Looks like no one added any tags here yet for you.
Parvovirus
Small, non-enveloped linear ssDNA virus
Mechanism:
Tropism for erythrocyte P Ag:
immature adult erythroid progenitor cells
placental trophoblasts, fetal liver, heart and myoblasts cells
Virus replicates in S-phase in rapidly dividing cells, causing S-phase arrest and cell death, reducing functional RBC
Clinical Findings:
Fever, Chills, HA, Myalgias, Rash, Arthralgia
Decreased Reticulocytes, HgB
Diseases:
Fifth Disease (Erythema Infectiosum)
Normal children: Low grade fever and malaise followed by rash during 2nd week
Rash seen first on cheeks, then progresses to reticular rash on trunk and limbs
Rash is result of Immune complexes that form after viral clearing
Arthropathy
Normal adults (+/- rash)
50% have transient arthralgia/arthritis, usually women
Acute “RA-like” arthritis
Symmetric joint stiffness
Mostly in small joints (wrists, hands, feet)
Diagnosis: B-19 antibodies in plasma
Transient Aplastic Crisis
In patients with increased destruction of rbc and corresponding increased production, B19 infects the rbc precursors and results in a loss of rbcs
Decreased erythropoiesis with severe anemia in patients with:
Sickle cell, thalassemia, anemia, malaria
Thrombocytopenia, neutropenia, pancytopenia
Persistent Anemia
Immunodeficient/Immunocompromised
Persistent infection because no Ab
Viruses aren’t cleared and continue infecting premature rbc
Hydrops Fetalis
Transplacental transmission from infected mother (may or may not have had mild cold symptoms)
Miscarriage and/or hydrops fetalis
2nd trimester highest risk
30% risk of infection if mother infected
5-9% fetal loss
Presentation
Fluid accumulation in fetus
From severe anemia, possible myocarditis
Diagnosed on ultrasound
For all cases, 50%-90% fatality
10-20% of cases due to B19
Congenital Anemia
Adenovirus
Naked, ds linear, Icosahedral virus with its own DNA-dependent-DNA polymerase
Attributes:
> 60 serotype, 7 subgroups (A-G)
3 vaccines for military against serotypes 4,7, delivered in a coated capsule
Transmission via respiratory droplets, fecal oral route, direct contact, fomites and cervical secretions during birth
Pathogenesis:
Replicates in dividing epithelial cells and kills
Immune evasion-interfere with MHC/peptide surface expression which results in decreased T cell recognition
Immunocompromised
more severe disease
Viremia spreads to kidneys, bladder, lymphatic system and causes inflammation
Pneumonia
Can remain in lymph nodes for 6-18 months
Shed virus (even if carrier is not overtly sick)
Clinical Presentation:
Accounts for 10% of acute febrile illness in the under 2 population
Acute Respiratory Distress (ARDs) in military recruits
Diseases:
Exudative pharyngitis
Occasionally progresses to pneumonia or Acute Respiratory Disease
In late winter, spring
#1 cause of infectious conjunctivitis
swimmer’s conjunctivitis from improperly maintained pools
#2 cause of diarrhea/gastroenteritis in kids
Watery, non-bloody diarrhea, nausea, vomiting, cramps
Summer
Daycares
Diagnosis
PCR or cell culture followed by Ab testing for epidemiology purposes
Human Papillomavirus
naked icosahedral, circular dsDNA viruses
Uses host DNA polymerases in nucleus
Attributes:
> 250 genotypes
Plantar, cutaneous, flat, genital and palmar warts
Asymptomatic/unknown infections in which HPV remains dormant are common
Transmission:
Viruses on wart surfaces transmitted by skin-skin contact
Breaks in skin/mucus membranes necessary for spread
Cutaneous warts don’t spread easily
Mucus membranes more conducive
sex causes microlesions in skin/efficient transfer
Possible vertical transfer
Pathogenesis:
Produced by low- and high-risk genotypes and needed for life cycle
Cells stimulated to enter S phase by E5, E6, E7
E5: binds EGF, stimulates mitosis, inhibits apoptosis
E6: degrades p53, blocks apoptosis
E7: inhibits RB, prevents cell cycle arrest
Persistent HPV infection can lead to cancer
Invasive cervical, intraepithelial neoplasia, anal, penile, oropharyngeal
DNA replication stress from entering cell cycle aberrantly - chromosome numerical and structural instabilities
E6 and E7 expression is deregulated leading to over-expression without productive virion production
HPV genome integrates into host cell DNA at unstable loci
Clinical Presentation:
Diseases:
Common Cutaneous Warts
HPV2, HPV4
Flat Warts
HPV 3, HPV 10
Plantar and Palmar Warts
HPV 1, HPV 4
Anogenital Warts, Cervical Papillomas, Penile Warts, Respiratory Papillomatosis
High Risk Cancer Genotypes: 16, 18, 31, 33, 45, 52, 58
16, 18, 31, 33, 45: 75% squamous cell carcinoma and 94% of all adenocarcinomas
Low Risk Cancer Genotypes: 6, 11
6, 11: 90% of genital warts
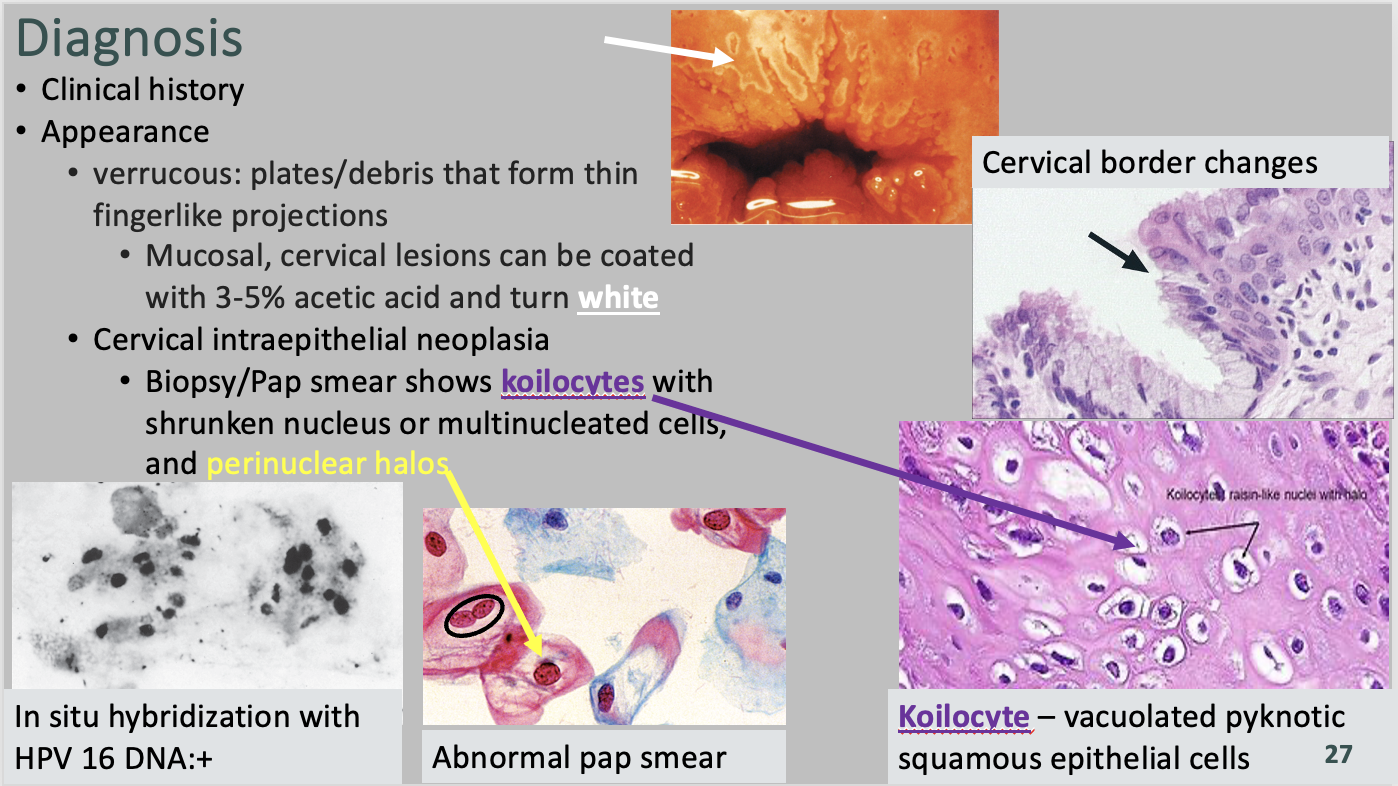
Diagnosis/Treatment
Verrucous: plates/debris that form thin fingerlike projections
Mucosal, cervical lesions can be coated with 3-5% acetic acid and turn white
Cervical intraepithelial neoplasia
Biopsy/Pap smear shows koilocytes with shrunken nucleus or multinucleated cells, and perinuclear halos
Vaccine
Gardasil 9, FDA licensed
Recombinant major capsid protein L1 (virus like particles)
Prevents infection: types 6, 11, 16, 18, 31, 33, 45, 52, 58
Recommended at 11-12, 13-26, 27-45
Polymavirus (John Cunningham)
nonenveloped, circular, dsDNA, icosahedral
Clinical Presentation:
Targets Immunocompromised
Diseases:
Progressive Multifocal Leukoencephalopathy (PML)
Impaired memory, confusion, neurological signs (hemiparesis, visual impairment, coordination issues)
Diagnosis/Treatment:
MRI/CT-white matter lesions, demyelination
Reduce immune suppression
Death 3-6 months after onset
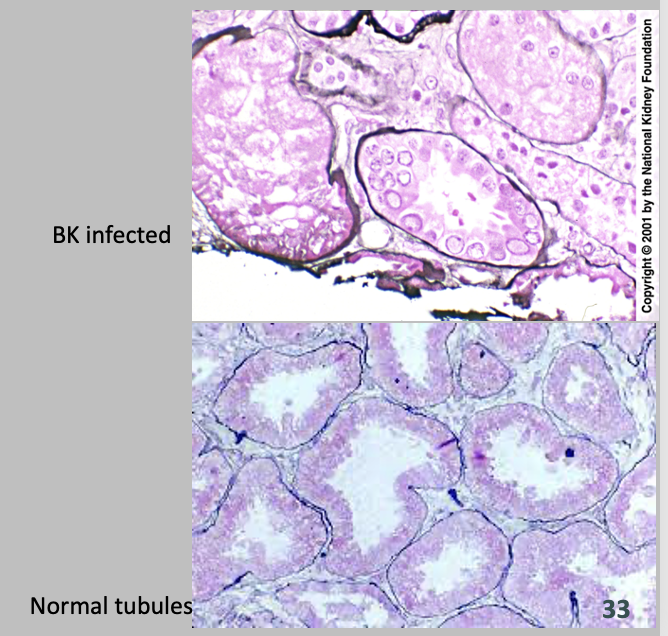
Polymavirus (BK)
nonenveloped, circular, dsDNA, icosahedral
Clinical Presentation:
Associated with kidney, bone marrow transplants, immunocompromised
Slow progressive rise in BUN and Creatinine
Diseases:
Hemorrhagic Cystitis
HSV 1
Enveloped, dsDNA virus
Attributes:
Has a primary, latency, and recurrence period
Latent Infection: Virus penetrates skin and replicates. It then enter the cutaneous neurons and migrates to a ganglion where it remains in a latent state.
Reactivation: Virus can subsequently be reactivated and travel through sensory neurons to the epidermis. A recurrent infection results.
