DSA04 - Pathology of the Thyroid
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
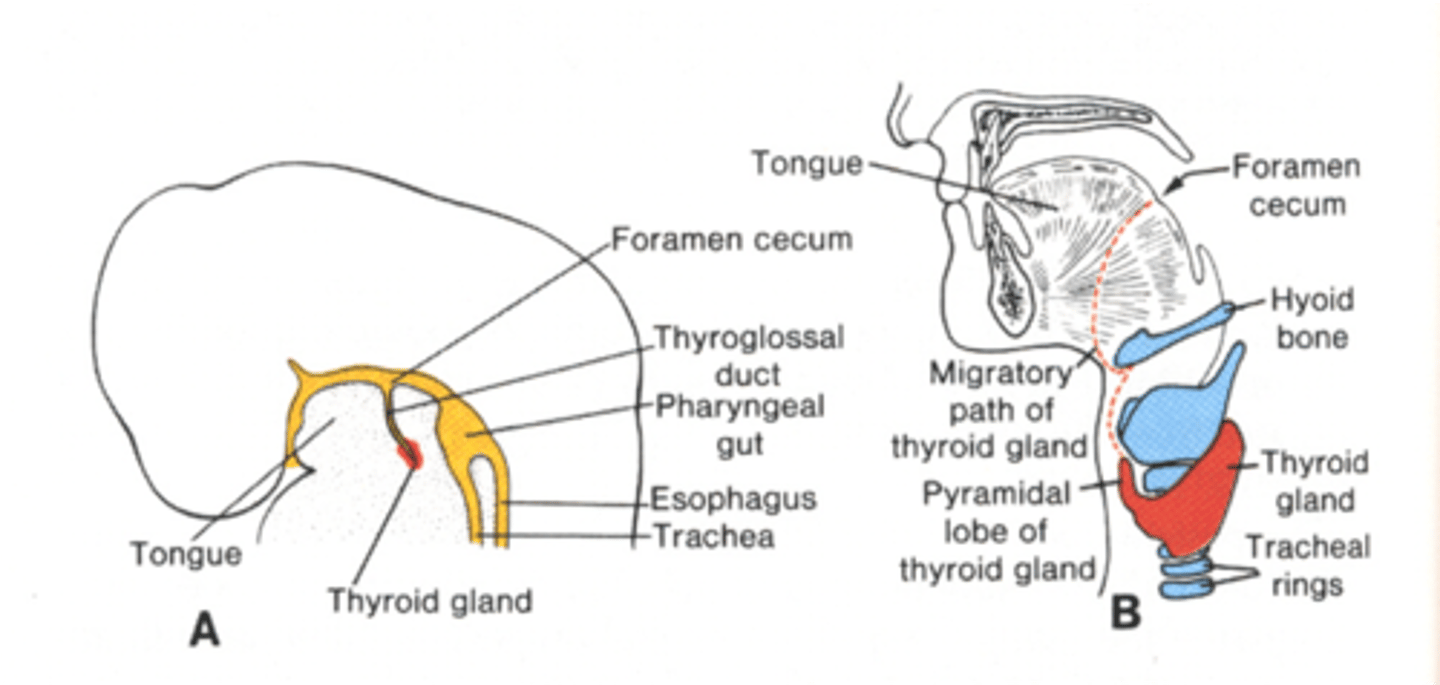
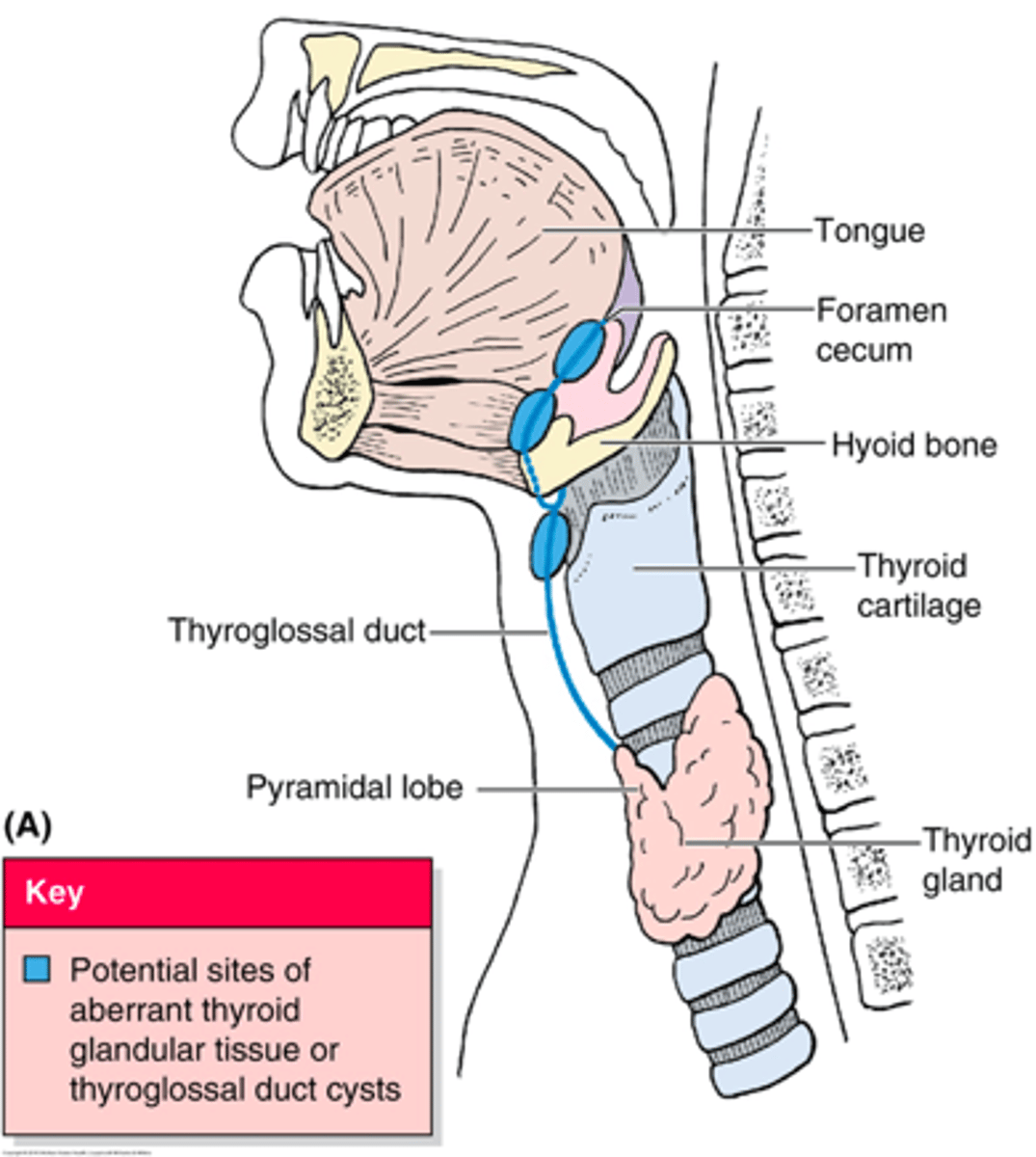
Pyramidal; Persistant remnant of the thyroglossal duct
The () lobe of thyroid is a normal anatomical variant seen in 15-50% of the population. What does it represent?

