what are the three major structures contained in the scrotum?
spermatic cord, epididymis, testes
tunica vaginalis
serous covering of testis
a double-layer extension of the peritoneum that separates scrotal layers from the tunica albuginea
covers testes except at the back where the epididymis is attached
what are the three layers of the tunica vaginalis
parietal, visceral, vaginalis sac
What are the three ducts that sperm travel through to exit the body?
epididymis, ductus (vas) deferens, urethra
What are the accessory sex glands?
seminal vesicles, prostate, bulbourethral glands
tunica albuginea
dense, fibrous capsule covering testis
extends inward and divides each testicle into 250-400 lobules
lobules
internal compartments formed by projections of tunica albuginea
contain seminiferous tubules and interstitial cells (Leydig) with their bases are near surface and apices converge toward mediastinum testis
seminiferous tubules
Each lobule contains 1-3 of these tightly coiled tubules
Produce sperm by spermatogenesis
sustentacular (Sertoli) cells
found in the tubules and among the sperm cells, form the blood-testis barrier need for immunity
rete testis
seminiferous tubules converge to form rete testis
located at testicular mediastinum
mediastinum teste
Thickened portion of albuginea along posterior border of testis that projects inside it and creates a linear fibrous structure
Point where tubules converge and exit into rete testis and efferent ducts
appendix testis
a remnant tissue after paramesonephric duct degenerates
small portion at cranial end
ductus/vas deferens
Muscular cord designed to pump sperm into the prostatic segment of the urethra
Ascends along posterior border of testis and enters pelvic cavity thru the inguinal canal where it travels over the side and posterior surface of bladder
Seminal vesicles connect to vas deferens to form ejaculatory ducts
Stores sperm for up to several months
spermatic cord
Supporting tube of testes
Contains blood vessels, nerves, lymph nodes, cremaster muscle
Attached to posterior border of testis
Travels through inguinal canal toward posterior surface of bladder where it joins the seminal vesicle duct to form the ejaculatory ducts
epididymis
comma shaped structure that curves along posterior border of testis
consists of head, body, tail, appendix epididymis, and efferent ductules
epididymis head
(globus major) most superior aspect, consists of first part of efferent ducts that transport sperm out of testes(globus major): most superior aspect, consists of first part of efferent ducts that transport sperm out of testes
epididymis body
(corpus) contains ductus epididymis, which is a tightly coiled single tube where the efferent ducts empty into
epididymis tail
(globus minor) distal part of epididymal ducts that exit and continue as ductus (vas) deferens in spermatic cord
appendix epididymis
mesonephric duct persists to form the ductus deferens, except for its most cranial portion, which becomes this structure
efferent ductules
pass from the rete to enter upper portion of the epididymis
normal testicle size
length= 4-5cm
width= 2-3cm
AP= 2-3cm
weight= 12.5-19g
symmetric, oval-shaped glands with smooth contour
arterial blood supply to the testes
Aorta → Testicular Artery → Travels in retroperitoneum & enters inguinal canal in spermatic cord where it branches into → Capsular Arteries (run in layer beneath tunica albuginea) and surround testis as → Centripetal Arteries (run into testicular parenchyma toward mediastinum)
testicular flow pattern
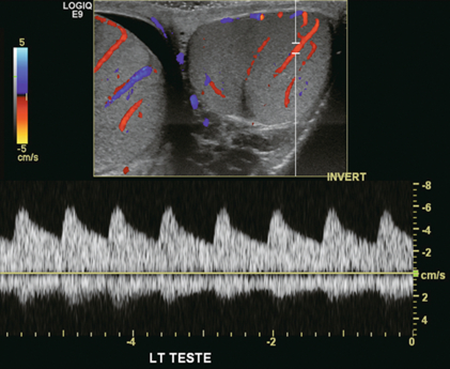
low resistance arterial flow
broad systolic peaks and high levels of diastolic flow throughout cardiac cycle
RI average: 0.55-0.64
arterial blood supply to scrotum and epididymis
Inferior Epigastric Artery → Cremasteric (External Spermatic) Artery (spermatic cord)
Inferior Vesical Artery → Deferential Artery (spermatic cord) courses through the tail of epididymis → divides into capillary network
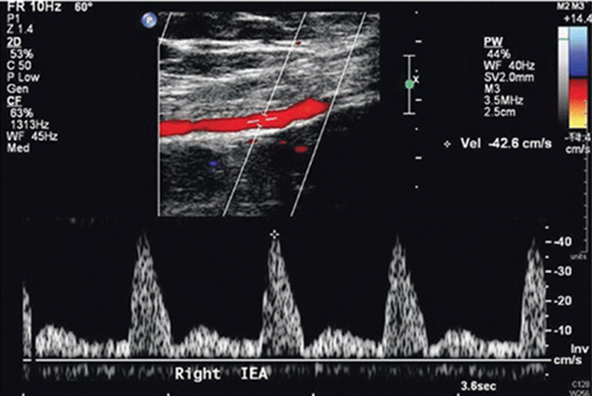
scrotum and epididymis flow pattern
does not supply testicular tissue
high-resistance arterial flow
narrower systolic peaks and diminished or absent diastolic flow
venous blood supply to testes
Intratesticular Veins exit mediastinum → Venous Outflow → Pampiniform Plexus → Internal Spermatic Vein → drains into:
Left Internal Spermatic Vein → Left Renal Vein → IVC
Right Internal Spermatic Vein → IVC
Typical venous flow pattern
lymphatic drainage of testes
Lymph plexuses under tunica vaginalis, testis, and epididymis
↓
Traverse in spermatic cord
↓
Follow testicular vessels
↓
Lumbar (para-aortic) nodes as high as renal veins
spermatogenesis
Sperm formation
Is the sequence of events in the seminiferous tubules that leads to the production of male gametes: sperm or spermatozoa.
