Steroids
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
Steroids do not have a mechanism for _____
Pain management
no analgesic properties
Steroids inhibits ______ pathways
clyclooxygenase
Lipoxygenase
Steroids have better ______ effects than NSAIDs
Anti-inflammatory
2 types of Steroids
Sex steroids
Corticosteroids
Types of Steroids - Sex steroids
Estrogen
Progesterone
Androgen (testosterone)
for sexual characteristics
Reproductive functions
Types of steroids - Corticosteroids
Mineralocorticoids
Glucocorticoids
fluids and electrolytes
Metabolism
Immune function
Sex steroids - estrogen + progesterone
Responsible for enlargement of breasts/hips, menstruation, ovulation (production of egg cells)
Sex steroids - Androgen
Responsible for the voice of males, bigger body mass, and bones, more hair growth, production of sperm cells
Corticosteroids - Mineralocorticoids
Fluids and electrolytes (sodium - potassium exchange in urine, electrolytes in the plasma and in the cell, amount of urine output)
Corticosteroids - Glucocorticoids
For metabolism and immune function
HPA Axis
Starts with the hypothalamus→ releases the corticotropin releasing hormone (CRH)→ stimulates the anterior pituitary gland→ releases adrenocorticotropic hormone (ACTH)→ stimulates the adrenal cortex lodged above the kidneys → releases cortisol
Controls and provides a list every year on the banned substances in sports
World Anti-Doping Administration
Cortisol
Naturally occurring in our body; controls our immune processes
If present in excessive amounts → sends negative feedback to stop the hypothalamus from releasing CRH and the anterior pituitary gland from releasing ACTH → decreased amount of cortisol
Cortisol: Immunosuppression
Decreased lymphocytes, eosinophils, monocytes, basophils
The immune response is suppressed
Increased RBC, neutrophils, platelets
AAS - Androgenic
enhance sexual characteristics
AAS - Anabolic
Increases muscle mass
AAS - Ergogenic
enhances sports performance
Evidence: AAS
Increase in muscle mass
Hypertrophy (increase in bulk)
Hyperplasia (increase in # of muscle cells)
Increase in strength
Enhanced calcium release from SR and/or increased calcium sensitivity of the contractile proteins
Anti catabolic effects
No breakdown is happening in the muscles
Endpoints (size and strength) are enhanced by training
Not allowed to take steroids without training
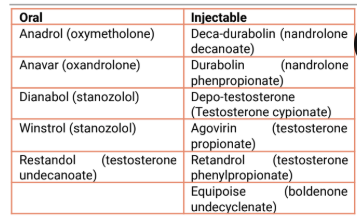
Examples of AAS
Which athletes use AAS?
contact sports
Body builders
Adverse Effects - Cardiovascular
increased LDL
Decreases HDL
Hypertension
Elevated triglycerides
Atherosclerotic heart disease
Adverse Effects - Male reproductive
testicular atrophy
Gynecomastia
Impaired spermatogenesis
Altered libido
Male pattern baldness
Adverse Effects - Reproductive Female
menstrual dysfunction
Altered
Clitoral enlargement
Deepening of the voice
Male pattern baldness
Adverse Effects - Hepatic
elevated liver enzymes
Jaundice
Hepatic tumors
Peliosis hepatis
Adverse Effects - Endocrine
altered glucose tolerance
Decreased FSH, LH
Acne
Adverse Effect - MSK
premature epiphyseal closure
Tendon degeneration
Adverse Effects - CNS
mood swings
Violent behavior
Depression
Psychosis
Irreversible Adverse effects of AAS
atherosclerotic heart disease
Male pattern baldness
Clitoral enlargement
Deepening of voice
Hepatic tumors
Peliosis hepatis
Premature epiphyseal closure
Tendon degeneration (??)
AAS - Is gynecomastia reversible?
