Adv chemistry exam 2
5.0(2)
Studied by 88 peopleCard Sorting
1/107
Earn XP
Description and Tags
Last updated 9:57 PM on 12/6/22
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
108 Terms
1
New cards
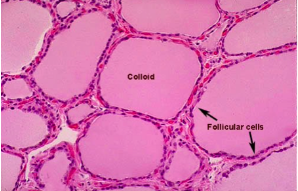
Thyroid anatomy:
2
New cards
TSH vs fT4 graph

3
New cards
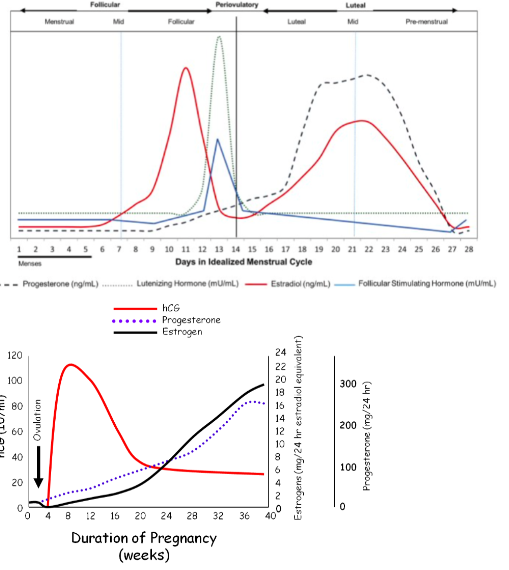
Female pituitary & sex steroids through course of menstrual period, and pregnancy
4
New cards
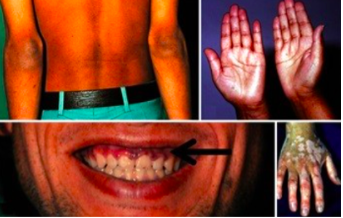
Primary adrenal Insufficiency:
hyperpigmentation
5
New cards
Cushing’s disease
striae

6
New cards
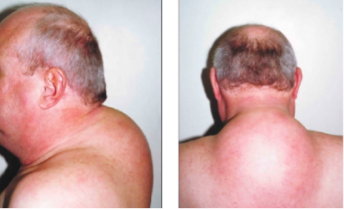
cushing's disease
supraclavicular fat deposits (buffalo hump)
7
New cards
cushing's disease
moon face (corticosteroid-induced lipodystrophy)

8
New cards
Grave’s disease
primary hyperthyroidism

9
New cards
goiter
hypothyroidism

10
New cards
thyroid eye disease

11
New cards
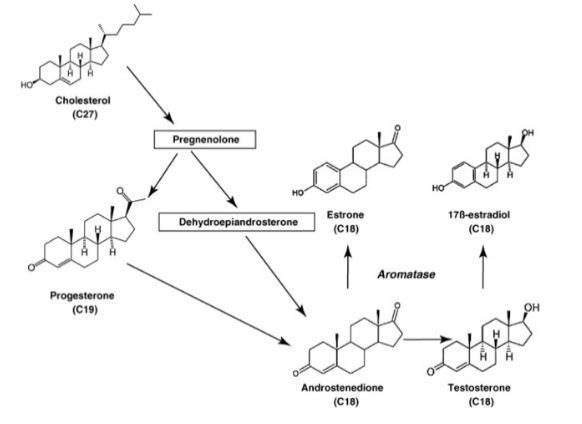
Aromatic steroid hormones
cholesterol, progesterone, estrone, androstenedione, testosterone, 17B-estradiol
12
New cards
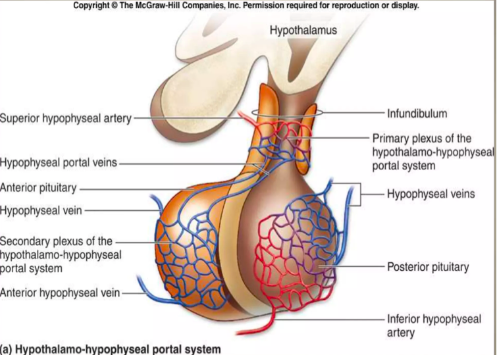
Hypothalamic-Pituitary portal circulation
13
New cards
What pituitary hormone in excess causes goiter?
Prolonged elevation of TSH (thyroid stimulating hormone) levels due to iodine or hypothyroidism
14
New cards
What pituitary hormone deficiency causes adrenal atrophy and failure?