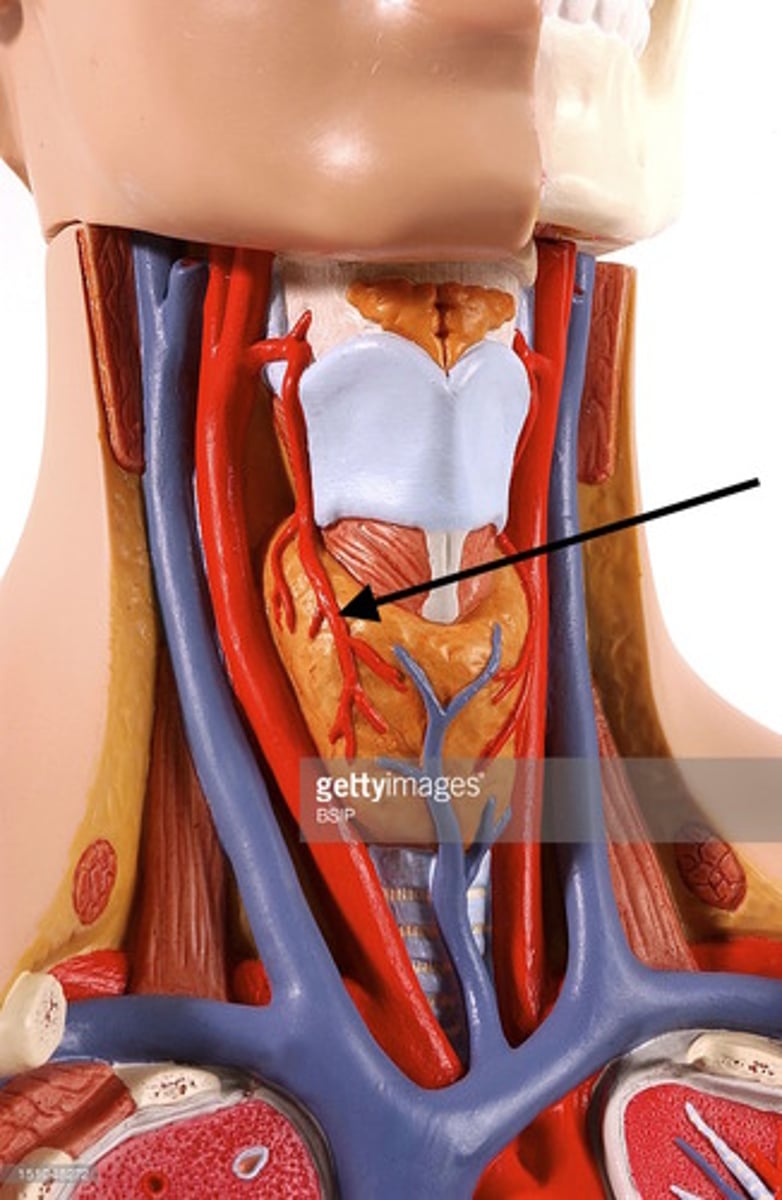
External Carotid
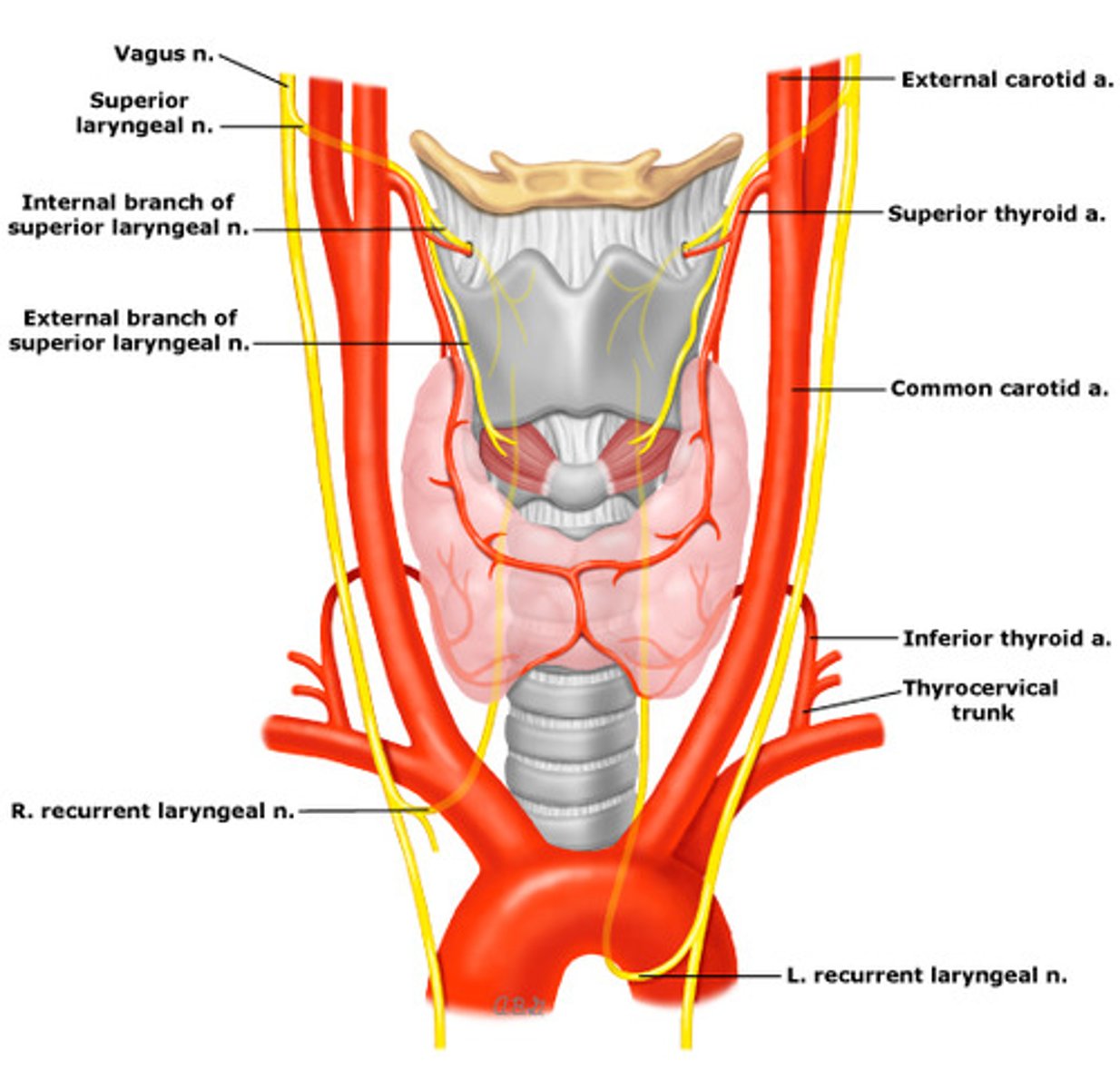
The Superior part of the thyroid is supplied by the Superior Thyroid Artery - what is this a branch of?
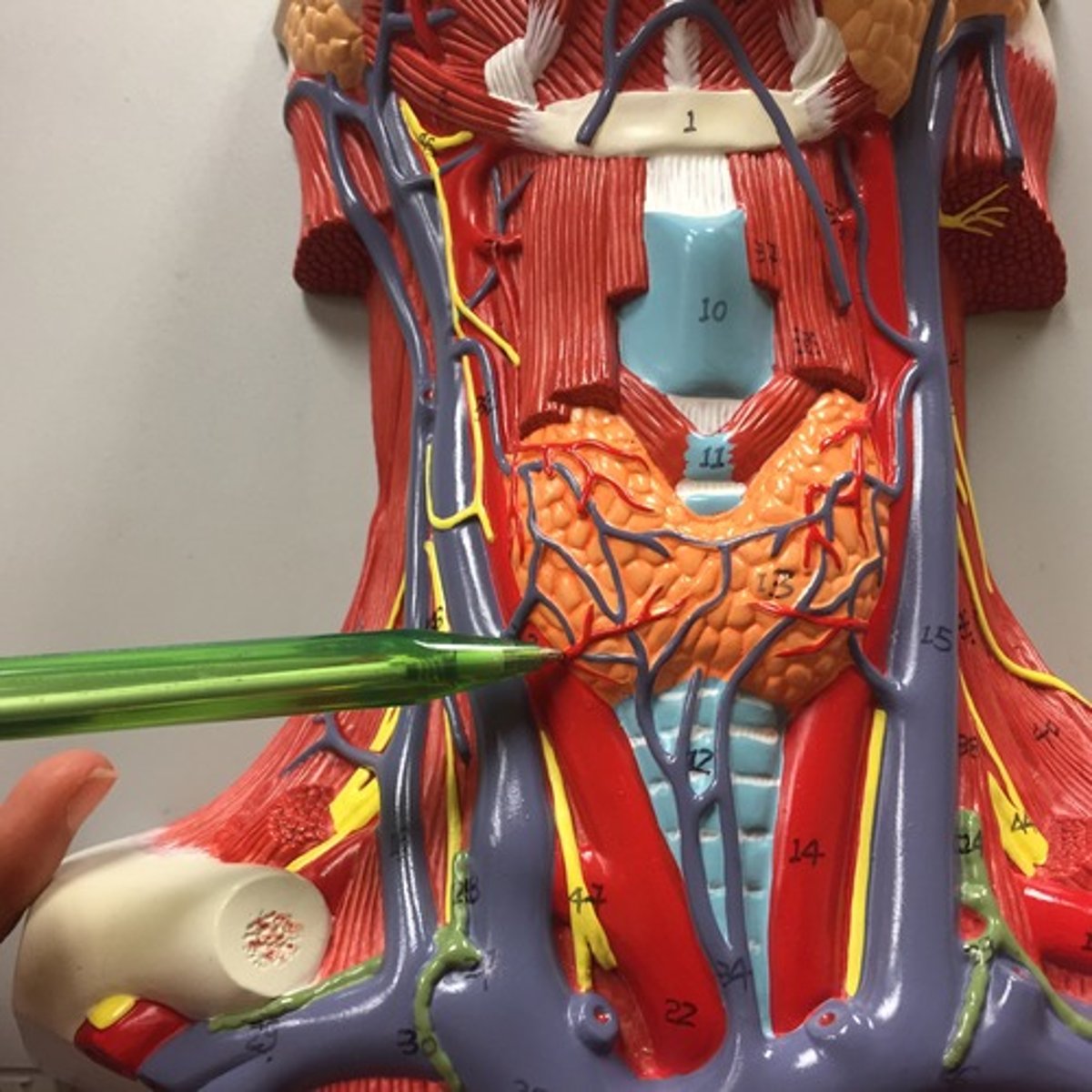
Thyrocervical trunk (branch of subclavian artery)
The Inferior part of the thyroid is supplied by the Inferior Thyroid Artery - what is this a branch of?
Supplies all intrinsic muscles of larynx - except cricothryoid (SLN)
What is the function of the Recurrent Laryngeal Nerve (runs near INFERIOR THYROID ARTERY)?
Forms as an outgrowth from the floor of the primitive pharynx - primordium originates at the FORAMEN CECUM
How does the Thyroid begin to grow in Embryology?
