Hypothalamus & Pituitary Gland - Chapter 17
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
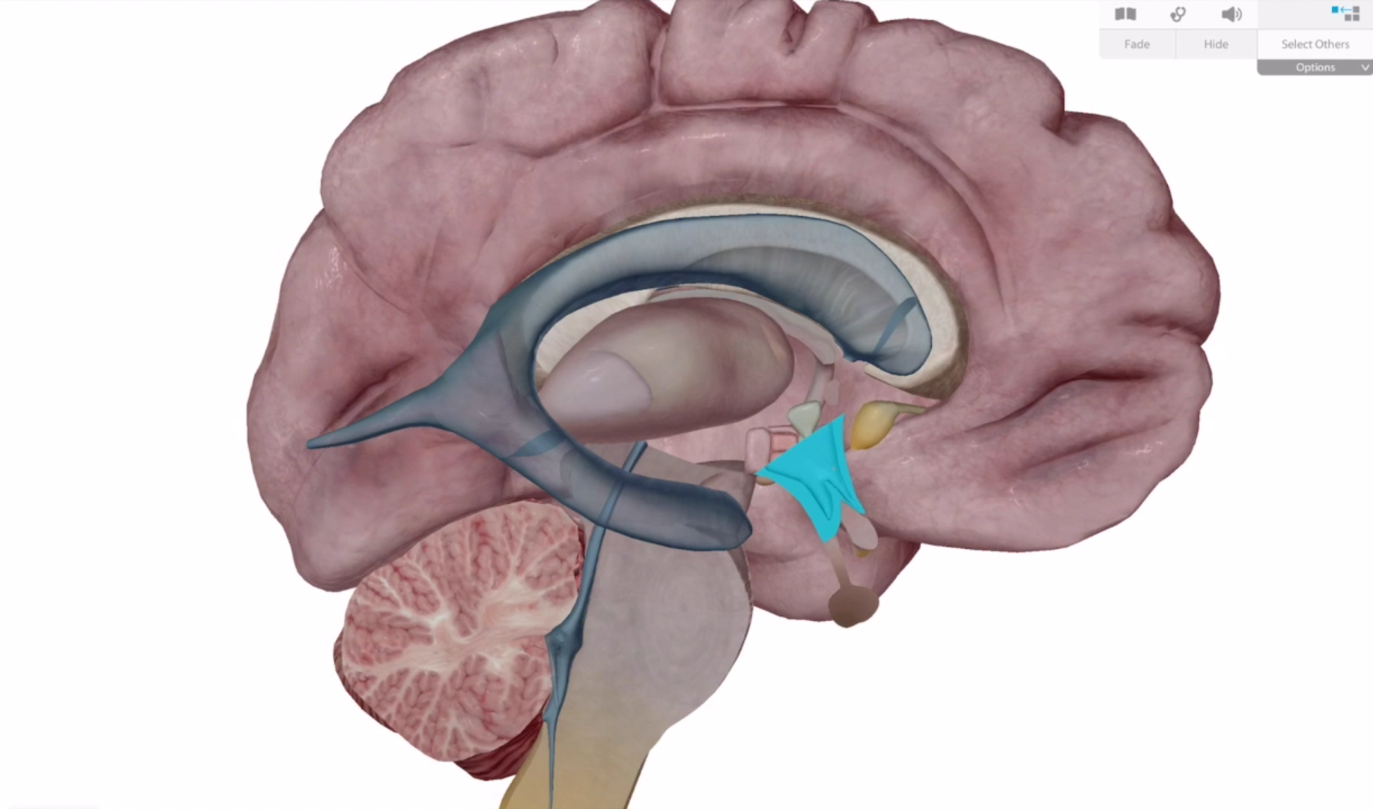
Hypothalamus
Its directly underneath the thalamus
Features of the Hypothalamus
One of the three regions of the dinocephalon
Maintains homeostasis
Connects information from the nervous system into the endocrine system
Participates in the limbic system for pleasure, fear, and rage.
