EXAM 4: CNS Pt 1 and PNS + Dementia Drugs
1/107
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
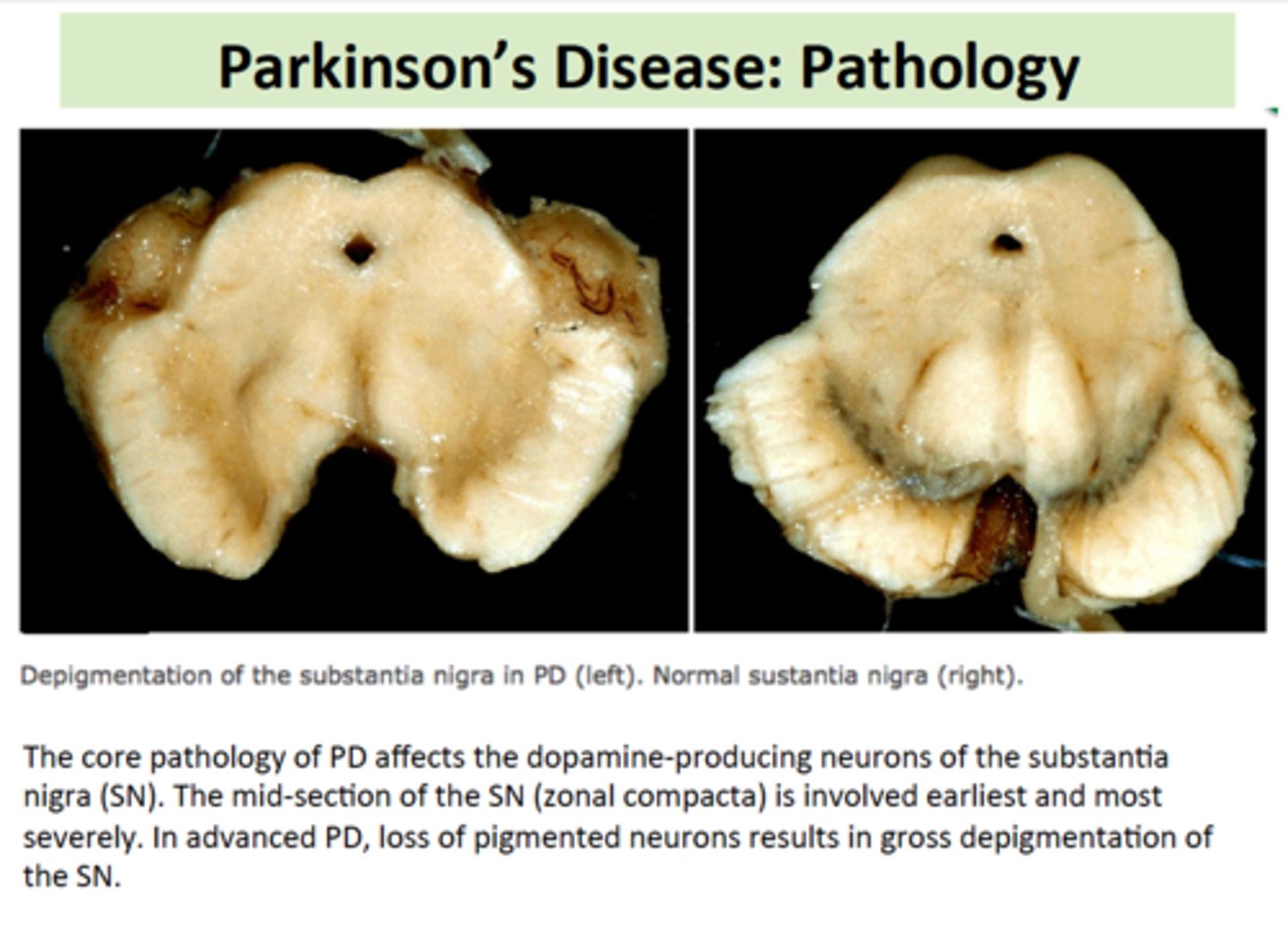
Parkinson's Disease Drug Management
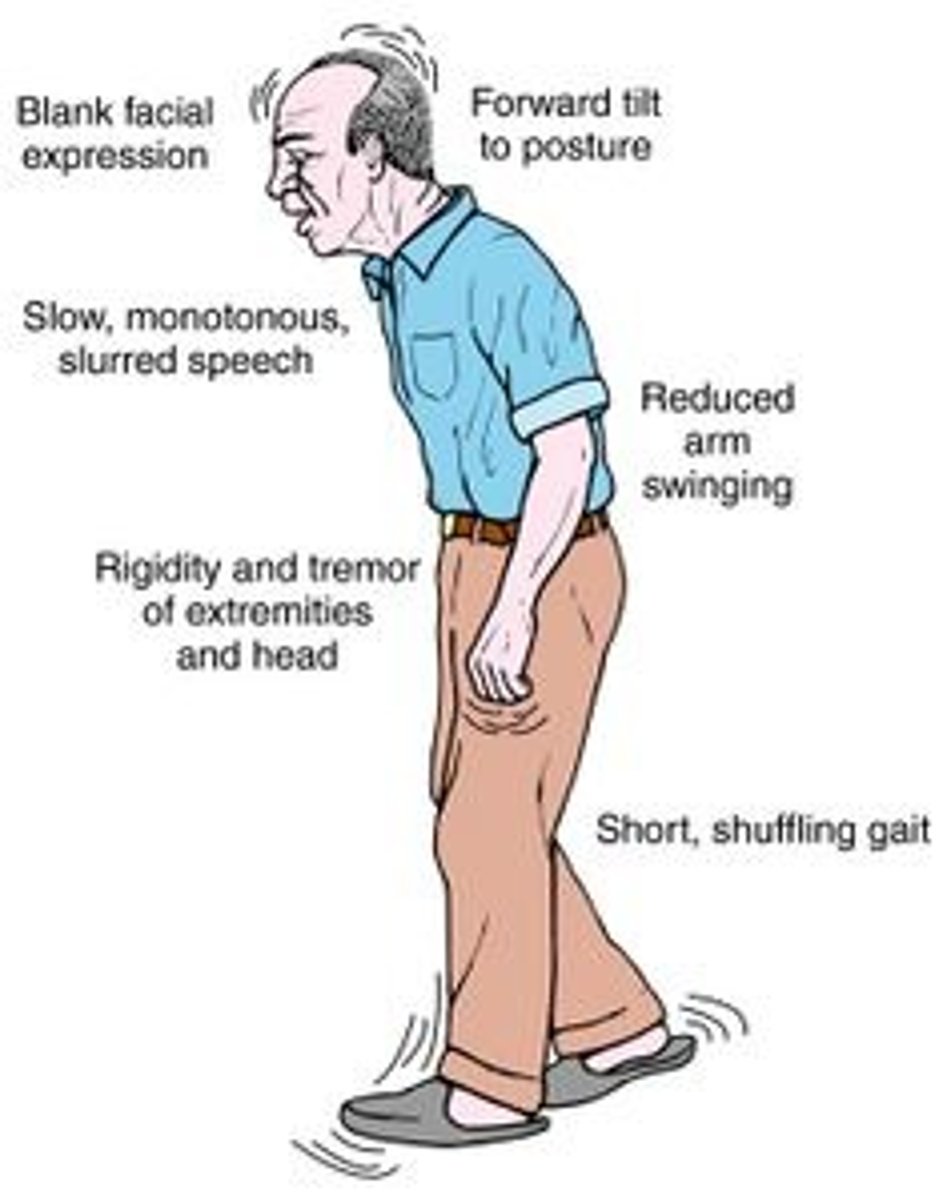
What is the underlying pathophysiology of Parkinson's Disease (PD)?
PD involves the malfunction and death of vital dopamine-producing neurons in the substantia nigra of the basal ganglia. Symptoms appear when approximately 80% of stored dopamine is depleted.
What is the relationship between dopamine and acetylcholine (ACh) in PD?
PD is characterized by an imbalance where there is too little dopamine and a relative overabundance of acetylcholine.
⬇️Dopamine ⬆️ACh
What is the MOA for Levodopa?
Relieves motor symptoms by conversion to dopamine (by decarboxylase) in surviving nerve terminals in the brain (striatum), increasing dopamine concentration and enhancing neurotransmission.