endoderm
Thyroid follicular cells are derived from (endoderm/mesoderm/ectoderm)
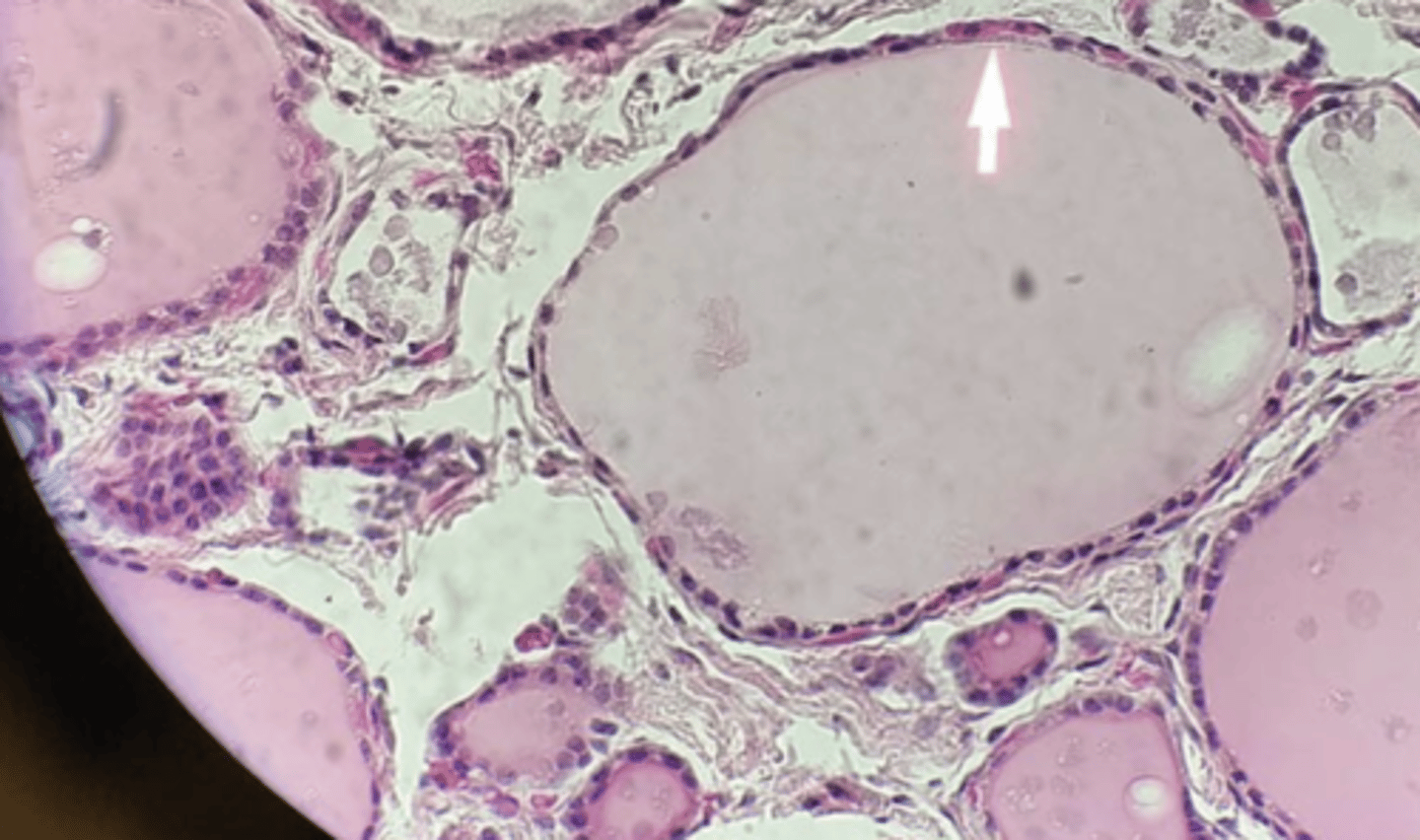
Follicle Epithelial Cells
What cells in the Thyroid...
> Acts a a single layer of cuboidal cells surrounding the follicles
> Synthesize Thyroglobulin (Convert T3 to T4) --> Thyroglobin stored in LUMEN of follicles as colloid (pink, proteinaceous material)
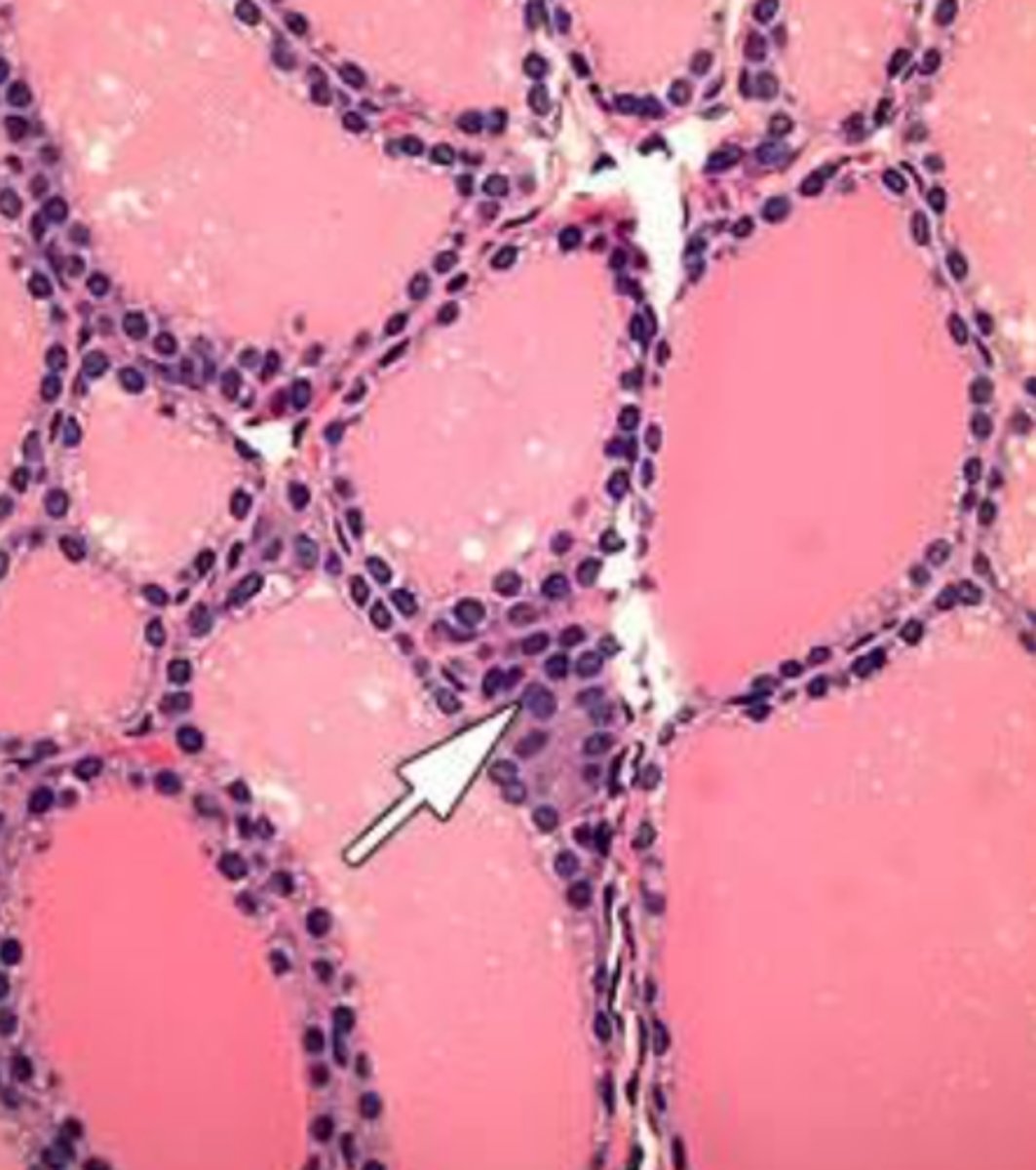
Parafollicular Cells
What cells in the Thyroid...
> Sit at the corner of 4 follicles
> Synthesize Calcitonin
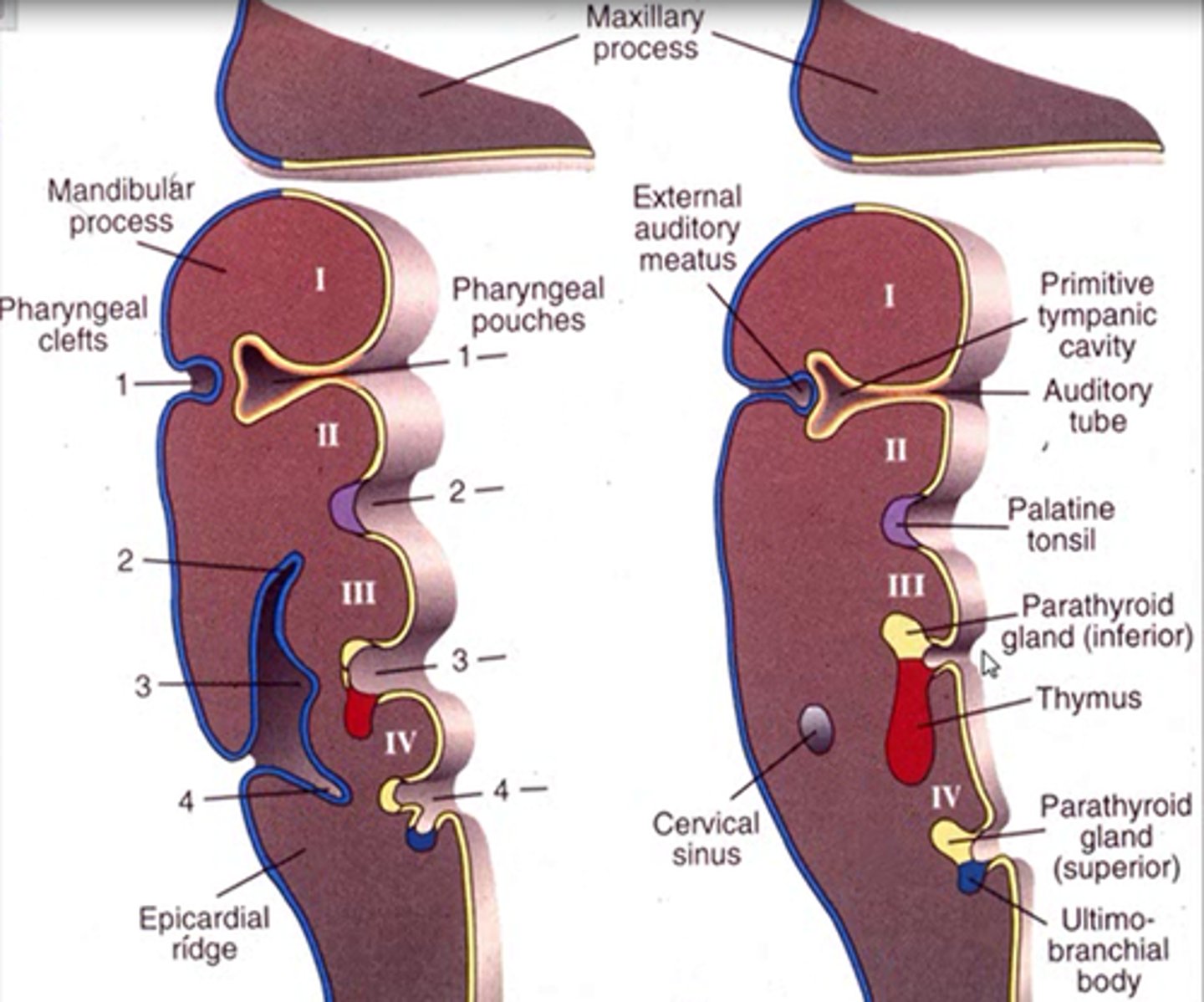
4th pharyngeal pouch
Parafollicular cells arise from what?
