UT 505 Final Study Guide
1/43
Earn XP
Description and Tags
UT 505 - MSK
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Triangulate
Imaging in two perpendicular planes to determine location of FB
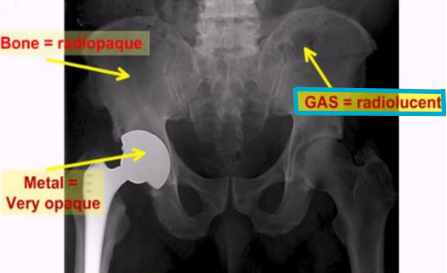
Radiopaque
FB or structure in which radiation cannot pass through easily
Blocks radiation → appears white/gray
Ex: metallic FB
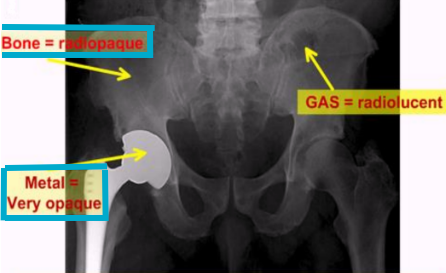
Radiolucent
FB or structure that allows radiation to pass through easily
Appears black or dark gray
Ex: air, soft tissue, abscesses, dental pulp
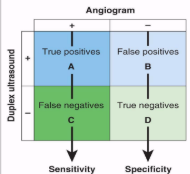
Specificity
How well an exam documents normal findings for people without disease or pathology
Exam’s ability to identify “normal” and confirms absence of disease
In vivo
Biological process that occurs within a living organism or natural setting
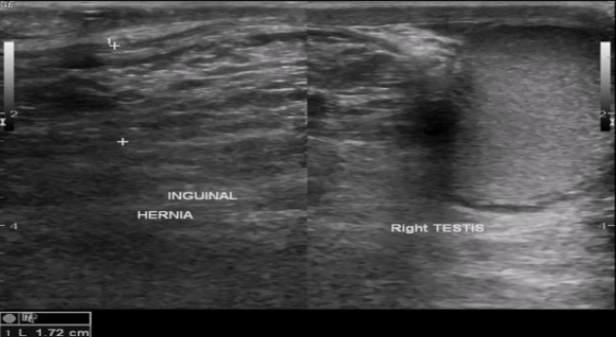
Strangulated hernia
Contents compressed → compromised blood supply → ischemia, necrosis, obstruction
Increased mortality & morbidity
US appearance
Thickened bowel wall, absent vascular flow, free fluid, no peristalsis
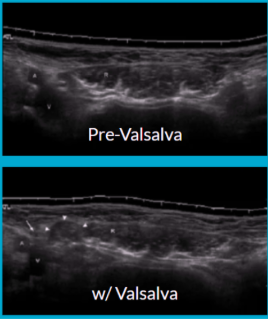
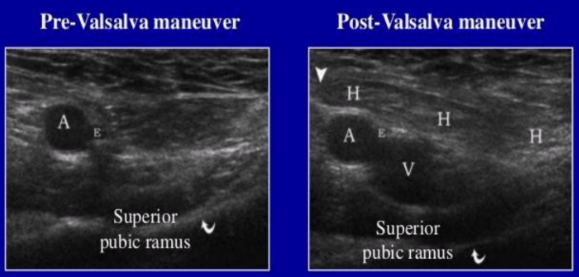
Valsalva maneuver
Increases intra-abdominal pressure
Have patients “bare down” like they’re preparing to take a punch to the abdomen
Contents move distally → hernia widens
Contents move back toward abdomen and sac narrows during relaxation
Key maneuver when looking for hernia due to dynamic study
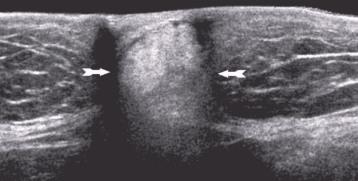
Lipoma
Most common benign tumor of abdominal wall
Fatty and benign
Soft, palpable, painless
US appearance:
Strongly echogenic - isoechoic
Difficult to distinguish from subcutaneous fat
Sarcoma
Malignant tumor of abdominal wall
Types: liposarcoma, rhabdomyosarcoma, fibrosarcoma
Limited clinical symptoms → very large upon discovery
Ultrasound appearance:
Hypoechoic or isoechoic to muscle
Heterogeneous
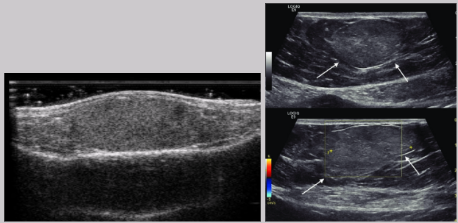
Hematoma
Collection of blood in tissue
Indication: trauma, pain, palp mass, ecchymosis, decreasing hematocrit
Can be uni or bilateral
US appearance:
Heterogeneous
Hypoechoic to hyperechoic
Fluid-fluid levels