The process begins during puberty, around the age of 14 years & continues throughout life
healthy adult male makes about 400 million sperm a day
hormonal regulation of testicles: reproductive function
brain-testicular axis
hormonal regulation of testicles: spermatogenesis & testicular androgen
hypothalamus, anterior pituitary gland, testes
the amount of testosterone and sperm produced by the testes reflects a balance among three sets of hormones:
Gonadotropins: which directly stimulate the testes
GnRH: which indirectly stimulates the testes via its effects on FSH and LH release
Testicular hormones (testosterone & inhibin): which exert negative feedback
the more testosterone produced, the more sperm produced
function of the scrotum
Supporting structure for testes
Regulates temperature of testes
Holds testicles outside the body where the temperature is more optimum for sperm maturation
Contraction of the cremaster muscles maintains scrotum position outside the pelvic cavity
function of epididymis
Site for sperm maturation, which requires 18 hours to 10 days
Site of sperm storage
Stores sperm until orgasm, then propels sperm from testicle to vas deferens within spermatic cord
exocrine function of testicles
producing spermatozoa (male germ cells)
endocrine function of testicles
synthesizing and secreting testosterone
human chorionic gonadotropin (HCG)
can be produced by tumors which can raise its levels in blood
what cancers is HCG elevated in?
seminoma
embryonic cell tumors of testes
testosterone
Main androgen secreted by Leydig cells
Induces puberty in males
Maintains male secondary sex characteristics
what pathologies is testosterone elevated in?
Testicular tumor
Adrenal hyperplasia
Benign or malignant tumors of testes, adrenal, pituitary
Adrenal tumor
what pathologies is testosterone decreased in?
Orchiectomy (removal of testes)
Testicular or prostate cancer
Cirrhosis of liver (no metabolism of testosterone)
Primary or secondary hypogonadism (gonads not fully developed)
normal ultrasound appearance of testicles
