Antibiotic Steroid Combos
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
What are the primary indications for stand‑alone topical ophthalmic antibiotics to treat active ocular surface infections?
Active bacterial infections of the ocular surface, including:
Bacterial conjunctivitis
Hyperacute conjunctivitis
Microbial keratitis (MK)
aka bacterial corneal ulcer
What clinical findings suggest bacterial conjunctivitis that warrant topical antibiotic treatment?
Mucopurulent discharge
“Eyelids stuck shut” (especially on waking)
How does hyperacute conjunctivitis present, and why is it treated urgently with topical antibiotics?
Rapid onset
Copious purulent exudate
Conjunctival chemosis
Suggests highly virulent bacteria → requires prompt antibiotic therapy

When are topical ophthalmic antibiotics used for prophylaxis or bacterial overgrowth prevention?
Prophylaxis:
Epithelial defects
Pre‑ or post‑surgical settings
Bacterial overgrowth:
Anterior blepharitis (“Staph bleph”)
What is the FDA‑approved indication for topical antibiotic-steroid combination eye drops/ointments?
“Ocular inflammation with a risk of superficial bacterial infection”
Used when inflammation is present and bacterial infection or overgrowth is a concern
What is the role of each component in a topical antibiotic–steroid combination?
Steroid:
Anti‑inflammatory (↓ redness, pain, swelling)
Antibiotic:
Prophylaxis against bacterial infection
↓ bacterial overgrowth, which often drives the inflammation
Why are antibiotic-steroid combinations preferred over steroids alone in certain ocular inflammatory conditions?
Steroids suppress local immunity
Antibiotic component:
Prevents secondary bacterial infection
Controls existing bacterial overgrowth contributing to inflammation
Makes steroid use safer in at‑risk eyes
Which inflammatory corneal conditions commonly require a topical antibiotic-steroid combination?
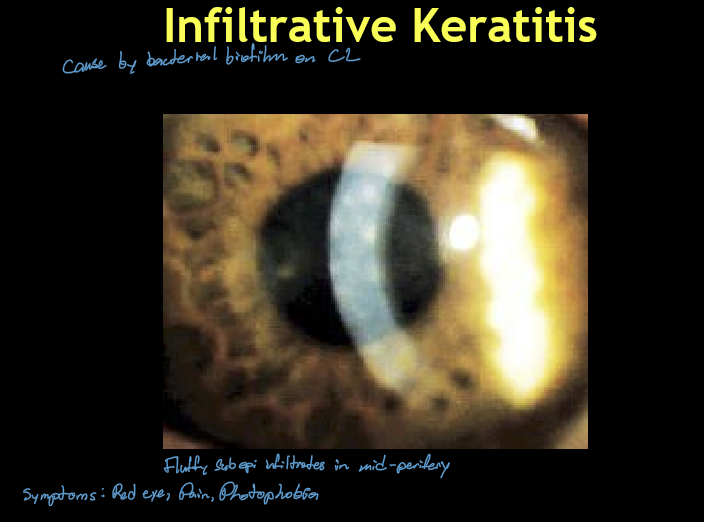
Infiltrative Keratitis (IK)
Contact Lens Acute Red Eye (CLARE)
Contact Lens–Associated Infiltrative Keratitis (CLAIK)
All are sterile inflammatory events with infection risk
What is the etiology and pathophysiology of Infiltrative Keratitis (IK)?
Sterile inflammatory reaction of the cornea
Triggered by bacterial biofilm/colonization on soft contact lenses
Not a true infection, but inflammation secondary to bacterial antigens
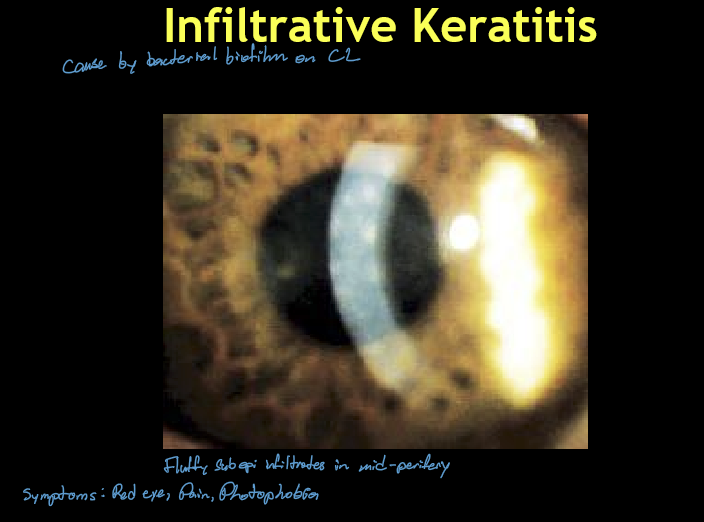
What are the typical clinical findings of Infiltrative Keratitis (IK)?
