New parameters for diastology power point 1
1/134
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
135 Terms
In healthy hearts, most of the blood flow into the left ventricle occurs during when? from the passive what?
Early diastole filling from the passive “PULL” of the left ventricle as it relaxes and expands (that is our E wave of our transmitral inflow)
if the LV is relaxing normally, you will expect it to?
Relax and expand quickly
pulls the blood from the LA to the LV
When diastolic dysfunction is present the LV no longer what?
The LV no longer pulls that blood, it is pushed from the LA
what are the parameters to assess for normal and abnormal diastolic function?
Ventricular relaxation
Myocardium chamber compliance
filling pressures - LAP and LVP
LV filling pressure is going to be equal to?
Mean left atrial pressure (LAP) = and this is from our E/e’ ratio= LV pre - A pressure
When we are looking at diastolic dysfunction that when there is elevated left atrial pressure it is associated with ?
Elevated left ventricular end diastolic pressure
We can also have elevated LVEDP but our LAP may be normal, where would this information comes from ?
comes from our A velocities of our transmitral inflow, our pulmonary veins, Our AR to A duration and our pump strain of our left atrium
what will Echocardiography allows us to evaluate?
LV filling patterns, myocardial motion, and LA filling patterns
Diastology assessment.
The guidelines starts with clinical data including?
Age
Heart rate
underlying rhythm
Blood pressure
As we age what happens to the performance of our LV
LV becomes less compliant.
Echo data includes Two-dimensional (2D) and Doppler echocardiographic finding for?
LV volumes and wall thickness, ejection fraction (EF), LA volumes, and presence and severity of mitral valve disease
(then we will use specific date for Diastology assessment)
LV diastolic function Grading and LAP Estimation, what are the 3 positive parameters
Reduced e’ velocity: septal <_6 or lateral <_7 or average <_6.5 cm/s
Increased E/e’: septal >_15 or lateral >-13 or average >-14
Increased TR velocity >_2.8 m/s or PASP >_35 mm Hg
what’s the yellow box include in cases where we cannot use the chart
MAC, MR, MS
Atrial Fibrillation
LVAD
Non-cardiac PH
HTX
Pericardial constriction
The first three parameters that we use to assess diastology come from where
Come from our E prime, which is our TDI and an E to E prime ratio and our TR velocity
the next step is we’re going to use what paramters to help us deduce whether it’s normal or we have diastolic dysfunction present
supplemental parameters
what are the parameters
Primary, Additional, supplementary
what does the primary Doppler include
(e’ (TDI), E/e’, TR Velocity)
Transmirtal inflow
Mitral Anuuli TDIs
TR peak velocity and right atrial pressure estimation- PASP estimate
what does the Additional include
PulVn Inflow, LAVI, LARS, IVRT
what does supplementary include
PREDv, L-wave (our transmirtral inflow) , Ar-A dur (this is using our pulmonary veins and our transmirtral inflow), Valsalva
For transmitral Inflow what view do we use and for our PW doppler sample volume to be what size and placed where?
Use A4C with color for alignment
PW doppler sample volume (1-3 mm) placed at MV leaflet tips
what are the transmitral inflow measurements
Peak E- wave velocity (cm/s): peak early diastolic modal velocity after ECG T wave
Deceleration time (ms): time interval from peak E-wave velocity along the deceleration slope to the zero baseline
Peak A -wave velocity (cm/s); peak late disastolic modal velocity after ECG P wave
E/A ratio: peak E-wave velocity divided by peak A-wave velocity
+- A duration (ms) time interval from the onset to the end of the A-wave signal
for normal diastology we that sucker type of phenomenon happening, so with this most of the blood flow moving from the LA to the LV should happen during our what velocity?
E velocity
A normal E to A wave duration is what?
greater than or equal to 0.8 (our E velocity is greater than our A) velocity
The A wave should only contribute about what % of blood flow into the LV
20%
Normal Diastolic function for Age
Normal young subjects, what are you expected to see
Myocardial relaxation is swift
Most filling during early diastole
Small atrial contraction contribution
with our mitral inflow for a young person, we do expect our E and A velocity be what?