Deficiency in production of ACTH (adrenocorticotropic hormone)
15
New cards
Anterior pituitary hormones:
SH (Thyroid-stimulating hormone),
ACTH (adrenocorticotropic hormone),
HGH (Human Growth hormone),
LH (Luteinizing hormone),
FSH (stimulating follicle hormone),
PRL (prolactin)
ACTH (adrenocorticotropic hormone),
HGH (Human Growth hormone),
LH (Luteinizing hormone),
FSH (stimulating follicle hormone),
PRL (prolactin)
16
New cards
Posterior pituitary hormones:
Oxytocin, antidiuretic hormone (arginine vasopressin)
17
New cards
Most common two pituitary adenomas
Somatotrophs Growth Hormone
Prolactin
Prolactin
18
New cards
Effect of hyperprolactinemia in males and females
Suppresses ovulation in both genders
- Males: infertility, lactation in male, breast development
- Females: infertility, menstrual irregularity
- Males: infertility, lactation in male, breast development
- Females: infertility, menstrual irregularity
19
New cards
Negative feedback players on TRF/TSH & ACTH
TRF/TSH: Triiodothyronine (T3)
ACTH: Cortisol
ACTH: Cortisol
20
New cards
Components of POMC
Secretion of ACTH and melanocyte stimulating hormones.
Y-MSH, ACTH (a-MSH and CLIP), and B-Lipotropin (Y-lipotropin (B-MSH), B-endorphin)
ACTH secreted as part of Proopiomelanocortin (POMC) precursor with melanocyte stimulating hormones
Y-MSH, ACTH (a-MSH and CLIP), and B-Lipotropin (Y-lipotropin (B-MSH), B-endorphin)
ACTH secreted as part of Proopiomelanocortin (POMC) precursor with melanocyte stimulating hormones
21
New cards
Function of thyroglobulin in physiology & thyroid cancer
Synthesized by follicular cells
Thyroglobulin (TG): useful as a post-treatment tumor marker of residual thyroid cancer
Useful tumor marker for post-treatment for differentiated thyroid cancer (recurrence)
Thyroglobulin (TG): useful as a post-treatment tumor marker of residual thyroid cancer
Useful tumor marker for post-treatment for differentiated thyroid cancer (recurrence)
22
New cards
ID Most potent thyroid hormone & most potent androgen
Thyroid hormone: T3 (Triiodothyronine)
Androgen: Dihydrotestosterone (DHT)
Androgen: Dihydrotestosterone (DHT)
23
New cards
Match receptor type (Tyrosine Kinase)
T3 (Triiodothyronine)
24
New cards
Match receptor type: GCPR (G-protein coupled receptor)
trophic hormones – TSH (Thyroid stimulating hormone)
25
New cards
Match receptor type: Nuclear Steroid (glucocorticoid receptor
cortisol, thyroxine (T4), Triiodothyronine (T3)
26
New cards
What laboratory test(s) aid in identifying Congenital Hypothyroidism
Spot test for babies
27
New cards
What laboratory test(s) aid in identifying Chronic lymphocytic (Hashimoto’s) thyroiditis
autoantibody panels: serum anti-TPO, blocking TSIs or less sensitive anti-TG -- Anti TSH receptor antibody panel, Anti TPO, anti-thyroglobulin
28
New cards
What laboratory test(s) aid in identifying Graves’ disease
Autoantibody TSI, Antibodies screen or panel. Includes some of Hashimoto’s tests like Anti-TSH receptor antibody panel, Anti-TPO, anti-thyroglobulin test
29
New cards
What laboratory test(s) aid in identifying Subclinical hypothyroidism
perform a panel for T3, T4, TSH. Results Normal T3 and T4, high TSH
30
New cards
What laboratory test(s) aid in identifying Cushing’s Syndrome and Diseases
-Disease due to pituitary adenoma (Secondary cause of cortisol excess).