Usually unilateral
Single or few small, round, hazy subepithelial infiltrates
Location: central or mid‑peripheral cornea
Often positive fluorescein staining
Mild-moderate irritation, redness, ± discharge
How does Asymptomatic Infiltrative Keratitis (AIK) differ from symptomatic IK?
Smaller infiltrates
Typically mid‑peripheral
No or minimal staining
Patient largely asymptomatic
Associated with mild limbal injection
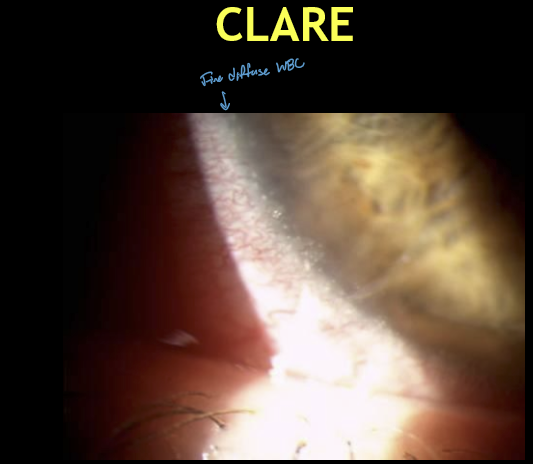
What is Contact Lens Acute Red Eye (CLARE) and when does it occur?
Acute inflammatory reaction of the cornea and conjunctiva
Occurs after overnight (extended‑wear) soft contact lens use
Symptoms classically present upon awakening
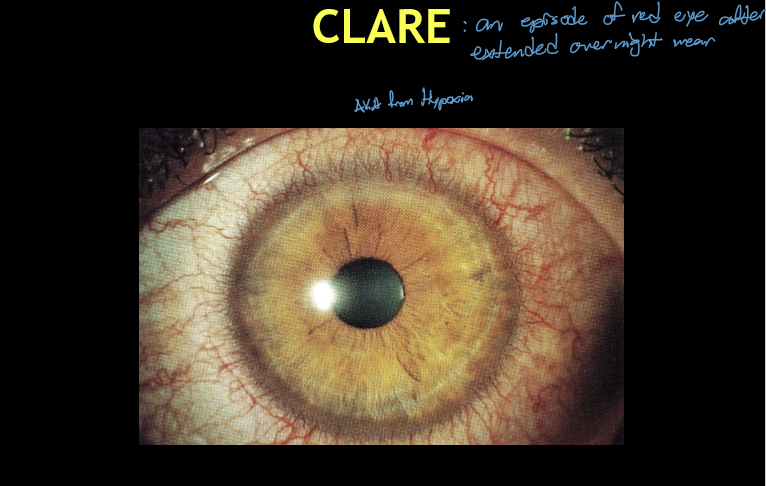
What are the major etiologic factors contributing to CLARE?
Inflammatory response to one or more of the following:
Hypoxic stress from overnight lens wear
Tight lens syndrome
Possible gram‑negative bacterial colonization on soft CL
What are the typical corneal findings in CLARE?
Usually unilateral
Multiple small infiltrates or diffuse WBCs
Location: just inside the limbus
Usually no fluorescein staining (intact epithelium)
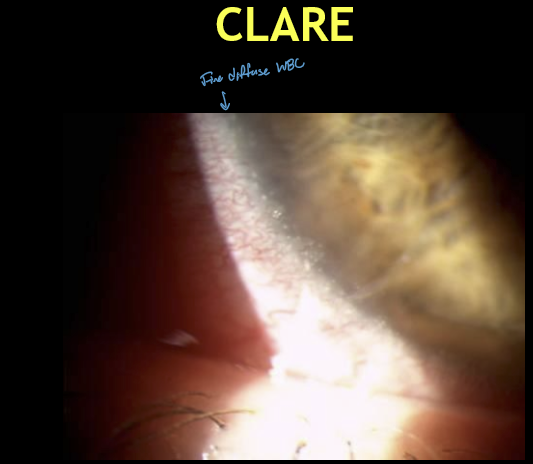
What are the classic symptoms and signs of CLARE?