Homogeneous with medium-level echoes
Smooth walls
Each testis and epididymis must be compared for matching size and echogenicity
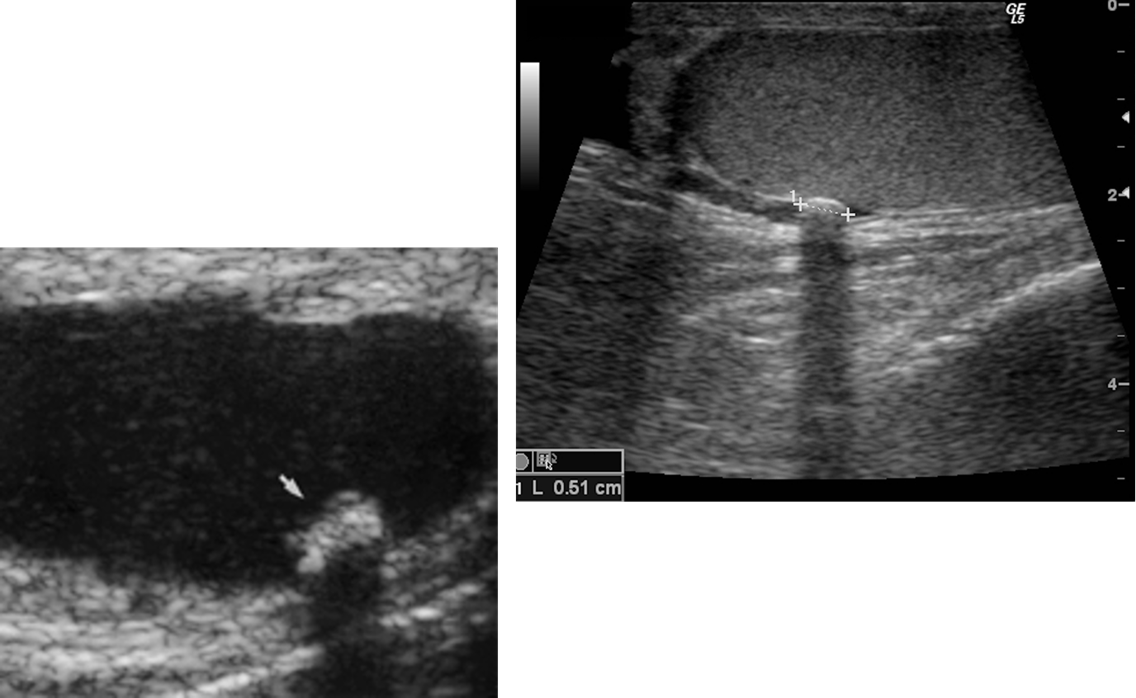
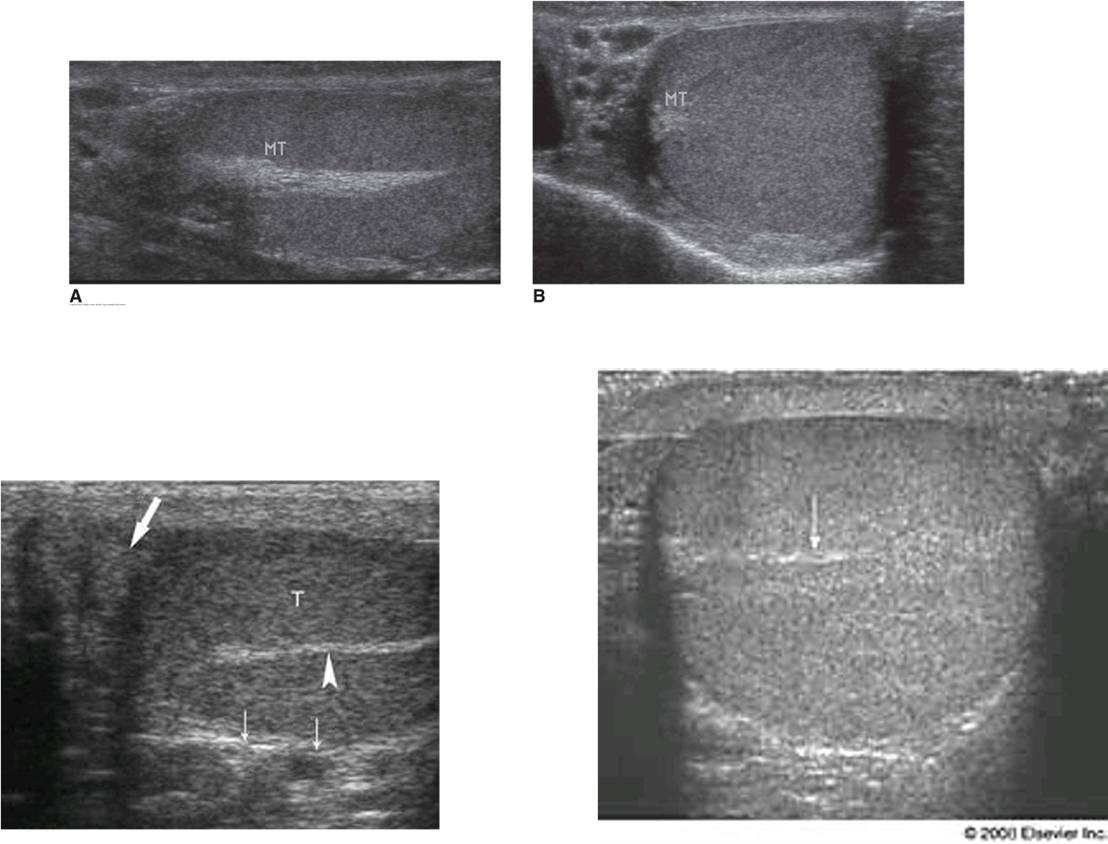
mediastinum testis
Highly echogenic linear structure peripherally located in posterior-superior aspect of testis (parallel to epididymis)
appendix testis
Small ovoid structure beneath head of epididymis
What is this structure?
mediastinum testis
What is this structure?
appendix epididymis
ultrasound appearance of epididymis
Head: Isoechoic or slightly more echogenic than testis
Body: Isoechoic or slightly less echogenic than head and testes
Tail: Slightly thicker than body
testicular artery doppler evaluation
low resistance (needs constant blood supply)
broad systolic peaks and high diastolic flow
deferential artery doppler evaluation
high resistance
narrow systolic peaks and low diastolic flow
cryptorchidism
undescended testis
etiology of cryptorchidism
Normally testes descends into scrotal sac at 8 months gestational age
where are the ectopic locations of cryptorchidism in children?
inguinal canal
where are the ectopic locations of cryptorchidism in adults?
small testis with normal echogenicity usually found in the inguinal canal
what are the potential concerns with cryptorchidism?
increased chance of malignancy (seminoma) in undescended testicle
infertility
cryptorchidism on ultrasound
Malpositioned testes situated anywhere along the normal track of descent from the retroperitoneum to scrotum
Most commonly found at or below level of inguinal canal
Appear more echogenic than muscle
Identify this pathology
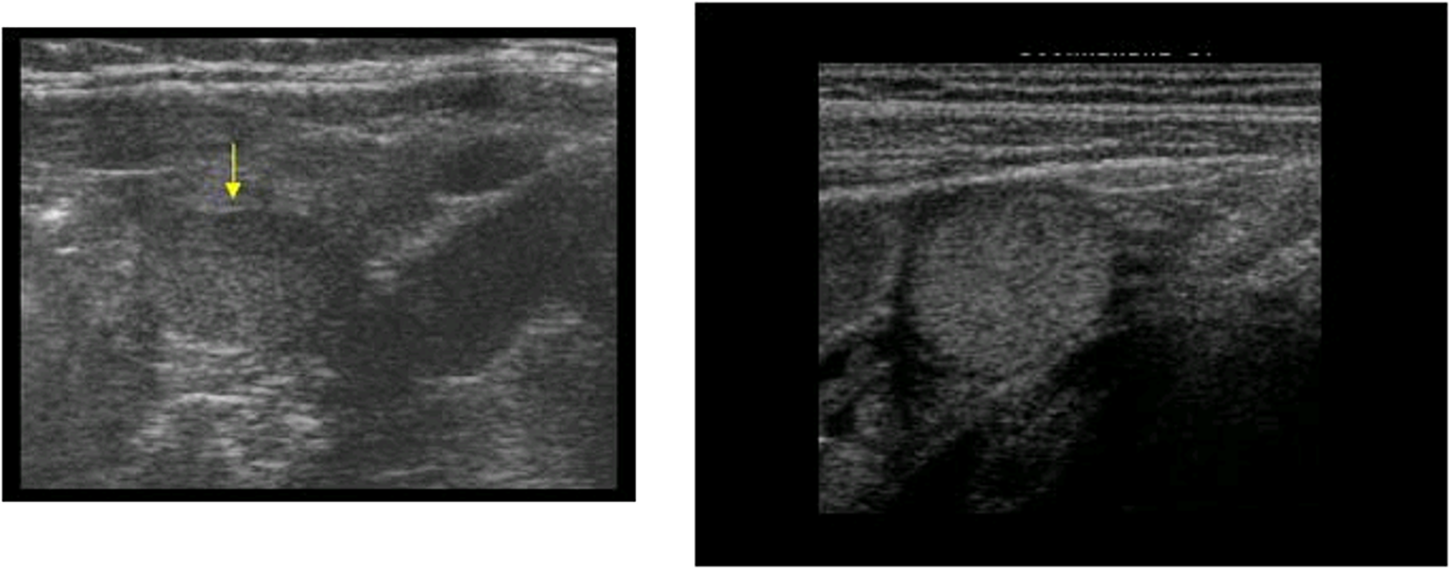
cryptorchidism
what is acute scrotum pain most commonly caused by?
epididymitis or orchitis
torsion cannot be ruled out
testicular torsion
Twisting of the spermatic cord that results in loss of blood supply to the testis and blocks venous drainage resulting in venous congestion within testicles
what is testicular torsion caused by?