Pathogenesis:
Spread via direct contact with lesions (oral sex)
Cell-cell spread locally, including multinucleated giant cells of skin/mucus membranes
Causes clustered, painful, fluid-filled infectious vesicles
Clinical Presentation:
Oral Sex transmission
Diseases:
“Cold Sores” - Herpes Labialis
Painful grouped vesicles-scalloped border
Vesicles to pustules to erosions to ulcers
Gingivostomatitis
on gingiva and mucosa
primarily in children
Fever, oral lesions, irritability
Lesions: yellow, perioral, vesicular lesions that crust over
Herpetic Whitlow (Finger)
Herpes Meningitis/Encephalitis
Rare, HSV1 most common cause of sporadic fatal disease
primary or reactivated infection
*necrosis of one temporal lobe-CT and MRI/best diagnostic tool
Herpes Keratoconjunctivitis
Corneal ulcers in conjunctival epithelium
#1 for infectious blindness in developed countries
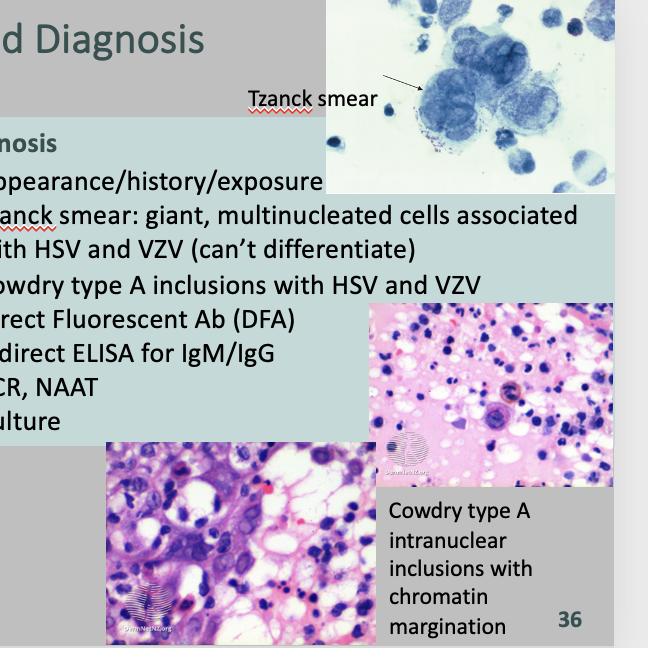
Diagnosis/Treatment
Appearance/history/exposure
Tzanck smear: giant, multinucleated cells associated with HSV and VZV (can’t differentiate)
Cowdry type A inclusions with HSV and VZV
Direct Fluorescent Ab (DFA)
Indirect ELISA for IgM/IgG
PCR, NAAT
Culture
Acyclovir: guanine analog
Used for encephalitis, neonatal, disseminated infections
(immunocompromised)
Famciclovir: prodrug metabolized in infected cells only to penciclovir
Not a cure-only works on replicating viruses not latent ones
Reduce shedding and recurrences
HSV 2
Enveloped, dsDNA virus
Attributes:
Transmission via sex, oral sex, childbirth
Pathogenesis:
Spread via direct contact with lesions (oral sex)
Cell-cell spread locally, including multinucleated giant cells of skin/mucus membranes
Causes clustered, painful, fluid-filled infectious vesicles
Clinical Presentation:
Primary infection includes fever and inguinal lymphadenopathy but recurrence does not
Diseases:
“Cold Sores” - Herpes Labialis
Painful grouped vesicles-scalloped border
Vesicles to pustules to erosions to ulcers
Gingivostomatitis
on gingiva and mucosa
primarily in children
Fever, oral lesions, irritability
Lesions: yellow, perioral, vesicular lesions that crust over
Herpetic Whitlow (Finger)
Herpes Meningitis/Encephalitis
Rare, HSV1 most common cause of sporadic fatal disease
primary or reactivated infection
*necrosis of one temporal lobe-CT and MRI/best diagnostic tool
Herpes Keratoconjunctivitis
Corneal ulcers in conjunctival epithelium
#1 for infectious blindness in developed countries
Neonatal Herpes
contact during vaginal birth, prevented by C-section
asymptomatic to skin, eye, mouth and body-wide vesicles; to encephalitis w/ permanent neurological damage or death
Diagnosis/Treatment
Acyclovir: guanine analog
Used for encephalitis, neonatal, disseminated infections
(immunocompromised)
Famciclovir: prodrug metabolized in infected cells only to penciclovir
Not a cure-only works on replicating viruses not latent ones
Reduce shedding and recurrences
HSV3/VZV
Enveloped, dsDNA virus
Attributes:
Virus eliminated except for latent in ganglia-leads to shingles
Diseases:
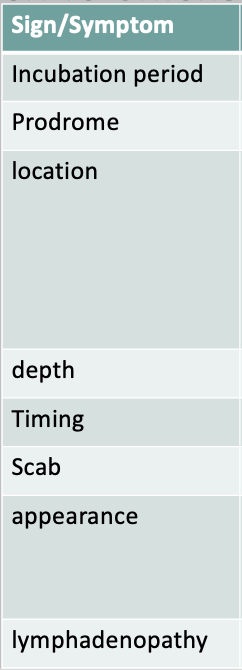
Chicken Pox (Children)
Mild, highly contagious
10-21 day incubation period
No viral prodrome/fever
Asynchronous vesicular rash occurs on face, trunk, lesions blister, crust, itch
Infectious until all lesions crusted over
Chicken Pox (Adults)
1° infection severe
Pneumonia, Liver failure, encephalitis, scarring
Shingles
Re-activation of latent VZV
Vesicles erupt along a dermatome-on skin along areas innervated by a particular dorsal root ganglion
Lesions identical to varicella zoster
Can lead to disseminated infections, post-herpetic neuralgia, Ramsay Hunt Syndrome
Diagnosis/Treatment
Direct fluorescent Ag
PCR
Tzanck smear
Varicella (Chickenpox Vaccine)
1st: 12-15mo
2nd: 4-6yrs
Zoster Vaccine
HSV 4
Enveloped, dsDNA virus
Attributes:
Two types, 1 (A), 2 (B)
Lifelong, latent infection
95% world infected
In immunocompromised patients with syphilis, syphilis can reactivate latent mono
Pathogenesis:
Immunocompetent: Ab and T cells keep EBV under control; T cells kill EBV-infected B cells
Splenic rupture
Immunocompromised: loss of T cells lets EBV-infected B cells proliferate
EBV in B cells for life
Clinical Presentation:
Developing countries
“Mono Rash”
If misdiagnosed and prescribed amoxicillin for Strep Throat--
Diffuse maculopapular rash…after about a week
Diseases:
Infectious Mononucleosis
Pharyngitis, fatigue, malaise, photophobia, sore throat, atypical white blood cells
Nasopharyngeal Carcinoma
Host genetic backgrounds, EBV strains matter
Latent and lytic genes differentially expressed
Activate oncogenes, inhibit tumor suppressors
Mutations/deletions in latent/lytic genes affect interactions with host cells, increase chances for cancer
Endemic Burkitt Lymphoma
Due to chronic malaria
Diagnosis/Treatment
CBC: high Lymphocyte count
>10% Atypical lymphocytes (Downey cells; reactive CD8+ T Lymphocytes)
MonoSpot (Heterophile Ab Test): No longer recommended by CDC as first test, needs CBC first
Serology
Elevated IgM, IgG = acute
Elevated IgG not IgM = chronic or reactivated
Anti-EBNA = older (remote), chronic
During an active EBV infection, EBV Antibodies in sera can (rarely) produce false positive results with
Lyme disease tests (B. burgdorferi Ag)
HIV test (HIV Ag)
VDRL Syphilis test
HSV 5
Enveloped, dsDNA virus
Clinical Presentation:
Abnormalities seen in utero for congenital CMV
Microcephaly, intracranial calcifications, occipital horn abnormalities, growth restriction, enlarged liver, pericardial effusion, placental inflammation, mortality, cerebral atrophy
Intracerebral calcifications (poor developmental prognosis)
Diseases:
Mononucleosis
Fever, malaise, pharyngitis, rash, leukocytosis
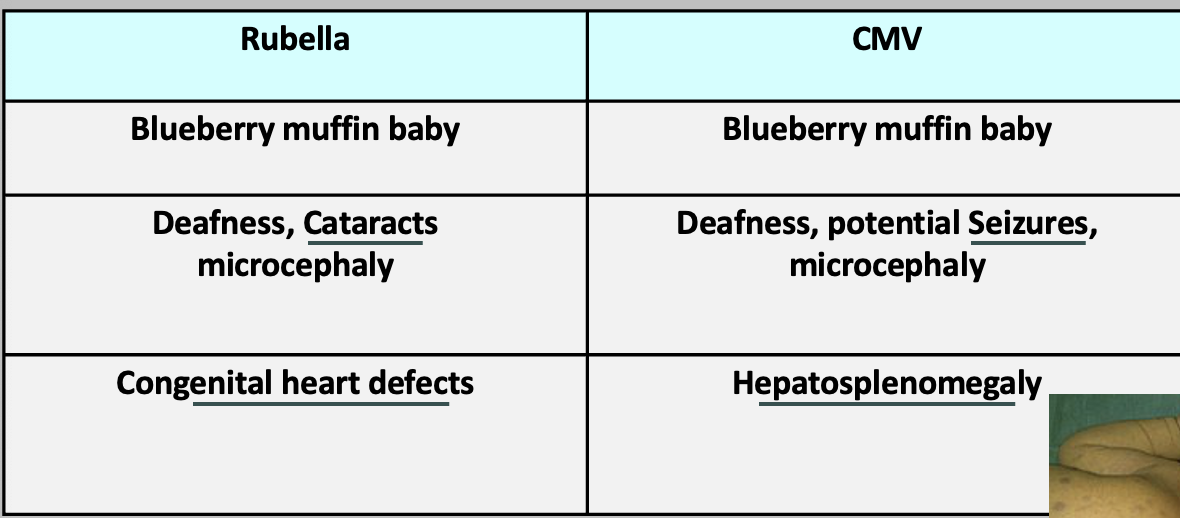
Congenital CMV
Transplacental transmission risk
Most common intrauterine infection in U.S
Most common cause of non-genetic hearing loss
Diagnosis/Treatment
NO heterophile antibodies
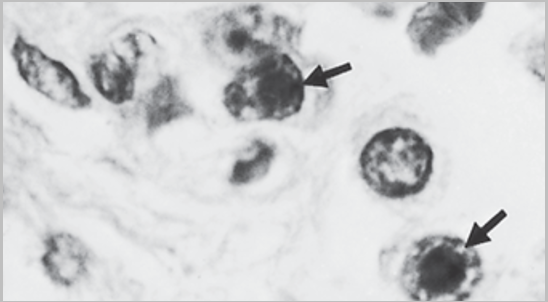
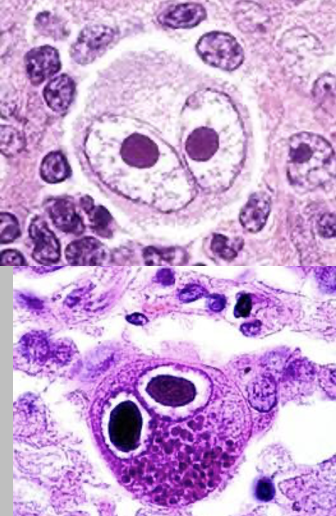
Biopsy cells to see Owl’s Eye Nuclei
Large, basophilic (dark) nuclear inclusion, perinuclear halo, cytoplasmic inclusions
Serological testing
Quantitative PCR
Treatment for Congenital: oral valganciclovir for 6 months if symptomatic
Diagnosis for Congenital: Consider TORCH
HSV 6/7
Enveloped, dsDNA virus
Clinical Presentation:
6th Disease, 6 months to 3 years
2 serogroups A, B
>90% of those> age 1 are seropositive
7th Disease, ages 1-3
>90% seropositivity after age 3
Diseases:
Roseola Infantum
Abrupt high fever for up to 5 days in child < 2-year-old
Irritable baby, lymphadenopathy, +/-rash
Fever breaks, maculopapular rash, starts on neck/trunk and spreads to face and limbs
Possible febrile seizures (unknown neurotropism)
Possible otitis, GI and/or respiratory distress
HSV 8
Enveloped, dsDNA virus
Attributes:
Lymphotropic, closely related to EBV
Lytic first then latent in B Cells
Pathogenesis:
Infects/transforms endothelial cells
Pathogenesis related to ability to interfere with cell proliferation, apoptosis and host response
Inactivates tumor-suppressor genes
Inhibits viral polymerase
Clinical Presentation:
Immunosuppressed, HIV/AIDS
Elderly men on lower extremities
Middle Eastern Descent
Diseases:
Kaposi Sarcoma
Rapid tumor formation, often in the mouth and lower extremities
Infected lymph nodes
Diagnosis/Treatment
High CD4 counts
Treated with Foscarnet, Famciclovir, Ganciclovir, Cidofovir
Excision/removal
Variola: Smallpox
Enveloped linear dsDNA virus
Pox in a box: Complex, divides in cytoplasm
Attributes:
Narrow host range (humans and monkeys)
WHO declared eradicated in 1980
Spread via respiratory droplets and fomites
Highly contagious
Bioterrorism threat
Pathogenesis:
Clinical Presentation:
Diseases:
Smallpox
Fever
Tiredness
Muscle aches
Flat spots that appear on the body
Blisters that form before scabbing and falling off, which can leave scars
Diagnosis/Treatment
Differential
PCR
DNA containing inclusion bodies in cytoplasm
JYNNEOS/IMVANEX/IMVAMUNE:
Modified Vaccinia Ankara (MVA) strain
highly attenuated, non-replicating
used for healthy and immunocompromised
Approved for Smallpox and MPX
Prophylaxis of MPX after exposure, high risk groups prior to exposure
ACAM2000:
Replication competent smallpox vaccine
Only for select patients and laboratory workers
More side effects than MVA
Monkeypox
Enveloped linear dsDNA virus
Pox in a box: Complex, divides in cytoplasm
Attributes:
Spread through direct contact with infected people or animals
Skin to skin, body fluids, Not STI
Pathogenesis:
Clinical Presentation:
Diseases:
Monkeypox
It's usually a self-limited infection with a painful rash that develops 5–21 days after exposure. Most people recover on their own after a few weeks.