Moderate-severe pain
Tearing and photophobia
Marked redness with circumlimbal injection
Acute onset on awakening
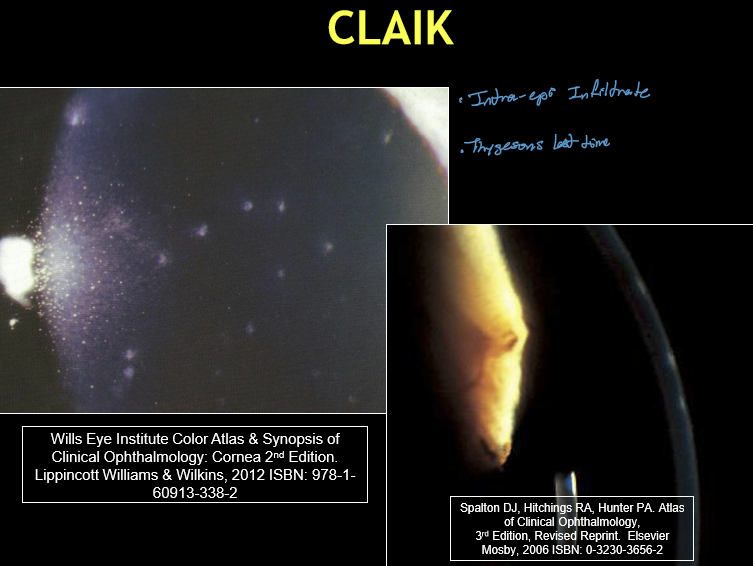
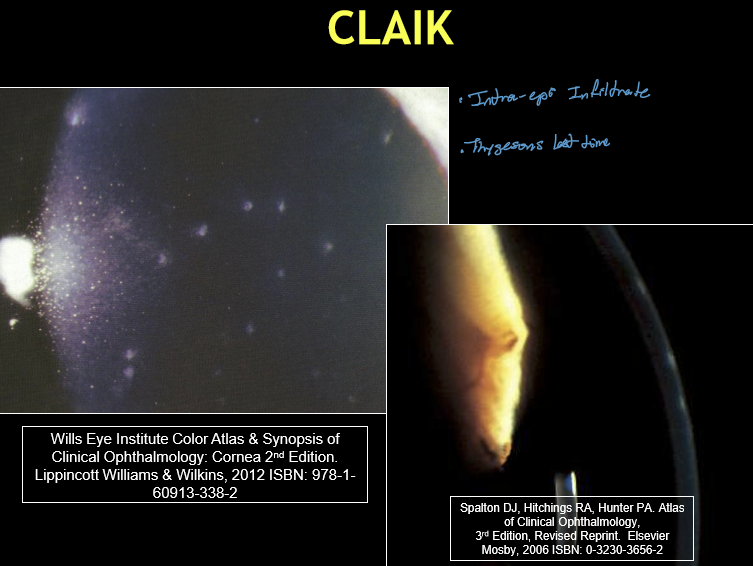
What is the etiology of Contact Lens-Associated Infiltrative Keratitis (CLAIK)?
Sterile inflammatory reaction of the cornea and conjunctiva
Triggered by certain multipurpose solutions (MPS)
MPS is harbored within silicone hydrogel (SiHy) daily‑wear lenses
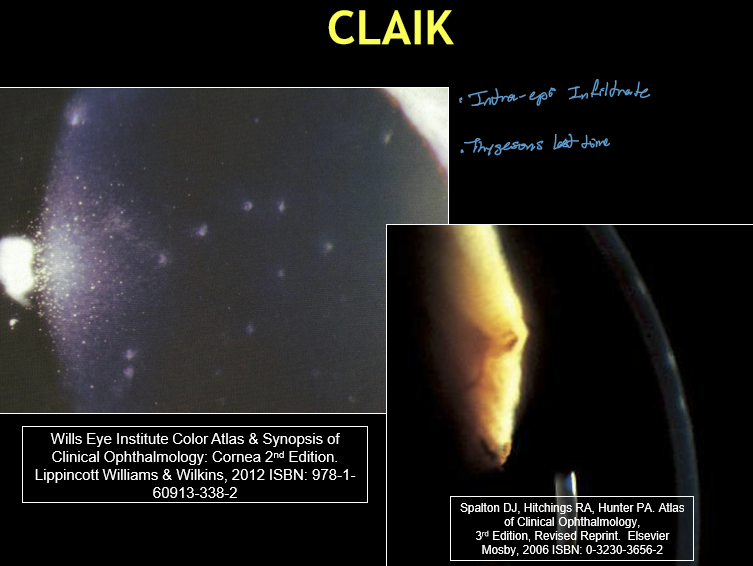
What are the typical corneal findings in CLAIK?