Works closely with the pituitary gland
Hypothalamus Hormones
GHRH Growth Hormone Releasing Hormone. Tells pituitary to release GH
GHIH
TRH Thyroid releasing hormone
CRH Corticotropin Releasing Hormone
PIH Prolactin inhibiting hormone
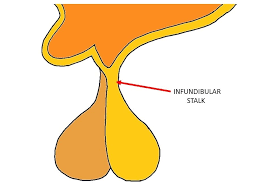
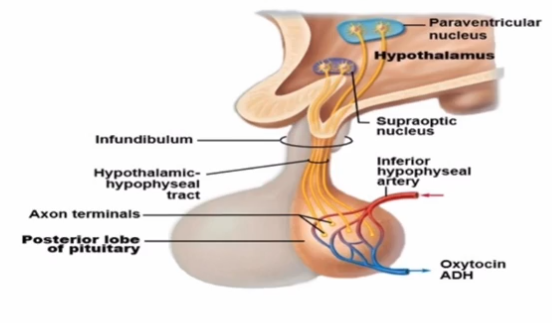
Infundibulum
Connects the hypothalamus to the pituitary gland
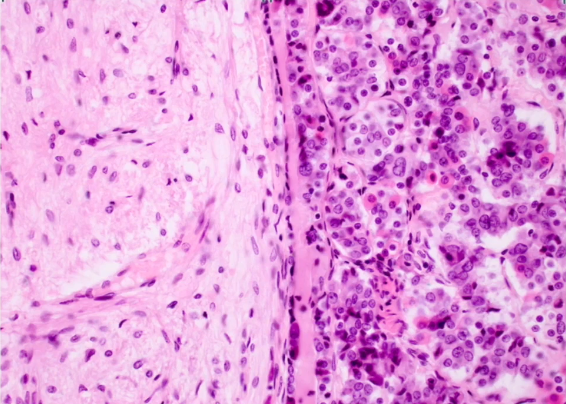
Pituitary Gland (Hypophysis) Lobes
Posterior Lobe is made of neural tissue.
Anterior Lobe is made of glandular tissue
Hormones secreted by the Posterior Lobe and their origin points:
Oxytocin is formed in the Paraventricular Nucleus
Antiduretic Hormone (ADH) is synthesized in the Supraoptic Nucleus.
Both are stored in the posterior pituitary gland
What does Oxytocin do and how does it work?
Stimulates uterine contraction and milk ejection in females via a positive feedback loop, and stimulates ejacul ation in males.
Operates via positive feedback loops.
Operates via the PIP2-Calcium Second Messenger
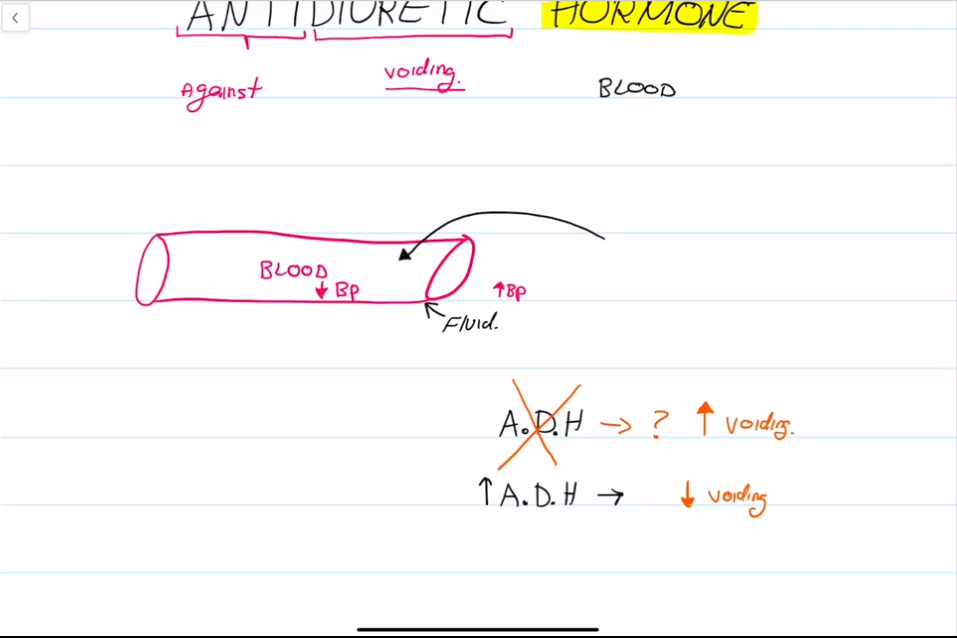
What does ADH do and how does it work?
ADH encourages urine retention in the body.
The hypothalamus contains osmoreceptors, if the concentration of solute in the blood becomes too high, then the hypothalamus instructs the pituitary gland to release ADH. Kidney tubules then reabsorb more water
Diuretics such as alcohol inhibit ADH.