Caused by developmental weakness of mesenteric attachment of spermatic cord to the testis and epididymis
bell clapper deformity
seen in testicular torsion
This abnormal development allows testicle to fall forward in scrotum and rotate freely within the tunica vaginalis creating this deformity
testicular torsion etiology
Spermatic cord and/or testicle twist
Limits vascular flow and drainage, which compromises blood supply and results in ischemia
Represents 20% of scrotal disease in post pubertal males
Occurs most commonly during adolescence (peak incidence at 14 years)
Surgical treatment within 4-6 hours in necessary as testicular viability can be lost very quickly
acute torsion signs & symptoms
Sudden onset of extreme testicular pain
50% of patients have nausea and vomiting
May have low-grade fever
Left testicle is more often affected than right testicle
After 24-48 hours, pain usually disappears indicating that the testicle is dead
ultrasound appearance of torsion after a period of ischemia
Testis and epididymis appear enlarged with decreased echogenicity, inhomogeneous
Scrotum appears with thickened wall, edematous, and hypervascular
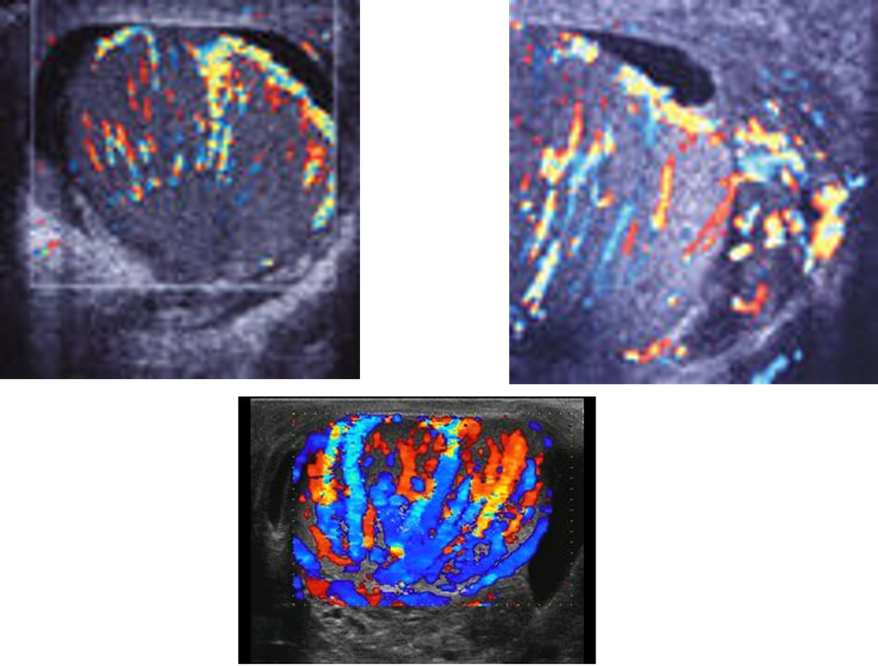
torsion on doppler
Testicular ischemia is noted by complete or near-complete absence of detectable blood flow in symptomatic testicle
After 24 hours, absent blood flow to testis is seen
If no flow is detected on color Doppler, there is complete torsion
chronic torsion etiology & symptoms
Spermatic cord and testicle twist, resulting in ischemia to testicle and complete cessation of blood flow