Diagnosis/Treatment
JYNNEOS/IMVANEX/IMVAMUNE:
Modified Vaccinia Ankara (MVA) strain
highly attenuated, non-replicating
used for healthy and immunocompromised
Approved for Smallpox and MPX
Prophylaxis of MPX after exposure, high risk groups prior to exposure
ACAM2000:
Replication competent smallpox vaccine
Only for select patients and laboratory workers
More side effects than MVA
Vaccinia (Smallpox Strain)
Enveloped linear dsDNA virus
Pox in a box: Complex, divides in cytoplasm
Attributes:
Smallpox vaccine strain
Close relative to cowpox
Infects wide host range
Natural reservoir unknown
Diseases:
Lesions
inoculation causes small lesions with discharge, ulceration and necrosis
Diagnosis/Treatment
Vaccine is successful if there is a venter pustule with red, raised area
Molluscum Contagiosum
Enveloped linear dsDNA virus
Pox in a box: Complex, divides in cytoplasm
Attributes:
Transmission:
Skin/skin contact: roughhousing, wrestling, sex
Fomites-shared towels, toys, gym mats etc
Common in children and young adults
Incubation period 2 wks to 6 months
Diseases:
Lesions
Pearly, umbilicated “flesh-colored dome” papule
“Central Dimple”
Itchy but often painless
Resembles chronic, localized miniature smallpox
Synchronous centripetal rash begins in mouth/face/arms/legs…then trunk within 24 hours
Diagnosis/Treatment
Self-limiting-resolves in 6-12 months
YCANTH: new approved Tx
Cryosurgery, Cantharidin (beetle juice), Curettage, Pulsed dye laser (PDL), Imiquimod cream (topical at home)
TX patients who are immunocompromised, skin conditions, possibly others
HBV (Hepadnaviridae)
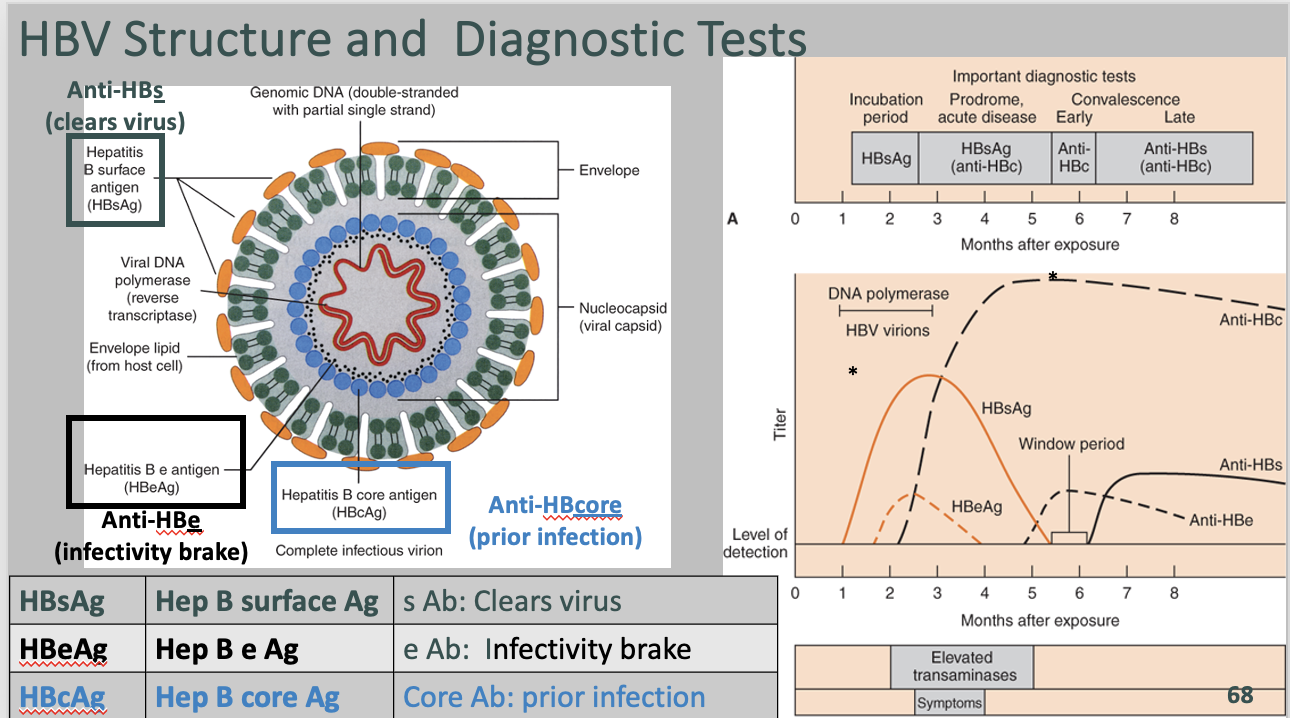
Enveloped, circular, partially double stranded DNA
Attributes:
Transmission
Body fluids, birth
Liver tropism: inflammation and replication
Pathogenesis:
Acute Infections:
Binds liver-specific bile transporter, NCTP
Replication aided by host enzymes
Innate and adaptive responses (T cell and Abs) clears infection BUT also causes liver injury due to inflammation and destruction of infected cells by CD8+ T cells
Clearance; lifelong immunity to HBsAg
Chronic Infection
chronic when not cleared
5% of infected adults/90% of infected newborns become carriers/chronically infected
Chromosomal integration-no replication
no cure; reactivated with loss of immune-competency
Extrahepatic: neuropathies, glomerulonephritis, vasculitis
Hepatocellular Carcinoma
Randomly integrated DNA: instability, disruption of genes, altered expression
Aberrantly expressed/mutated viral proteins interfere with gene expression and/or activate oncogenic signaling pathways
Expression of HBVx promotes proliferation by inactivating p53
Inflammation and speeding through cell cycle causes genetic damage (because T cells killed infected cells and liver trying to replace)
Diseases:
Hep B Infection
Mild-acute
Asymptomatic
Mild flu-like symptoms
Fever, fatigue, abdominal discomfort
Severe acute
<1% Liver failure
Bilirubin accumulation-jaundice (test)
Encephalopathy (no detox)
Decreased clotting factors (test)
Elevated serum transaminases (ALT)
Swollen liver, wrinkled capsule due to parenchymal collapse, small regenerative nodules, no fibrosis.
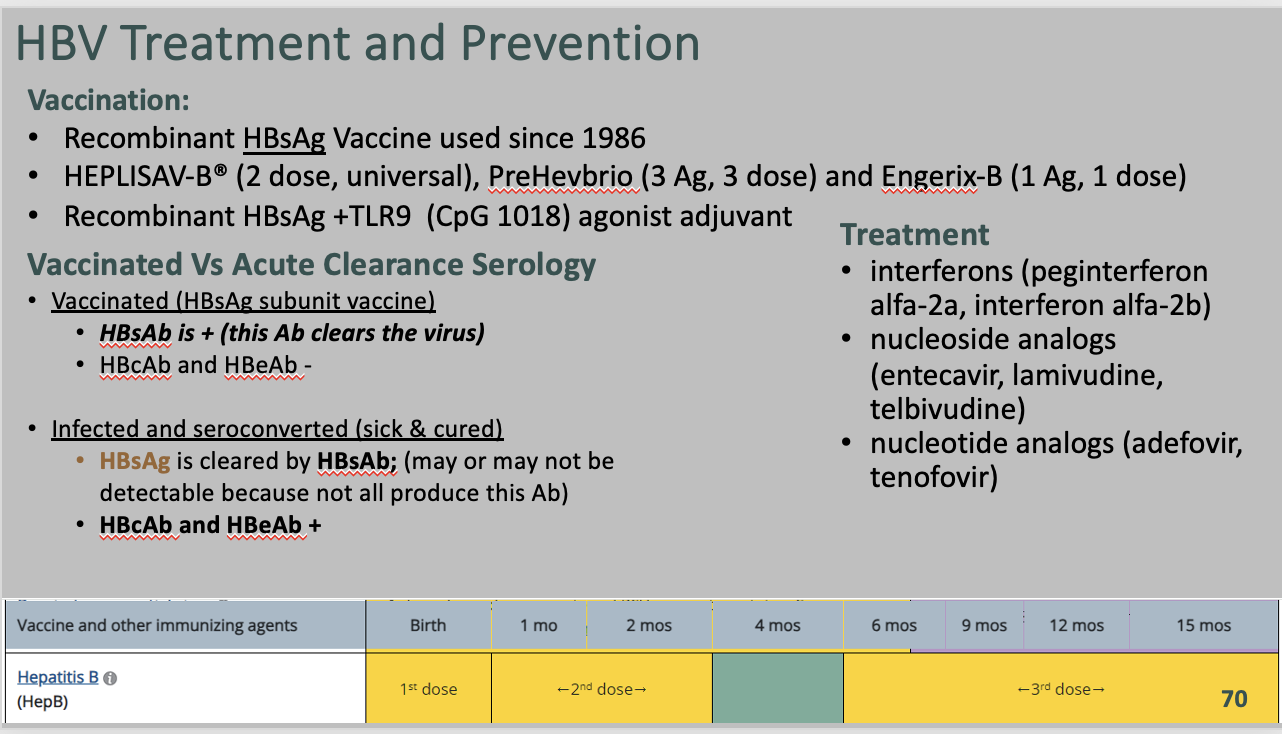
Diagnosis/Treatment
Acute—supportive
Possible antivirals:
nucleotide/nucleoside analogs
analogstenofovir
Entecavir
lamivudine
REST ON DIFF CARD CAUSE THERE IS TOO DAMN MUCH
Mono symptoms and negative heterophile antibody test strongly suggests
CMV
Difference between CMV and Rubella with newborn deafness
Smallpox vs Chickenpox vs Monkeypox
Explain what happens in the case of chronic hepatitis infection.
Progressive Disease:
Acute → chronic → cirrhosis → carcinoma
Chronic serology and liver injury due to loss of cells caused by inflammation, destruction by T cells
Ground glass cells in 50-75% chronic
Stained for Hep B Surface Ag
Contrast-enhanced CT scan- malignant hepatocellular lesions
Describe the relation between HBV structure and diagnostic tests that can be done.
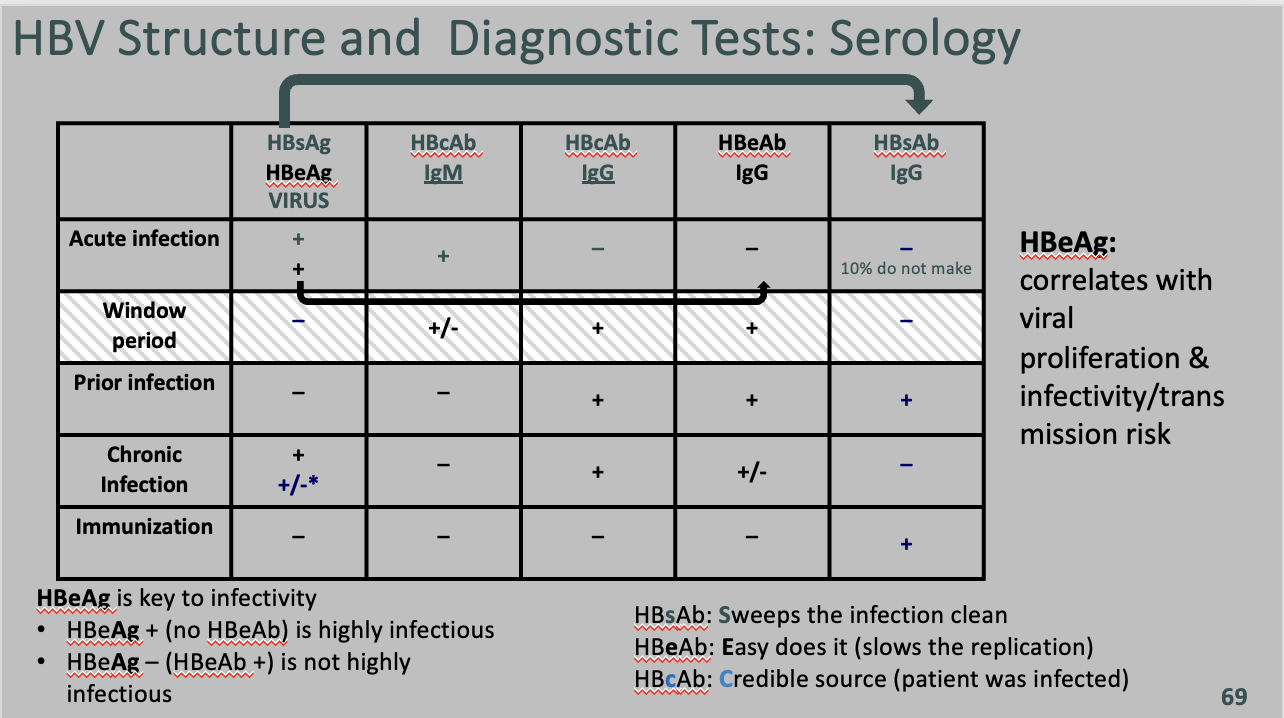
HBsAg (Hepatitis B surface antigen): This is a protein present on the surface of the Hepatitis B virus. It is the earliest marker to appear in the blood after infection and can be detected during acute or chronic HBV infection. Detection of HBsAg indicates active HBV infection.
HBeAg (Hepatitis Be antigen): This is a marker of active viral replication. Its presence indicates that the virus is actively replicating in the liver and the patient is highly infectious.
HBcAg (Hepatitis B core antigen): This antigen is part of the Hepatitis B core and is not detectable in the blood. However, detection of antibodies against HBcAg (HBcAb) indicates prior exposure to the virus, whether acute or chronic, and does not confer immunity.