Usually bilateral
Multiple, small, coarse, granular intraepithelial infiltrates
Positive fluorescein staining
Location: central or paracentral cornea
What symptoms are associated with CLAIK, and how severe are they?
Asymptomatic to mild symptoms, including:
Mild irritation
Tearing
Photophobia
Conjunctival injection commonly present
Less painful than CLARE or microbial keratitis
What exam pearls help differentiate CLAIK from other CL‑related inflammatory events?
CLAIK: bilateral, central/paracentral, MPS‑related, mild symptoms
IK: usually unilateral, subepithelial infiltrates, biofilm‑related
CLARE: acute, painful, post‑overnight wear, peripheral infiltrates
Which ocular conditions are classic examples of staph‑mediated hypersensitivity requiring antibiotic-steroid combinations?
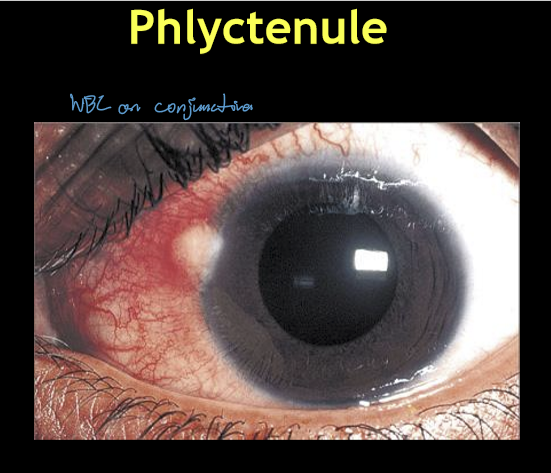
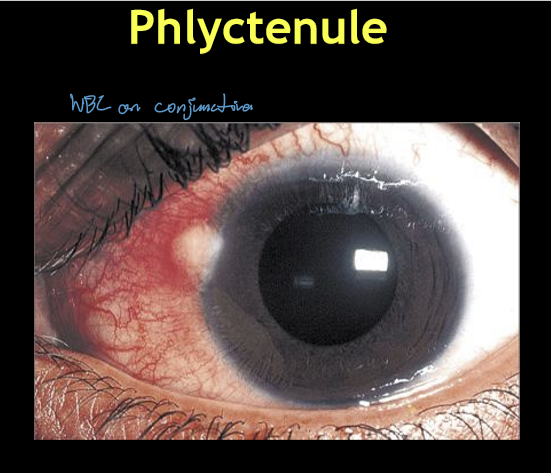
Phlyctenular keratoconjunctivitis (phlyctenulosis)
Marginal keratitis
aka staph ulcer
aka sterile peripheral ulcer
Contact lens peripheral ulcer/infiltrate (CLPU/CLPI)
Anterior blepharitis with staph hypersensitivity
Why are steroids alone insufficient in staph hypersensitivity ocular conditions?
Steroids suppress inflammation but do not remove antigen source
Persistent staph overgrowth → recurrent inflammation
Antibiotics ↓ bacterial load → ↓ immune stimulation
What is the etiology and immunologic mechanism of a phlyctenule?
Type III hypersensitivity reaction
Triggered by excess exotoxins from Staphylococcal overgrowth in normal flora
Lesion is sterile (immune‑mediated, not infectious)
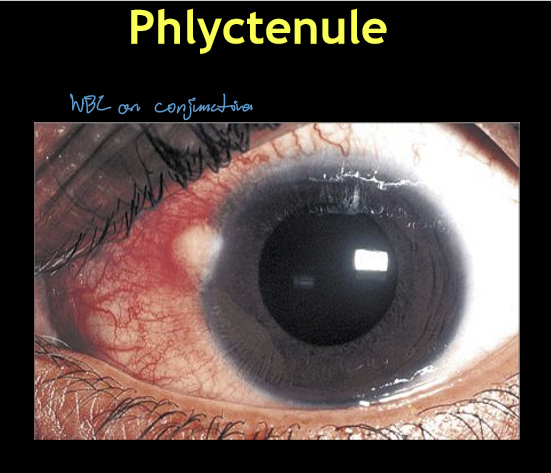
How does a phlyctenule typically present clinically?
