on cell wall of inside of collecting duct
Aquaporin-2 allows water to diffuse down its osmotic gradient
Increases conductance for flow of water from filtrate into the interstitial space then the peritubular capillaries
Excretion
Filtrate is excreted as urine (urination = micturition)
Once the filtrate enters the collecting ducts it drains into the renal pelvis
Renal pelvis to Ureter, then Ureter to Bladder
Wave like contraction of smooth muscle surrounding ureter push the urine down the ureter
Micturition (urine) reflex stimulated when there is fluid buildup in the bladder to create urination
there are smooth muscles (detrusor) for involuntary control and skeletal muscles for voluntary control
Primary purposes of the lung
Allow oxygen (O2) to diffuse into blood
needed for ATP synthase
Allow carbon dioxide (CO2) to diffuse out of blood
buildup of CO2 is toxic
External respiration
Pulmonary ventilation
Exchange of O2 and CO2 between lungs and blood
Transport of O2 and CO2 to the tissues
Exchange of O2 and CO2 between blood and tissues
Upper airway and respiratory tract
Begins at mouth and nose, makes its way through system (epiglottis, glottis, trachea, larynx) and ends at alveoli where gas exchange occurs. Two distinct zones:
Conducting Zone
Respiratory Zone
terminal bronchial
once the broncials becomes less than 1mm in diameter
The conducting zone
Consists of trachea, branches, and bronchioles. Carries (conducts) air from the mouth/nose into the lungs. Trachea branches and bronchioles enter lungs.
Contains ‘dead space’ air where no gas exchange occurs. Until a breath is larger than 150mL in volume, no gas exchange occurs.
The respiratory zone
Active/functional portion of the lung, where gas exchange actually occurs. Bronchioles branch into individual respiratory units. Alveoli are where gas exchange takes place.
Alveoli
functional unit of the respiratory zone. There are ~300 million alveoli in the lungs. Total surface area of ~100 000 cm^2.
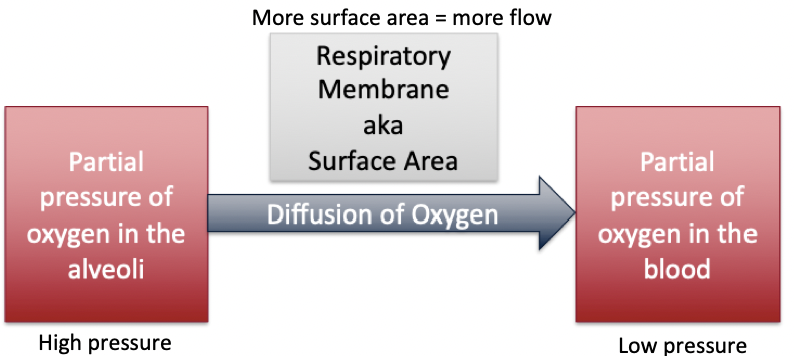
Respiratory membrane
Alveoli are open sacs, surrounded by capillaries. Almost 1000 km of capillary are laid over the alveoli. Huge surface area for gas exchange = huge conductance for diffusion of O2 and CO2
0.2 μm thick
↑↑ conductance for gas exchange
Trachea anatomy
2.5 cm in diameter, 10 cm in length, Total surface area of ~78 cm
Chronic Obstructive Pulmonary Disease
Inflammation of alveoli and a mucous build up causes a permanent destruction of alveolar walls, which severely reduces capacity for gas exchange in alveoli'.
Thoracic cavity
Includes two main components:
Chest Wall: Includes rib cage, sternum, thoracic vertebrae, connective tissue, intercostal muscles. Airtight sealed system which protects the lungs.
Diaphragm: Divides thoracic cavity and abdominal cavity. Primary inspiratory muscle.
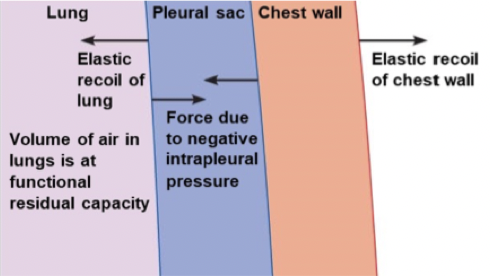
Pleura
Intrapleural space maintains negative pressure between the lung and chest wall, which keeps the lung expanded and allows them to stay connected. Each lung is surrounded by a separate pleural sac.