Possible
Direct Measures of AAS
Gas chromatography - mass spectrometry
Liquid chromatography - mass spectrometry
Metabolites may be present up to 30 days depending on agent, dose, route
Why are steroids prohibited in sporting events
Competitive advancement, inc performance - cheating
Tested by blood or urine
Adverse health effects
In the long run, heart attack can happen
If found positive = strip of medals, suspended (depends on federation)
Therapeutic-use exemptions
E.g. asthma
Even if tested positive = exempted, no sanctions will be given
Cortisol physiologic effects - list
Increase in blood glucose / increase in liver glycogen
Anti-inflammatory
Immunosuppression
Enhances sodium and water reabsorption
Behavioral and mood changes
Cortisol - Increase in Blood Glucose / Liver Glycogen
Increase in Liver
Protein synthesis
Glycogen synthesis
Glycogen storage
Gluconeogenesis
Makes sure that you have enough blood sugar in the system
Other tissues
Increase in uptake and utilization of glucose
Increased Lipolysis
Increased Proteolysis
Increased fat deposition in abdominal adipose tissue
Cortisol - Anti-inflammatory
Inhibits eicosanoids biosynthesis
Inhibits chemotaxins
Stabilizes lysosomes
Cells responsible for the immune/inflammatory response
Allows lesser cells to attack the area of inflammation
Vasoconstriction
Vasodilation: ↑ blood/cells in the area = ↑ swelling, redness, warmth
Vasoconstriction = limiting inflammatory response
Inhibits both the cyclooxygenase and lipoxygenase pathways
Leukotrienes are also inhibited
Steroids have better anti-inflammatory properties because they inhibit both pathways
NSAIDs only target the cyclooxygenase pathway
Cortisol - Immunisuppression
Decreased lymphocytes, eosinophils, monocytes, basophils
The immune response is suppressed
Increased RBC, neutrophils, platelets
Routes - List
Topical
Inhalational
Oral
IV
Injection
Epidural
Routes - Topical
Simple mosquito bites, psoriasis, skin allergies, eczema, etc.
Eye drops for conjunctivitis
Too much inflammation, too much redness
Routes - Inhalational
Inhaled steroids are given if bronchodilators aren’t effective in addressing the bronchoconstriction for wheezing
Routes - Oral
E.g. prednisone, dexamethasone, and methylprednisolone
Some steroids prescribed to patients
Any anti-inflammatory management
Severe OA
Chronic diseases not responsive to topical (e.g. eczema and psoriasis)
Cancer (as part of the chemotherapeutic management)
If topical is not working, you can shift to oral.
Routes - IV
If pt cannot tolerate oral routes or refused to drink and the patient needs to be admitted to the hospital
E.g. methylprednisolone, dexamethasone
Can also be given IM
IV is preferred for less incidence
Routes - Injection
Inject steroids in joints
Shoulder inflammation (e.g. adhesive capsulitis, rotator cuff syndrome)
Knees (e.g. torn ligaments, chronic/severe OA)
Can use US to identify structure
Routes - Epidural
E.g. for chronic low back pain
Done under x-ray, image intensifier
See exact level of the vertebra
Adverse Effects - Cushing’s Syndrome
Centripetal/Truncal Obesity- fat deposition is on the trunk/abdomen
Moon facie (cheek/face enlargement)
Buffalo hump (fat on the back)
Hyperglycemia (↑ blood sugar)
Hypertension (↑ blood pressure)
Cardiac hypertrophy (heart enlargement)
Adrenal: hyperplasia and tumor formation
Muscle wasting (weakness and thin extremities)
Thinning of scalp hair
Increased facial hair
Osteoporosis
Striae of the skin- skin becomes stretched out forming striae
Acne
Adrenocortical Suppression is caused by?
Prolonged steroid use leading to the hypothalamus and pituitary gland to stop secreting.