Unilateral red eye
Focal accumulation of conjunctival WBCs
Located at or near the limbus
Coincides with lid crossing points:
10:00, 2:00, 4:00, 8:00
What eyelid condition is commonly associated with phlyctenular keratoconjunctivitis?
Anterior blepharitis
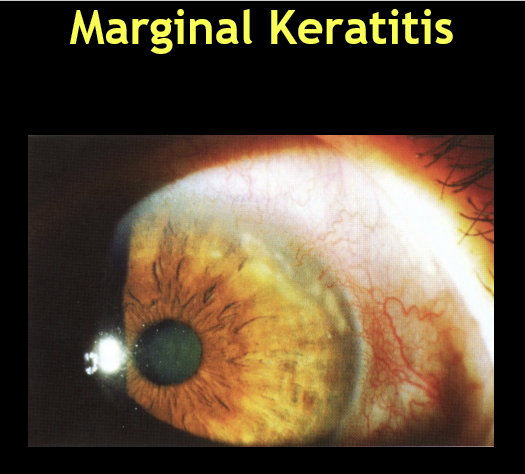
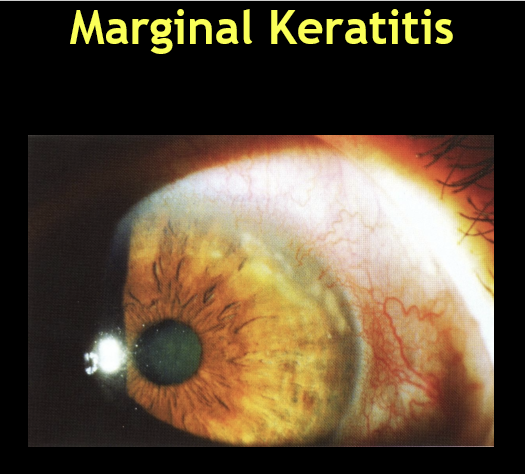
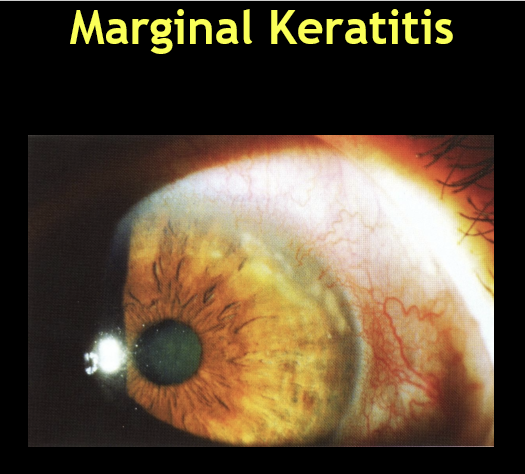
What is the etiology and immunologic mechanism of marginal keratitis?
Type III hypersensitivity reaction
Triggered by excess exotoxins from Staphylococcal overgrowth in normal lid flora
Lesion is sterile (immune‑mediated, not infectious)
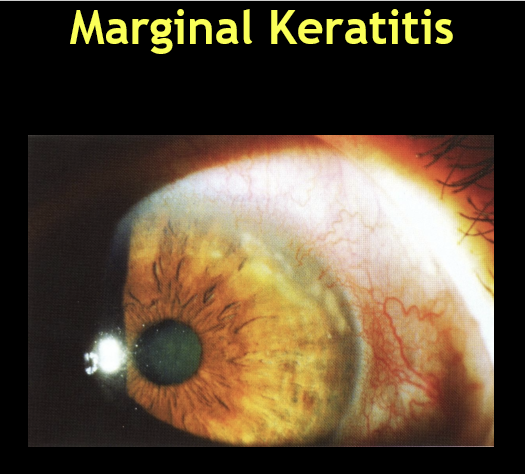
What are the typical corneal findings in marginal keratitis?
Unilateral red eye
Single or multiple peripheral (marginal) corneal infiltrates
Positive fluorescein staining
Lesions correspond to lid crossing points:
10:00, 2:00, 4:00, 8:00
What symptoms are associated with marginal keratitis, and how severe are they?