Hepatitis Diagnostic Chart
Hepatitis Treatment and Prevention
Calciviridae (Norovirus)
Naked, (+) ssRNA virus
Attributes:
Encodes RDRP but isn’t premade
Replication occurs in cytoplasm
Major capsid protein VP1 used for genotyping based on sequence
#1 cause of gastroenteritis worldwide
Fecal-Oral
Pathogenesis:
Diarrhea: Abnormal absorption and secretion relating to changes in microvilli, crypt hypertrophy, disruption of barrier functions, apoptosis
Diseases:
Gastroenteritis
Acute, watery, non-bloody diarrhea with projectile vomiting
Typically 3 days of vomiting, with non-inflammatory, negative fecal leukocytes
Presentation:
Schools, ships, hospitals, nursing homes
Diagnosis/Treatment
Clinical Presentation & RT-PCR
Echovirus (Picornaviridae)
Nonenveloped, (+) ssRNA virus
Attributes:
Spread via Fecal-Oral
Diseases:
Aseptic Meningitis
Swallowed, 2-14 day incubation, multiplies peyer’s patches, viremia, organs infected, more viremia, possible CNS
Enteroviruses (Type of Picornaviridae, not Rhinovirus)
Nonenveloped, (+) ssRNA virus
Attributes:
Spread via Fecal-Oral
Seasonal
Primarily pediatric
Vertical transmission during birth
hepatic necrosis, meningoencephalitis, myocarditis, sepsis, death of neonate
Pathogenesis:
Target and replicate in GI and URT
Diseases:
Mild Case
Mild, febrile illness
Summer colds, diarrhea
Enterovirus D68
acute respiratory illness in summer, fall
respiratory secretions
Higher risk: young children that suffer from asthma, wheezing, or other breathing abnormalities
large outbreaks
associated with acute flaccid myelitis
Enterovirus A71
hand-foot-mouth disease
rarely: meningitis, encephalitis, acute flaccid paralysis
respiratory secretions, fecal-oral, contact, fomites
children in the late summer, fall
Enterovirus 70
Hemorrhagic conjunctivitis
Rhinovirus (Type of Picornaviridae, Enterovirus Genus)
Nonenveloped, (+) ssRNA virus
Attributes:
Spread via respiratory droplets
More severe in immunocompromised
Pathogenesis:
Virus spreads to nasal epithelium
Replicates and sheds causing the infection to spread
Ab and interferons facilitate recovery. Infection will end and epithelium regenerates
Diseases:
Primary cause of exacerbations of COPD and asthma
50% Common Colds
Sneezing, sore throat, restlessness, coughing, fever, HA, myalgias
Coxsackievirus (Type of Picornaviridae, Enterovirus Genus)
Nonenveloped, (+) ssRNA virus
Attributes:
Worldwide distribution, summer and fall
Group A and B
Target:
A: skin and mucous membranes
B: invasive=heart, pleura, pancreas, liver
Both: meninges. motor neurons (anterior horn cells), paralysis
Transmitted by fecal-oral and respiratory secretions from human reservoirs
Pathogenesis:
Replicate in oropharynx, GI tract
Enter blood stream
Diseases:
Group A
Herpangina
high fever, sore throat, painful vesicles in oropharynx; summer
Hand-Foot-Mouth disease
rash on hands and feet, mouth ulcers, benign, self limiting, usually A16
Acute Hemorrhagic Conjunctivitis
only A24
Group B
Pleurodynia (Bornholm Disease)
“epidemic myalgia”: fever, severe pleuritic chest pain, inflammation of intercostal muscles
Myocarditis, Pericarditis
Pancreatitis
Diagnosis/Treatment
Clinical findings, PCR, Ab
Supportive treatment
Poliovirus (Enterovirus C)
Non-enveloped, (+) ssRNA virus
Attributes:
three serotypes: 1, 2, 3
Fecal-oral route
4-35 day incubation period possible, but usually 7-14 days
95% of cases are asymptomatic
Pathogenesis:
Infection enters intestine as passes through the blood and lymphatics
Could also pass straight through to the feces
Replicates in the oropharynx and small intestine
Febrile Illness (Day 3)
Meningitis (Day 6)
Paralysis (Day 8)
Diseases:
Abortive Poliomyelitis
HA, Nausea, ST
Nonparalytic Poliomyelitis
Nearly identical to aseptic meningitis
Paralytic Poliomyelitis
Muscle paralysis follows myalgias, and asymmetric weakness. Respiratory paralysis may occur.
Post-Polio Syndrome
40yrs post polio, develop new muscle pain, weakness, paralysis
Diagnosis/Treatment
Iron lungs helped polio paralysis victims breathe, either temporarily or permanently.
Polio Vaccines
1955 - Salk’s inactivated vaccine IPV against Type 1-no patent/free (USED IN US)
IgG response
Stopped disease but not transmission
1959-1962 Sabin Oral live Polio Vaccine (OPV) against Type 1
stopped disease and transmission, IgA response
1963-combined Type 1, 2, 3 OLPV vaccine
OLPV reverts to wild type = Vaccine-derived polioviruses
Can spread person to person and cause polio in unvaccinated (vaccine associated paralytic poliomyelitis)
Does not happen with IPV!!
Dengue Virus (Flavaviridae)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: •Aedes aegypti and albopictus mosquitoes
Pathogenesis:
Ab to other strains do not neutralize but enhance entry of viruses to immune cells with Fcγ receptors where they multiply
Diseases:
“Breakbone Fever”
1st infection
high fever, SEVERE muscle, joint, bone pain, enlarged lymph nodes, rash
Correlate with immune response, replication in lymph nodes and dissemination
Rarely fatal with few sequelae
Only a few strain-specific neutralizing Ab; most non-neutralizing
Severe-Dengue Hemorrhagic Fever
Usually 2nd infection with a 2nd strain
Initially classic then worsens due to ADE
High fever, rash from skin hemorrhages, Intestinal hemorrhages related to replication and immune system, shock and death likely
Diagnosis/Treatment
Dengvaxia
live, attenuated, tetravalent (Yellow Fever virus vaccine base)
For 9-16 years only WITH a prior infection aka positive serology
Not for travelers
Serology, PCR, culture, ID proteins
Supportive, no antivirals
Eliminating mosquito breeding grounds and insecticides
vaccine
Yellow Fever Virus (Flavaviridae)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: Aedes mosquitoes during the rainy season
Pathogenesis:
Diseases:
“Yellow Fever”
50% mortality due to internal bleeding within 2 weeks
HA, myalgias, lumbosacral pain, nausea, malaise, dizziness, conjunctival injection
Symptoms will abate and then progress and worsen 50% will lead to mortality due to internal bleeding within 2wks
Jaundice
Diagnosis/Treatment
Difficult, confused with other viruses, malaria
PCR and NAAT
Later-serology and id proteins
No antivirals, symptomatic Tx
Prevention
Eradication
Avoidance
Live attenuated since 1935
YF-VAX in US
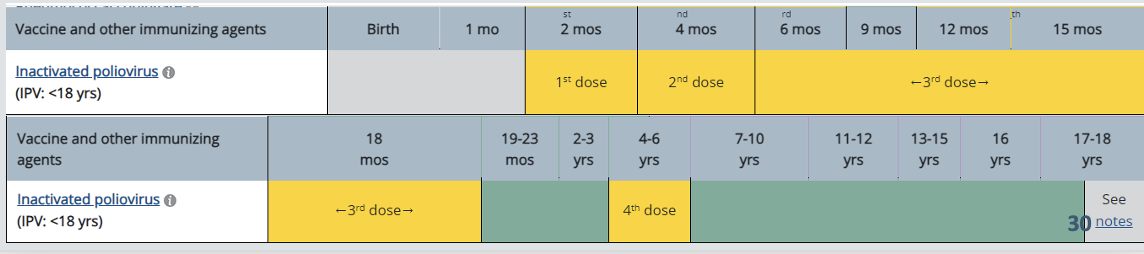
Vaccination dates for Polio
What is the issue with vaccine derived polio?
Problems:
Decreased vaccination rates
Use of OLPV, even newer versions, allows reversion and results in spread
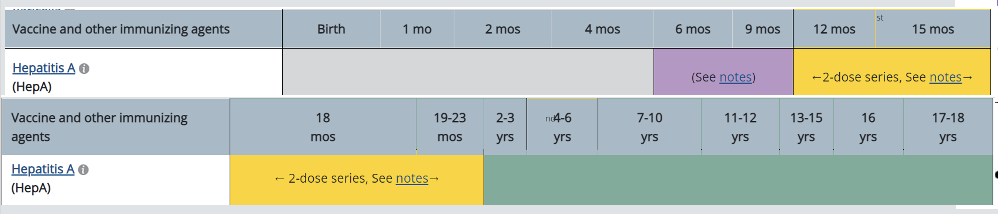
Hepatitis A Vaccine Times
What is the difference between a reservoir host and an incidental host?
Reservoir host - the natural host in which the virus lives and replicates and from which the vector can gain an adequate dose of the virus to spread it to another reservoir host
Incidental host - a host that can be infected and become ill but is considered a “dead-end” because the vector can’t get enough virus out to spread to another host
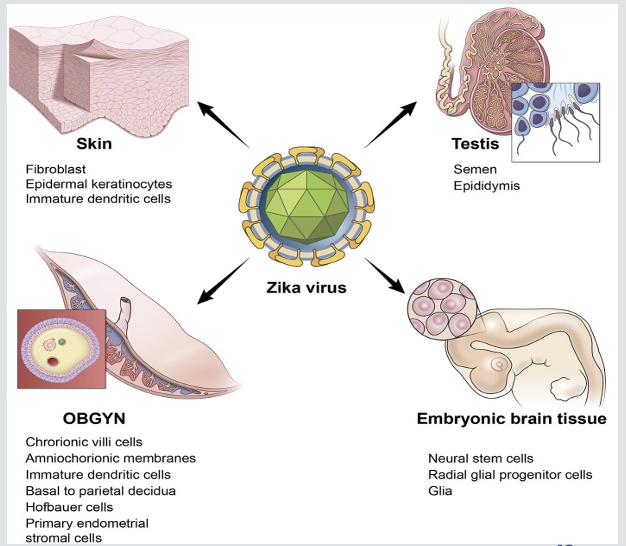
Zika Virus
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Many hosts
Tropical/Subtropical regions
Transmitted by female Aedes aegypti, albopictus
Sexual contact, body fluids, organ transplants, transplacental
Pathogenesis:
Refer to image
Diseases:
Self-resolving, asymptomatic or mild fever, rash, conjunctivitis, muscle and joint pain, malaise, and headache unless congenital
Possible GBS, arthritis (resolves in 2 weeks)
Fetal infection-microcephaly, birth defects, problems in pregnancy and/or partially collapsed skull
Decreased brain tissu
Eye damage, hearing issues
Joints with restricted motion
Developmental challenges
Seizures
Stops neural development, cell division in the fetus
targets neural progenitors
Diagnosis/Treatment
Symptomatic, supportive treatment
Diagnosis via PCR, serology, plaque reduction assasys in presence of IgM
Powassan Virus (Flavaviridae)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Transmission via:
Ixodes ick bites
I. cookei (groundhog tick)
I. marxi (squirrel tick)
I. scapularis (blacklegged deer tick)
Canada, Russia, US
Diseases:
4-6 week incubation
Most asymptomatic
Fever, headache, vomiting, weakness, rarely encephalitis and meningitis
Diagnosis/Treatment
Serology, possibly RT-PCR
Supportive only
Variable appearances on MRI
St. Louis Encephalitis Virus (Flavaviridae)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: Culex mosquito
Diseases:
Mostly asymptomatic
CNS Disease
Headache, fever, agitation
Lymphocytic meningitis affects gray matter
Hypothalamus, cerebral and cerebellar cortex, basal ganglia, brainstem, spinal cord
CSF-elevated pressure, lightly increased lymphocytes, decreased protein, IgM; PCR
EEG-possible abnormalities
Diagnosis/Treatment
Symptomatic → supportive
West Nile Virus (Flavaviridae, Arbovirus)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: Culex mosquito
Diseases:
Mostly asymptomatic, some develop fever and/or meningitis
CNS Disease
Acute inflammatory response causes headache, memory loss, disorientation
Meningoenceophalits
Destruction of neurons in spinal column and brain stem gray matter
CSF-elevated protein, leukocytes, normal glu, IgM; PCR
CT-no abnormalities for weeks
Diagnosis/Treatment
Symptomatic → supportive
What is the purpose of sentinel chickens?
Monitoring the presence of arboviruses. They do not get sick when exposed but can generate antibodies.