🌟So basically, Levodopa turns into dopamine in the brain, boosting levels, so nerve signals work better, and movement symptoms get better.
What are the limitations of Levodopa therapy?
⁕ Benefits diminish over time
⁕ It generally works for 2-5 years.
⁕ Full therapeutic effect can take months to develop.
What is the "On-Off" phenomenon associated with Levodopa?
A loss of response over time characterized by gradual "wearing off" at the end of a dose or abrupt loss of effect at any time.
What are the dietary restrictions for Levodopa?
⨀ Avoid high-protein meals → protein blocks levodopa absorption and entry into the brain
⨀ Protein competes with levodopa in the intestines and at the blood-brain barrier
⨀ Vitamin B6 can reduce the effectiveness of levodopa (when taken alone)
In the combination drug Sinemet (Levodopa/Carbidopa), what is the role of Carbidopa?
Carbidopa has no benefit alone; it prevents the breakdown of Levodopa in the gut (periphery), allowing more Levodopa to reach the CNS and reducing the required dose by 75%.
What are the potential side effects/adverse effects of Sinemet?
Nausea and vomiting
Postural hypotension (drop in BP when standing)
Arrhythmias (irregular heartbeat)
Psychosis (~20%)
Dyskinesias (~80%)
Harmless red/brown discoloration of urine, sweat, or saliva
What is the MOA of Dopamine Agonists?
Direct activation of dopamine receptors in striatum
What are the two types of dopamine agonists?
•Derivatives of ergot - less selective for DA
•Nonergot derivatives (next slide) - highly selective for DA receptors & less SE
What are the Nonergot derivatives drugs?
Pramipexole (Mirapex)
Ropinirole (Requip)
How do Non-ergot Dopamine Agonists (Pramipexole, Ropinirole) compare to Levodopa?
They are less effective than Levodopa but do not compete with dietary proteins and have a lower incidence of response failure and dyskinesias.
What are the adverse effects of newer non-ergot dopamine agonists when used as monotherapy?
Nausea
Dizziness
Daytime sleepiness ("sleep attacks")
Insomnia
Constipation
Weakness
Hallucinations
What is the Ergot-derived dopamine agonist drug?
Bromocriptine (Parlodel).
What is the Mechanism of Action (MOA) for Bromocriptine?
It activates pre-synaptic dopamine receptors to stimulate the production of more dopamine.
What are the primary adverse reactions to Bromocriptine?
GI upset
Dyskinesia
Sleep disturbances
What are the adverse effects when newer dopamine agonists are combined with levodopa?
Orthostatic hypotension
Dyskinesias
Increased hallucinations
What is the role and MOA of COMT Inhibitors (Entacapone)?
They have no direct effect alone
They block the COMT enzyme that breaks down dopamine to prolong the time Levodopa is available to the brain.
Why are Anticholinergic drugs (Cogentin) used in Parkinson's?
To block receptors for ACh, which helps:
- Control tremors
- Decreases rigidity (cogwheeling)
- Reduces drooling (sialorrhea)
What is the mnemonic for cholinergic effects (what anticholinergics oppose)?
SLUDGE:
Salivation
Lacrimation
Urination
Diarrhea
GI motility
Emesis
What are the side effects of Anticholinergic drugs like Cogentin?
Tachycardia
Urinary retention
Constipation
Dry throat
Confusion
Blurred vision / increased intraocular pressure (IOP)
What are the Nursing Interventions for patients on Anticholinergic drugs? 👩🏾⚕️
👩🏾⚕️Provide ice chips or sugarless candy for dry mouth
👩🏾⚕️Increase fluids and fiber for constipation
👩🏾⚕️Monitor for urinary retention
Epilepsy and Anticonvulsant Drug Management
What is the Mechanism of Action (MOA) for Phenytoin (Dilantin)?
It stabilizes nerve cells to keep them from getting overexcited by modulating sodium channels, calcium flux, and enhancing sodium-potassium ATPase activity. It only works when neurons are hyperexcitable.
🌟So basically, it calms overactive nerve cells so they don't fire too much.
Why are Phenytoin and Dilantin NOT interchangeable?
Phenytoin and Dilantin aren't interchangeable because they are absorbed differently, which can change blood drug levels.