classified after 10 days
history of severe acute pain in the past
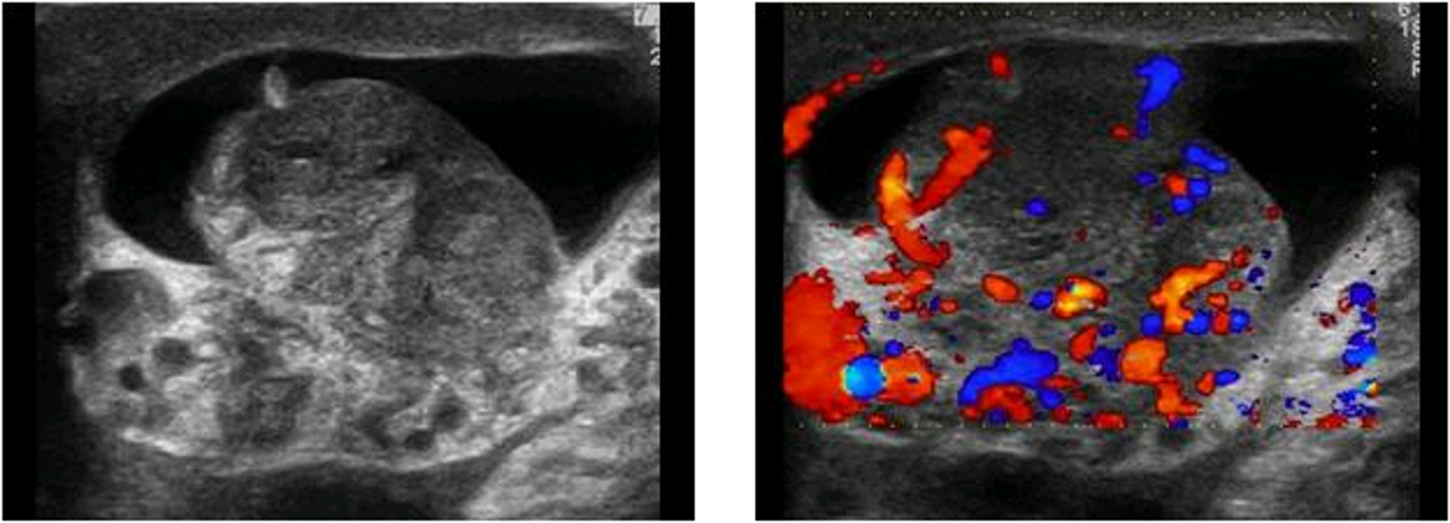
chronic torsion on ultrasound
Heterogeneous appearance of testes
Peripheral rim or normal appearing testicular tissue
Testicle atrophies (gets smaller) with the epididymis remaining enlarged and hyperechoic
chronic torsion on doppler
no blood flow
unable to obtain arterial and venous waveforms
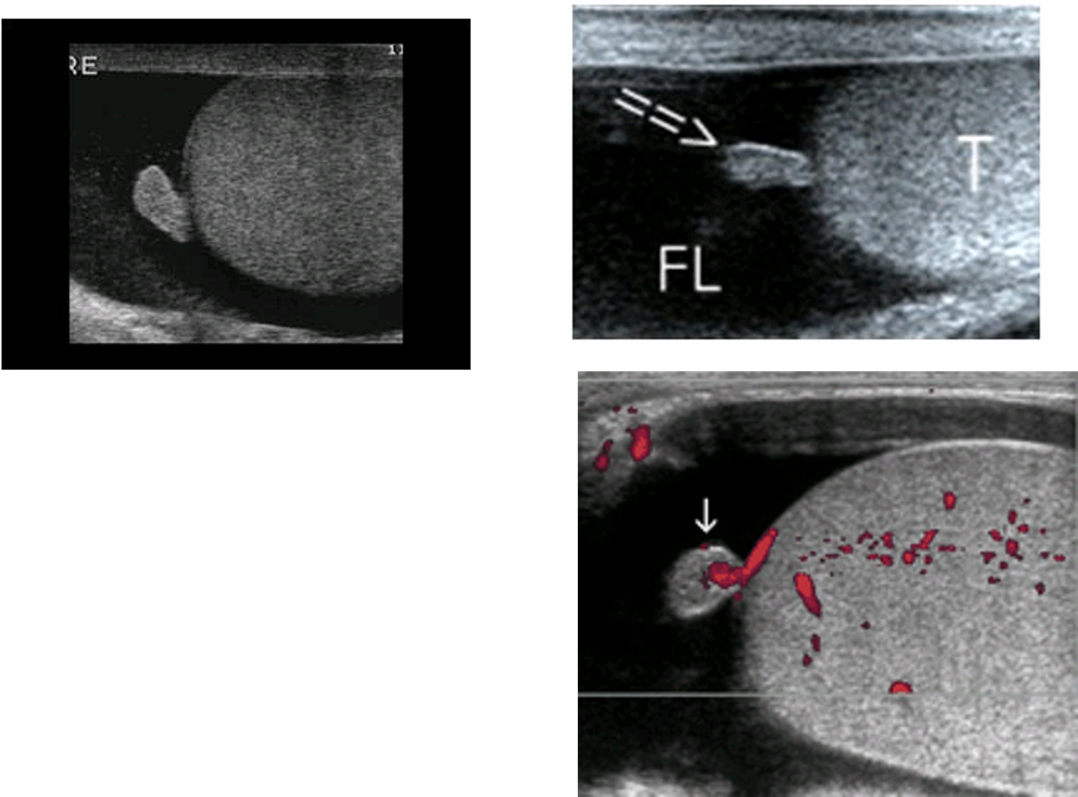
identify this pathology
enlarged epididymis and testicle with acute torsion
no blood flow visualized on color Doppler evaluation
identify this pathology
left: Heterogeneous testicle with peripheral normal appearing tissue consistent with chronic infarction
right: Inhomogeneous echotexture of testicle with chronic infarction
torsion-detorsion & partial torsion signs and symptoms
Acute and intermittent sharp testicular pain and scrotal swelling
Interspersed with long asymptomatic intervals
torsion-detorsion & partial torsion on ultrasound
During spontaneous detorsion, there is increased perfusion demonstrated as hypervascularity with low-resistance flow patterns within the testicles
Testis may be enlarged
Focal infarcts may or may not be present as hypoechoic areas
torsion of appendages etiology
Loss of blood supply to the appendix testis or appendix epididymis
Over 90% of torsed appendages involve appendix testis
Peak incidence between 7-14 years of age
torsion of appendages signs & symptoms
acute scrotal pain
mimics testicular torsion
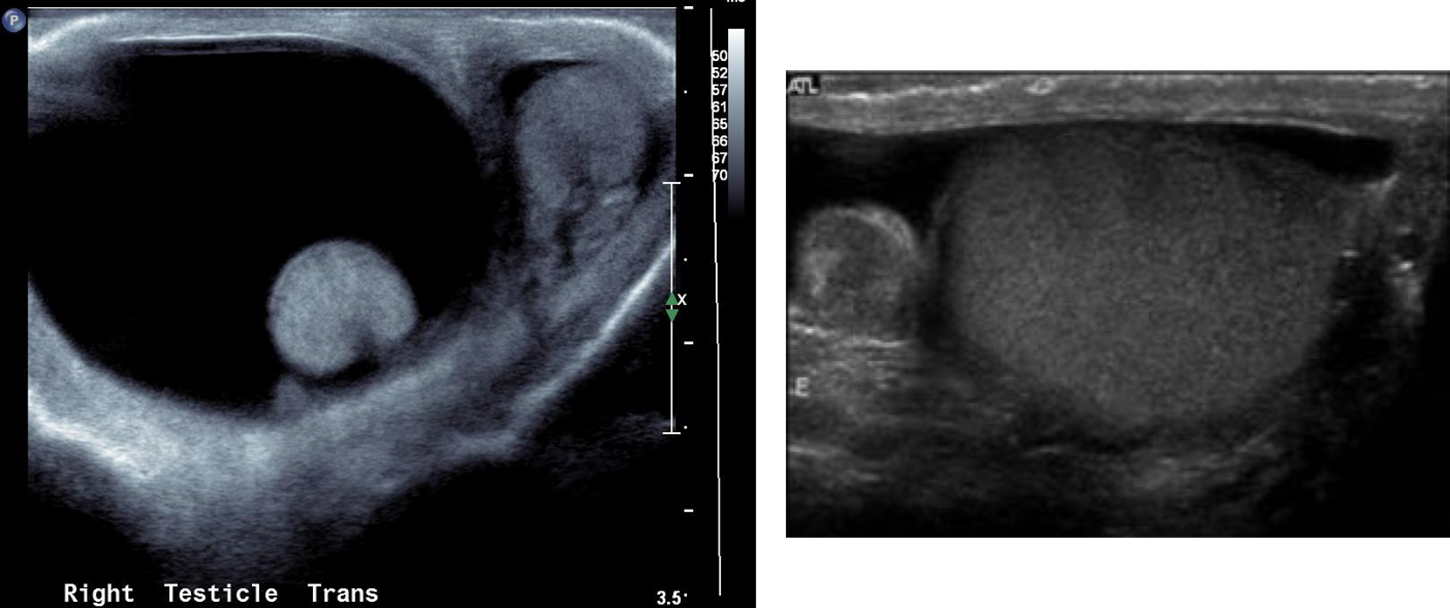
torsion of appendages on ultrasound
Testis is normal on color Doppler