Chinkungunya (Togaviridae, Family Arbovirus)
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: Aedes aegypti and albopictus mosquitoes
Can be spread during 2nd trimester of pregnancy and rarely but possible during birth
Spread by breast feeding
Old world
Anyone; young, old, immunocompromised at higher risk
Pathogenesis:
Diseases:
fever, polyarthralgia, joint pain, myalgia
debilitating pain can persist for months (1/1000)
Diagnosis/Treatment
No NSAIDs unless it is not dengue
Venezuelan Equine Encephalitis
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Vector: LOTS OF THEM, LOTS OF HOSTS
Mammals are not dead end 💀
Biological weapon
Diseases:
96% asymptomatic
5% symptomatic
<5% flu like symptoms, then altered mental state and seizures indicating encephalitis
1/3 of the 5% die
2/3: neuro deficits, paralysis and other permanent neuro changes
Diagnosis/Treatment
Horse vaccine 🐴 slayyy
Hepatitis A
Common Name: “Infectious”
Virus Structure: Picornavirus, capsid, (+) RNA
Transmission: Fecal-Oral
Onset: Abrupt
High-Risk groups: injection drug users, MSM, travelers to endemic regions, aid workers
Incubation Period (Days): 15-50
Severity: Mild
Symptoms: nausea, vomiting, fatigue, right upper abdominal discomfort, fever, poor appetite, jaundice, dark urine
Chronicity/Carrier State: No
Other Disease Associations: Rare Fulminant Hepatitis
Hepatitis B
Common Name: “Serum”
Virus Structure: Hepadnavirus; envelope, DNA
Transmission: Parenteral, sexual
Onset: Insidious
Incubation Period (Days): 45-160
Severity: Occasionally severe, 3%-10% chronicity in adults; 30%-90% in infants and children
Chronicity/Carrier State: Yes
Other Disease Associations: Primary Hepatocelluar carcinoma, cirrhosis
Hepatits C
Common Name: “Non-A, non-B posttransfusion”
Virus Structure: Flavivirus; envelope, (+) RNA
Transmission: Parenteral, sexual
Percutaneous blood, needles risk
Onset: Insidious (Chronic Acute)
Symptoms: malaise, nausea, and right upper quadrant pain, dark urine and jaundice
Incubation Period (Days): 14-180+
Severity: Usually subclinical; 70% chronicity
Chronicity/Carrier State: Yes
HCV viral loads, fibrosis and active liver inflammation, persistently elevated AST/ALT
Other Disease Associations: Primary Hepatocelluar carcinoma, cirrhosis, chronic hepatitis
Treatments:
Direct Acting Antivirals for 12-24 weeks
combination of 2nd generation protease inhibitors, inhibitors of structural proteins, polymerase inhibitors
+/- ribavirin
95% success
Hepatitis D
Common Name: “Delta Agent”
Virus Structure: Viroid-like; envelope, circular RNA
Transmission: Parenteral, sexual
Onset: Abrupt
Incubation Period (Days): 15-64
Severity: Co-infection with HBV occasionally severe; superinfection with HBV often severe
Chronicity/Carrier State: Yes
Other Disease Associations: Cirrhosis, Fulminant hepatitis
Hepatitis E
Common Name: “Enteric non-A, non-B”
Virus Structure: Hepevirus capsid, (+), RNA
Transmission: Fecal-Oral, often in places with poor sanitation, undercooked deer and wild swine
Symptoms:
1-6 weeks of symptoms:
transient watery diarrhea, Jaundice, loss of appetite, enlarged liver, nausea and vomiting, fever, itching, rash, joint pain, dark urine, clay colored stool
1% fatality
fulminant hepatitis and liver failure
Acquiring during pregnancy increases risk of fulminant hepatitis and fetal mortality
Onset: Abrupt
Incubation Period (Days): 15-50
Severity: Severe in pregnant women, mild in adults
Chronicity/Carrier State: No
Other Disease Associations: None
Diagnosis: IgM Ab, PCR
Eastern Equine Encephalitis
Icosahedral, Enveloped, (+) ssRNA virus
Attributes:
Biological weapon
Found in the Eastern side of the US
Pathogenesis:
Diseases:
Fever, chills, aches, meningitis for 1-2 weeks, followed by encephalitis or recovery
1/3 with encephalitis die
2/3 recover; long-term physical or mental impairments and early death
50-70% mortality
Rubivirus (Matonaviridae)
Enveloped +ssRNA
Attributes:
Human Reservoir, respiratory secretions
Highly contagious
Winter & Spring
Pathogenesis:
URT, replicates, viremia, localizes to lymphoid tissues, skin, organs, rash, possible arthritis, due to immune complexes
Virus shed up to 8 days
2-3 week incubation
Diseases:
Congenital Rubella Syndrome
Congenital infection: placental infection, transplacental spread
Classic triad in newborn:
Deafness – Ears
Cataracts – Eyes
Cardiac disease (Patent ductus arteriosus = PDA)
PLUS: Blueberry muffin baby = extramedullary erythropoiesis
Diagnosis:
TORCHeS infections: Toxoplasma, Others, Rubella, CMV, Herpes, Syphilis
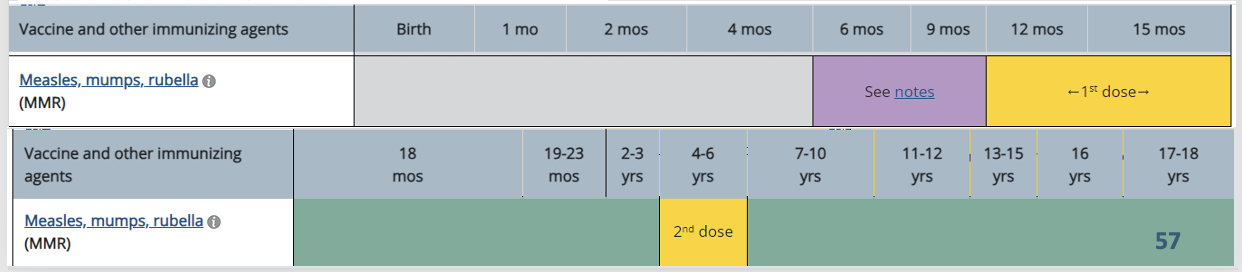
Rubella Vaccine schedule
MMR or MMR II: attenuated live measles and rubella viruses for 12 months and over, non-pregnant
HTLV
Enveloped, +ssRNA, retrovirus
Attributes:
Use RT and incorporates into chromosome
Lifelong infection
95% asymptomatic
Affects >5-10 million worldwide
4 groups: I, II, III, IV
Diseases:
HTLVI
Most oncogenic virus known
Breast feeding, blood transfusions prior to 1988, needles, sex
Adult T cell leukemia-lymphoma (ATL), HTLV-1-associated myelopathy (tropical spastic paraparesis)
Different subtypes in different regions
HTLVII
Hairy Cell Leukemia
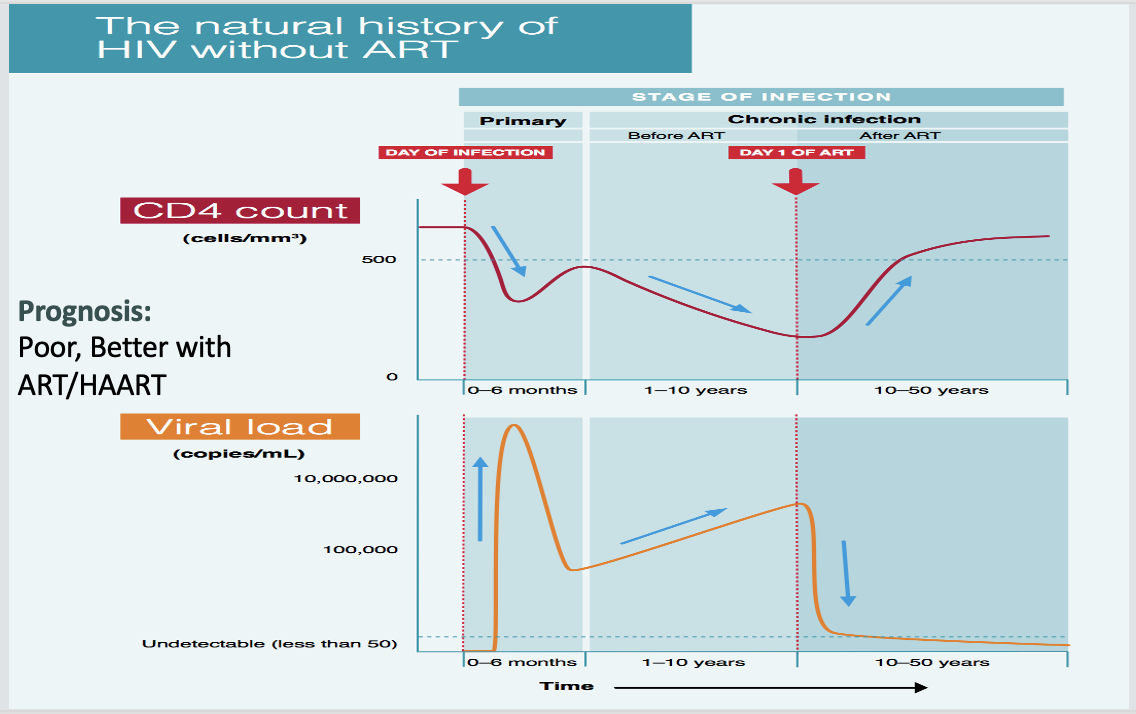
What cells does HIV attack?
CD4 & CCR5
How does HAART therapy work?
Antiretroviral drug combinations-Highly Active Anti Retroviral Therapy (HAART)
Nucleoside/tide Reverse Transcriptase Inhibitor (NRTI)
Integrase Inhibitors
Non-Nucleoside/tide Reverse Transcriptase Inhibitor (NNRTI)
Protease Inhibitors
CCR5 Inhibitors (Entry)
How does PrEP work for HIV?
Medication: PrEP involves taking a prescription medication called Truvada or Descovy. These medications contain a combination of two antiretroviral drugs: tenofovir and emtricitabine.
Mechanism of Action: When taken consistently, these drugs work to prevent HIV from establishing itself and replicating within the body. Tenofovir and emtricitabine interfere with HIV's ability to replicate by blocking an enzyme called reverse transcriptase, which the virus needs to multiply.
Preventative Effectiveness: When taken daily as prescribed, PrEP has been shown to significantly reduce the risk of HIV transmission. Studies have demonstrated that PrEP can reduce the risk of HIV infection by up to 99% when taken consistently.
Consistency is Key: It's important to emphasize that PrEP must be taken consistently and correctly to be effective. Missing doses can reduce its effectiveness in preventing HIV transmission.
Regular Testing and Monitoring: Individuals taking PrEP are typically recommended to undergo regular HIV testing and monitoring for other sexually transmitted infections (STIs) to ensure their ongoing health and the effectiveness of the treatment.
Combination Prevention Approach: PrEP is often used as part of a comprehensive HIV prevention strategy, which may include other preventive measures such as condom use, regular HIV testing, and access to comprehensive sexual health services.
CD4 count with HIV
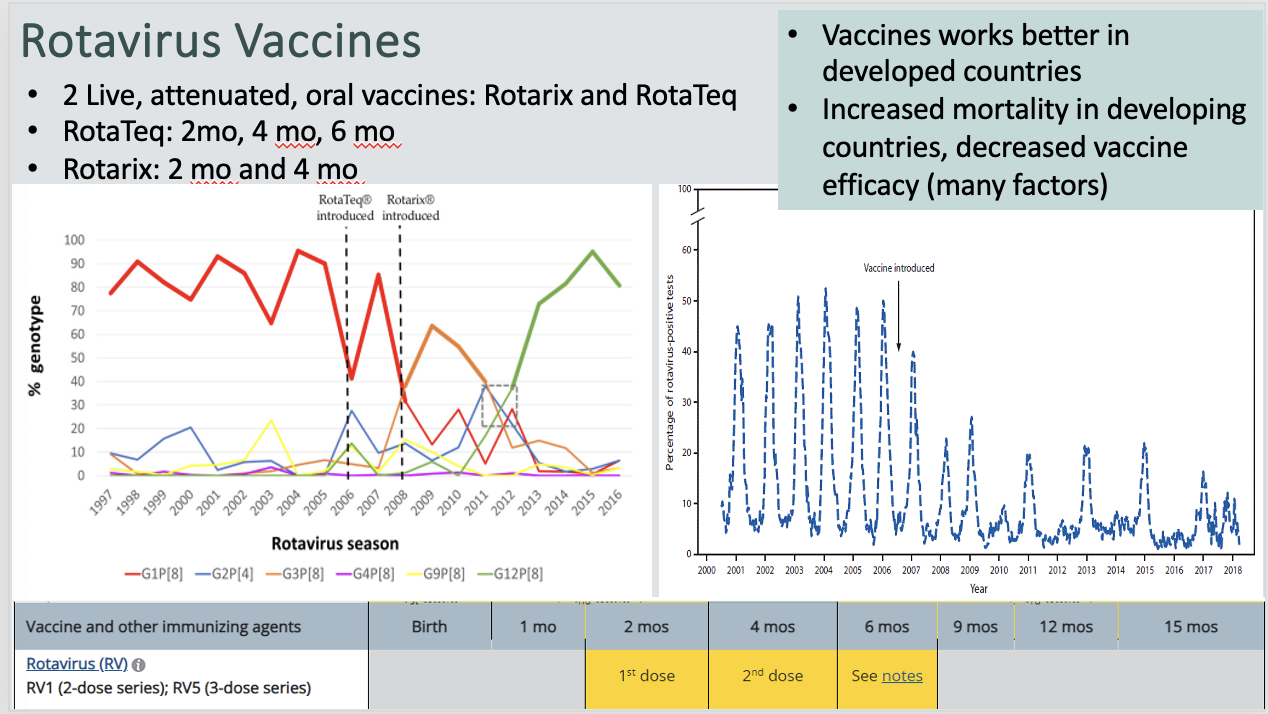
Rotavirus (Sedoreoviridae)
Attributes:
Use RT
Wheel-Shaped
11 segments dsRNA
3 layers of protein around RNA = very stable
Classification based on VP6 capsid
8 groups (RVA to RVH)
Fecal-Oral
Diseases:
Gastroenteritis (<5yrs)
Vomiting, diarrhea, and fever
Dehydration, loss of electrolytes
No blood or fecal leukocytes
Presentation:
Most common in young infants and children.