Fluid can contain echogenic debris
Blood work is used to differentiate between hematomas and abscesses
T/F: hematomas and abscesses appear similarly on US
True
T/F: decreasing hematocrit is associated w/ hematoma formation
True
T/F: decreasing white blood cell count is associated w/ abscess formation
False
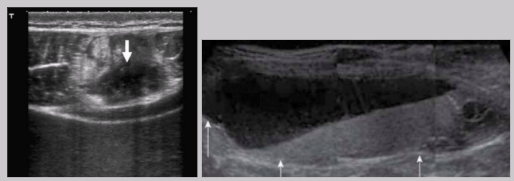
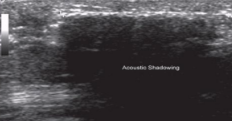
Acute phase of foreign body
Foreign body present < 3 days
Immediately after injury → air or dirty shadowing
24 hrs after injury → hypoechoic ring/halo develops
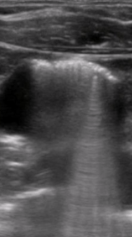
Intermediate phase of foreign body
Foreign body present 3 - 10 days
Fluid replaces air
Most pronounced hypoechoic halo
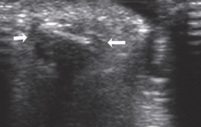
Chronic phase of foreign body
Foreign body present > 10 days
Dense granular material develops around FB
Inflammatory response → clean shadowing similar to bone
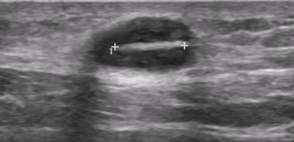
Organic foreign bodies
Made of biological plant material or animal products
Ex: thorns, wood, bee stinger, barb
Inorganic foreign bodies
Man-made products made of minerals
Ex: glass, gravel, plastic, pencil lead
Metallic foreign bodies
Products w/ metallic alloy
Ex: wires, needle, fish hook, etc.
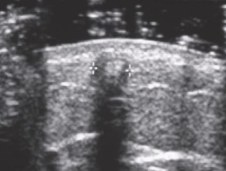
Clean shadowing
Caused by attenuation of an object
Ex: stones, metals, bone, needle
Dirty shadowing
Caused by refracting properties of gas bubbles or impedance of gas
Hernia
Protrusion of part/structure through the tissue normally containing it
Cause: anything that increases pressure in abdomen
Ex: obesity, heavy lifting, coughing, straining
Dynamic US study - diagnosis requires movement of hernia contents via Valsalva maneuver
Hernia characteristics
Reducible
Irreducible
Incarcerated
Strangulated
Reducible hernia
Hernia contents can be pushed back in w/ pressure
Irreducible hernia
Hernia contents cannot be pushed back in w/ pressure
Incarcerated hernia
Hernia is irreducible but still has vascularity
Strangulated hernia
Hernia is irreducible and has no vascularity
Parts of a hernia
Sac - consists of diverticulum of peritoneum
Sac covering - intestines, fat, omentum, etc.