Appearance of torsed appendage varies:
Large circular hyperechoic mass with central hypoechoic area
Enlarged circular heterogeneous mass adjacent to a normal testis or epididymis
Increased periappendiceal flow and absent central flow demonstrated on color Doppler
identify this pathology
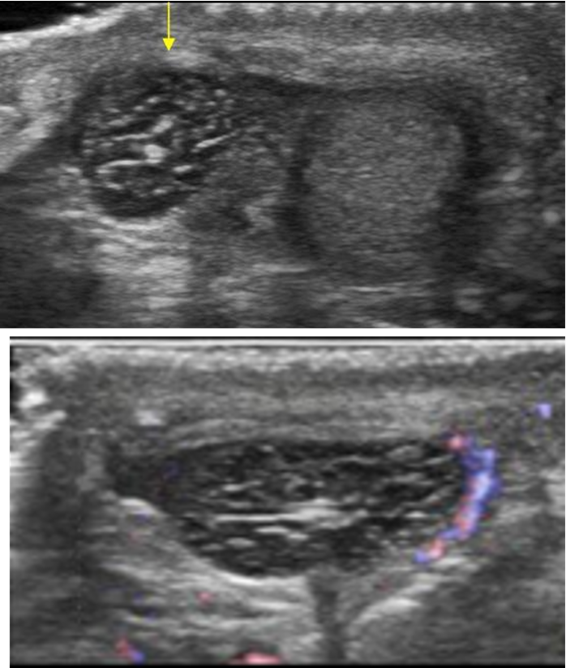
torsion of appendages
testicular rupture etiology
Rare
Occurs when the capsule, the tunica albuginea, is torn by trauma
Associated with athletic injuries, industrial, and motor vehicle accidents
testicular rupture on ultrasound
Contour abnormality due to irregular fibrous tunica albuginea
Extrusion of testicular contents into scrotal sac
Hematocele and hematoma may be present
Infarction of testicular contents
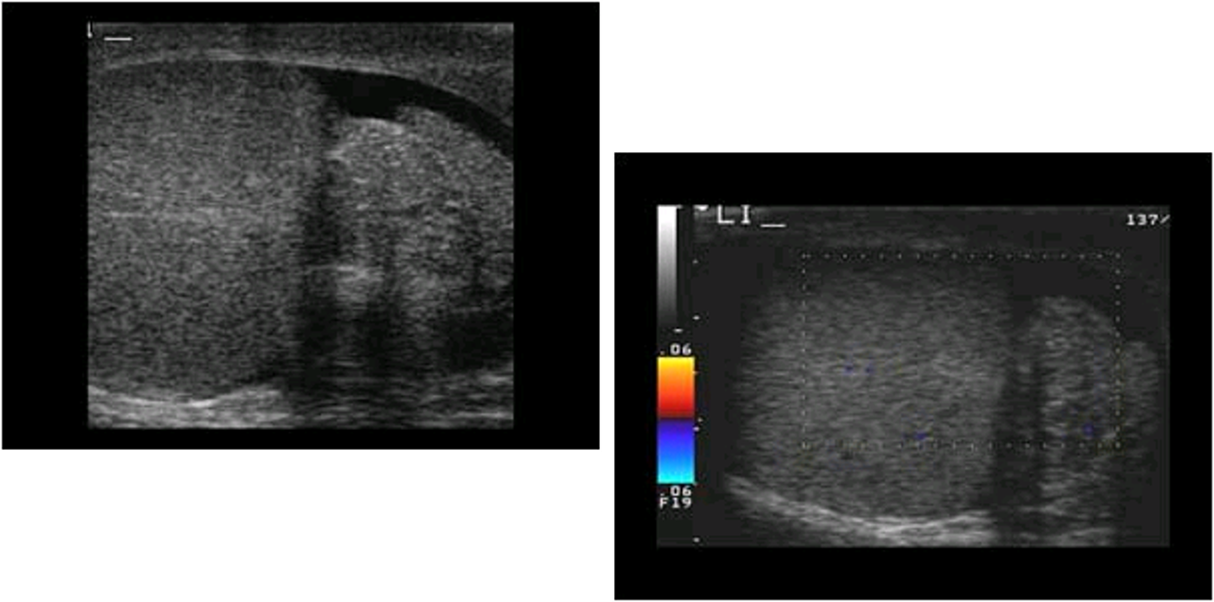
identify this pathology
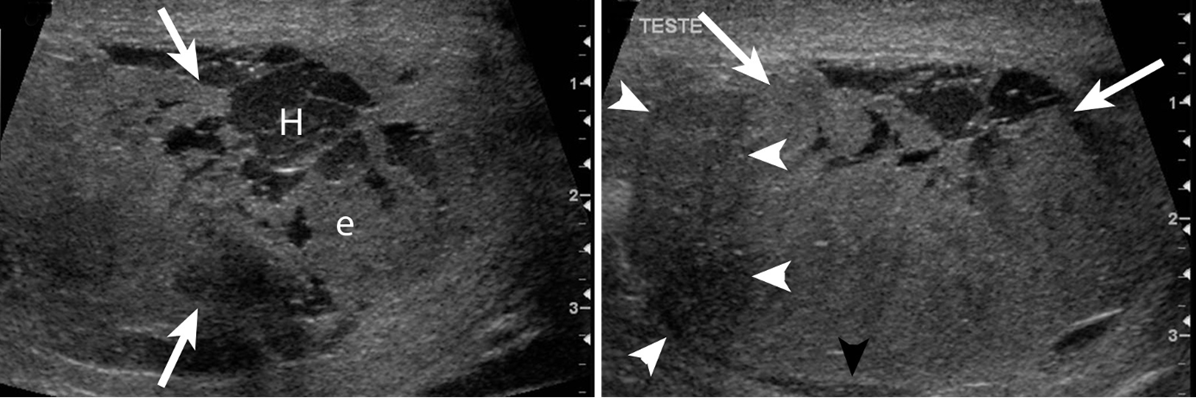
testicular rupture due to blunt trauma featuring a hematoma (left) and irregular contour of disruption of tunica albuginea (right)
epididymitis etiology
Most common cause of acute scrotal illness/pain
Caused by retrograde spread of bacterial infection from bladder or prostate
Associated with prostatitis
Sexually transmitted organisms including gonococci and Chlamydia are common causes in young men
epididymitis signs & symptoms
slight fever, chills, heavy sensation in affected testicle, testicle sensitivity to touch or pressure, enlargement of testicle, abdominal/pelvic pain, blood in urine, discharge from penis, painful ejaculation, burning sensation during urination, frequent urge to urinate
acute epididymitis on ultrasound