7th week
When should the Thyroid reach its final position during gestation?
Ectopic Thyroid Tissue
Define Condition:
Thyroid tissue located OUTSIDE of normal position in anterior neck
-Hx/Path: MC Secondary to failure of embryological descent
-Sx/PE:
> MC at Base of Tongue (LINGUAL)
-Prog: Removal --> Hypothyroidism (if it's the only thyroid tissue present)
10th week
When should the Thyroglossal duct be obliterated during gestation?
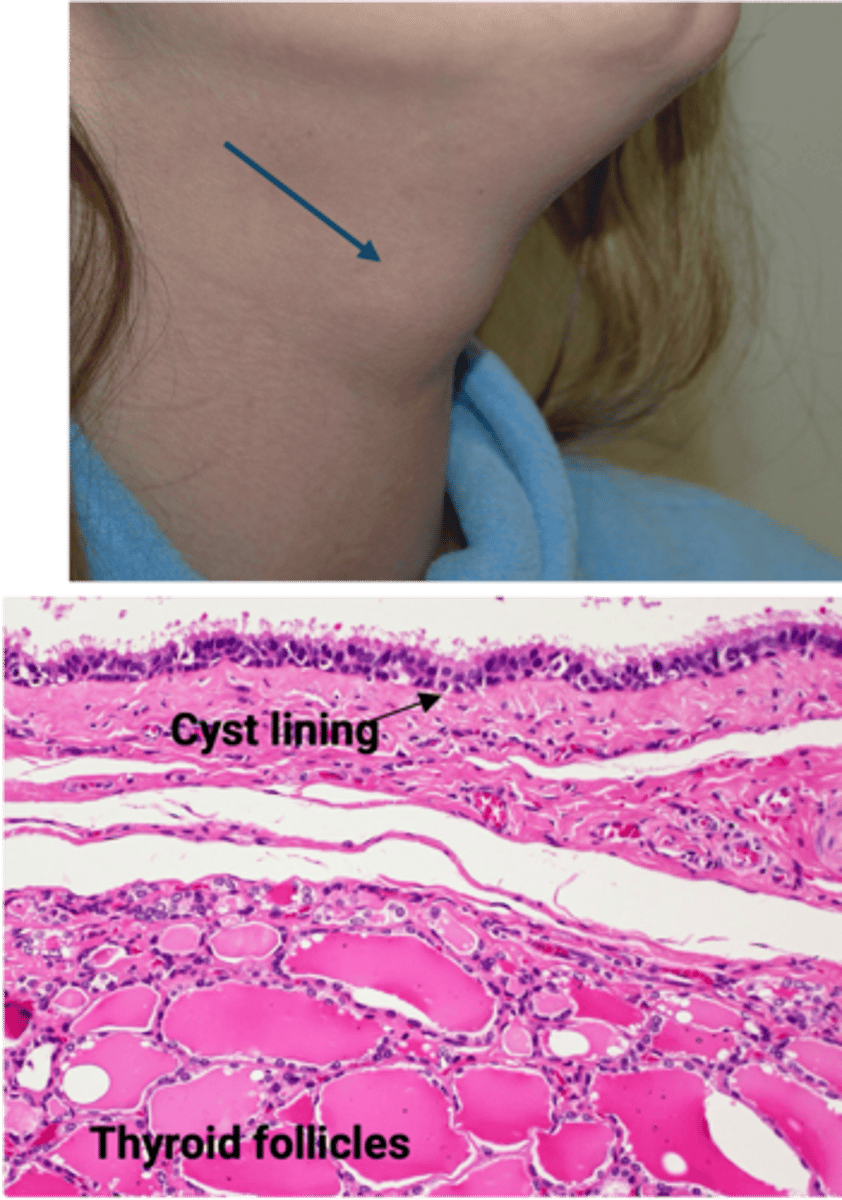
Thyroglossal Duct Cyst
Define Condition:
When portion of thyroglossal duct fails to involute
-Sx/PE:
> Anterior Midline Neck Mass moving w/ swallowing or tongue protrusion
-Dx: (Histo)
> Thyroid follicles in cyst/duct wall
> Lining can either by Nonkeratinizing Squamous Cells (if near foramen cecum) OR Ciliated Epithelium (if in lower neck)
-Basal Metabolic Rates
-Beta-Adrenergic Effects
-Blood Sugar Increase
-Breakdown Lipids
-Bone Growth
-Brain Maturation
-Bowel Movements
-Baby Surfactant
What are the functions of the Thyroid Hormone? (8 Bs)
Hyperthyroidism
Define Condition:
Increased levels of Thyroid Hormones (T3/T4)
-Hx:
> Graves disease
> Hyperfunctioning ("Toxic") Multinodular Goiter
> Hyperfunctional ("Toxic") adenoma of Thyroid
-Path: Metabolism speeds up and increase ANS activity
-Sx/PE:
> Hyperactivity
> Heat Intolerance
> Sweating
> Wt Loss
> Diarrhea
> Tachycardia
> Anxiety
> Tremor
-Prog: THYROID STORM
> Thyrotoxic crisis
> Abrupt onset of severe pathology
> MEDICAL EMERGENCY (can die of cardiac arrhythmia)
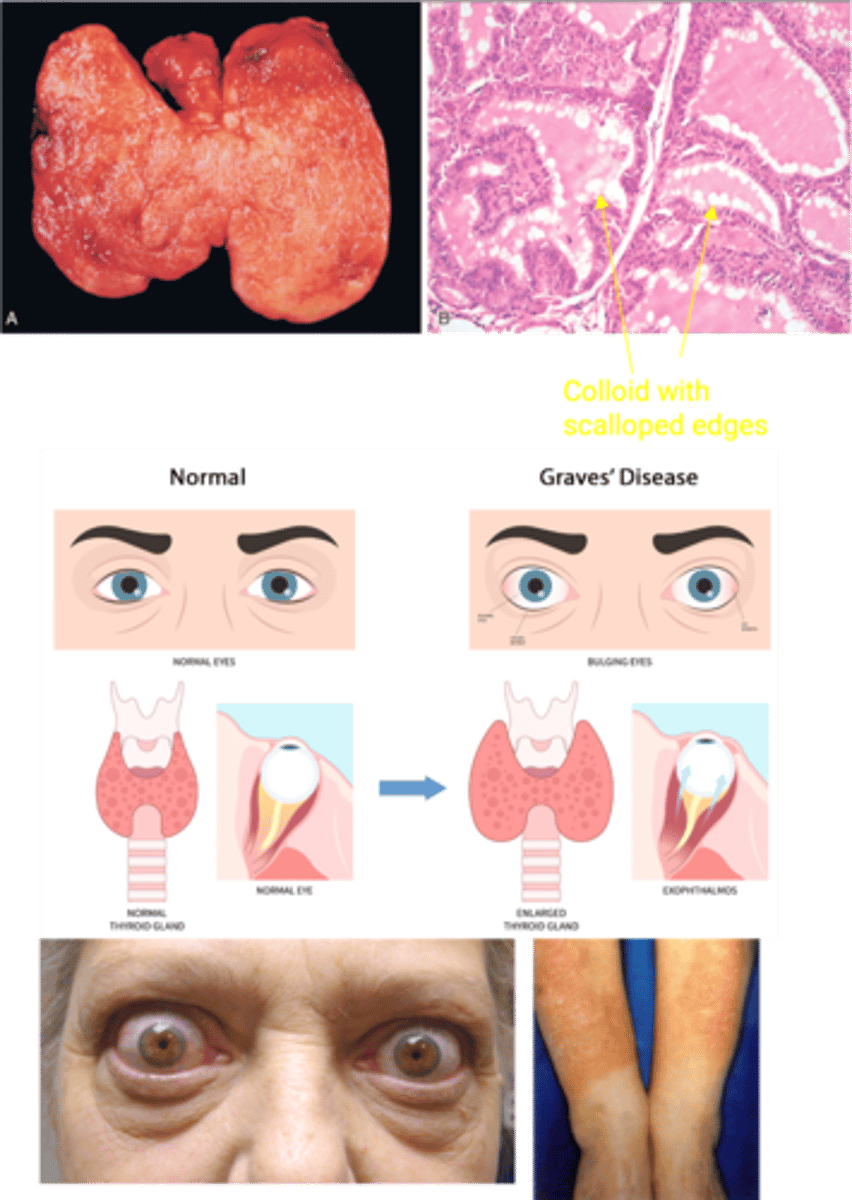
Graves Disease
Define Condition:
MCC of Hyperthyroidism
-Path: Autoimmune response against multiple thyroid antigens (most important = TSH receptor) --> TSH-receptor Antibody (TRAb), aka Thyroid-stimulating Immunoglobulin (TSI)
> IgG Autoantibody that mimics TSH --> Binds TSH receptor --> Follicular cells release TH --> More T3/T4, but Less TSH
-Sx/PE:
> Diffuse thyroid enlargement
> Bulging Eyes (infiltrative ophthalmopathy w/ exophthalmos)
>> CD4 T cells secreting cytokines and orbital fibroblasts have TSH receptors -> TSH receptors stimulated by TRAb -> fibroblast proliferation and secretion of hydrophilic glycosaminoglycans -> draws in water -> swelling
> Pretibial Myxedema (aka Infiltrative Dermopathy)
>> Deposition of glycosaminoglycans (HA) in dermis and subcutis
>> Early lesions are bilateral, firm, non-pitting, asymmetrical plaques or nodules
>> Can coalesce to form scaly, thickened and hardened skin areas
>> Overlying skin may be discolored
-Dx:
> Gross = Diffusely enlarged thyroid
> Micro =
>> Tall, crowded epithelial cells --> papillae
>> Pale, scalloped colloid
>> Lymphocytes (mostly T cells), plasma cells
Hypothyroidism
Define Condition:
Deficient Thyroid Hormone (T3/T4) production
-Path: Metabolism slows down
-Sx/PE:
> Lethargy
> Fatigue
> Cold Intolerance
> Wt Gain
> Constipation
> Bradycardia
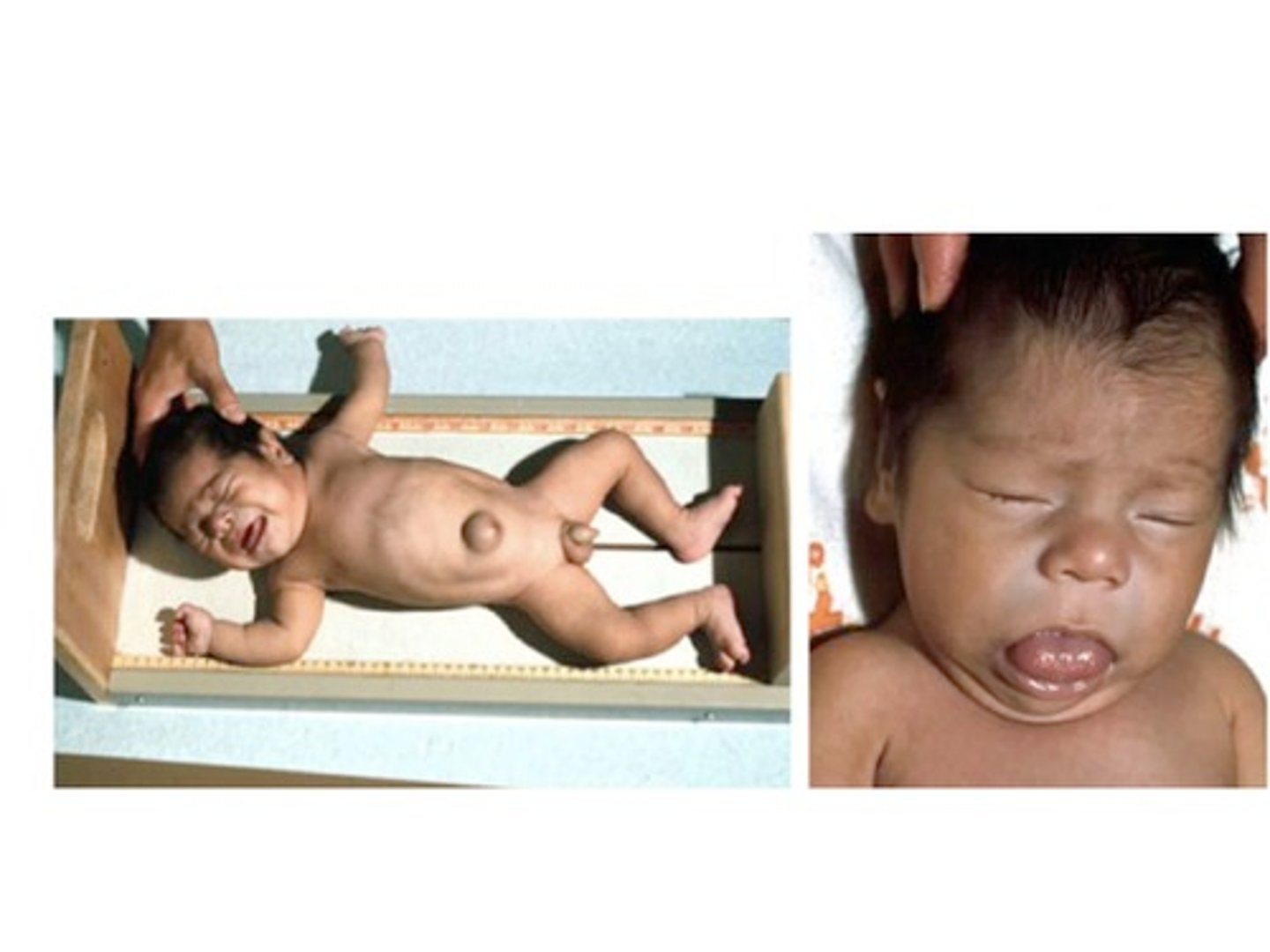
Congenital Hypothyroidism
Define Condition:
Thyroid Hormone deficiency AT BIRTH; Most Common TREATABLE CAUSE of Intellectual Disability
-Hx:
> Thyroid dysgenesis (abnormal gland developmet)
> Dyshormonogenesis (abnormal TH synthesis), ex = mutations in thyroid peroxidase
> Iodine Deficiency in mother during pregnancy
-Tx: Supplemental TH therapy
-Sx/PE/Prog: (if no Tx) = 6 Ps
> Pot bellied
> Puffy-faced (coarse facial features)
> Protruding umbilicus (umbilical hernia)
> Protuberant tongue (macroglossia)
> Poor brain development (poor myelin sheath development)
> Poor bone growth (short stature)
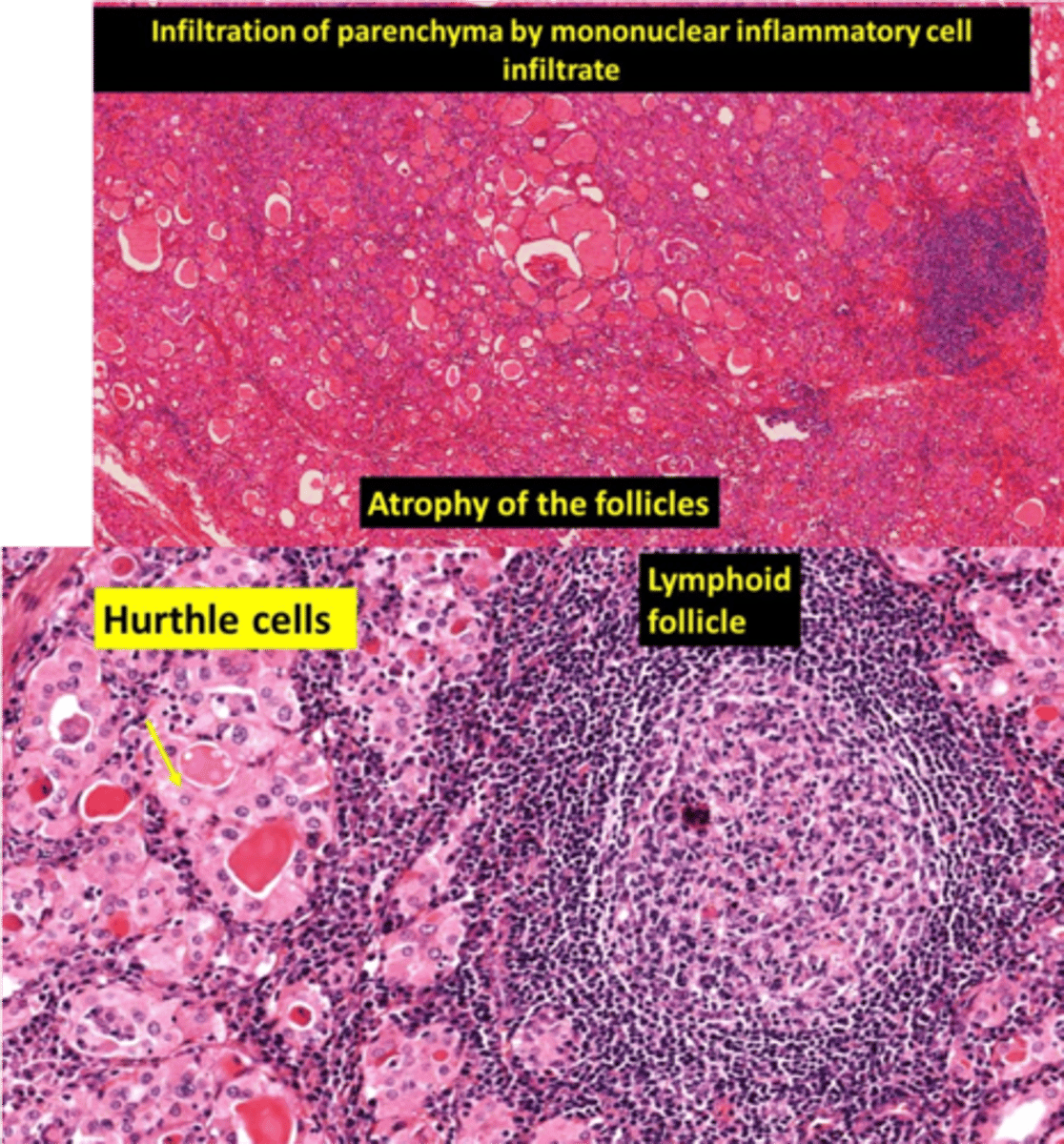
Hashimoto (Chronic Lymphocytic) Thyroidits - aka Autoimme Thyroiditis
Define Condition:
MCC of Hypothyroidism in Iodine Sufficient Regions
-Hx: A/w... (Autoimmune Diseases)
> SLE
> T1DM
-Path: Autoimmune response against Thyroid antigens (d/t breakdown of immune self-tolerance to thyroid autoantigens)