As the chest wall or lung moves, they move together. At rest there is elastic recoil pulling chest wall in one direction and elastic recoil pulling lung in the other direction.
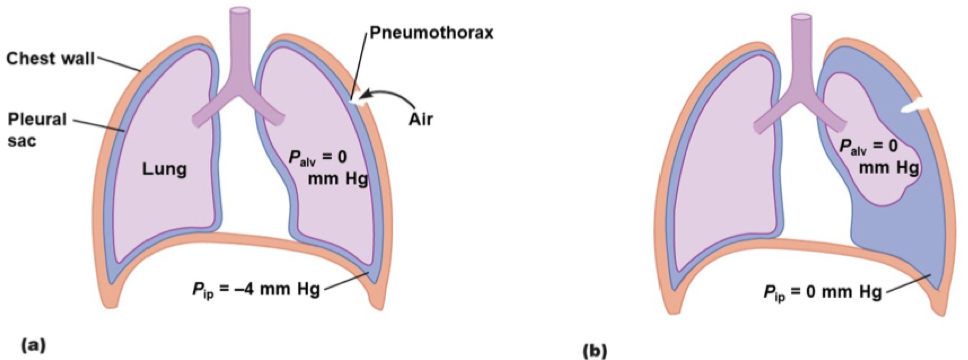
Pneumothorax
Lung collapse. Occurs when the pleural sac is punctured. The negative pressure is filled with air and the connection between lung and chest wall no longer exists, so the lung pulls away from chest wall
Each lung is separate in this case; only one can collapse and the other can be fine because lungs are individually wrapped in their own pleural sac.
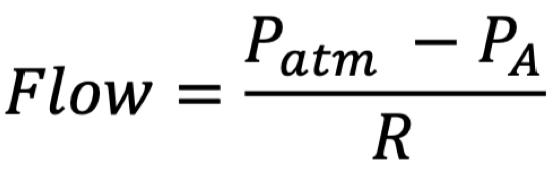
Flow of breathing mechanisms
Phi: Atmospheric Pressure = Patm
Remains relatively constant at ~760 mmHg
Plo: Alveolar Pressure = PA
Change in pressure here affects gradient for flow
Amount of pressure in alveoli; we can actively change this through respiration
Resistance = R
Depends on airway radius
Opposite of conductance
Generally very constant
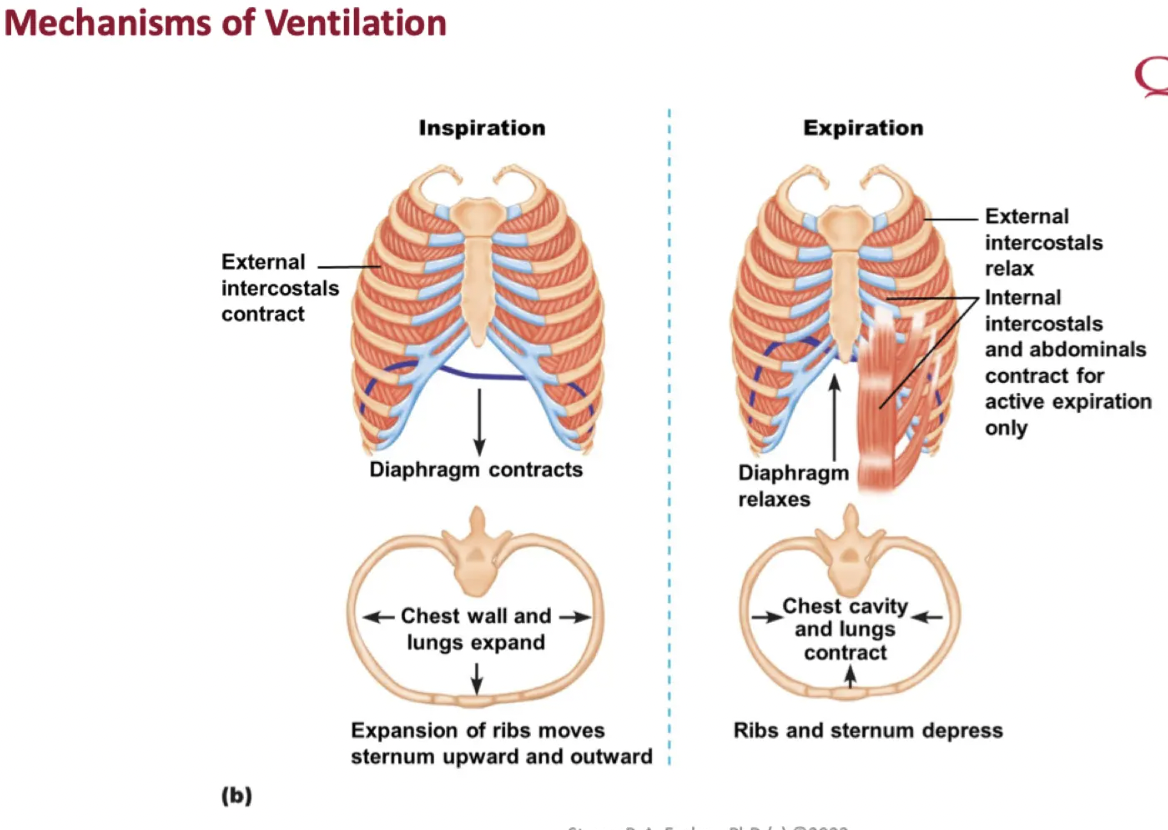
Inspiration vs expiration