Contents - layers of abdominal wall
Two main types of hernias
Ventral
Anterior and lateral abdominal wall
Types: umbilical, paraumbilical, epigastric, hypogastric, and incisional (subtype is parastomal)
Groin
Ilioinguinal crease and adjacent areas
Types: indirect inguinal, direct inguinal, femoral, and Spigelian
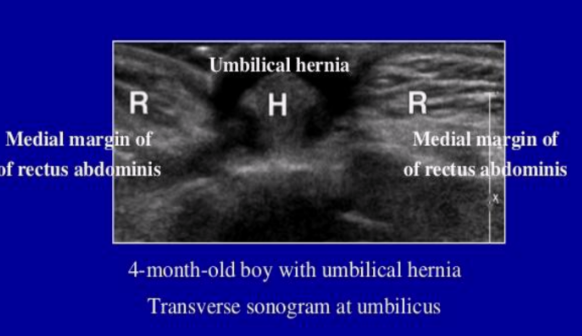
Umbilical hernia
Most common ventral hernia
Common in women and children
Epigastric hernia
Occurs in the linea alba above umbilicus
Hypogastric hernia
Occurs in the linea alba below umbilicus
Incisional hernia
Delayed complication from surgery
Most commonly occur due to vertical incisions
Subtype: parastomal
Complications of ventral hernias
Strangulation
Incarcerated or non-reducible
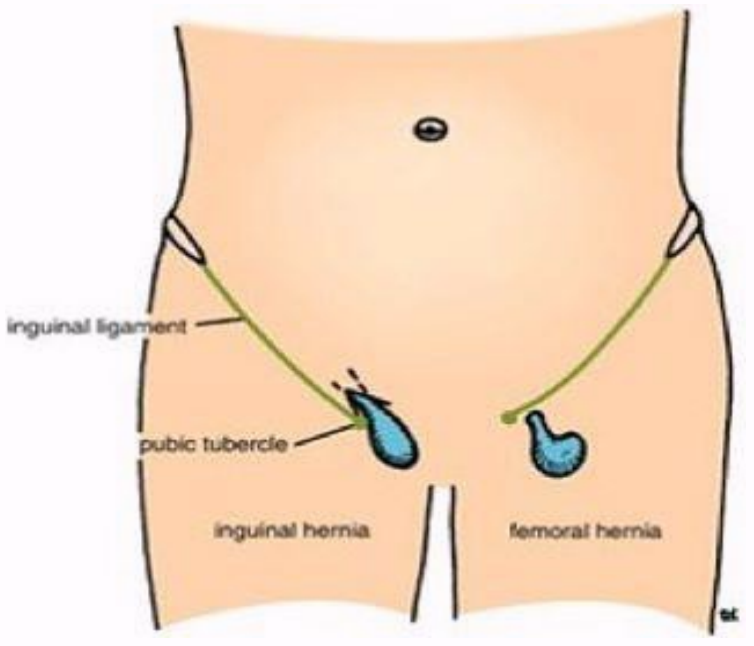
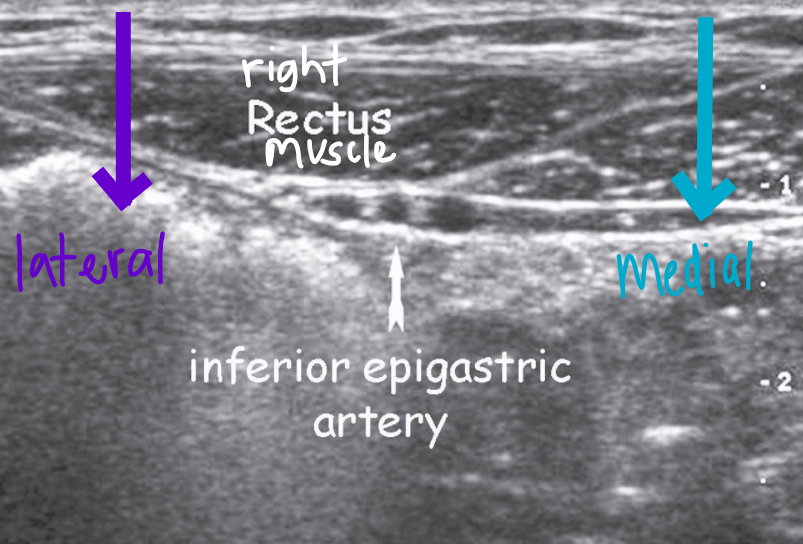
Inguinal hernias
Most common location for a hernia (~75% of all hernias)
Location: near internal inguinal ring, surrounding inferior epigastric vessels (IEV)
Medial to IEV: direct inguinal hernia
Lateral to IEV: indirect inguinal hernia
Direct inguinal hernia
Occurs medial to IEV
Acquired hernia
Affects elderly men w/ weakened transversalis fascia
Appear immediately when standing
Indirect inguinal hernia
Most common form of hernia
Occurs lateral to IEV
Congenital hernia
20x more common in men than women
Can extend into the scrotum in men and labia majora in women
More likely to become strangled than direct inguinal
⅓ are bilateral, but are more common on the right side if unilateral
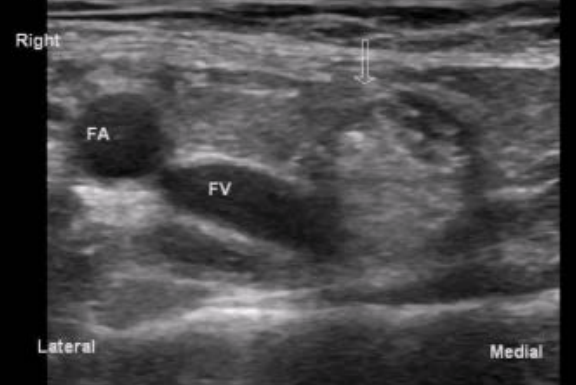
Femoral hernia
Protrusion of transversalis fascia - medial to CFV
More common in women (especially w/ pregnancy)