Clinical Conditions Regarding ADH:
Diabetes Insipidus
Syndrome of Inappropriate ADH Secretion (SIADH)
Diabetes Insipidus
Caused by a lack of ADH in the body.
Characterized by frequent, clear urination, with sugar in the urine.
Dangerous as the patient may be losing too much water.
SIDAH
Characterized by too much ADH in the body.
Patient retains too much fluid, does not urinate frequently.
Retention can cause headaches, diuresis, and edema.
Must monitor sodium levels, additional sodium may worsen symptoms.

What pathway do hormones take to reach the Anterior Lobe from the Hypothalamus:
Hypophyseal Portal System. A series of capillary’s that carry inhibiting and releasing hormones.
Primary capilary plexus → hypophyseal portal veins → Secondary capillary plexus
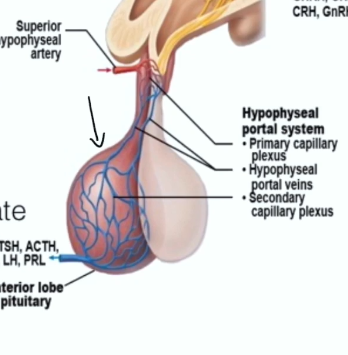
Anterior Pituitary Gland Hormones:
Growth Hormone GH
Thyroid-Stimulating Hormone
Adrenocorticotropic Hormone
Follicle-Stimulating Hormone
Lutenizing Hormone
Prolactin
All except for Growth Hormone activate cyclic AMP second messenger systems at their targets.
TSH, ACTH, FSH, and LH are all tropic hormones (They make other glands release hormones)
Next slides, what hormones control the hypothalamus?
GH
Growth Hormone Releasing Hormone GHRH
Growth Hormone Inhibiting Hormone GHIH
TSH
Thyroid Releasing Hormone (TRH)
ACTH
Corticotropin-Releasing Hormone (CRH)
FSH/LH
Gonadotropin Releasing Hormone (GnRH)
Prolactin (PRL)
Prolactin Releasing Factor
Prolactin Inhibiting Hormone
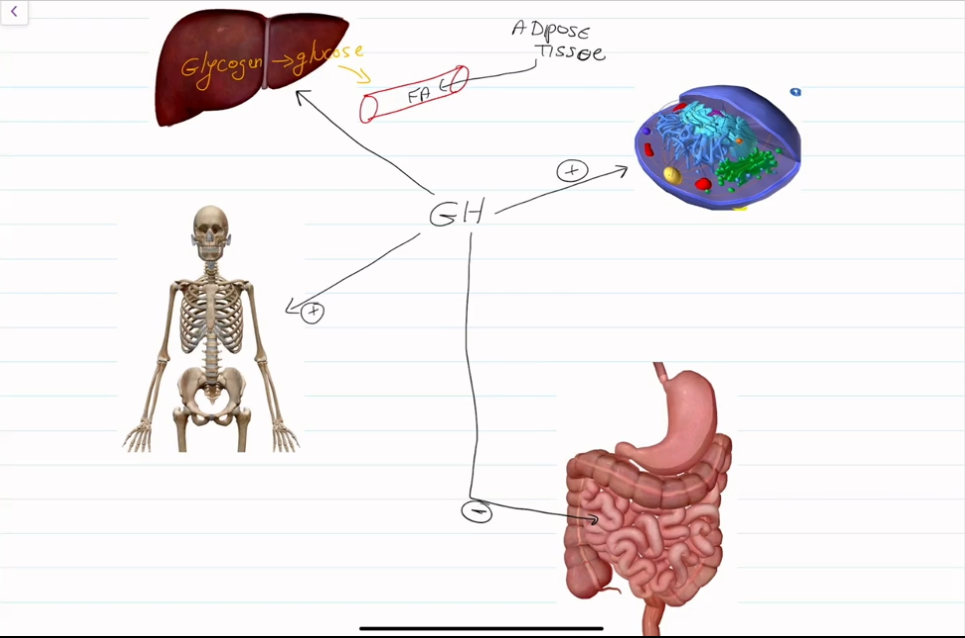
What does Growth Hormone do?
Encourage the growth of bones at growth plates.