E velocity to be very tall and our A velocity to be normal
As we age, what do we see with our E velocity and A velocity
E velocity will drop and the A wave does contribute a little bit more
Then as we get even older what happens with our E and A velocity
Our E velocity will drop more and the majority of the filling will be coming from the A wave velocity
Normal Diastolic function for age,
With age and NL LA pressure what happens with the myocardial relaxation and of elastic recoil
A gradual decrease rate of myocardial relaxation and of elastic recoil
Normal Diastolic function for age,
With age and NL LA pressure what happens with the LV pressure decline
Slower LV pressure decline (but it doesn’t necessarily mean there’s going to be diastolic dysfunction we need to make sure we look at our other parameters and use our numbers and our flow chart to call diastolic dysfunction)
Normal Diastolic function for age,
With age and NL LA pressure what happens with the
Slower LV pressure decline…. include
Later MV opening, decreased E velocity
Changes equalization or pressure between LA and LV (longer DT)
Increased dependence on atrial contribution (increased A velocity)
what age does E velocity approaches A velocity
Age 65
what Age does E/A ratio Usually <1.0
age 70 and older
TDI a mitral Annulus (Annular Tissue Doppler imaging)
what view do you want to use? where do you want to use TDI? what should be our gate size?
Apical four chamber with TDI
Septal annulus and Lateral annulus
we increase our gate size from 5 to 10 millimeters
TDI and mitral Annulus measurements what are they?
e’ velocity (cm/s): peak early diastolic modal velocity after ECG T-wave
a’ velocity (cm/s): peak late diastolic modal velocity after ECG P-wave
MV E/e’: MV peak E - wave divided by the TDI e’ velocity
Average E/e’: MV peak E-wave divided by the average of the TDI septal e’ and lateral e’ velocities
what is our TDI looking at?
our myocardial motion, we look at our LV compliance and how well it moves and that shows us if diastolic dysfunction is present
what is the normal muscle movement for our E prime velocity (TDI) (value)
greater than or equal to 8 cm/s (centimeters per second)
If your E prime parameters quality is poor and unable to get a clean crisp signal you can use your what?
Lateral E prime and also E to e prime ratio
Mitral annular e’ velocity values for diagnosis of impaired LV relaxation (diastolic dysfunction is present) what are values for a 20-39 year old
Septal e’ cm/s <7
lateral e’ cm/s <10
Average e’ cm/s <9
Mitral annular e’ velocity values for diagnosis of impaired LV relaxation (diastolic dysfunction is present) what are values for a 40-65 year old
Septal e’ cm/s <6
lateral e’ cm/s <8
Average e’ cm/s <7
Mitral annular e’ velocity values for diagnosis of impaired LV relaxation (diastolic dysfunction is present) what are values for a >65 year old
Septal e’ cm/s <6
lateral e’ cm/s <7
Average e’ cm/s <6.5
Tissue doppler imaging TDI Limitations most of it comes from?
regional wall motion abnormalities (especially in our inferior septal wall or the anterior septal wall) - the motion will be affected so may not get a true TDI E prime velocity
what are other Tissue doppler imaging TDI Limitations?
Mitral annular calcification, or any sort of surgical rings or prosthetics… CAD, regional dysfunction in the sampled segments, pericardial disease - why? this will affect the motion the myocardial motion therefore our TDI may not be accurate. since we need to sample both the septal and lateral, but again diastology parameters will change in the presence of of these things
what ratio has been found to be fairly sensitive in evaluating the degree ot diastolic dysfunction?
E/e’ ratio
what does a higher the e’ on septal or lateral tell us
the higher the e’ the better diastolic function / muscle relaxation, so when we perform E'/e’ it should be lower ratio
The LOWER the E/e’ ratio is what does tell us?