Treatment:
Rehydration
Rotavirus Vaccine Schedule
Coltivirus (Colorado Tick Fever Virus)
Naked, dsRNA virus
12 ds RNA segments with 3 capsids
RDRP
Replication cycle same as Reo
Attributes:
Co-infections with Rickettsia
Dermacentor andersoni range
May-July
Diseases:
Fever, chills, myalgias, headache
Can target CNS or liver
Self-limited with good prognosis
Rare deaths due to DIC (disseminated intracellular coagulation) and thrombocytopenia
What are the four keys to fungal pathogenesis in humans?
Thermal tolerance
Penetrating or circumventing host barriers to reach internal tissues
Digestion and absorption of human tissues
Withstand/resist the human immune system
Histoplasm Capsulatum
Attributes:
Bat guano, bird droppings
Hot humid conditions
Pathogenesis:
Spores are inhaled and morph into yeast in the lungs
7-21 day incubation
Ingested by macrophages: prevent macrophage killing and multiply
Macrophages carry to other sites and establish infection
Dendritic cells engulf and produce pro-inflammatory cytokines
Cytokines finally activate macropahges to kill yeasts
Clinical Presentation:
Mostly asymptomatic, self limiting
Symptomatic:
Slow onset
High fever, productive cough, chest pain
Dissemination possibly fatal: CNS, GI, anemia, bone marrow
Granulomas = relapsing, chronic
Presentation:
Caves, poultry coops
Key indicators
History of high-risk exposure
Conditions:
HIV / AIDS
TNF-alpha inhibitors
Hepatosplenomegaly
Mouth and tongue ulcers
Pancytopenia (bone marrow involvement)
Often misdiagnosed as TB
Diagnosis/Treatment:
Fungi in Monocytes
A. Lung Biopsy: Culture and staining, Histopathology/Cytopathology
B.Antigen Detection: Enzyme Immuno-Assay
C. Immune Reaction:
Immunodiffusion (Ab)
complement fixation (C’)
enzyme immunoassay (Ab)
skin test (Ab)
D. Molecular Methods: Not FDA approved yet
For severe cases treated with amphotericin B for 1-2wks followed by itraconozole for 12wks
Blastomycosis
Attributes:
Endemic areas overlap with histoplasma
Can cause
Extrapulmonary disease
Verrucous (warts), pustules
Osteomyelitis
Pathogenesis:
Inhaled w/ 21-106 days of incubation
Phagocytosed and killed by bronchopulmonary phagocytes.
Some people eliminate better and remain asymptomatic
Converts to yeast, impairs innate and adaptive immunity
Yeast multiply and disseminate through blood and lymphatics
Eventually controlled by T cells, macrophages and antifungals
Clinical Presentation:
Acute: fevers, chills, productive cough with or without sputum production
severe cases progress to ARDS.
Slow onset pneumonia
Skin lesions with possible bone pain
Subacute/chronic: 2–6 months: fever, night sweats, cough, hemoptysis, weight loss
20% extrapulmonary dissemination
more common in patients with chronic pulmonary illness or immunocompromised.
Depends on organ involved
Diagnosis/Treatment:
Laboratory Tests
Histology
does not colonize so presence is confirmatory
Broad based budding yeast
Various stain
Culture
Serum/urine E1A Ag
Ab detection
Diff Diagnosis: Mimics acute pneumoccoccal pneumonia
Treatment
Depends on mild, moderate, severe, CNS
Complicated, 6-12 mo of tx
Amphotericin B and/or Azoles-Itraconazole
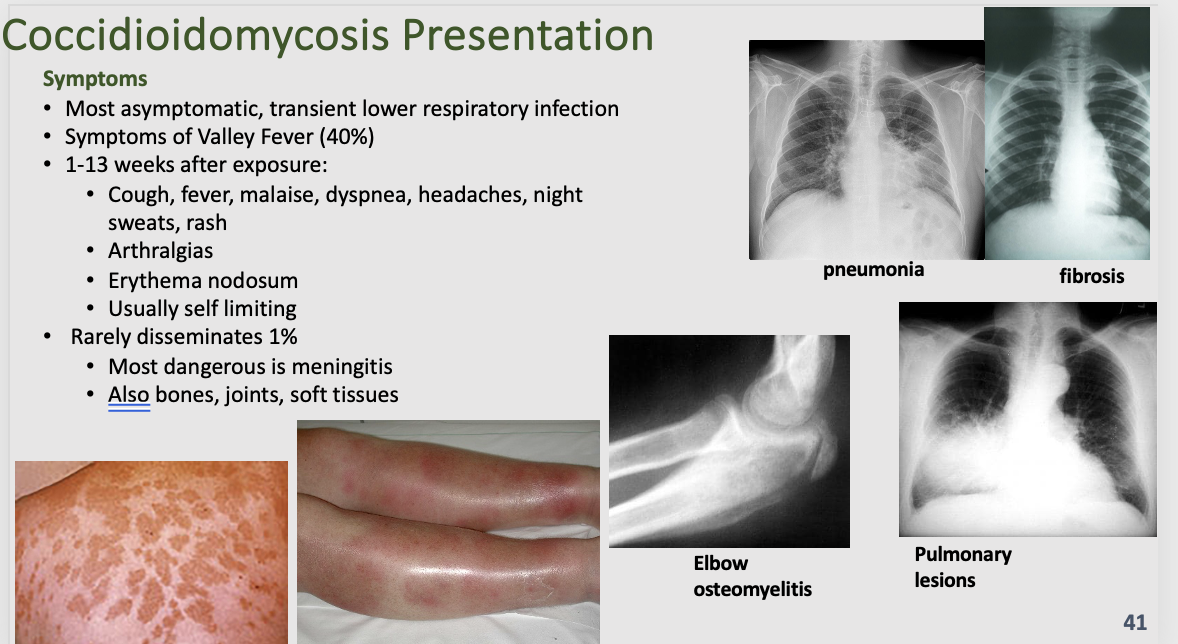
Coccidioidomycosis
Attributes:
Generally, southwestern US
Washington State through Mexico, several locations in South America
Grows as mold beneath desert surface
Dry conditions causes mold to fracture into spores
Not spread person to person
Pathogenesis:
Inhalation of spores, 10-50
Symptoms begin 1-4 weeks after inhalation
Spores enlarge to spherule
Spherules produce and release endospores
Each endospore produces another spherule, in lungs or other tissues
Macrophages carry endospores to other sites: bones, joints, soft tissues, CNS
Clinical Presentation:
Most asymptomatic, transient lower respiratory infection
Symptoms of San Joaquin Valley Fever or Valley Fever (40%)
Cough, fever, malaise, dyspnea, headaches, night sweats, rash
Arthralgias
Erythema nodosum
Usually self limiting
Rarely disseminates 1%
Most dangerous is meningitis
Also bones, joints, soft tissues
Presentation:
Clues: endemic area, pneumonia/URT disease that isn’t treatable with antibiotics, +/- rash and other symptoms
Diagnosis/Treatment:
Most Common Dx methods:
Serology for Ab (IgM, IgA)
Ag in blood and urine
Culture and staining
Tissue Histology
Spherule: Classic pathology finding: Spherule filled with endospores “Cocci Cactus”
Imaging
Treatment
Africa American or Filipino descent-more likely to have extrapulmonary complications
Mild disease: no need to treat
Moderate disease:
Flucanazole (400 mg daily) for 6 to 12 weeks
Severe:
intravenous amphotericin B in combination with Flucanazole 400 to 800 mg daily until stable and transition to Flucanazole (400 mg daily) for 12 to 14 weeks
Immunocompromised (regardless of severity)
Same as above but with extended time or lifelong treatment
Consult with ID specialist regarding tx of immunocompromising condition with coccidioidomycosis for specific tailored treatments of multiple conditions
Paracoccidioidomycosis
Attributes:
(Sub)Acute: famers, construction workers, generally males
Chronic: male, 30-60 years old (skin, mucus membranes, lymph nodes, spleen, liver, adrenals, more)
Pathogenesis:
The saprophytic form of Paracoccidioides spp. are found in the soil as mycelium (25 °C). Conidia and hyphal fragments inhaled by mammalian hosts are the primary sources of infection. The propagules are inhaled and established in the lungs, which, at body temperature (37 °C), initiate the dimorphic transition to pathogenic yeast form. The immune cells present within the host, such as macrophages, neutrophils, and dendritic cells, recognize the pathogen and trigger defense mechanisms such as the production of reactive nitrogen and oxygen species (RNS/ROS).
Clinical Presentation:
Cough, fever, malaise
granulomas form
Latent in granulomas
Reactivate decades later
Chronic, progressive pulmonary disease
Diagnosis/Treatment:
Diagnosis
Skin test
Culture, staining (gold)
Tissue Histology (gold)
MICKEY MOUSE HEAD OR PILOT’S WHEEL
Serology to detect Ab
PCR
Differentiate from TB
Treatment
Severity, form, co-morbidities, immune state
Mild/moderate: Itraconazole 9-18 months
Severe: amphotericin B usually 2 to 4 weeks, followed by Itraconazole 9
18 months
What are the four cutaenous implantation mycoses?
Sporotrichosis
Chromoblastomycosis
Mycetoma
Entomophthoramycosis
Lacaziosis
How do cutaenous implantation mycoses get in the body?
Fungi enter thru cuts/punctures caused while working with soil, sphagnum moss, decaying wood, vegetation throughout the world
Seen in people involved in farming, landscaping, and gardening
Usually due to inoculation from thorn pricks and splinters but can be from other trauma
Sporotrichosis
Attributes:
Sporothrix species
Some are human and animal pathogens and others are plant pathogens but not both
plant and organic matter, soil, wood, rose and other thorns
Dimorphic fungi
Sporothrix schenckii, S. schenckii, is a dimorphic fungus that can cause Sporotrichosis. S. schenckii exists in either a hyphal form at temperatures less than 37 degrees Celsius or as a budding yeast at 37 degrees Celsius or greater.
Pathogenesis:
Skin, not systemic
Traumatic spore inoculation leads to papule formation after days/weeks
Travels up from site to lymphatics via macrophages “ascending lymphangitis”
Deep trauma = bone and joint infections
Other trauma leads to multiple sites
Clinical Presentation:
Rose Gardener’s Disease
The first symptom of sporotrichosis is a small, painless bump that is pink, red, or purple and resembles an insect bite. The bump usually appears on the finger, hand, or arm where the fungus first entered through a break in the skin.
Presentation:
Gardeners, potting soil
Diagnosis/Treatment:
Most Common Dx methods:
Tissue histology and/or culture followed by staining and microscopy (yeasts)
Molecular ID (sequencing PCR)
serology
Treatment
Itraconazole, 3 to 6 months
Supersaturated potassium iodide (SSKI)
Bone/deep: Amphotericin B followed by Itraconazole for 1 year
Chromoblastomycosis
Attributes:
chronic localized infection with different types of lesions
Multiple fungal species with same presentation
Brazil, Mexico, southern China, Australia, and Madagascar
Present but not diagnosed/reported in Africa
Poor treatment outcomes, resistance a problem
Clinical Presentation:
Verrucous Lesions
Lesions showing a keratotic exophytic surface composed of sharp or blunt epithelial projections with keratin-filled invaginations (plugging), but without obvious fibrovascular cores.