-Syndrome caused by cortisol excess from Stress, Cushing’s disease (cortisol excess from pituitary adenoma), Cushing’s syndrome (cortisol excess from any cause), Adrenal adenoma, Ectopic ACTH syndrome (paraneoplastic syndrome)
-Syndrome caused by cortisol excess from Stress, Cushing’s disease (cortisol excess from pituitary adenoma), Cushing’s syndrome (cortisol excess from any cause), Adrenal adenoma, Ectopic ACTH syndrome (paraneoplastic syndrome)
31
New cards
What laboratory test(s) aid in identifying
Primary Adrenal Insufficiency (Addison’s disease)
Primary Adrenal Insufficiency (Addison’s disease)
-Cosyntropin Stimulation test (Cosyntropin is hR ACTH fragment. Low dose stimulation (1ug) elicits cortisol peak of >18 ug/dL. (Used for suspected cortisol insufficiency)
-Dexamethasone suppression test (used for suspected cortisol excess)
-Dexamethasone suppression test (used for suspected cortisol excess)
32
New cards
What laboratory test(s) aid in identifying 21-hydroxylase (Congenital Adrenal Hyperplasia)
elevated 17-beta-hydroxyprogesterone levels, androgen, and cortisol
33
New cards
What laboratory test(s) aid in identifying Growth Hormone deficiency
provocative testing: stimulation tests using insulin-induced hypoglycemia or GHRH or suppression test. low IGF-1 (insulin-like growth factor-1 – surrogate marker – synthesized by liver).
-IGF-1 assay is preferred for GH deficiency or excess.
-GH secretion by pituitary adenoma: 75g oral glucose load suppression – adenoma not suppressed
-IGF-1 assay is preferred for GH deficiency or excess.
-GH secretion by pituitary adenoma: 75g oral glucose load suppression – adenoma not suppressed
34
New cards
Thyroid storm (Thyrotoxic crisis):
heart - acute exacerbation of thyrotoxicosis and presenting cardiac abnormalities.
35
New cards
Myxedema
Low T3, Low T4, high TSH. Severe hypothyroidism, Unresponsive hypometabolic state. Treatment: replacement hormone (levothyroxine).
36
New cards
Adrenal crisis (adenosine crisis)
hypoglycemia, hyperkalemia, mineralocorticoid deficiency, fluid imbalance.
37
New cards
Primary hyperthyroidism (Grave’s disease)
thyroid stimulating immunoglobulins (autoantibodies -TSI) activate TSH receptors causing over secretion of T4 and T3. Low TSH.
38
New cards
Secondary hyperthyroidism
pituitary function issue. Decreased TSH
39
New cards
Tertiary hyperthyroidism
hypothalamic issue. Decreased TSH.
40
New cards
Clinical findings of primary, secondary, and tertiary hyperthyroidism
anxiety, emotional lability, weak, tremor, palpitations, heat intolerance, increased perspiration, weight loss despite normal or increased appetite (thyroid storm/thyrotoxicosis
41
New cards
lab tests for primary, secondary, and tertiary hyperthyroidism
low TSH, overt hyperthyroidism
42
New cards
Primary hypothyroidism
increased serum TSH. Low Free T4
43
New cards
Secondary hypothyroidism
due to pituitary TSH deficiency. TSH normal or low. FT4 low.
44
New cards
Tertiary hypothyroidism
due to hypothalamic TRH deficiency
45
New cards
Clinical findings of primary, secondary, and tertiary hypothyroidism
fatigue, cold intolerance, weight gain, constipation, dry skin, myalgia, menstrual irregularities, bradycardia, hypertension, delayed relaxation phase of deep tendon reflexes (myxedema coma)
46
New cards
lab tests for primary, secondary, and tertiary hypothyroidism
elevated TSH, low Free T4. Majority of patients with Hashimoto’s (autoimmune thyroiditis) have elevated thyroid peroxidase (TPO) autoantibodies
47
New cards
Primary adrenal insufficiency (Addison’s disease)
deficiency in glucocorticoids or mineralocorticoids resulting in adrenocortical insufficiency resulting in destruction or dysfunction of Cortex. Produces renal wasting and potassium retention leading to severe dehydration. Hypotension, hyponatremia, hyperkalemia, and acidosis
48
New cards
Secondary adrenal insufficiency
deficiency in secretion of pituitary ACTH (adrenocorticotropic hormone). Caused by exogenous glucocorticoid therapy.
49
New cards
Tertiary adrenal insufficiency
deficiency in secretion of corticotropin-releasing hormone (CRH) from hypothalamus.
50
New cards
clinical findings in adrenal insufficiency
weak and fatigue, anorexia, weight loss, GI issues, nausea, vomiting, hyperpigmentation
51
New cards
lab tests in adrenal insufficiency
Cosyntropin stimulation test and rapid ACTH stimulation test. Hypoglycemia, hyperkalemia, hyponatremia, hypotension.