What are the indications (uses) for Phenytoin (Dilantin)?
Complex partial seizures and Tonic-clonic seizures. It is used for all major forms of epilepsy EXCEPT absence seizures.
What are the side effects and adverse effects of Phenytoin (Dilantin)?
Nystagmus
Diplopia
Sedation
Cognitive impairment
Hirsutism
Gingival hyperplasia (~20%)
Increased suicidal ideation
Skin reactions (SJS/TEN)
Cardiovascular effects (hypotension, dysrhythmias)
What is the therapeutic range for Phenytoin, and how is toxicity recognized?
Range: 10-20 mcg/mL. Toxicity levels:
20-30: Nystagmus.
30-40: Ataxia, slurred speech, hand tremors.
> 40: Decreased LOC.
What is the pregnancy category for Phenytoin (Dilantin)?
Category D (teratogenic).
What is the MOA for Carbamazepine (Tegretol)?
The mechanism of action is the same as phenytoin (modulates sodium channels).
What are the indications for Carbamazepine (Tegretol)?
Partial seizures
Generalized tonic-clonic seizures
Mixed seizure types
Complex partial seizures (drug of choice)
Trigeminal neuralgia pain
Bipolar disorder
What are the side effects and adverse effects of Carbamazepine (Tegretol)?
Diplopia
Blurred vision
Nausea and vomiting
Leukopenia
SIADH (low sodium)
Bone marrow suppression
Photosensitivity
What is the pregnancy category for Carbamazepine (Tegretol)?
Category D
What is the MOA for Valproic Acid (Depakote)?
It is thought to increase GABA (an inhibitory neurotransmitter) and have a direct membrane-stabilizing effect.
What are the indications for Valproic Acid (Depakote)?
Absence seizures
Myoclonic seizures
Tonic-clonic seizures
Partial seizures
Neonatal seizures
Migraine prevention
Bipolar disorder
What are the side effects and adverse effects of Valproic Acid (Depakote)?
Nausea and vomiting (N/V)
Lethargy
Impaired PT & PTT
Hair loss
Leukopenia
Liver toxicity
Drowsiness
Ataxia
What is the pregnancy category for Valproic Acid (Depakote)?
Category X
What is the primary use for Gabapentin (Neurontin)?
Adjuvant for partial seizures and widely used for neuropathic pain
What is the MOA of Gabapentin (Neurontin)?
Thought to bind to a carrier protein resulting in elevated GABA in the brain.
What are the adverse effects of Gabapentin (Neurontin)?
Fatigue
Somnolence (sleepiness)
Dizziness
Ataxia (loss of coordination)
Leukopenia (low white blood cells)
What is the use of Lamotrigine (Lamictal)?
Adjuvant treatment for partial seizures (adults)
Generalized seizures (children under 2)
Bipolar disorder
What is the MOA for Lamotrigine (Lamictal)?
Blocks sodium channels, inhibiting the release of glutamate and aspartate while enhancing GABA release.
What are the adverse effects of Lamotrigine (Lamictal)?
Dizziness
Ataxia
Somnolence (sleepiness)
Headache
Diplopia (double vision)
Nausea and vomiting (N/V)
Rash
What is the Black Box Warning for Lamotrigine (Lamictal)?
Stevens-Johnson Syndrome (SJS) related to a generalized erythematous rash.
What are the unique uses for Topiramate (Topamax)?
Partial and primary generalized seizures, prevention of migraines, and weight loss.
What is the MOA of Topiramate (Topamax)?
Blocks the spread of seizure, blocks sodium channels, enhances GABA activity, and antagonizes glutamate.
What are the adverse effects of Topiramate (Topamax)?
Drowsiness
Dizziness
Confusion
Memory loss
Paresthesia (tingling)
Weight loss/loss of appetite (anorexia)
Decreased folate and vitamin B12 levels
What is the use of Levetiracetam (Keppra)?
Partial seizures and adjuvant for generalized, partial, and myoclonic seizures.
What is the MOA of Levetiracetam (Keppra)?
Binds to synaptic vesicle glycoprotein SV2A to inhibit presynaptic calcium channels, acting as a neuromodulator to impede impulse conduction.
What is the Drug of Choice (DOC) for Absence Seizures?