Diagnosis/Treatment:
Treatment
Itraconazole or surgical removal
Mycetoma
Attributes:
Can be bacteria (Actinomycetoma, eg Nocardia) or fungal (Eumycetoma-primarily Africa)
Clinical Presentation:
Granulomatous infection of skin, subcutaneous, fascia, bone usually in hands or feet
Painless but debilitating
Presentation:
Gardeners, potting soil
Diagnosis/Treatment:
Diagnosis
Grains in biopsy
Hyphae in grains
Treatment
Itraconazole or surgical removal
Candida (General)
Attributes:
Normal flora of the mouth, skin, vagina, gut
Pathogenesis:
Adhere to epithelial cells
endocytose into cells or penetrate into cells
causes apoptosis and necrosis
forms biofilms
Clinical Presentation:
Nail infection
Vulvovaginal candidasis
Oral thrust
Candidal Intertrigo
Diaper Dermatitis
Candidemia
Rare - Immunosuppressed patients
Most common fungal bloodstream infection in hospitalized patients
Neutropenic patients-chemotherapy
Patients with IVs and intravenous catheters
ICU / Central lines
Hyperalimentation/Total parenteral nutrition (TPN)
IV Drug Users
Can occur when gut Candida crosses intestinal epithelium and gains access to blood vessels
Presentation:
opportunist of skin or mucus membranes
Diabetes (sugar/yeast connection)
Infections identified by body location
Infants or inhaled topical steroids (asthma)
Esophagitis – HIV/AIDS patients
Diagnosis/Treatment:
Diagnosis
fungal detection in blood cultures
Detection of fungal Ag, Ab to Ag
PCR tests
Treatment
Nystatin, Clotrimazole, Amphotericin B, Miconazole
Candida Auris
Attributes:
Nosocomial, MDR
Yeast, no germ tubes, rarely forms hyphae
Clinical Presentation:
Fever and chills that don’t improve after antibiotic treatment for a suspected bacterial infection
Diagnosis/Treatment:
Diagnosis
Culture, staining (CHROM AGAR)
Often misidentified in automated systems
MALDI TOF MS is best
NA methods including sequencing
Treatment
Problematic with MDR
Echinocandins preferred
Multiple drugs together for synergism
Remove catheters
Don’t treat non-invasive
30-72% mortality rate
Aspergillus (Aspergillus Fumigatus)
Attributes:
Environmental
Pathogenesis:
Inhaled and reach alveoli
Clinical Presentation:
Pneumonia
allergies
aspergilloma “fungus ball”
Commonly in pulmonary TB cavities
Cough, Coughing up blood, Shortness of breath, Possibly fatigue and weight loss if chronic
Allergic Bronchopulmonary Aspergillosis (ABPA)
Classical Presentation
Asthma or CF patient
Recurrent episodes of cough, fever, malaise
Hemoptysis
brownish mucus plugs/casts
Diagnosis/Treatment:
Diagnosis
must see and ID the asexual conidium forming structure which is rare in vivo
Treatment
Steroids
Cryptococcosis (Neoformans & Gatti)
Attributes:
30 species, 2 pathogens
Environmental
Exposed in childhood, disease is reactivation of previous infections
NOT spread person to person
Chronic and Relapsing
Budding yeast with polysaccharide capsule
Pathogenesis:
Latent infection in alveolar macrophages
Depressed immunity, grow, disseminate, replicate
>100 proteins help establish virulence and protect from immune system
Yeasts in macrophage or not in macrophage invade CNS
CD4+ T cells and cytokines are primary response
Clinical Presentation:
Cough
Pulmonary: asymptomatic to visible on X-ray to life threatening pneumonia and ARDS
CNS: headache, fever, cranial neuropathies, altered mentation, lethargy, memory loss, and signs of meningeal irritation
Meningitis: neoformans
Presentation:
Immunocompetent=low risk
associated with immunocompromised
CD4 T cell defects
HIV pts
Diagnosis/Treatment:
Diagnosis
India ink
Latex agglutination test
Detects polysaccharide capsular antigens
Serum and CSF levels correlate with severity
Treatment
Amphotericin B formulations +/- flucytosine
Mucormycosis (Rhizopus & Mucor)
Attributes:
25% to 80% mortality
Pathogenesis:
Inhalation leads to pneumonia or rhinocerebral zygomycosis in facial sinuses
May invade deeper: orbital cellulitis, vascular thrombosis, coma, death
Both thrive in high glucose environments and during ketoacidosis
Clinical Presentation:
Severe sinusitis – fever, discharge, congestion, sinus pain
Necrosis of the palate
Erythema and cyanosis of skin over sinuses
Orbital pain and swelling
Black eschars
Facial numbness
Cavernous sinus thrombosis
Presentation:
Neutropenic, diabetic ketoacidosis, cancer pts, extreme malnutrition, trauma
Diagnosis/Treatment:
Treatment
Remedy underlying cause
Amphotericin B and Isavuconazole
Surgery
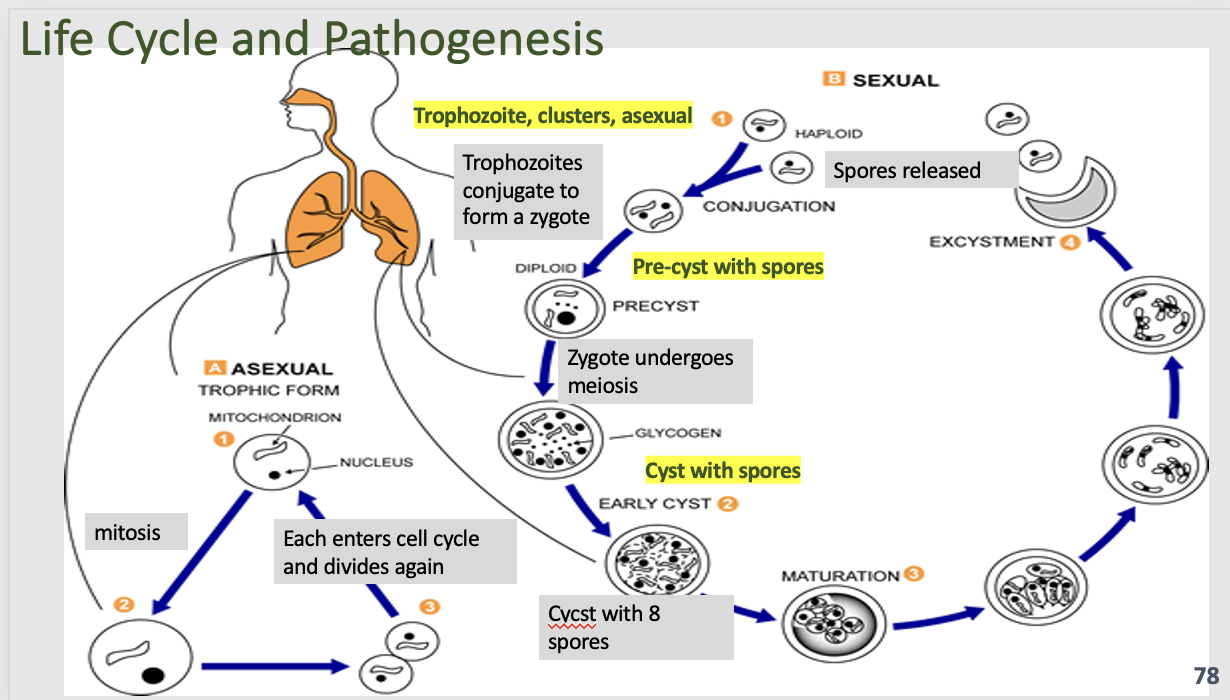
Pneumocystis Jirovecii
Attributes:
Common fungi we breath in all the time
25% to 80% mortality
Pathogenesis:
Spores attach to alveoli and replicated unimpeded
Hypoxemia
Impaired gas exchange capacity
Changes in total lung capacity and vital capacity
Clinical Presentation:
Diffuse bilateral infiltrates in the lung
Fever, Cough, Difficulty breathing, Chest pain, Chills, Fatigue
Presentation:
Immunocompromised (HIV*, transplant, corticosteroids, Chronic lung diseases, cancer, inflammatory diseases, autoimmune diseases)
Diagnosis/Treatment:
Diagnosis
Lung biopsy silver stain
Treatment
trimethoprim/sulfamethoxazole (TMP/SMX)
Fatal without Tx
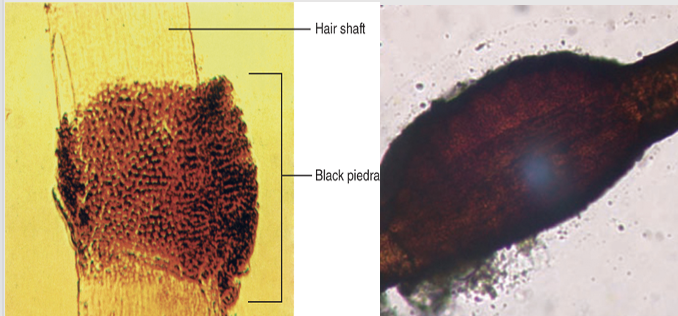
Piedraia Hortae
Black Piedra-hair with nodules of hyphae around the hair shaft appearing black
Hortae Werneckii
Tinea nigra-dark brown to black discolorations on the palm occurring more commonly in warm coastal regions among young women
Trichosporon spp
White piedra: Piedra-hair with nodules of hyphae around the hair shaft appearing white
Pityriasis versicolor (Malassezia Furfur)
discoloration or depigmentation and scaling of skin
Dimorphic
Infects as yeast, transforms into mycelia to spread
Superficial so not a true tinea
KOH prep shows hyphae and yeast
“Spaghetti and Meatballs”
factors: pregnancy, heat/humidity, immunodeficiency, oil/lotions, genetics
Multicolored hypopigmentation patches
Degrades lipids, produces acids
Damages melanocytes – causes hypopigmentation
Triggers: Tropical vacation, Hot & humid weather, Increased sweating. Commercial tropical skin oils
Frequently seen in adolescents- increased sebum
Tineas
Attributes:
fungal skin/hair/nail infection
Dermatophytes: Fungi that feed on keratin in skin, hair, and nails
Scaling of skin, loss of hair, crumbling of nail
Diagnosis/Treatment:
Diagnosis
Potassium hydroxide (KOH)
dissolves keratin & epidermal keratinocytes
Fungal elements visible in skin scrapings
Woods’ Lamp
Treatment
Depends on site/depth/seriousness
Topical treatment and/or systemic treatment
Azoles, amphotericin B and other polyenes, echinocandins
Tinea Pedis
Commonly known as athlete's foot, tinea pedis affects the feet, particularly the spaces between the toes and the soles. It can cause redness, itching, burning, scaling, and sometimes blisters and fissures.
Tinea Corporis
Also known as ringworm, tinea corporis affects the skin on the body, excluding the scalp, beard, groin, and feet. It presents as circular, red, scaly patches with a raised border that may be itchy or painful.
Tinea Capitis
This type of tinea affects the scalp and hair follicles. It is more common in children but can also occur in adults. Tinea capitis can cause hair loss, scaling, crusting, and sometimes swollen lymph nodes in the neck.
Tinea Cruris
Also called jock itch, tinea cruris affects the groin area, inner thighs, and buttocks. It presents as red, itchy, and often ring-shaped rashes with well-defined edges.
Tinea Unguium
Also known as onychomycosis, tinea unguium affects the nails, typically the toenails but can also affect fingernails. It can cause thickening, discoloration, crumbling, and deformity of the nails.
Lassa Fever Virus
Attributes:
Negative sense ssRNA viruses
2 segments of -ssRNA
BSL-4 due to human-human transmission
Exposure via droppings, contaminated food
1-3 week incubation
Vector: Mastomys Natalensis
Pathogenesis:
Clinical Presentation:
80% mild with slight fever, malaise, weakness headache
20% hemorrhaging, respiratory distress, facial swelling, pain, shock, neurological problems, encephalitis, multi-organ failure
1% of total dies, 10% during epidemics
3rd trimester pregnancies: 95% fetal mortality
Deafness develops in mild and serious cases
Presentation:
West Africa
Diagnosis/Treatment:
Diagnosis and Treatment
Detect IgM and IgG
RT-PCR
Culture
Supportive care
Ribavirin
Hantavirus
Attributes:
Negative sense ssRNA viruses
New World
Vectors (different but overlapping habitats): cotton rat, deer mouse, rice rat and white footed mouse
Pathogenesis:
Clinical Presentation:
Hantavirus Cardiopulmonary Syndrome (HCPS)
NEW WORLD
Rodent urine/feces/saliva
Flu-like symptoms, myalgia, cough, diarrhea,
Followed by rapid respiratory failure with pulmonary edema, cardiac shock
The Four corners (UT, CO, AZ, NM)
Hemorrhagic Fever with Renal Syndrome (HFRS) and NE (Nephropathia endemica)
Mortality 0.8% to 100%, dependent on virus, host genetics
Generally, mortality ranges up to 15%
OLD WORLD
Presentation:
Diagnosis/Treatment:
Crimean-Congo Hemorrhagic Fever
Attributes:
Negative sense ssRNA viruses
Most widely distributed hemorrhagic fever
Endemic in Africa, Europe, Asia, Mediterranean
Spread via contact with tick vector or from infected animals or humans via contaminated blood/body fluids
Hyalomma genus
Pathogenesis:
Clinical Presentation:
Incubation: 3-7 days (1-10 organisms!!)