The Lower the E/e’ ratio the better the diastolic function
A patient with Normal Diastolic Function should have an E/e’ ratio of what
less then or equal to 8
(Tricuspid regurgitation) peak TR signal
acquired from what view
what should we pay attention to when we are looking at our peak TR signal is the absence of ?
Acquired from any view
Absence of Pulmonary disease (if pulmonary disease is present that suggest also an elevated LAP)
what are the positive parameters for TR and PASP
Increased TR velocity greater than or equal to 2.8 m/s or PASP greater than or equal to 35 mmHg - diastolic dysfunction is present
An age-related difference when we’re looking at our RAP is when we have a dilated IVC that measures greater than 2.1 and may demonstrate or may not demonstrate collapsibility but we have a young healthy individual between 20 and 39 that RAP estimate would be what?
3 mmHg (make sure to look at our other parameters which are e ‘ and our E/e’ ratio to say that diastolic dysfunction is not present)
Additional doppler for diastology what are the positive parameters include ?
S/D ratio (our ratio our systolic to diastolic waveforms in our pulmonary veins looking at the pattern) less than or equal to 0.67
LARS less than or equal to 18%
LAVi greater than or equal to 34 mL/m2
IVRT less than or equal to 70 ms
these parameters are very important in a LAP estimation)
Pulmonary veins, the atrium serves as a “conduit” for flow from the ?
venous circulation to the ventricle
Elevations in ventricular diastolic pressures will be reflected in where
elevated pressures in the atrium (going to see this in pulmonary vein flow)
what would a normal pulmonary vein waveform look like
systolic that is higher than the diastolic and there is atrial reversal flow that we typically see with the atrial kick
for pulmonary veins what should the sample volume gate size be?
where can it be placed ?
sample volume gate size be 3 and 5 mm
can be placed into either the right Upper PV or right lower PV just past roof or the atria
what measurements are needed for the pulmonary veins
The peak S -wave velocity (cm/s): peak systolic velocity at ECG T wave
when two systolic peaks (S1 and S2) the peak S2 should be measured for the S/D ratio
Peak D-wave velocity (cm/s) peak early diastolic velocity after ECG T wave
S/D ratio: peak S - wave velocity divided by peak D - wave velocity
+- peak AR velocity (cm/s): peak late disastolic velocity after ECG P wave
+- AR duration (ms): time interval from the onset to the offset of the Ar-wave signal at zero baseline
pulmonary veins
the S wave is what to the D wave in normal adults
the S-wave velocity is influenced by changes in the what?
D-wave velocity is mainly influenced by what
decreases in LA compliance and increase in LAP is associated with?
ARev velocity >35 cm/s indiactes what?
The S wave is greater than or equal to the D wave in normal adults
S-wave velocity is influenced by changes in LAP, LA contractility, and LV and RV contractility
D-wave velocity is mainly influenced by early diastolic LV filling and compliance, and it changes in parallel with mitral E velocity
decreases in LA compliance and increase in LAP is associated with decrease in S velocity and increase in D velocity
decreases in LA compliance and increase in LAP is associated with decreae in A velocity and increase in D velocity
ARev velocity >35 cm/s indiactes an increased LVEDP
where is when you will a lot of problems getting a nice pulmonary vein in?
ICU patients because they’re on BIPAP and supine so its really hard to see
for Pulmonary veins if a patients has A FIB what will be absent
atrial reversal wave will be absent
the pulmonary veins measurement is really reliable in patients with
LV systolic dysfunction
pulmonary veins
in patients with normal left ventricular ejection fraction, what will be our ratio be
can be greater than 0.67 despite elevated filling pressures - so although this is an additional parameter for us we still need to perform another one which will be the IVRT to show whether there is diastolic dysfunction present
what is our caveat for the pulmonary veins
age related changes with pulmonary veins - in a normal healthy young individual around up 30 years of age you will see the S wave lower than the D wave this is showing excellent elastic recoil of the ventricle and its going to fill a very large volume of blood during diastole
LA volume the volume reflects what over time?