Ethosuximide (Zarontin)
What is the MOA of Ethosuximide (Zarontin)?
Opens calcium channels leading to inhibition of neuron firing.
What are the patient teaching points for anticonvulsants? 👩🏾⚕️
Take exactly as prescribed; do not stop abruptly.
Take with food to reduce GI upset.
Wear a medical alert bracelet.
Avoid hazardous activities/driving until the effects are known.
Phenytoin may discolor urine pink or red-brown.
Heavy alcohol use diminishes drug benefits.
Drugs to Manage Muscle Spasms/ Spasticity

What is the difference between a muscle spasm and spasticity?
Muscle spasm is an involuntary contraction of a muscle or muscle group that is usually self-limiting.
Spasticity is abnormal muscle tightness due to prolonged contraction caused by damage to the CNS (e.g., MS, Cerebral Palsy), characterized by stiff muscles that resist stretching and increased Deep Tendon Reflexes (DTRs).
What are the Centrally Acting Muscle Relaxants?
•Carisoprodol (soma)
•Chlorzoxazone (Lorzone)
•Cyclobenzaprine (Flexeril)
•Metaxalone (Skelatxin)
•Methocarbamol (Robaxin)
•Orphendrine (Norflex)
Tizanidine (Zanaflex)
What is the Mechanism of Action (MOA) and usage for Centrally Acting Muscle Relaxants?
They work at different receptors in the brain to relieve local muscle spasm, decrease local muscle pain, and increase Range of Motion (ROM). Note: They are NOT for spasticity.
What are the adverse effects of Centrally Acting Muscle Relaxants?
General CNS depression (drowsiness, dizziness)
Hepatic toxicity (Tizanidine, Metaxalone)
Physical dependence with long-term use
Withdrawal/abstinence syndrome after long-term use
What is the recommended length of time for using Centrally Acting Muscle Relaxants?
They are taken for a short time, typically 2 to 3 weeks; they are not meant for chronic use.
What are the therapeutic uses for Baclofen (Lioresal)?
It is the Drug of Choice (DOC) for spasticity associated with spinal cord injury (paraplegic or quadriplegic), Multiple Sclerosis, and trauma.
What are the adverse effects and risks of Baclofen (Lioresal)?
General CNS depression (drowsiness, dizziness)
Abrupt stopping of intrathecal baclofen can cause severe withdrawal
Withdrawal effects: high fever, altered mental status, seizures, rhabdomyolysis, and death
What is the MOA for Dantrolene (Dantrium)?
It acts directly on skeletal muscle by suppressing the release of calcium from the sarcoplasmic reticulum (SR).
What are the adverse effects of Dantrolene (Dantrium)?
Liver toxicity (hepatic toxicity)
Muscle weakness
Drowsiness
Diarrhea
Acne-like rash
What is Malignant Hyperthermia?
It is a potentially fatal condition triggered by succinylcholine and general anesthetics.
Who is at risk for Malignant Hyperthermia?
People who carry a specific gene for it are at risk, though they may never develop symptoms until exposed to triggers.
What are the signs and symptoms of Malignant Hyperthermia?
Very high fever (up to 113°F)
Severe muscle rigidity (especially jaw)
Fast heart rate (tachycardia)
Fast breathing (tachypnea)
Flushed skin
Brown/cola-colored urine
How is Malignant Hyperthermia managed?
Stop the triggering inhaled gas immediately
Start IV fluids
Rapid cooling (ice, cooling measures)
Give IV dantrolene (the only effective antidote)
CNS Stimulants
What is the Mechanism of Action (MOA) for Methylphenidate?
It is thought to work by increasing levels of dopamine and norepinephrine by blocking their reuptake, enhancing presynaptic release, and inhibiting MAO.
What are the therapeutic uses for Stimulants like Methylphenidate?
ADHD (reduced impulsiveness/hyperactivity, improved attention span)
Chronic illness-related fatigue
Narcolepsy
What are the common adverse effects of Methylphenidate?
Dizziness
Insomnia
Seizures
Palpitations/angina
Arrhythmias
Abdominal pain
Rash
Thrombocytopenia
Hypertension
Increased blood sugar
Dry mouth
What is the abuse potential for Stimulants?