Increases blood levels of fatty acids; encourages use of fatty acids for fuel; encourages protein synthesis
Decreases the rate of glucose uptake and metabolism, conserving glucose
Breaks down glycogen to release glucose into the bloodstream
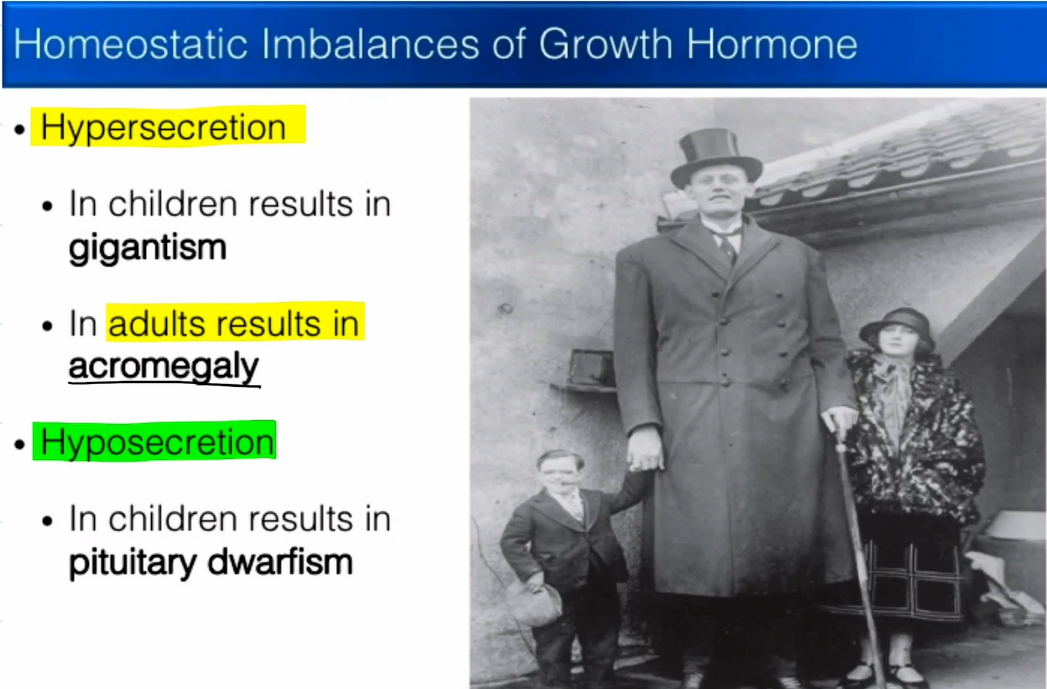
Clinical Conditions Regarding Growth Hormone
Hypersecretion:
Gigantism
Acromegaly
Hyposecretion
Pituitary Dwarfism
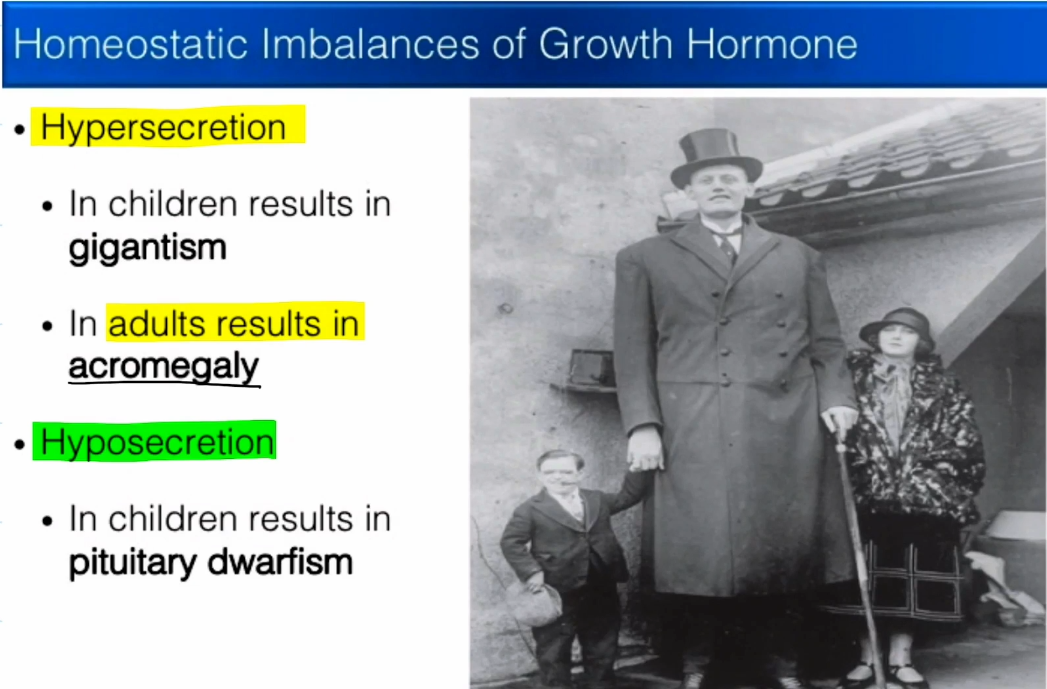
Gigantism
Occurs when too much GH is released during childhood.