A volume reflects the cumulative effects of increased LVEDP over time
(if your LA volume is enlarged you most likely have elevated LAP which then correlated to elevated left ventricular end diastolic pressure)
LA volume
increased LA volume is an independent predictor of what (clincle indications)
death, heart failure, A-Fib, and ischemic stroke
LA Volume
we can visualize the LA diameter from which view to see if its enlarged if it reaches what then its dilated
PLAX, 4cm
we can compare the left atrium diameter to the what and how do we know if we have dilatation
to our aortic root and again if its larger than the aortic root we have dilatation
The LA can enlarge without diastolic dysfunction in high output states like what
Heart transplant patients, A-fib, a flutter, significant MV disease and even in well trained athletes
LA Strain
Left atrial strain in diastolic function primarily focused on?
LARS shows a direct correlation with what?
LARS worsens as what and inversely related to what?
The lower the LARS, the higher the?
The LA reservoir strain
LARS shows a direct correlation with the degree of diastolic dysfunction (LARS worsens as the degree of diastolic dysfunction worsens) and is inversely related to LVEDP
The lower the LARS, the higher the LVFP (LVEDP)
What are the steps/how do we perform Left Atrial Reservoir strain (LARS), requires and dedicated what? where would you place the caliper?
We need a dedicated software package; we can’t use LV strain and pull it down on the LA strain it must be a dedicated LA package (very easy to perform and reproducible) Place a caliper at the septal annulus inside the LA and place another caliper on lateral wall annulus and then one at the roof of atrai and then the machine does its work and thats how we are able to get a left atrial strain
Ap4 chamber only needed
peak + ve strain during ventricular systole
what is the % for the LA strain
should be greater than 18%
LA strain reduces when?
when the LAP is elevated (so less then 18%)
LARS dependent on?
LV systolic function (may be normal despite elevated LVFP in pt with normal EF and GLS)
Left atrial strain age related changes we can expect Lars to?
Decrease naturally with age
LARS should not be used to assess LV filling pressure in patients with?
A -fib, significant MR, heart transplant, LA stunning
(normal EF/GLS >18% - LARS abnormal less then or equal to 18%)
Also for LARS avoid performing when interatrial septum is
Hypermobile
For LARS can use only one view if poor image quality and what do we not want include
apical 4 chamber view otherwise we want to do a biplane of our four and two chamber and sure we have high frame rate
fossa ovalis, the left atrial appendage or any pulmonary vein
how should the normal LA strain pattern look like
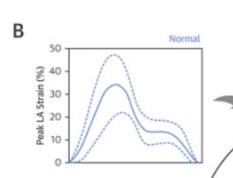
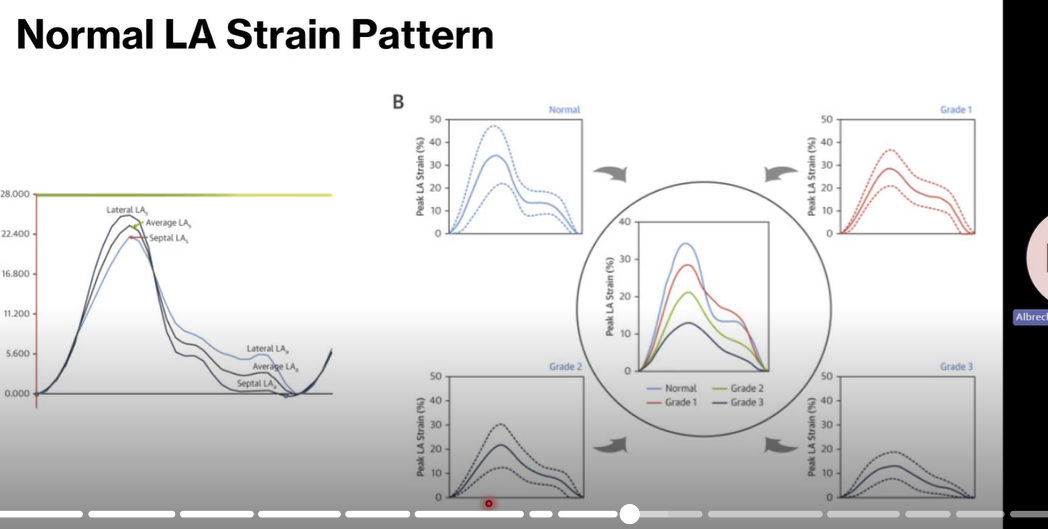
which one is normal
B its tall, normal in peak LA strain between 30 and 40
abnormal the velocities decrease shown in grade 2 and 3
grade 1-3 strain pattern reduces
LA strain pattern
the lower the strain
the higher the left atrial pressure
Left atrial pump strain (conduit function) measures the ?
