Gastric Acid Disorders Patho
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
gastric pits
there are millions of these in the lining of the GI tract that lead to the gastric glands that produce gastric juice
g cells
cell type that secretes gastrin
parietal cells
cell type that secretes gastric acid
proton pump
hydrogen-potassium pump located on the surface of parietal cells
hydrogen
the parietal cell proton pump moves one of those ions OUT of the cell into the stomach lumen
potassium
the parietal cell proton pump moves one of these ions INTO the cell
concentration gradient
the parietal cell proton pump moves potassium and hydrogen ions against their…
chloride
this ion enters the parietal cell to form HCl with hydrogen
gastrin, acetylchloine, histamine
these 3 hormones stimulate acid secretion
h2
histamine receptor on the surface of parietal cells
g protein coupled
type of receptor that the h2 receptor is
h2 receptor
the cellular response of this receptor is translocation of proton pumps to the plasma membrane → dec pH of stomach lumen
h+ secretion
when the cellular response occurs from h2 receptor, this is the mechanism BY WHICH pH decreases
acid disorders
these result from an imbalance of aggressive/damaging (or potentially damaging) factors and mucosal defense/protective factors
mucosal barrier
maintaing the integrity of this in the gastric environment is the key to avoiding damage from acid
tight junctions
this feature between epithelial cells prevents HCl from leaking into underlying tissue
HCO3
component of mucosal barrier fluid (mucus) that neutralizes stomach acid
mucin
protein in mucus that helps it perform its functions
GERD
symptomatic condition or histologic change associated with retrograde movement of gastric contents to esophagus
PUD
gastritis, erosions, and ulcers of the GI tract that requires gastric acid for their formation
duodenum
more common site of peptic ulcers
lower esophageal sphincter
most commonly, GERD is caused by incompetency of this feature
pressure
when the LES in incompetent, this is reduced and when stomach pressure exceeds LES pressure the contents will come up
hiatal hernia
a risk factor for GERD where the stomach bulges up into the chest through the hiatus of the diaphragm
peppermint
a food that can often trigger GERD in sensitive patients
barretts esophagus
a sequelae of more severe GERD that involves metaplasia of stratified squamous cells into columnar and goblet cells
adenocarcinoma
barretts esophagus cellsare more likely to develop into this condition
PUD
injury to the mucosa of the stomach that can range from slight injury to severe ulceration and bleeding
helicobacter pylori
bacteria that is the most common cause of PUD
smoking
increases the risk of developing PUD
flagella
feature of h. pylori that help it move below the mucosal surface to coloize the gastric epithelium
mucous layer
h pylori can cause PUD by disrupting this layer, neutralizing pH, and releasing enzymes and toxins
urease
enzyme that converts urea to CO2 and ammonia, which neutralizes the acid and can injure/irritate the mucosa
gastric cancer
h pylori is also associated with this condition because it inhibits apoptosis of gastric pit cells and encourages chronic inflammation
cagA
toxin produced by h pylori that can degrade p53 proteins that normally suppress protein
de-gelling
this is required before the h pylori can move further and cause damage to gastric epithelium
endoscopy
gold standard for diagnosing h pylori infection
breath test
another method of detecting h pylori infection that is less invasive
co13 and co12 ratio
isotopes used to detect presence of h pylori in breath
neutrophils
NSAIDS can increase adherence of these to the vascular endothelium, causing more ROS damage
COX-1 and COX-2
NSAIDs inhibit these, which therefore also inhibit several beneficial prostaglandins
arachidonic acid cascade
NSAIDs inhibit prostaglandins that are produced in this process
corticosteroids
combination of this medication class with NSAIDs can make a patient more susceptible to PUD
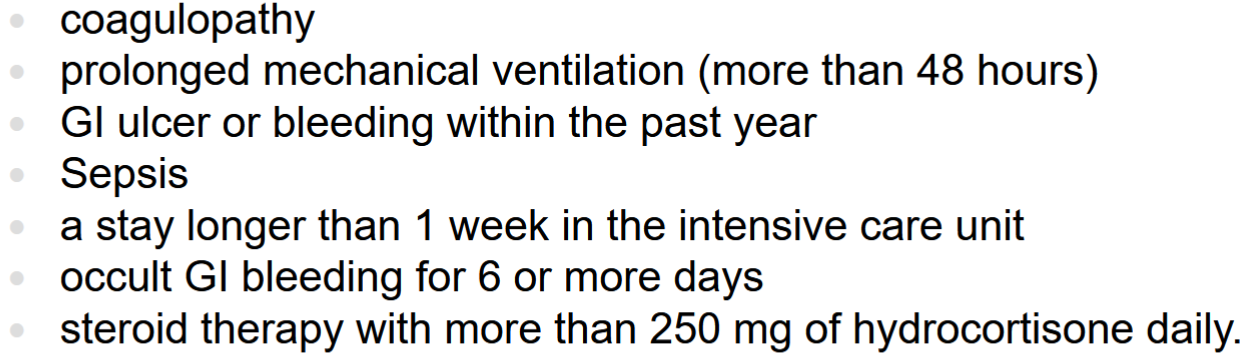
stress ulcer prophylaxis
the use of medications to prevent peptic ulcers while a patient is in the hospital
no
do all patients need stress ulcer prophylaxis
epigastric pain
main symptom of PUD
stomach
ulcer type where pain is aggravated by food
duodenum
ulcer type where pain is relieved by food
alarm symptoms
present in patients with chronic PUD, can indicate need for emergency care
alarm symptoms
these include: bleeding (melena or hematemesis), perforation (Radiating pain to back), obstruction (vomiting, abdominal distention)