Inspiration: lungs expand during inspiration
PA decreases
△P drives air into the lungs
Alveolar volume increase
Expansion creates a negative pressure: alveolar pressure becomes more negative which increases flow into the lungs
We are subtracting a more negative number so flow increases
Expiration: Lungs recoil during expiration
PA increases
△P drives air out of the lungs
Alveolar volume decreases
Passive vs active expiration
At resting level, there is passive expiration which is simply relaxation of the muscles
Active expiration is 'forced' intentional expiration
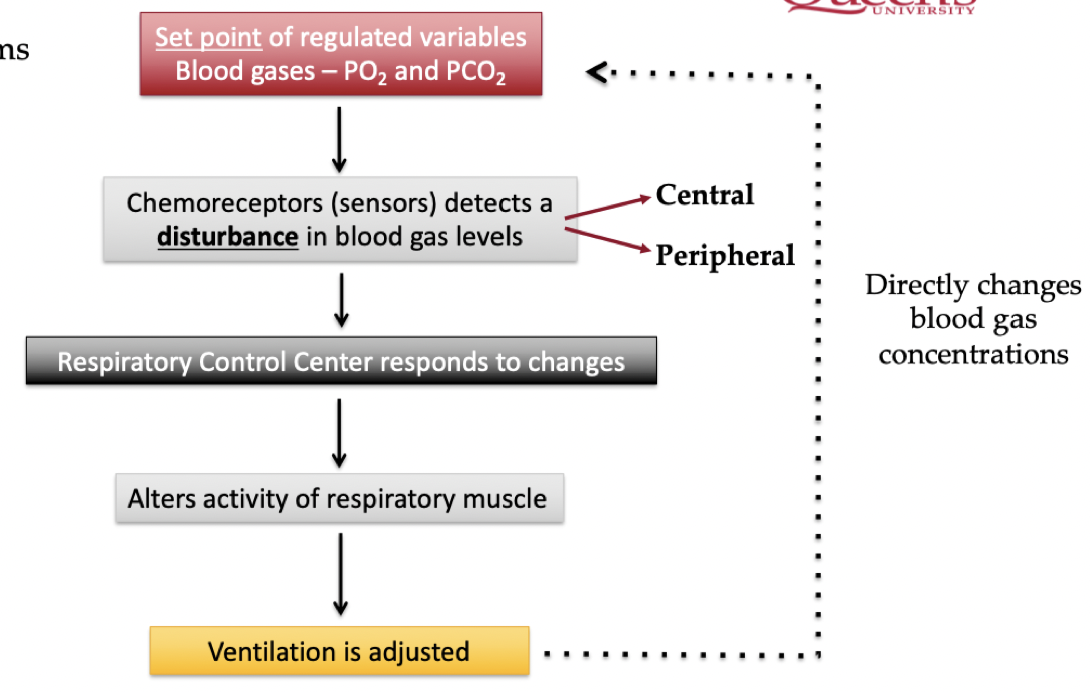
Neural control of ventilation
There is both voluntary and involuntary control of breathing
Feedback Control System: ventilation is adjusted in order to maintain concentrations of blood gases (O2 and CO2)
Feedback Controller (Integrator): respiratory control center in medulla of brain stem. Adjusts firing rate of α-motor neurons of respiratory muscles, which impacts the diaphragm and intercostal muscles.