Enlarged, hypoechoic epididymis
Mainly involves head
Entire epididymis involved in 50% of cases
Hypoechoic areas are secondary to edema
Color Doppler may demonstrate increased flow in epididymis
chronic epididymitis on ultrasound
Thickened echogenic epididymis
May contain calcifications
what findings are more suggestive of an infectious process than a tumor?
swelling, epididymal abnormalities, skin thickening, and hydrocele
what is this pathology?
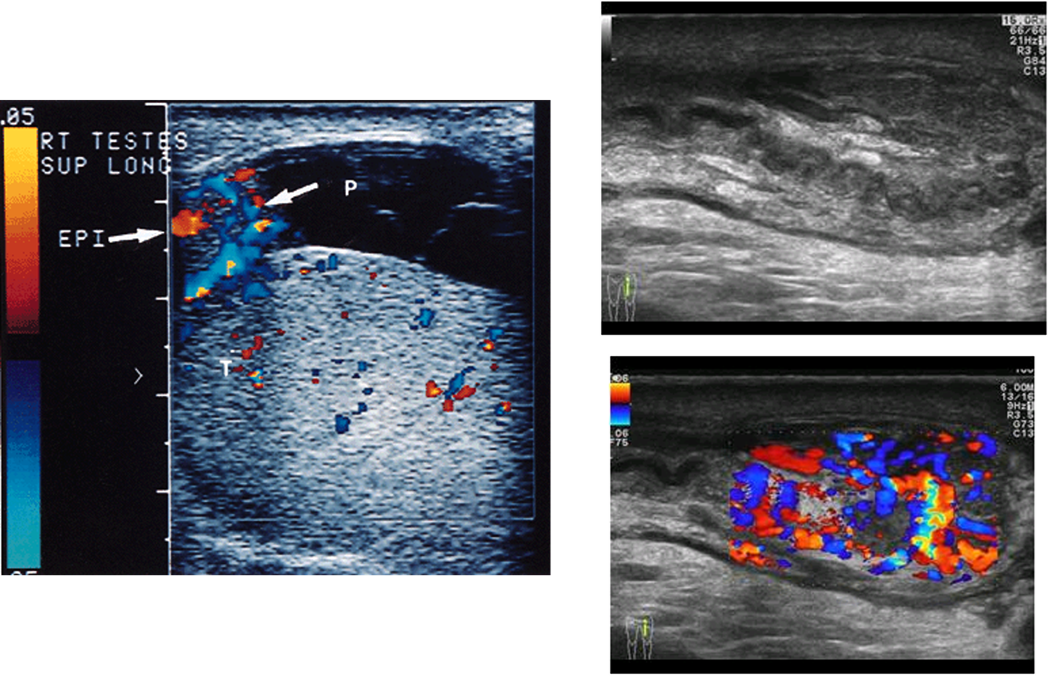
epididymitis
orchitis
Inflammation of testis due to trauma, metastases, mumps, or other (bacterial or viral) infection
orchitis etiology
Isolated orchitis is rare, usually occurs as secondary result of epididymitis
Can be focal or involve entire testicle
Neoplasm must be ruled out by serial US exams or surgery; if it persists, orchitis will resolve but neoplasm will not
orchitis signs & symptoms
Acute scrotal pain, with or without fever
See epididymitis
acute orchitis on ultrasound
Diffuse: decreased echogenicity and increased size
Focal: focal areas of decreased echogenicity
Doppler: Testicular hyperemia, increased number of blood vessels in affected area, increased venous flow in epididymis
chronic orchitis on ultrasound
Thickened tunica albuginea
Echogenic, thickened, irregular epididymis
Both may contain calcifications
Affected testis is smaller
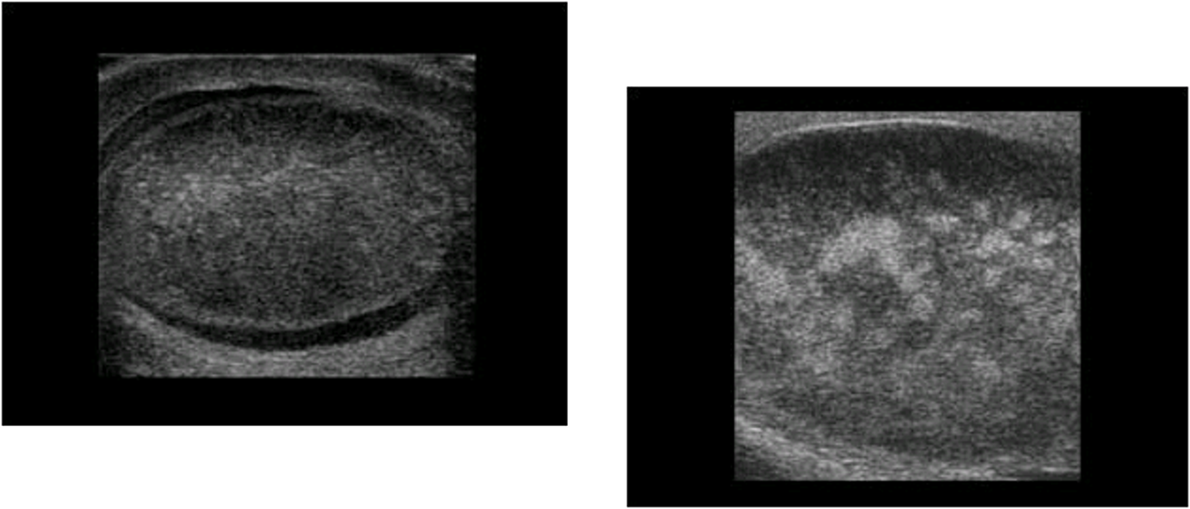
granulomatous orchitis
multiple focal hypoechoic lesions
identify this pathology
orchitis
epididymo-orchitis etiology
Inflammation of the testis and epididymis
20% of epididymitis involves the testis