52
New cards
Cushing’s syndrome
from any cause including stress
53
New cards
Cushing’s disease
cortisol excess from pituitary adenoma, ACTH
54
New cards
clinical findings in cushing's
striae, supraclavicular and other fat deposits (buffalo hump, moon-face), delayed wound healing, impaired immune response.
55
New cards
lab tests for cushing's
Plasma ACTH, salivary, and 24 hr urinary cortisol, dexamethasone suppression test
56
New cards
21-Hydroxylase deficiency (CAH)
over secretion of adrenal androgens in females
57
New cards
clinical signs of 21-Hydroxylase deficiency (CAH)
females: excess adrenal androgens, virilization of fetus due to androgen excess, acne, hirsutism, clitoromegaly.
males: (Hercules)
males: (Hercules)
58
New cards
tests for 21-Hydroxylase deficiency (CAH)
neonatal testing of elevated 17-beta-hydroxyprogesterone levels
59
New cards
Cosyntropin stimulation test
Cosyntropin is hR ACTH fragment with biological activity towards adrenal receptors. Low dose stimulation elicits cortisol peak >18 ug/dL in 1-2 hrs.
60
New cards
Dexamethasone suppression test
has potent negative feedback on ACTH release. High dose: 8 mg, most people with Cushing’s disease suppress, those with ectopic ACTH syndrome do not. Low dose: 1mg, AM cortisol >14, Cushing’s syndrome suspected.
61
New cards
Thyrogen stimulation test
synthetic TSH given to stimulate thyroid and unmask residual cancer
62
New cards
Provocative test
for growth hormone excess and deficiency – suppression and stimulation
GH secretion by pituitary adenoma: 75g oral glucose load suppression – adenoma not suppressed
GH deficiency: stimulation tests using insulin-induced hypoglycemia or GHRH
GH secretion by pituitary adenoma: 75g oral glucose load suppression – adenoma not suppressed
GH deficiency: stimulation tests using insulin-induced hypoglycemia or GHRH
63
New cards
Iodine Deficiency
causes goiter (enlargement) – hypothyroidism – main one
64
New cards
Rate limiting step in steroid biosynthesis induced by ACTH
Conversion of cholesterol to Pregnenolone
65
New cards
Identify TPO inhibitors
Methimazole
Propylthiouracil (PTU)
Propylthiouracil (PTU)
66
New cards
Liver failure
low TBG, low SHBG, low CBG
67
New cards
Chronic illness
low SHBG, low CBG, low TBG
68
New cards
Pregnancy
high TBG, high SHBG, High CBG
69
New cards
Total hormone levels
low TBG, low CBG, low SHBG cause low total hormone
total T4 less informative than free T4
total T4 less informative than free T4
70
New cards
Tumor marker for medullary Thyroid Cancer
calcitonin
71
New cards
Salivary Cortisol:
used for accurate free cortisol levels in patients with abnormal serum-binding proteins. best in sensitivity and specificity for Cushing’s syndrome. Not normal nadir for people with Cushing’s
72
New cards
24-hr urinary Free cortisol tests
diagnosis of Cushing syndrome. Great for cortisol excess – poor for cortisol deficiency (adrenal insufficiency) – lacks sensitivity at low levels because low cortisol excretion can be found in normal levels of urine
73
New cards
Thyroid hormones
T3 and T4 bound by albumin, TBG and Transthyretin.
Free (unbound) TH are biologically active in combination with TH nuclear receptors and feedback loops. Responsible for oxidative metabolism at acceptable level for life – temperature, fever (metabolism high)
Free (unbound) TH are biologically active in combination with TH nuclear receptors and feedback loops. Responsible for oxidative metabolism at acceptable level for life – temperature, fever (metabolism high)
74
New cards
Cortisol
cortisol bound to albumin and CBG with free cortisol circulating. Plasma free cortisol is a biologically active cortisol regulated for ACTH
75
New cards
Diurnal rhythm of testosterone
highest levels early morning
lowest levels at midnight
lowest levels at midnight
76
New cards
Diurnal rhythm of Cortisol
peak early morning.
- 8 AM cortisol: 10-20 ug/mL.
- 4PM cortisol: 3-10 ug/mL.
- During sleep:
- 8 AM cortisol: 10-20 ug/mL.