Results in the formation of very long, weak bones.
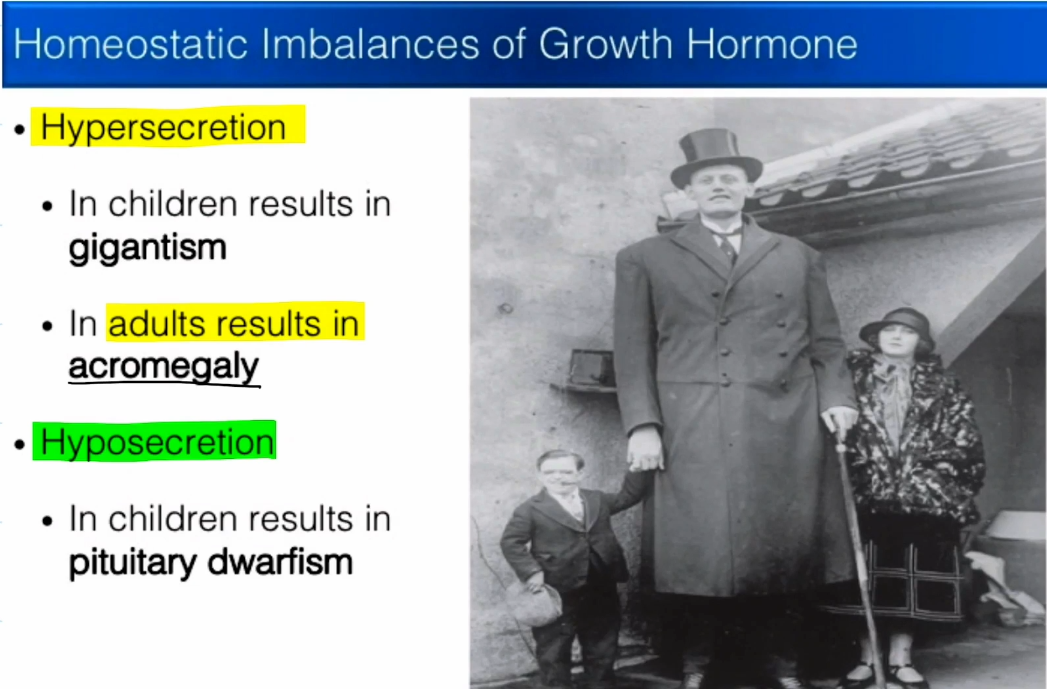
Acromegaly
Occurs when too much GH is released after growth plates have closed.
Results in the formation of large facial features and organs, weakening the heart.