Testicular involvement can be focal or diffuse
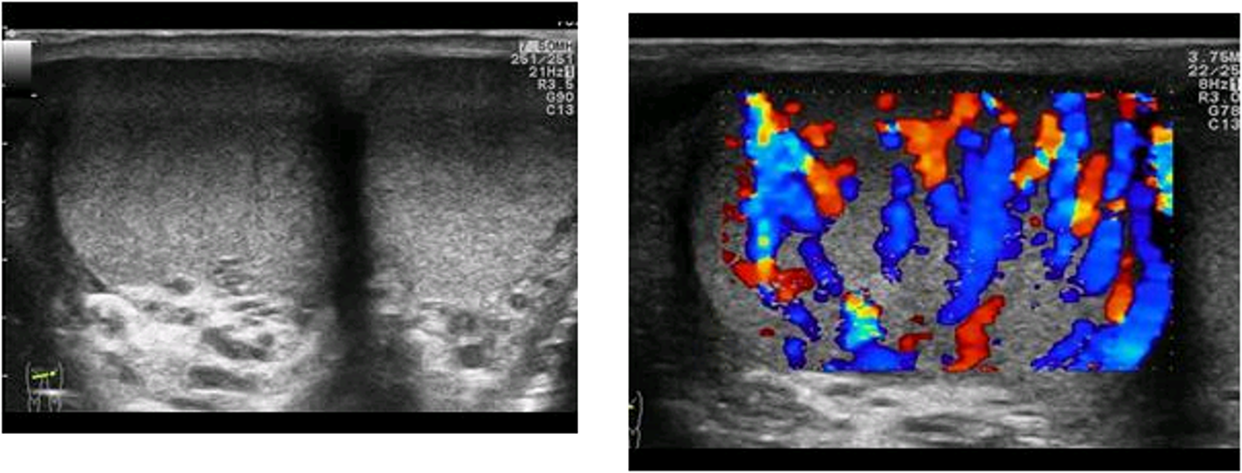
epididymo-orchitis on ultrasound
Hypoechoic area extended from epididymal region
Increased blood flow (hypervascularity) in affected testicle and epididymis
identify this pathology
epididymo-orchitis
what are the benign scrotal masses?
hydrocele, spermatoceles & epididymal cysts, tubular ectasia of rete testis, varicocele, scrotal hernia, scrotal abscess, scrotal hematoma, hematocele, pyocele, tunica albuginea cyst, benign neoplasms
hydrocele
Abnormal collection of serous fluid in potential space between the two layers of tunica vaginalis (between visceral and parietal layers)
hydrocele etiology
Most common cause of painless scrotal swelling
Congenital or acquired, often idiopathic or associated with epididymitis, torsion, trauma (25-50%)
Usually occur in anterior aspect of scrotum and displace testis posteriorly
hydrocele signs & symptoms
painless swelling of scrotum
scrotal mass
hydrocele on ultrasound
anechoic fluid collection
enhanced through transmission
typically surrounding the anterolateral aspects of testis
chronic ones can contain calcifications that produce posterior shadows
scrotal pearls etiology
AKA scrotoliths
Calcifications that often result from inflammatory deposits on the tunica vaginalis that have separated from the lining
May be single or multiple
scrotal pearls on ultrasound
Echogenic free-floating calculus outside testicle
Appear as echogenic foci between layers of tunica vaginalis
May produce posterior shadow depending on size
Visualization aided by presence of hydrocele