Which motor nerves are connected to the respiratory center?
Phrenic Nerve: diaphragm muscle
External IC Nerve: external intercostal muscles
Internal IC Nerve: internal IC muscles
Motor nerve stimulates muscles
Respiratory muscles are skeletal muscles
Flow of gas exchange
Gas exchange = (Phi x Plo) x K
More oxygen brought into the lungs = higher drive for diffusion flow
CO2 moves the opposite direction as O2 (blood to alveolar space)
Conductance for flow into blood is respiratory membrane (constant; not increasing or decreasing)
Diffusion of gas is determined by pressure gradients
Gas solubility
O2 has low solubility in water
Partial pressure is not necessarily about the number of molecules, it is about the dispersion and solubility
Hemoglobin
Because of the low O2 solubility in the blood, hemoglobin (Hb) is used to transport O2. 98.5% of all oxygen is transported in the blood by hemoglobin.
Hemoglobin has heme (iron containing group) and globin (4 polypeptide groups). Oxygen binds to the heme group.
Because Oxygen is bound to the heme groups, there is a reduced partial pressure of dissolved O2 in the blood, which maintains gradient for diffusion of new oxygen.
No O2 bound to hemoglobin = Deoxyhemoglobin
O2 Bound to hemoglobin = Oxyhemoglobin
Factors affecting diffusive conductance
Thickness of barrier: single cell separates air and blood
Surface area: 1000km of capillaries laid of 100,000 cm2 of alveoli. Larger surface area = more diffusion.
Ability of gas to diffuse: O2 and CO2 = fat soluble, therefore easily diffuse across a membrane
atmospheric partial pressures of gases
PO2 = ~21% x 760 mmHg (sea level atm pressure)
160 mmHg
PCO2 = ~0.03% x 760 mmHg
= 0.23 mmHg
PN2 = ~79% x 760 mmHg
= 600 mmHg
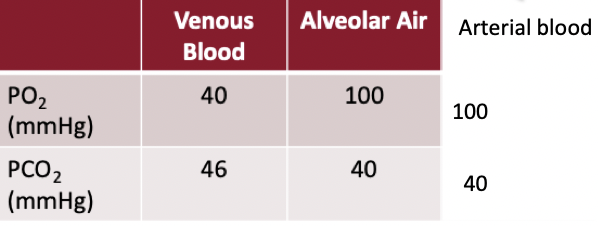
Partial pressures of different gases in different body parts
With ventilation we don’t get 100% turnover of the air from the atmosphere in the lungs
100mmHg oxygen is leftover in lungs after all factors
Diffusion drives oxygen into the cell because there's less oxygen in the cell than in the blood
Once oxygen enters the cell partial pressure of oxygen decreases and carbon dioxide increases
Partial pressure of oxygen throughout the body is changing and this drives flows
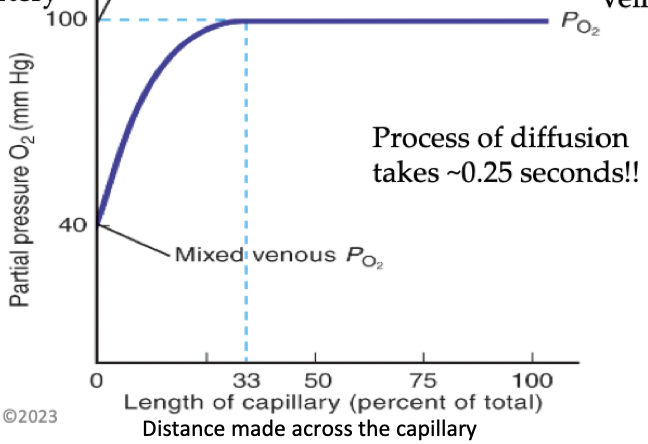
Flow of O2 along the capillaries
O2 diffuses from alveoli to blood
Doesn’t take entire capillary length to do the diffusion
Less and less diffusion as you move across the capillary
Gradient decreases so diffusion rate decreases
P1 in alveoli is higher than P2 in pulmonary capillaries, drives flow
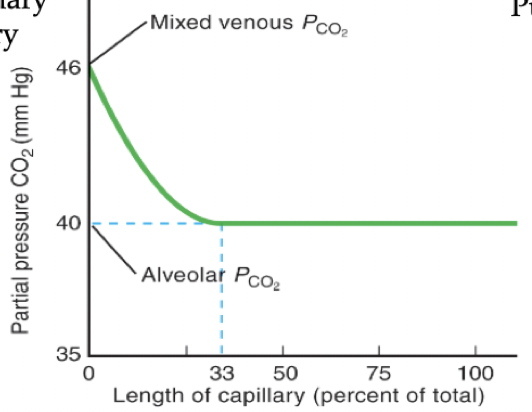
Flow for CO2 along the capillaries
We start with high CO2 and offload it so it decreases
CO2 diffuses from blood to alveoli
P1 in pulmonary capillary is higher than P2 in alveoli drives flow
Peripheral chemoreceptors
Found in carotid bodies and aortic arch. Direct contact with blood. Sensitive to changes in PO2, PCO2 (indirectly), pH (H+). Afferent feedback sent to medullary respiratory control center, which stimulates changes in ventilation.