Pre-hemorrhage: 4-5 days, headache, high fever, joint/back pain, vomiting, red eyes/throat, petechiae on palate, nonbloody diarrhea
Hemorrhage: petechiae, conjunctival hemorrhage, epistaxis, hematemesis, hemoptysis, and melena, possible hepatosplenomegaly
Presentation:
Diagnosis/Treatment:
Rift Valley Fever Virus
Attributes:
(-) ss segmented RNA virus, enveloped
Virus in cattle, sheep, livestock in Africa
Transmitted primarily through handling meat but also mosquitos directly
Increased mosquitos during excess rainfall
Negative sense ssRNA viruses
Pathogenesis:
Clinical Presentation:
Mild and self limiting with flu-like symptoms that can mimic meningitis
Presentation:
Diagnosis/Treatment:
California Encephalitis Disease
Attributes:
Mosquito-borne viruses in north central US (rare in CA)
Negative sense ssRNA viruses
Pathogenesis:
Clinical Presentation:
Primary viremia: Damages endothelial cells and lymphatic system, causes fever, drowsiness, disorientation
Secondary CNS localization: neurologic findings, seizures, encephalitis
Presentation:
Diagnosis/Treatment:
Nipah and Hendra Virus
Attributes:
Negative sense ssRNA viruses
Emerging zoonotic pathogens, outbreak frequency increasing
Transmitted from animals to humans via fruit bats, animal contact
Veterinary cross-protective vaccine under development, along with human vaccine
Pathogenesis:
Clinical Presentation:
Fever, headache, respiratory illness that can lead to encephalitis with seizures, coma and death
Presentation:
Diagnosis/Treatment:
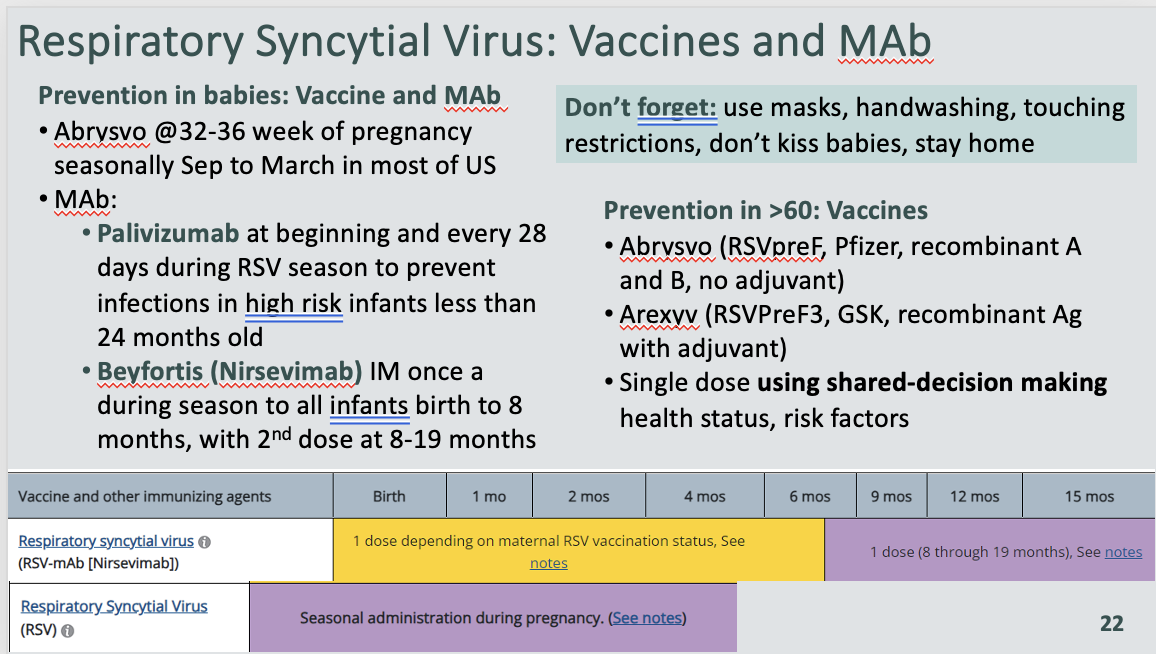
Respiratory Syncital Virus
Attributes:
Negative sense ssRNA viruses
A and B subgroups worldwide
Shed between 5 days and 3 weeks, prior to symptom onset
Symptoms overlap other respiratory symptoms
Problems for young and elderly
Pathogenesis:
Coughs, sneezes, droplets, fomites
Lives for many hours in hard surfaces
Almost all infected by 2 yrs
Immunity not protective so reinfections occur
Clinical Presentation:
mild URT to life threatening LRT
Infants/toddlers: most common cause of bronchiolitis
Young children: croup and tracheobronchitis
Elderly: tracheobronchitis, interstitial pneumonia
Presentation:
Sept-Mid december
Predisposing factors: preterm birth, smoking, lung disease, immunodeficiency, congenital heart disease
Diagnosis/Treatment:
Interstitial Lymphocytic Lung Infiltrates
Giant cells = Syncytia
No steroids or antibiotics
Rubulavirus (Mumps)
Attributes:
(-) ss RNA virus, enveloped
Pathogenesis:
Clinical Presentation:
Parotitis: inflamed/tender “chipmunk” parotid glands
30-40% of patients
Normally resolves in 1 week
Orchitis: exquisitely painful & inflamed testes
May cause sterility in post-pubertal adolescent male
Aseptic Meningitis
pre-vaccine: 15%
Causes fever, meningitis
Usually, self-limiting
Presentation:
Diagnosis/Treatment:
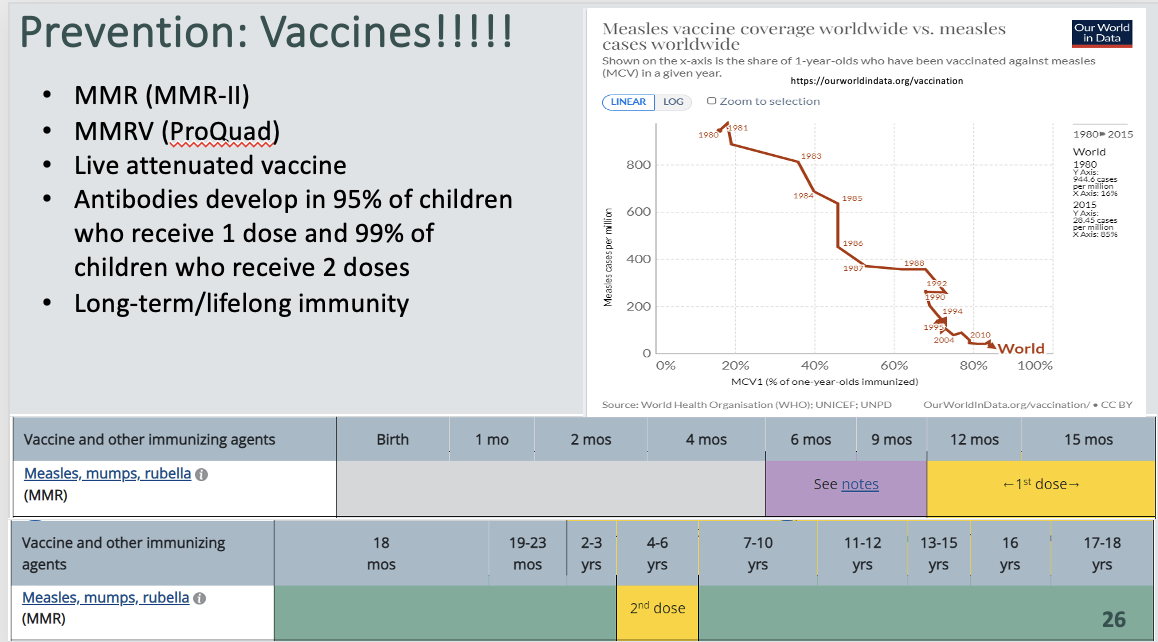
Morbillivirus (Measles)
Attributes:
(-) ss RNA virus, enveloped
Spread via respiratory droplets, aerosols
Contagious 4 days before rash-4 days after
Pathogenesis:
Clinical Presentation:
flu-like illness, conjunctivitis, swelling of eyelids, photophobia
high fever (~105°F), hacking cough, coryza, fatigue
Kopilik’s spots, rash
Red maculopapular (flat-to-bumpy) rapidly becomes confluent, spreads from head to face, to neck, to torso, to feet within 3 days
Blanches initially but not later
Rash disappears in same sequence it develops over 3-days
Presentation:
Diagnosis/Treatment:
No treatment
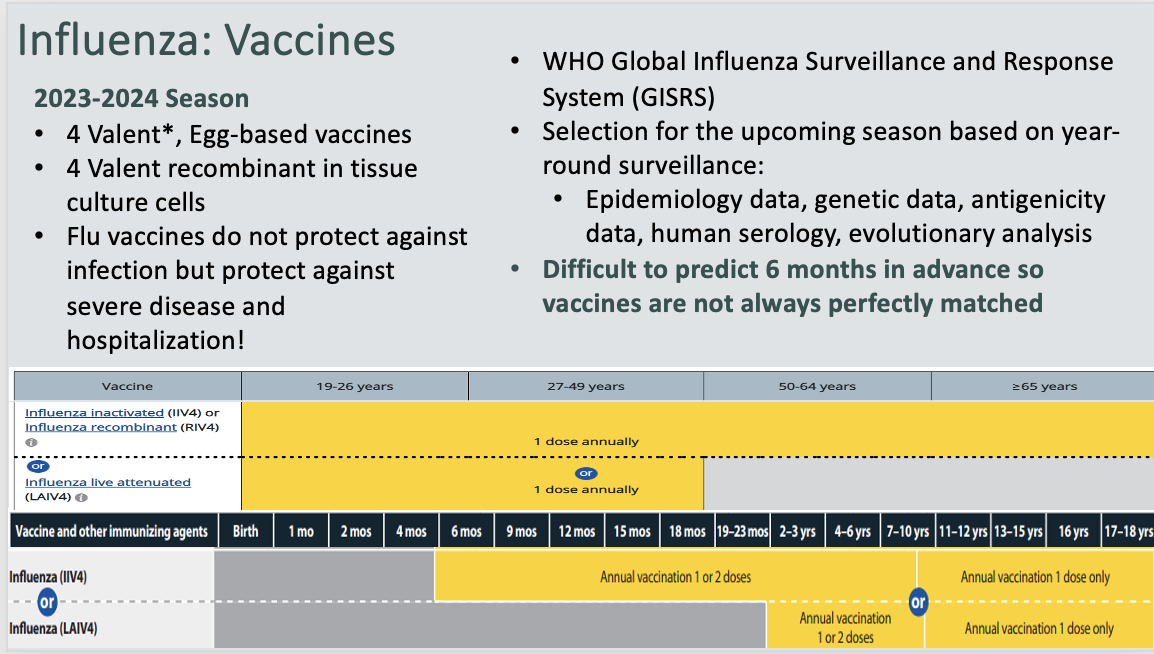
Influenza
Attributes:
(-) ss RNA virus, enveloped
Animal reservoirs: humans, birds, pigs, whales, more
Flu A: animals, subtypes
Flu B: less widespread (humans)
Flu C: rare (humans)
Transmission:
respiratory secretions and droplets
Survives 24-48 hours on hard surfaces but generally 4-9 hours
less on non-porous surfaces
Virus Specificity: sialic acids of different species have different internal linkages; HA subtypes are specific for particular sialic acids
Uses RDRP
Glycoprotein Spikes
Hemagglutinin(HA) : attach to sialic acid
•18 antigenic forms
Neuraminidase(NA): release/budding by cleaving sialic acid
•11 antigenic forms
Pathogenesis:
Clinical Presentation:
Mild and self limiting with flu-like symptoms that can mimic meningitis
Presentation:
Diagnosis/Treatment:
Zofluza inhibits the RDRP
Rapivab, Relenza, Tamiflu, Permivir, Zanamivir, Oseltamivir —> Block release of virus via neuraminidase
Rhabdovirus
Attributes:
(-) ss RNA virus, enveloped
Bullet Shape
There are no natural antibodies formed for rabies, so if you aren’t treated you will die
99% dogs or wildlife
Pathogenesis:
Clinical Presentation:
3 phases in humans:
Prodromal phase: non-specific symptoms
Excitation phase: hydrophobia, excitability, abnormal sensation; CNS disease obvious
Paralytic phase: apathy, stupor, coma, flaccid paralysis, vascular collapse and death
Presentation:
Diagnosis/Treatment:
Post-Mortem you will see Negri bodies
Two vaccines in US
RabAvert: GSK, chicken fibroblast culture, inactivated, processed, lyophilized
Pre-exposure vaccination for high-risk groups
Post exposure vaccination in all age groups
IMOVAX: human diploid cell vaccine, inactivated, processed, lyophilized
Post-exposure prophylaxis
Require 7-10 days to induce active immunity
Treatment
Exposed, early, no symptoms, never vaccinated: vaccine on day 0, 3, 7, 14 PLUS immune globulin (HRIG) AND regardless of the length of time between the bite and the ER
Exposed, early, no symptoms, vaccinated: additional vaccine doses
Exposed, with symptoms, never vaccinated: vaccine won’t work, immune globulin increases symptoms
•Palliative care because inevitably fatal…
Ebola Virus (Filoviridae)
Attributes:
(-) ss linear RNA virus, enveloped
6 strains: Zaire (80%), Sudan (60%), Tai Forest, Reston, Bombali, Bundibugyo
Pathogenic for humans, highly virulent
Hosts: chimpanzees, gorillas/African apes, monkeys, humans
Reservoir(s): unknown, possibly includes bats
Pathogenesis:
Clinical Presentation:
Hemorrhagic Fever
Persist in eye and testicles and likely other immune privileged sites
Presentation:
Diagnosis/Treatment:
rVSV-ZEBOV (Ervebo®)
•Single dose vaccine (Zaire)
•FDA approved in US: +18, Ebola responders, lab staff, treatment centers
•Approved by African countries for outbreak use
Vaccine: Zabdeno
•2-dose with 56-day booster (Zaire)
•Not appropriate for outbreaks unless already have first dose
•+>1 year old
Marburg Virus
Attributes:
(-) ss RNA virus, enveloped
severe hemorrhagic virus of human and non-human primates
Reservoir-African fruit bat
Human to human spread via body fluids accessing broken skin or mucus or fomites with body fluids
Pathogenesis:
Clinical Presentation:
2-21 day incubation
sudden fever, chills, headache, myalgia
5th day-rash on trunk, nausea, vomiting, stomach pain, diarrhea
RECOVERY possible OR
increasingly severe jaundice, pancreatitis, weight loss, delirium, shock, liver failure, massive hemorrhages, multi-organ failure
Presentation:
Diagnosis/Treatment:
MMR vaccines