If there are high levels of cortisol in the blood → signals the hypothalamus and pituitary gland to stop secreting
Adrenocortical Suppression - Effects
Anorexia (loss of appetite)
Nausea/vomiting
Nausea - feel of vomiting
Vomiting - the actual expulsion of gastric contents
Weight loss (d/t muscle loss)
Lethargy (inactive, feeling lazy and sleepy)
Headache
Fever
Muscle and joint pains
Postural hypotension (when assuming the upright position from supine, they are not able to tolerate changes in position
If patient already benefited from steroids →
gradually decrease the dose (do not abruptly stop the treatment)
E.g. 50 mg 2x/day → 50 mg q morning for 2 wks → 25 mg q other day for 2 wks
Allows the hypothalamic-pituitary axis to recover
Takes a while to recover
Adverse Effects of Chronic Steroid use - Catabolism
Muscle wasting
Muscle weakness
Osteoporosis
Vertebral compression fractures (common)
Adverse Effects of Corticosteroids - Ulcers
Peptic ulcers (irritant to the gastric mucosa)
Give antacids and proton pump inhibitors along with steroids to prevent gastric irritation or peptic ulcers
Proton pump inhibitors will aid in preventing the secretion of excessive gastric juices
Adverse Effects of Corticosteroids - Infections
Increased susceptibility to infections
Ex: when you see cancer pts, they are wearing masks because they are immunosuppressed
Reverse isolation
Adverse Effects of Corticosteroids - Growth
Growth retardation especially in children who were given steroids before their growth spurt.
Premature closure of long bones (epiphysis)→ inhibits ideal height
Adverse Effects of Corticosteroids - Eyes
Glaucoma, cataracts
Increased pressure in the eye that can lead to blindness
Adverse Effects of Corticosteroids - Mood
Nervousness, mood swings, psychosis (behavioral changes)
Nervous, jittery, irritable
Mood swings - happy and the next moment, they are sad; part of the imbalance of hormones
Adverse Effects of Corticosteroids - Psychosis
Psychosis - extreme; have both delusions, and hallucinations
Delusions of grandeur - you feel as though you are the best
Delusion of persecution - worse behavioral effect of steroids; nobody likes you
Steroid Preparations - Biologic Half-Life
Different from elimination half-life
Certain amount of steroids is still left after stopping the medication, exerting its biological effect
Focused on how long the half-life will still be
Steroid Preparations - Short Acting
Biologic half-life = 8-12 hrs
Cortisol (Cortef, Hydrocortone)
Cortisone (Cortone)
Not on how fast they are eliminated but on how long the half-life will still be
Steroid Preparations - Intermediate Acting
Biologic half-life = 12-36 hrs
Prednisone (Prednisone, Decortisyl)
Prednisolone (Histacort)
6-Methyprednisolone (Solumedrol)
Triamcinolone (Kenacort, Ledercort)
Steroid Preparations - Long Acting
Biologic half-life = 36-72 hrs
Paramethasone (Haldrone)
Betamethasone (Celestamine, Betnovate)
Dexamethasone (Oradexone, Decilone, Maxitrol)
Neuropathic pain
Neuropathic pain - pathologic type of pain where there is damage to the spinal cord, nerve roots, peripheral nerves, sensory pathways, nociceptive pathways
Adjuncts for Neuropathic pain - Tricyclic Antidepressants
Amitriptyline
Increases descending inhibitory signals in the spinal cord
The DHC has descending signals that can regulate the release of nociceptive impulses → where the action of these antidepressants happen
(Amitriptyline + Chlordiazepoxide) Limbitrol
Anticholinergic side effects
Tachycardia
Drying of the secretion
Tricyclic Antidepressants - Anti-cholinergic side effects
Drowsiness
Dry mouth
E.g. pt asks to drink again
Blurring of vision (secondary to the pupillary vasodilation)
Constipation
Difficulty in urinating
Weight gain
Adjuncts for Neuropathic pain - Anticonvulsants
For seizures (epilepsy)
Membrane stabilizers
Able to stabilize the neuronal membranes so that it prevents the transmission of nociceptive impulses.
Pregabalin (Lyrica)
Carbamazepine (Tegretol)
Na Valproate (Epilim)
Gabapentin (Neurontin)
Mostly prescribed nowadays
Anticonvulsants side effects
Fatigue
Stomach upset/discomfort
Dizziness
Blurring of vision
May be prone to falls or accidents if you ask them to do an activity alone
Important to note these side effects to know when to defer physical therapy.