> CD8+ T cells attack thyroid epithelial cells
> Activation of CD4+ T cells --> inflammatory cytokines (INF-gamma) release --> Macrophage recruitment/activation --> Follicle damage
> Antithyroid Abs (Anti-TPO/Tg) = Cell mediated Cytotoxicity/Complement dependent damage
-Sx/PE:
> NONTENDER thyroid enlargement (preceded by transient hyperthyroid state - aka Hashitoxicosis - d/t follicular reupture and TH release)
-Dx:
> Labs =
>> (+) Anti-TPO (antimicrosomal Ab)
>> (+) Anti-Tg
> Gross = Diffusely and symmetrically enlarged thyroid
> Micro
>> Diffuse infiltration of thyroid parenchyma w/ lymphocytes and plasma cells
>> Lymphoid follicles w/ germinal centers
>> Atrophic thyroid follicles
>> Hurthle cell (abundant pink, granular cytoplasm) metaplasia d/t ongoing injury
-Prog: Risk of Non-Hodgkin B cell Lymphoma
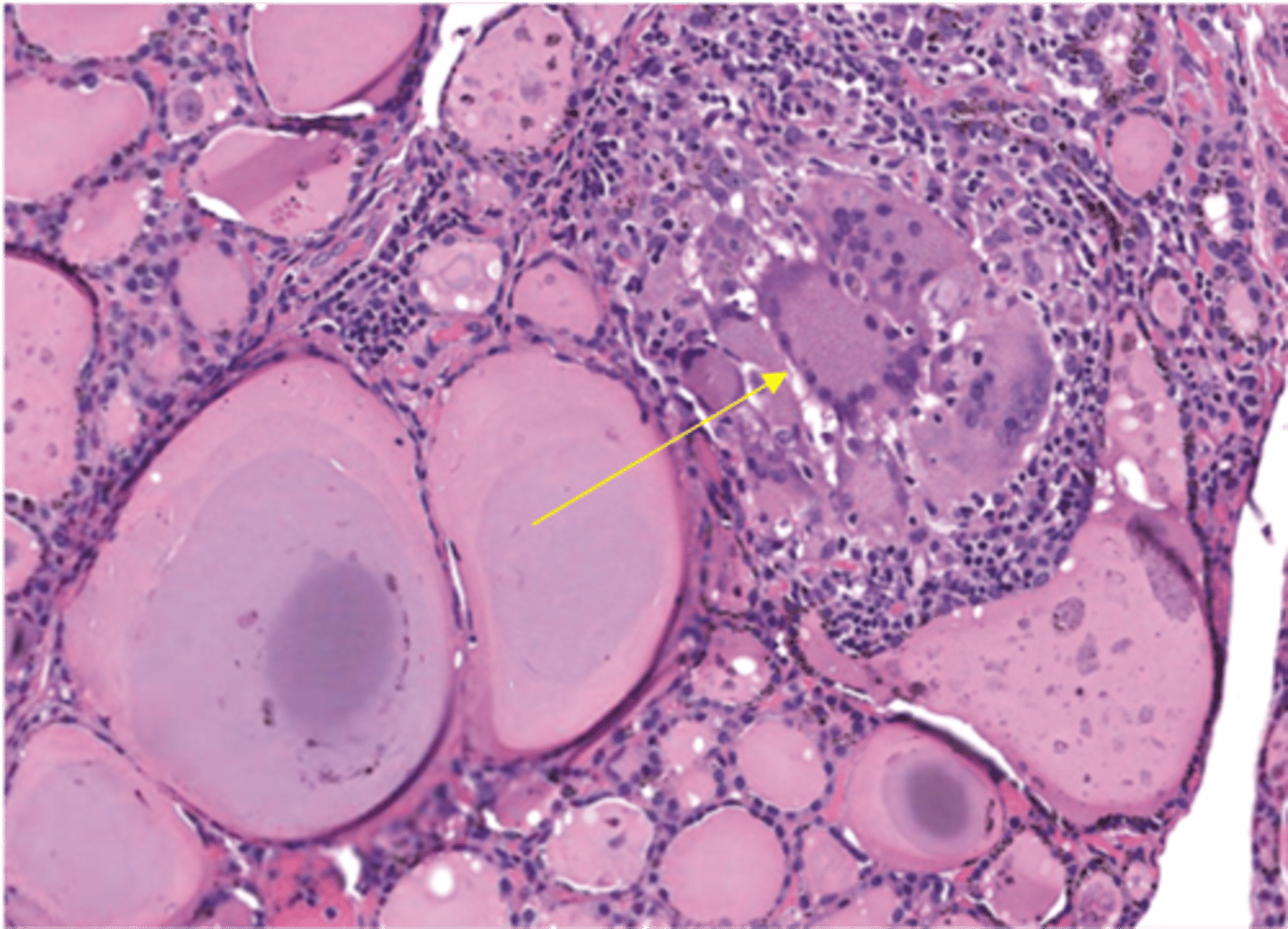
Subacute Granulomatous (de Quervain) Thyroiditis
Define Condition:
Self-limiting Granulomatous inflammation of the thyroid
-Hx: Transient Hyperthroidism --> Euthyroid State --> Hypothyroidism --> Euthyroid State
-Path: URI shortly before (d/t viral infection or inflammation in response to infection)
-Sx/PE:
> PAINFUL/TENDER Thyroid
-Dx:
> Gross = Firm, enlarged (unilateral or bilateral) thyroid)
> Micro =
>> Mixed inflammatory infiltrate (Partial destruction of follicles with a mononuclear lymphocytic infiltrate)
>> Follicle disruption --> granulomatous inflammation (macrophages and mulitnucleated giant cells)
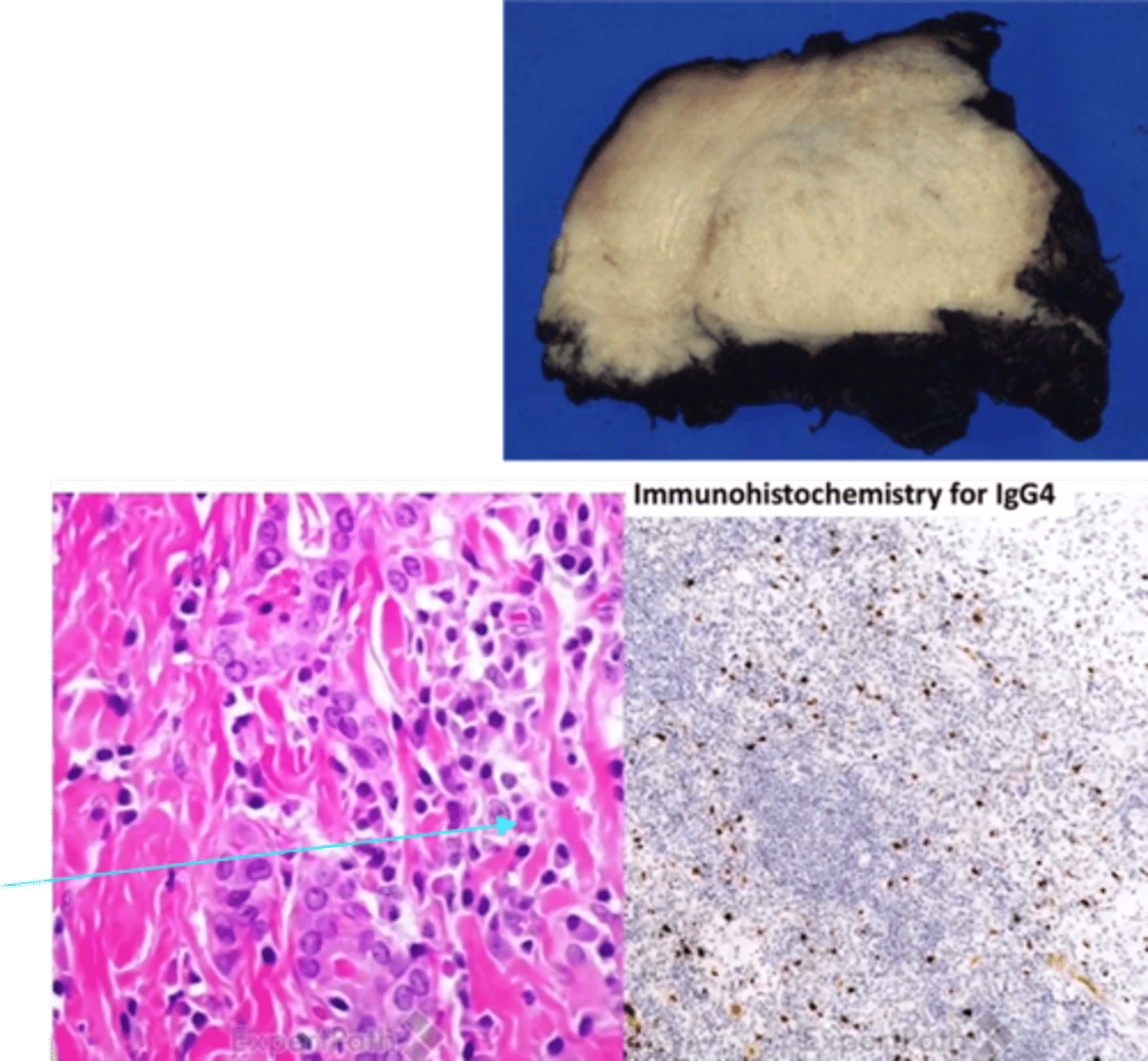
Riedel Thyroiditis
Define Condition:
Invasive fibrous thyroiditis
-Path: IgG4 related disease
> IgG4-producing plasma cells and lymphocytes
> Fibrosis and complete/partial obstruction of medium sized veins
> Hypothyroidism ONLY in 1/3 pts
-Sx/PE:
> Hard, fixed, NONTENDER, thyroid
-Dx:
> Gross =
>> "ROCK HARD" fixed thyroid mass adherent to surrounding tissues --> mimics malignancy