Central chemoreceptors
Located in the medulla oblongata (part of the brain). Not in direct contact with blood, it is separated by the blood brain barrier. Respond to changes in pH of the cerebral spinal fluid (CSF).
They are H+ sensitive, but H+ does not occur in the blood brain barrier. CO2 does cross the blood-brain barrier, but does not stimulate chemoreceptors.
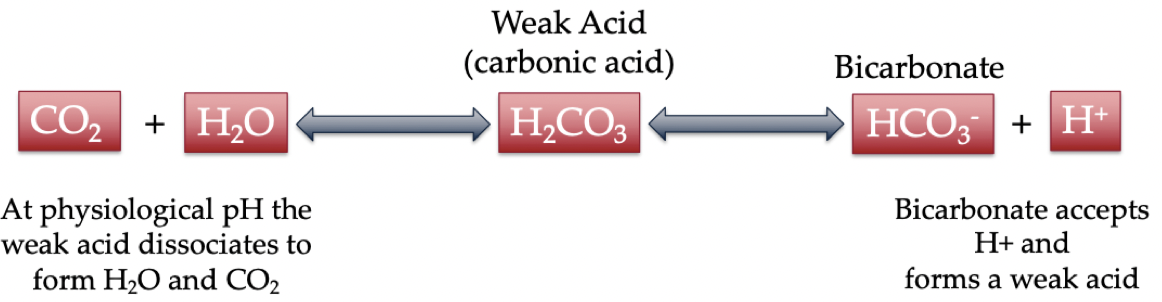
Bicarbonate buffering
Maintains blood pH by allowing central chemoreceptors to sense the blood pH.
The more CO2 that enters, the more hydrogen that is produced, which is sensed
This is a near-equilibrium reaction so can occur in both directions, increased H+ results in increased CO2 and increased CO2 results in increased H+
Control of ventilation feedback mechanism
When oxygen drops, ventilation is increased
increasing ventilation increases alveolar PO2, which increases ∆P for O2 into the blood
When CO2 rises, ventilation is increased
Increasing ventilation decreases alveolar PCO2, this increases the ΔP for CO2 diffusion out of the blood
Important terminologies for ventilation rate
Minute Ventilation: VE in L/min (liters per minute)
Tidal Volume: VT in L (volume per breath)
Breathing Frequency: fB in breaths/min
VE = VT x fB
Alveolar Ventilation = (Tidal Volume – Dead Space) x breath frequency
Components of the cardiovascular system
Heart (Cardiac muscle): Acts as a high pressure pump which allows blood to flow down Pressure Gradient (ΔP)
Vascular System:
Arteries – O2 & nutrient rich - blood flows away from heart to the body
Veins - O2 & nutrient poor (waste rich) - blood flows to heart after it goes throughout the body to be reoxygenated
Order of blood flow in the heart
Blood enters the heart through the inferior and superior vena cava
Then continues into right atrium, travels through right AV tricuspid valve into the right ventricle
From the right ventricle blood moves through the semilunar valve, into the pulmonary artery
Pulmonary artery brings oxygen/nutrient poor blood to the lungs to be oxygenated and have gas exchange
After the lungs, blood comes to the heart through pulmonary veins, then enters left atrium, which is then pumped through left AV bicuspid valve into left ventricle
Left ventricle is very strong and creates high pressure gradient to push blood from left ventricle through aortic semilunar valve into aorta, which travels blood throughout the body
Heart
The heart is found in the thoracic cavity. Heart is size of fists and weighs 250-300grams. Heart is surrounded by the pericardium.