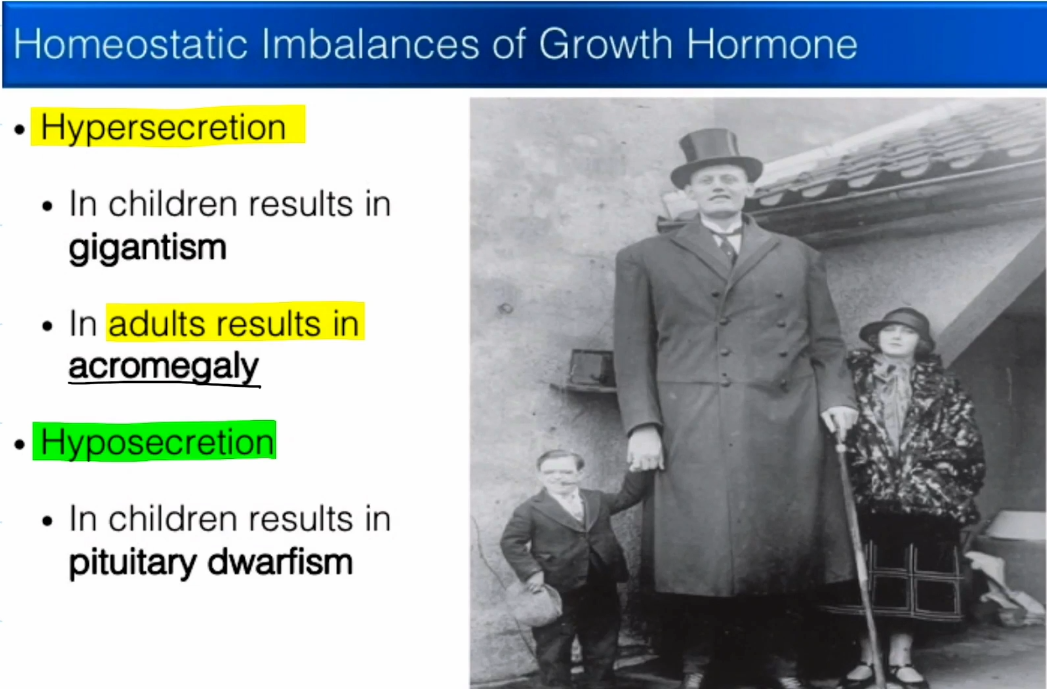
Pituitary Dwarfism
Occurs when too little GH is released during childhood.
Very little growth occurs at the growth plate, resulting in a dwarf.
Thyroid Stimulating Hormone Pathway:
Hypothalamus is going to release Thyroid Releasing Hormone
Anterior Pituitary Gland is going to release Thyroid Stimulating Hormone.
Thyroid is going to release hormones towards the target tissue.
The release of thyroid hormones is regulated by a negative feedback loop, if there is too much thyroid hormone, then production of TRH and TSH will be shut down.

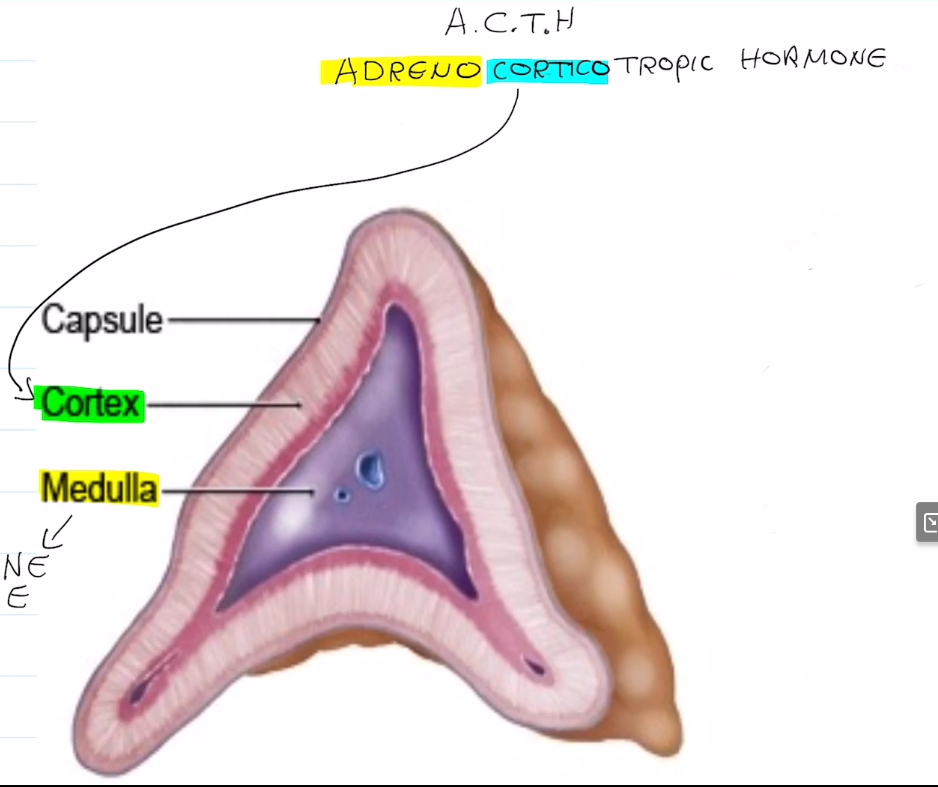
Adrenocorticotropic Hormone (Corticotropin) Pathway:
Corticotropin-Releasing Hormone (CRH) is released by the hypothalamus
Adrenocorticotropic Hormone is released by the anterior pituitary gland
ACTH interacts with the cortex of the Adrenal Glands (atop the kidneys) and stimulates the release of cortisol
Cortisol can also be released by fever, hypoglycemia, and stress.