- 4PM cortisol: 3-10 ug/mL.
- During sleep:
77
New cards
Diurnal rhythm of ACTH
peak early morning.
- 8AM ACTH: 10-50 pg/mL.
- 4PM ACTH:
- 8AM ACTH: 10-50 pg/mL.
- 4PM ACTH:
78
New cards
Biochemical markers of Pheochromocytoma & Paragangliomas
Metanephrines
79
New cards
Normal doubling time of hCG in first trimester v. ectopic pregnancy
First trimester: 2-3 days (doubling)
Ectopic pregnancy: does not meet doubling time criterion – flat line
Ectopic pregnancy: does not meet doubling time criterion – flat line
80
New cards
Pre-eclampsia
urinalysis screening
81
New cards
Neural tube closure defects
screening at 15-20 gestation. Alpha-fetoprotein measured first in maternal serum (MSAFP).
82
New cards
Fetal lung maturity
lecithin-sphingomyelin ratio (L/S ratio) (2:1) indicator. Phosphatidyl choline/glycerol (PC) another indicator (delayed in maternal DM). Thin layer chromatography detection
83
New cards
Differentiating urine from amniotic fluid
creatinine levels lower in amniotic fluid than urine. Fern test. pH (amniotic fluid 7.1-7.3, urine 4.5 – 6.0)
84
New cards
Cell free DNA screening (cf-DNA)
ratio of cell-free DNA from fetus and mom compared to determine trisomy
Also determines gender of the fetus and X/Y chromosomal abnormalities
Also determines gender of the fetus and X/Y chromosomal abnormalities
85
New cards
Trisomy 21:
Down syndrome
86
New cards
Trisomy 18
Edwards syndrome
87
New cards
Trisomy 13
Patau syndrome
88
New cards
TLC (Thin Layer chromatography)
stationary phase: thin layer (coated plate)
hydrophobic or hydrophilic stationary phase
mobile: solvent that mixes up the liquid phase
hydrophobic or hydrophilic stationary phase
mobile: solvent that mixes up the liquid phase
89
New cards
GC (Gas chromatography)
stationary phase: capillary columns, coils can be packed with material (inside the column)
mobile phase: volatile gas (hydrogen)
affinity for either stage
a compound that has equal affinity for both stages
mobile phase: volatile gas (hydrogen)
affinity for either stage
a compound that has equal affinity for both stages
90
New cards
which of the following pathways is responsible for maintaining the change in water balance (increase in volume)
renin angiotensin aldosterone axis
91
New cards
method for neonatal screening tests
tandem mass spectrometry (MS/MS)
92
New cards
Identify major indications for monitoring therapeutic drugs
Compliance: medication has adverse effects
toxicity levels may be close to therapeutic ranges (Digoxin, lithium)
toxicity levels may be close to therapeutic ranges (Digoxin, lithium)
93
New cards
When should peak and trough drug levels be collected
peak: above minimum
15-30 minutes after intravenous injections or infusions
30-60 minutes after intramuscular injections
1 hours after drug taken orally
trough: below maximum
-immediately before next dose is given
15-30 minutes after intravenous injections or infusions
30-60 minutes after intramuscular injections
1 hours after drug taken orally
trough: below maximum
-immediately before next dose is given
94
New cards
Preferred methods for detecting aspirin, ethanol, and alcohols other than ethanol
Can be measured by enzymatic technique exploiting NADH production by ADH
Or identified and quantified by Gas chromatography
Or identified and quantified by Gas chromatography
95
New cards
major metabolites of methanol
formic acid
96
New cards
major metabolites of ethylene glycol
glycolic acid
oxalic acid
oxalic acid
97
New cards
major metabolites of isopropanol
acetone
98
New cards
major metabolites of ethanol
acetaldehyde
acetate
acetate
99
New cards
lethal ethanol concentration
50-100 mL
300-500 mg/dL
300-500 mg/dL
100
New cards
lateral flow immunoassay
-sample pad is the first stage of the absorption process
-conjugate pad stores conjugated labels and antibodies will get sample
-binding reagents on nitrocellulose membranes will bind to the target
-colored lines will form
-sample will pass through membrane into absorbent pad
-absorbent will absorb excess samples
-conjugate pad stores conjugated labels and antibodies will get sample
-binding reagents on nitrocellulose membranes will bind to the target
-colored lines will form
-sample will pass through membrane into absorbent pad
-absorbent will absorb excess samples