Pericardium
membranous sac that surrounds the heart, which lubricates heart to decrease friction among other body parts when the heart pumps.
Pericarditis
condition in which there is inflammation of the pericardium
Blood vessels
Arteries: larger smooth muscle layer to allow for contraction. Bring oxygenated blood away from heart to other body parts
Veins: have valves, bring oxygen/nutrient poor blood back to the heart
Valves allow blood to move against gravity back up to the heart
Order of blood flow in the body
From the left ventricle of the heart, the blood enters the aorta then the arteries
From the arteries there are smaller vessels called arterioles which have a high resistance
Capillaries are sites for blood to exchange nutrients and oxygen with tissues
Venules are small converging vessels
Veins are larger converging vessels
Blood enters the heart at the vena cava
This system is a close loop system; the blood does not leave the body vessels intentionally
Pulmonary arteries vs pulmonary veins
Pulmonary arteries: oxygen poor, but still moves blood away from heart to lungs
Pulmonary vein: oxygen rich but moves blood towards the heart
Blood composition
Blood is 55% plasma; least dense layer
Fluid and solutes that exist in blood
Buffy coat; contains leukocytes and platelettes, only about 1%
Erythrocytes: red blood cells, very important for oxygen and co2 transport, about 45%
Sickle cell anemia
Inherited disease in which blood cells have a reduced capacity to bind oxygen, making it difficult to deliver to the body. Blood cells have a sickle shape.
How does the heart receive blood?
Arteries on the heart called coronary arteries supply blood to the heart to allow it to function and work
Heart attack
When coronary arteries are blocked (usually from plaque build up) a heart attack occurs. Blood can no longer continue through these arteries to supply heart muscles with oxygen and nutrients, the muscles of the heart stop functioning.
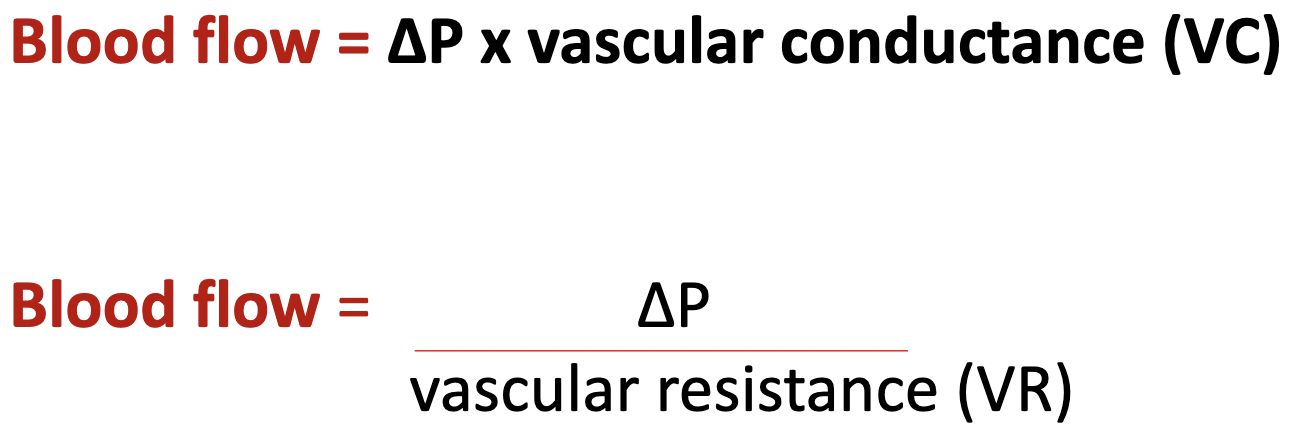
Blood flow flow model
vascular resistance and conductance are opposites
The heart beating/contraction creates the high pressure for inflow for blood into the arteries
the ventricle gets smaller, and blood is pushed out
The arterioles create resistance to blood leaving (outflow) the arteries