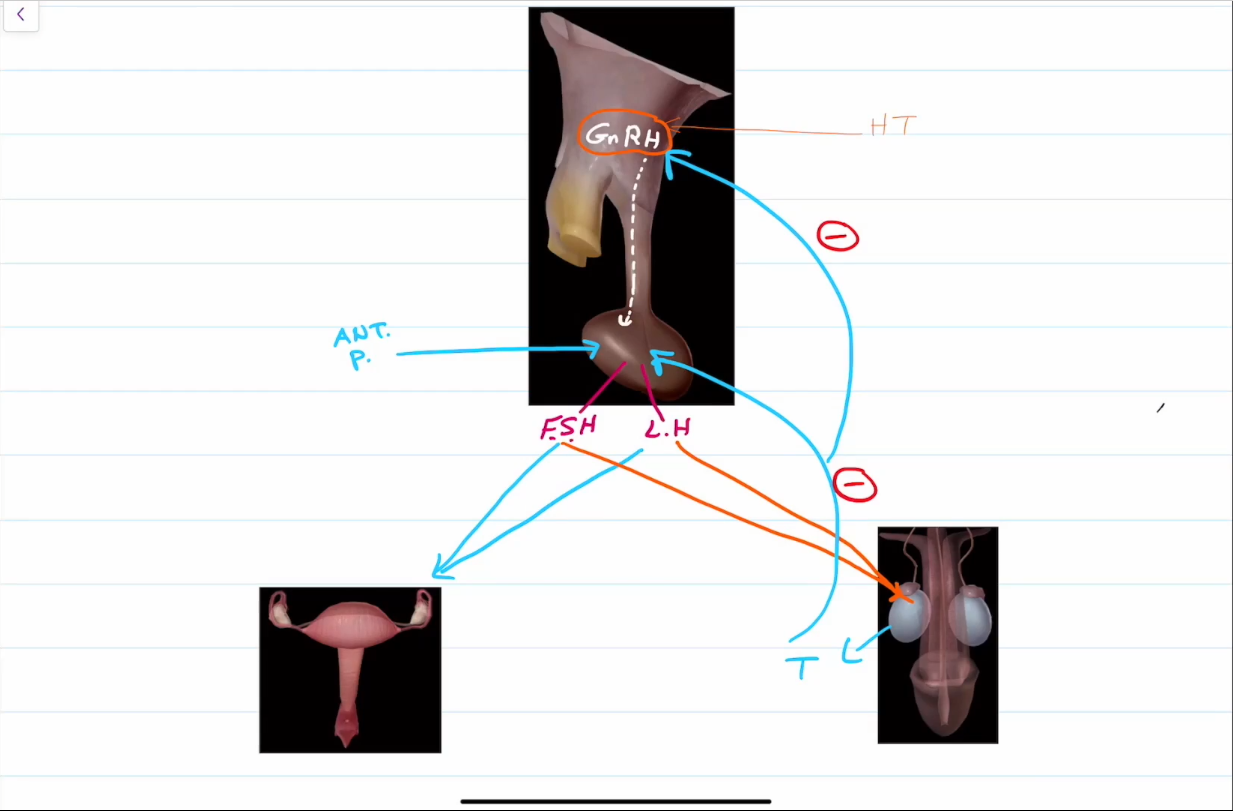
Follicle Stimulating Hormone and Lutenzing Hormone Pathway:
Both are very low/absent in prepubecent males and females.
Gonadotropin-releasing hormone from the hypothalamus encourages the release of FSH and LH from the anterior pituitary gland.
FSH stimulates gamete production in both males and females.
LH encourages the production of testosterone from the testes, and ovulation from the ovaries.
Regulated by a negative feedback loop, in which gonadotropins will eventually travel through the blood, back to the hypothalamus, and will cease production.
Prolactin Pathway
Prolactin is usually inhibited by Prolactin Inhibiting Hormone.
PIH levels decrease during pregnancy and when suckling occurs, encoraging lactation.
The role of prolactin is not well understood in males, however, high levels can cause lactation and impotence.