High risk of incarceration and strangulation
Because they are long w/ narrow neck
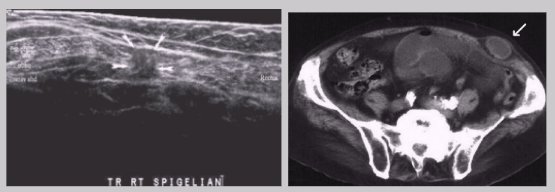
Spigelian hernia
Rare
Almost all occur at the inferior end of semicircular line, inferior to arcuate line where posterior sheath is absent
~ About 2 cm from the inguinal crease
High frequency of incarceration
Hard to diagnose because it occurs between the muscle or fascial layers of the wall rather than protruding through the wall
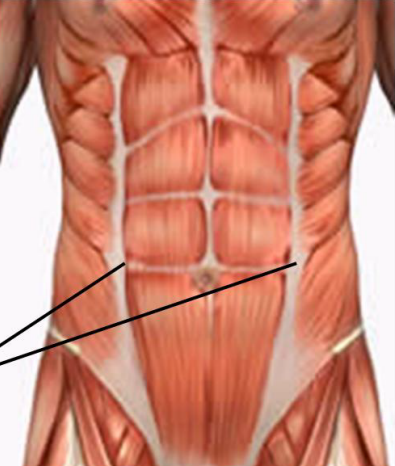
Linea semilunaris
Curved line on the ventral abdominal wall parallel to midline and halfway between side of the body that marks the lateral border of the rectus abdominis muscle
Abdominal wall complications after hernia repair surgery
Hematoma
Most common reason for abdominal lump after hernia repair
Abscess
Seroma
Recurrent hernia
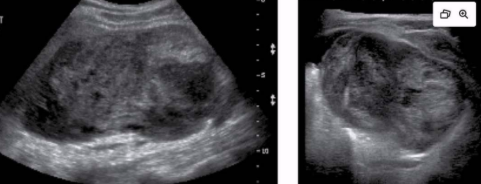
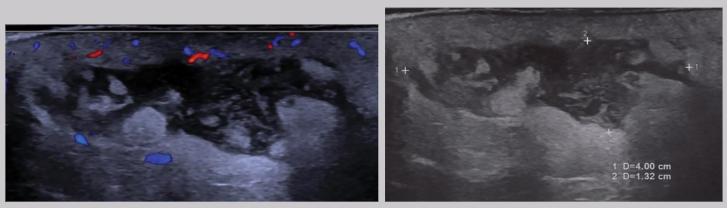
Abscess
Caused by cuts, scrapes, crushing injuries, surgical trauma, etc.
Abdominal wall abscesses are usually a surgical complication
Clinical presentation - redness, pain, swelling, elevated WBC (AKA leukocytosis)
US appearance:
Heterogeneous
Hypoechoic fluid w/ echogenic debris
Irregular borders
Posterior enhancement
Peripheral hypervascularity
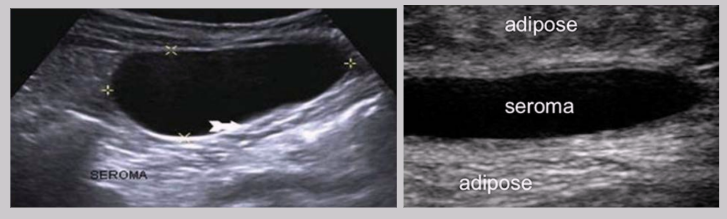
Seroma
Collection of serum in the tissue
Results from a surgical incision or liquefaction of a hematoma
Distinct from hematomas because they contain no red blood cells
US Findings:
Anechoic cystic structure
Well-circumscribed
Posterior enhancement
Scrotal hernia
Indirect inguinal hernia → can extend down to the scrotum