The active contraction of the LA during late diastole, reflecting (a-wave velocity)
LA pump strain which is inversely related to?
LVEDP
Low LA pump strain signals?
Increased LV filling pressures (diastolic dysfunction)
IVRT what views is it performed at?
what doppler must be used?
where would your doppler be placed?
we need a ___wall filter and a very ___ sweep speed?
want tp make sure that the aortic valve ___ ___ is showing and clear onset of the what opening
what is the timing measurement
Apical 3 or 5 chamber view
CW
the anterior MV leaflet and the aortic valve
low wall filter and a very high sweep speed
aortic valve closing click and mitral valve opening
closing of the aortic valve to the MVO
IVRT what is the measurement that it will tell us we have diastolic dysfunction
IVRT less than or equal to70 ms
IVRT measurement is directly related to? and inversely related to?
How the LV is relaxed and inversely related to LAP
In pt with impaired LV relaxation and normal LVEPs (>___ms) what happens to the IVRT, and what grade is this?
our IVRT is prolonged
Grade one and it will be greater than 110 milliseconds
when we have increased LAP whats happens to the IVRT
The IVRT is going to decrease in time <70 milliseconds (ms)
The IVRT is highly specific for what?
for elevated LAP in pt with cardiac disease
for Supplementary parameters what are you required to have
primary and Additional parameters
what are the + parameters for Supplementary
PREDv greater then or equal to 2 m/s
PADP greater than or equal to 16 mmHg
L-wave greater than or equal to 50 cm/s
Ar-A dur greater than 30 ms
decrease in E/A ration greater than or equal to 50% with valsalva
PR end - diastolic velocity where do you measure
what are you determining
peak velocity measurement at end - diastole , its at the peak velocity on out PR signal
PA end diastolic pressure (PAEDP= 4 X (PRED PR velocity)2+RAP) thats why we get a pressure value
PREDv
this signal can be used when we are not able to get a TR signal, and in the absence of Pulmonary disease our end - diastolic pressure approximates our?
Mean LAP (backwards flow) - if we have elevated PA End diastolic pressure then we have elevated mean LAP, if we have elevated LAP we have diastolic dysfunction
L wave velocities what are we looking for? what flow
That mid diastolic flow that happens during diastasis
for L wave velocities how is this waveform appear
if pressures are elevated thats when this waveform appears
L wave velocities we can aslo see this L wave in our TDI trace that will be between where
the e’ and a ‘ velocities
L wave signal is specific for?
elevated pressures
L wave velocities limitations
may be seen with normal LV diastolic function on a rare occasion when the subject has
the velocity is usually? whats abnormal
Bradycardia
<40 cm/s normal
greater or equal to 50 cm/s is abnormal
Ar- A duration how/where is the doppler performed?
AR duration from pulmonary veins and the transmitral inflow and we will use the timing from the onset of the A wave to the end of the A wave
Ar -A duration the time difference between duration of PV flow atrial reversal and mitral inflow during atrial contraction is associated with?
LVEDP
AR-A duration the longer the time difference the?
The higher LVEDP