>> Cut surface = Tan/gray, WOODY, avascular
> Micro =
>> Dense, thick fibrosis --> replacing normal thyroid tissue
>> Marked lymphoplasmacytic infiltrate
-Tx:
-Prog: Fibrosis extending to local structures (trachea, esophagus) --> MIMICS ANAPLASTiC CARCINOMA
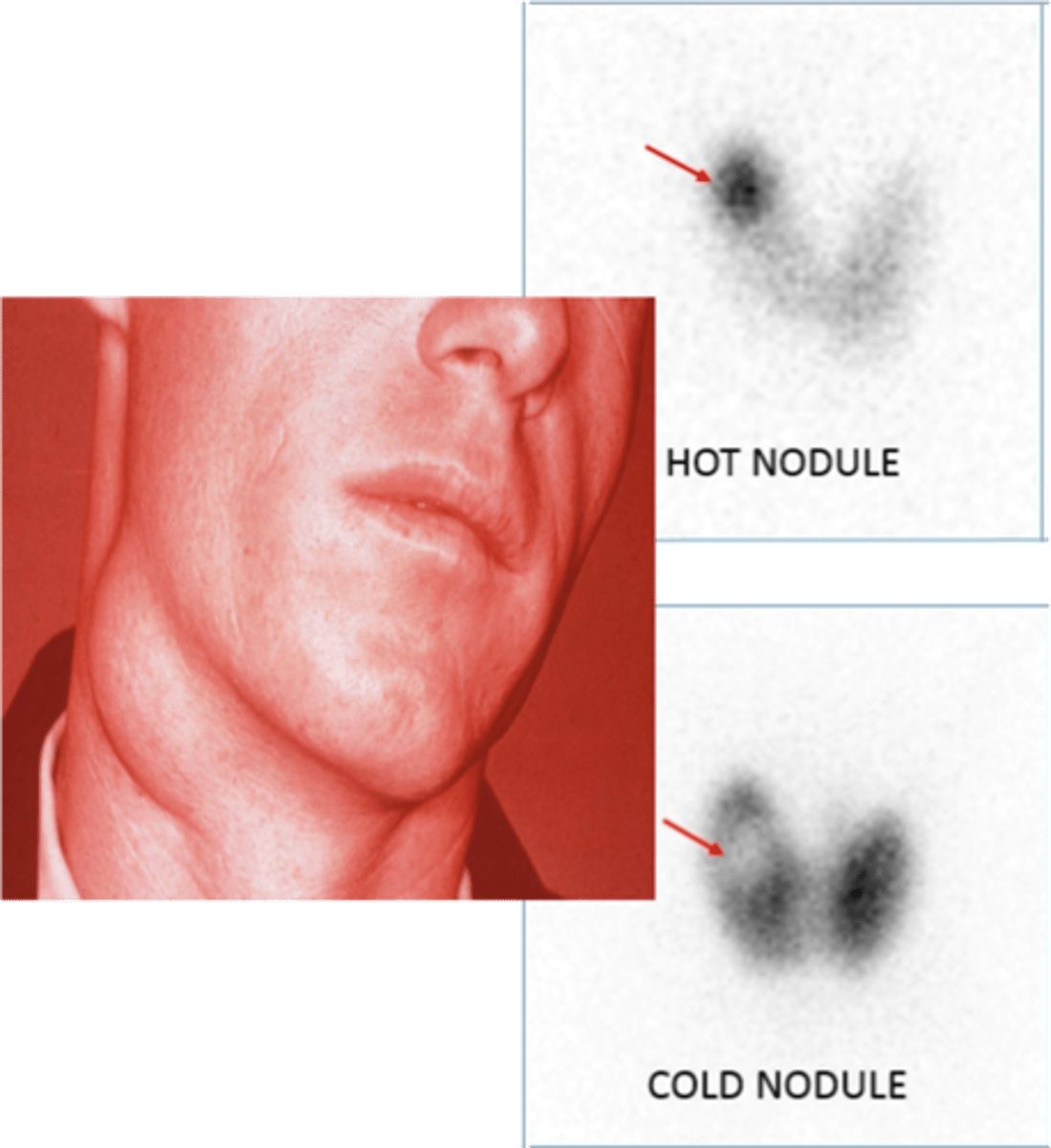
Thyroid Neoplasms
Define Condition:
-Sx/PE: Solitary Thyroid Nodule
-Prog: MOST ARE BENIGN
-Dx:
> Check TSH to determine if functional or non-functional
> Fine Needle Aspiration
> Functional
>> Low TSH
>> Radioactive iodine uptake (RAIU) confirm it to be "hot"
> Non-Functional
>> Normal or High TSH
>> RAIU show low uptake/cold (10% cold = MALIGNANT)
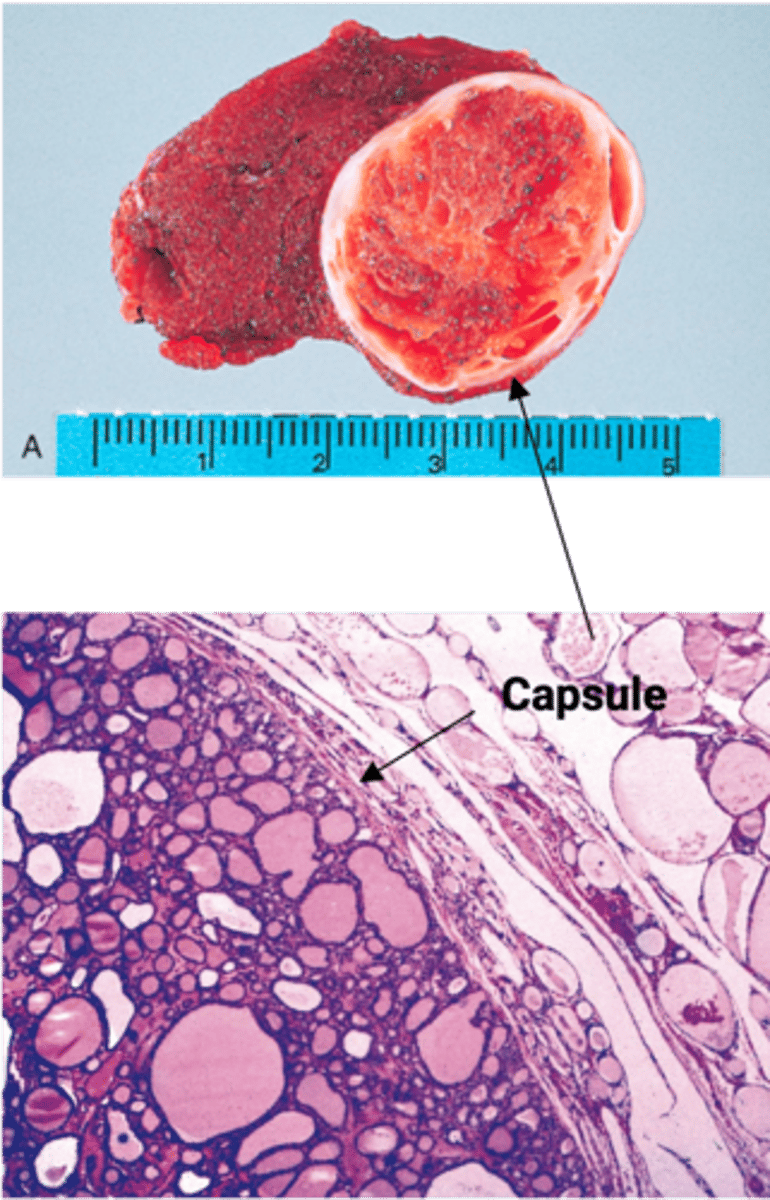
Follicular Adenoma
Define Condition:
MC Benign Thyroid Neoplasm (proliferation of thyroid follicles)
-Sx/PE: Solitary NONPAINFUL nodule (most non-functional, but functional = toxic adenoma)
-Dx:
> Gross = Solitary nodule w/ well-defined intact capsule
> Micro = Thyroid tissue completely surrounded by fibrous capsule - can't differentiate this from carcinoma b/c entire capulse can't been see in frozen section
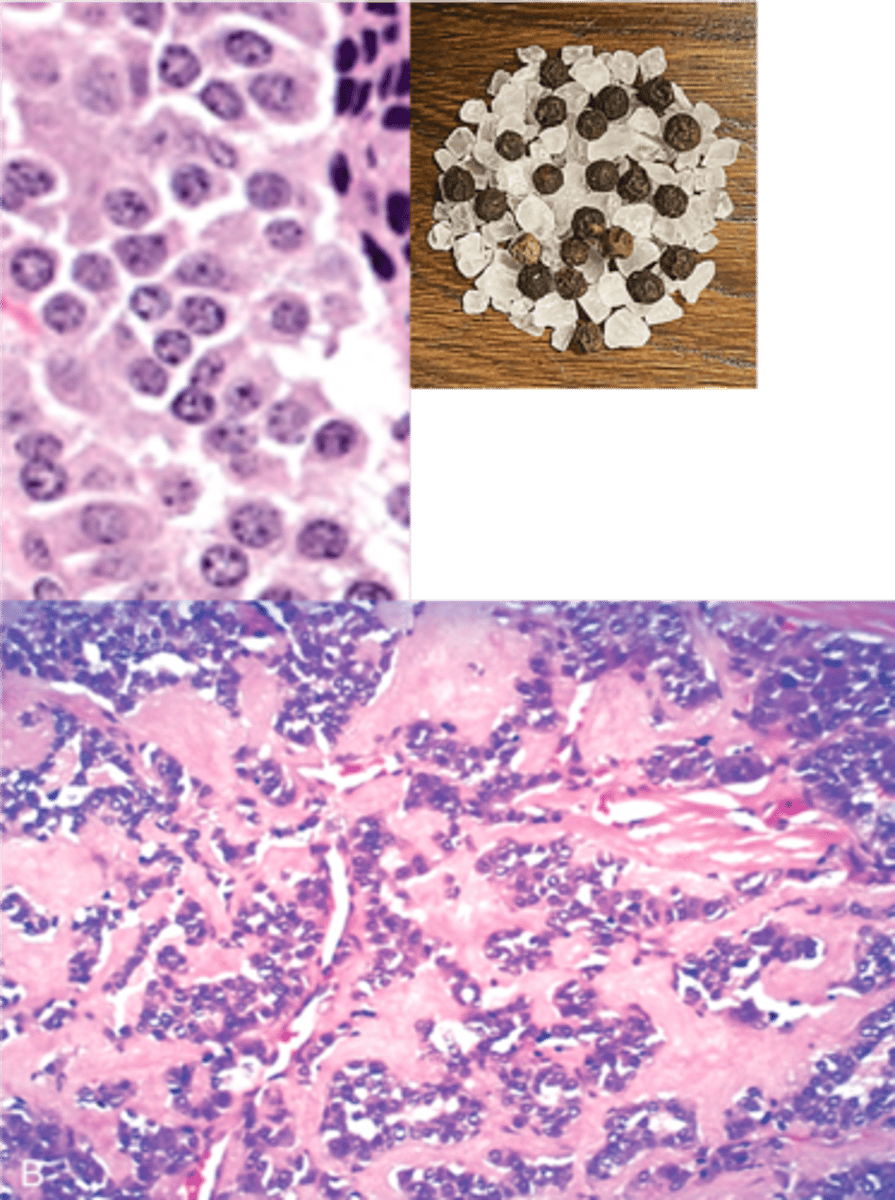
Papillary Thyroid Carcinoma
Define Condition:
MC Thyroid Carcinoma
-Hx: RADIATION EXPOSURE
> Children who had radiation for cancer Tx
> Chernobyl nuclear disaster
-Path: Activation of MAP kinase signaling pathway
> MC = BRAF mutation
> RET/PTC fusion
-Sx/PE: NONPAINFUL Neck Mass
-Dx:
> Gross = Solid, white cut surface; Solitary OR Multifocal
> Micro (Dx based on NUCLEAR FEATURES - via FNA)=
>> Branching papillae w/ fibrovascular core
>> Optically clear (empty, ground glass) nuclei = OPRHAN ANNIE Nuclei
>> Nuclear pseudoinclusions
>> Intranuclear grooves
>> Psammoma bodies (concentric calcifications)
-Prog: Spreads to cervical LNs, but prognosis is good (>95% 10 yr survival)

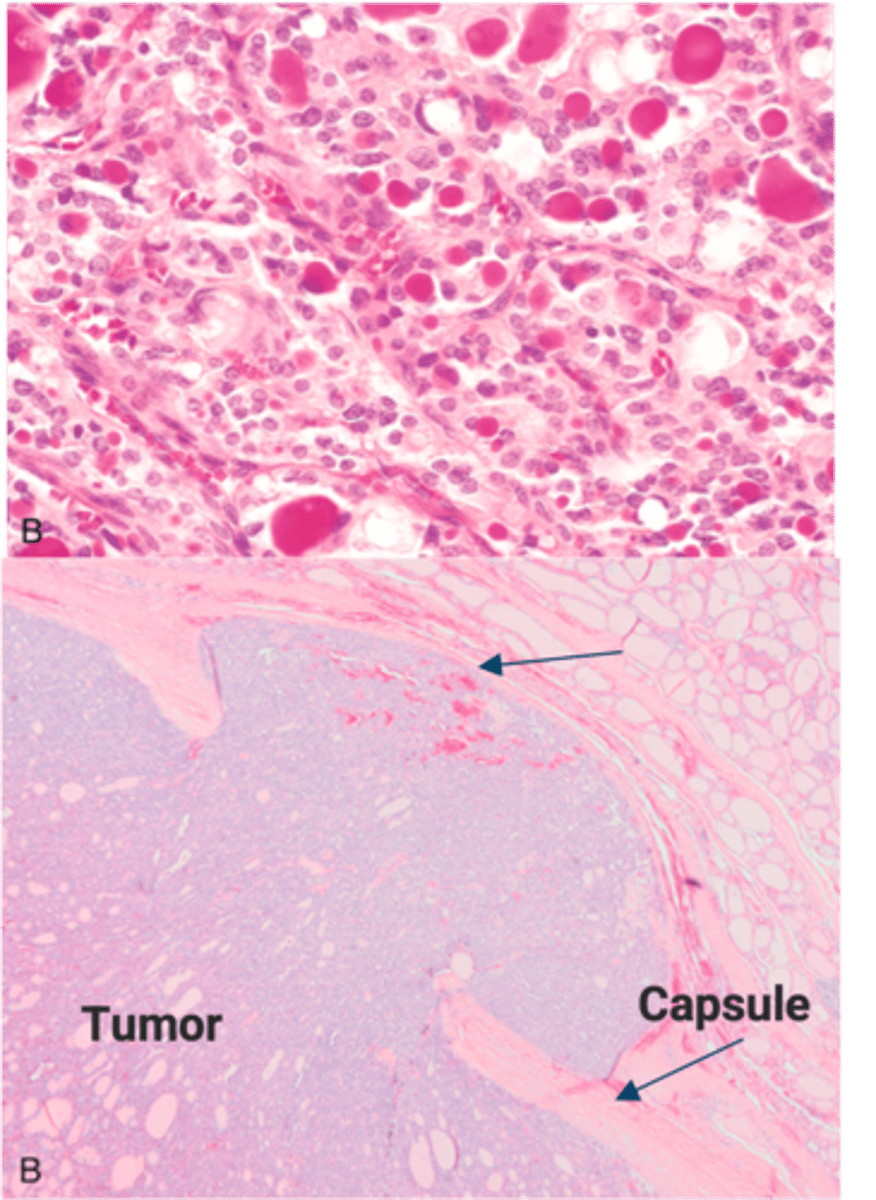
Follicular Thyroid Carcinoma
Define Condition:
-Hx:
> Peak = 40-60 y/o
> MC in areas of dietary iodine deficiency
-Path: A/w RAS mutation and PAX8-PPARG translocation
-Sx/PE: Solitary Cold Thyroid Nodule
-Dx:
> Micro (Dx on FNA) = Similar to Adenoma; Capsular invasion and/or vascular invasion
-Prog: Spreads hematogenously --> LUNGS, BONES, LIVER, but GOOD PROGNOSIS
Medullary Thyroid Carcinoma (MTC)
Define Condition:
Malignant proliferation of parafollicular "C" cells
-Hx:
> 70% are SPORADIC (nonhereditary)
>> Ages 40-60
>> Solitary
> 30% are FAMILIAL (hereditary)
>> Younger (mean = 35 y/o)
>> Bilateral and Multicentric
>> Seen w/ Multiple Endocrine Neoplasia (MEN) Syndrome 2A and 2B but not associated
>> ALL a/w RET mutations
-Path: More CALCITONIN --> ↓ serum Ca2+ by inhibiting osteoclasts (↓bone resorption) and ↓ kidney Ca2+ reabsorption, but not important in normal Ca2+ homeostasis
> Altered Calcitonin Deposits ==> AMYLOID DEPOSITS
-Dx:
> Gross: Solid, Gray-Tan yellow
> Micro:
>> Polygonal to spindle-shaped tumor cells arranged in nests, cords, or glands
>> Round nuclei with finely stippled to coarsely clumped chromatin (“Salt and pepper” chromatin)
>> Amyloid deposits in stroma (homogeneous pink extracellular material -> stains red on Congo red stain and shows apple green birefringence under polarized light)
>> Tumor cells AND Amyloid = (+) CALCITONIN IHC Stain
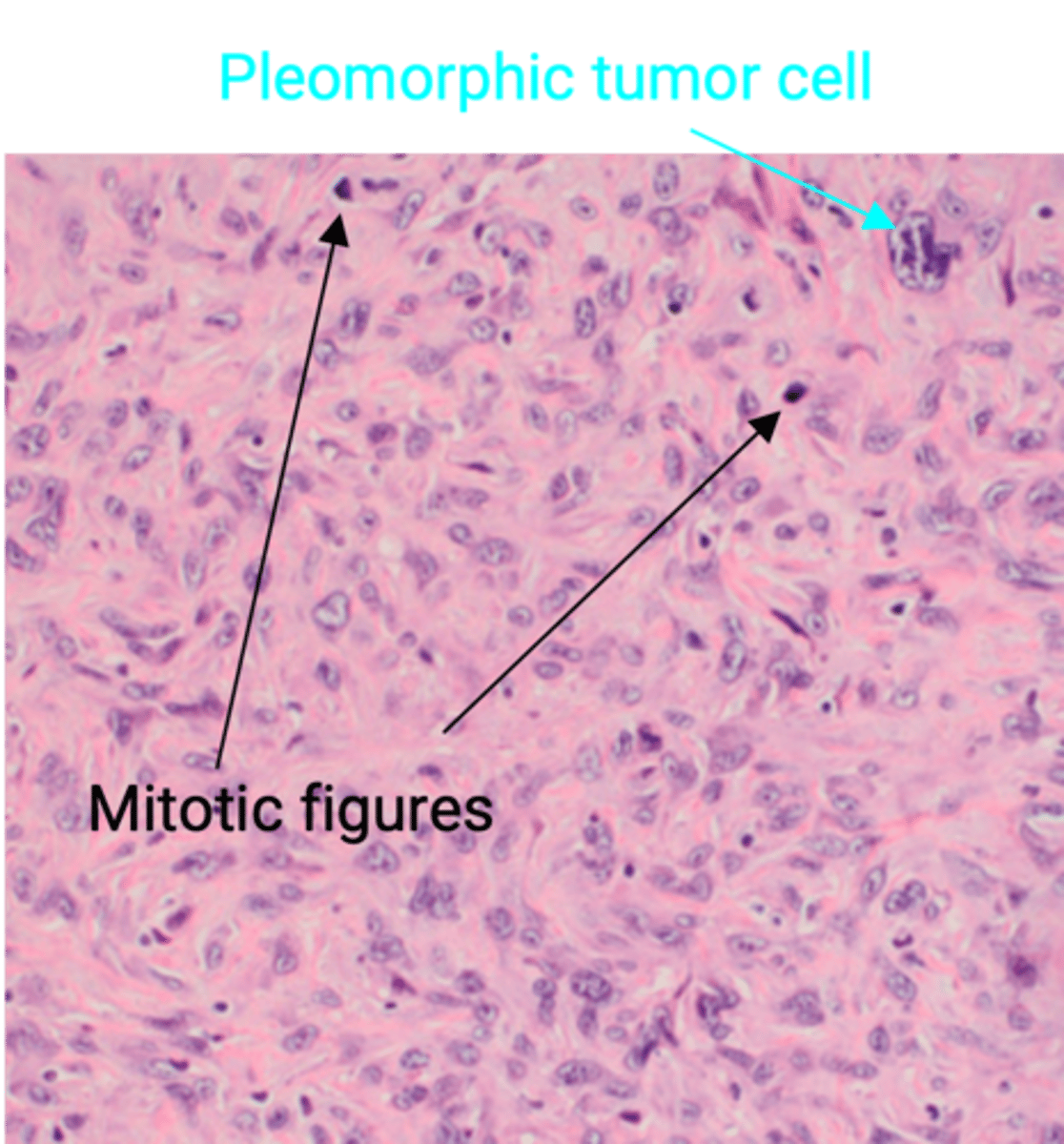
Anaplastic Thyroid Carcinoma
Define Condition:
Undifferentiated malignant tumor of thyroid follicular epithelium
-Hx:
> A/w TP53 mutation
> Mean Age = 65 y/o
> Arises from well-differentiated PTC or FTC (or de novo)
-Path/Sx/PE: VERY AGGRESSIVE (rapidly invades/compresses local tissue)
> Trachea = Dyspnea
> Esophagus = Dysphagia
> RLN = Hoarseness
-Dx:
> Micro = Anaplastic Cells (large, pleomorphic tumors cells)
-Prog: POOR PROGNOSIS (mortality rate ~ 100% w/n less than 1 yr) d/t aggressive local growth and compromising vital structures in neck