They are highly abused substances; close monitoring is required.
What are the instructions for the timing of Methylphenidate administration?
Give the drug 4 to 6 hours before bedtime to avoid sleep interference.
What should a patient avoid while taking Stimulants?
Avoid hazardous activities until CNS effects are known and avoid drinks containing caffeine, as they increase the effect of amphetamines.
How should the drug be discontinued after prolonged use?
Reduce the dosage gradually to prevent acute rebound depression.
What specific parameters must be monitored in children taking Stimulants?
Monitor height and weight closely, as stimulants may affect growth or stunt growth. 👩🏾⚕️👶🏼
What should be monitored in adult and Diabetic (DM) patients taking Methylphenidate? 👩🏾⚕️👩🏽🦰
Check blood pressure (especially when starting) and monitor glucose levels.
Anti-Migraine Medications

What is the MOA for Serotonin Agonists (Triptans)?
They bind with serotonin receptors on blood vessels, leading to constriction and inhibition of pro-inflammatory neuropeptide release (inflammation).
What are the COMMON adverse effects of Triptans?
Dizziness
Weakness
Nausea
Sleepiness
Medication overuse headache
What are the SERIOUS adverse effects of Triptans?
Heart attack
Stroke
Serotonin syndrome
Severe stomach pain
Hypertension
Allergic reactions (rash)
What are the contraindications for Triptans?
Heart problems (e.g., Prinzmetal angina)
Dyslipidemia
Hypertension
History of stroke
Peripheral arterial disease
Seizure disorder
Liver disease (hepatitis, cirrhosis)
What are the side effects/adverse effects of Ergot Alkaloids (Ergotamines)?
Nausea and vomiting
Cold or clammy hands/feet
Muscle pain
Dizziness
Hypertension
Severe allergic reactions
What are the risks of long-term Ergotamine use?
Dependence and withdrawal symptoms.
What is the Black Box Warning for Botox when used for chronic migraines?
Possible spread of the toxin beyond the injection site, resulting in dysphagia (difficulty swallowing) and breathing difficulties.
Peripheral Nervous system drugs + Drugs for Dementia
What are the two classes of drugs used to manage Alzheimer's dementia?
Cholinesterase Inhibitors and NMDA Antagonists.
What is the MOA for Cholinesterase Inhibitors in Alzheimer's disease?
They prevent the breakdown of Acetylcholine by acetylcholinesterase, increasing its availability at CNS cholinergic synapses.
✨They stop acetylcholine from being broken down, so more of it stays available in the brain.
What is the MOA for NMDA Antagonists like Memantine?
They act as an NMDA receptor antagonist.
What are the common adverse effects of Cholinesterase Inhibitors?
Nausea
Vomiting
Dyspepsia (indigestion)
Diarrhea
Dizziness
Headache
Dose-dependent bradycardia (slow heart rate)
How effective are Cholinesterase Inhibitors for Alzheimer's patients?
Benefits are modest and short-lasting, with only about 1 in 12 patients experiencing clinical benefit.
What is the MOA of Bethanechol?
It is a reversible muscarinic agonist that acts only on muscarinic receptors.
What is the primary clinical indication for Bethanechol?
Relieving urinary retention in postoperative and postpartum patients.
What are the major adverse effects of Bethanechol?
Hypotension
Bradycardia
Excessive salivation
Increased gastric acid
Abdominal cramps
Diarrhea
Asthma exacerbation
What is the clinical indication for Oxybutynin?
Overactive bladder and urgency incontinence caused by inappropriate detrusor muscle contractions.
What are the common side effects of Oxybutynin?
Dry mouth
Constipation
Tachycardia
What is the MOA of Atropine?
It competitively antagonizes acetylcholine and other cholinergic agonists at muscarinic receptors.
List four clinical indications for Atropine.
1️⃣Symptomatic bradycardia
2️⃣Preoperative secretion reduction
3️⃣Adjunct for peptic ulcer / GI disorders
4️⃣Antidote for muscarinic agonist poisoning
What are the primary contraindications for Atropine?
Glaucoma
Intestinal atony
Urinary obstruction
Tachycardia
Why should Atropine be used with caution in patients with asthma?
It carries a risk of thickening airway secretions.