Variable severity
May range from asymptomatic to:
Tearing
Pain
Photophobia
What eyelid condition is commonly associated with marginal keratitis, and why is this important?
Anterior blepharitis (Staph bleph)
Acts as the source of staph exotoxins
Underlies recurrence if lid disease is untreated
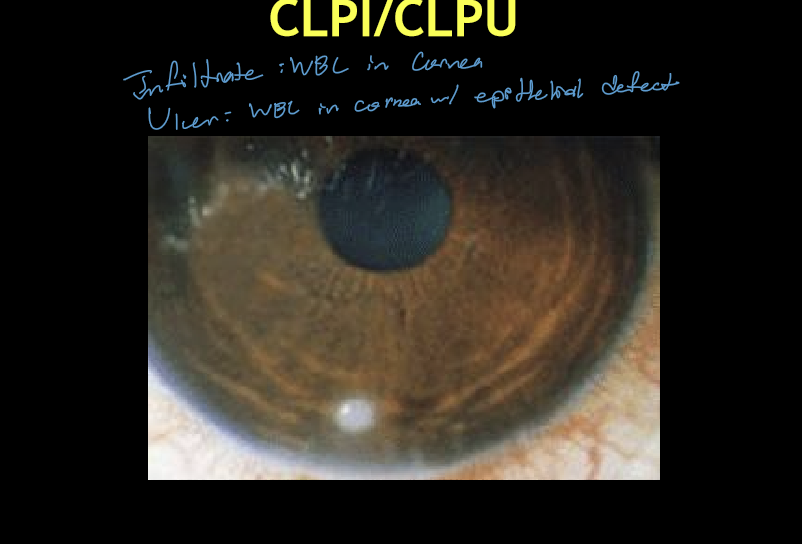
What is the etiology and pathophysiology of CLPI/CLPU?
Type III hypersensitivity reaction
Triggered by excessive Staphylococcal colonization on soft contact lenses
Essentially marginal keratitis in a contact lens wearer
Sterile inflammatory process, not a primary infection
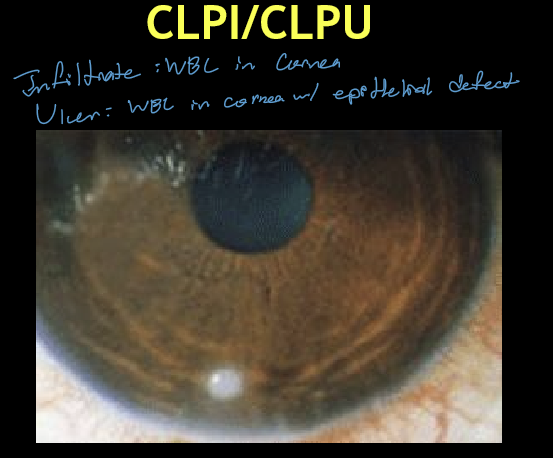
What are the typical corneal findings in CLPI/CLPU?
Usually unilateral
Single, circular, well‑defined focal infiltrate
Size: ≤ 2 mm
Location: peripheral cornea just inside the limbus
CLPI: no fluorescein staining
CLPU: positive staining (epithelial defect)
What symptoms are associated with CLPI/CLPU, and how severe are they?
Wide spectrum: asymptomatic → severe pain & photophobia
Common symptoms:
Foreign body sensation
Tearing
Signs:
Bulbar and limbal injection
What are the components and formulation options of Tobradex?
0.3% Tobramycin + 0.1% Dexamethasone
Available as:
Suspension (generic available)
Ointment (trade name only)
What is the typical dosing regimen for Tobradex?
q2h for 2 days, then
QID for 5 days
Why is dexamethasone used instead of other steroids?
Dexamethasone is the only one that does not degrade when mixed with antibiotics.
How does Tobradex ST differ from standard Tobradex?
0.3% Tobramycin + 0.05% Dexamethasone
No generic available
Lower steroid concentration with enhanced delivery technology using Xanthan gum
What does the “ST” in Tobradex ST stand for, and why is it important?
ST = Suspension Technology
Uses a xanthan gum vehicle
↑ contact time on ocular surface
Allows bioequivalent steroid effect despite lower dexamethasone concentration
What is the typical dosing regimen for Tobradex ST?
q2h for 2 days, then
QID for 5 days
Same dosing as Tobradex, despite lower steroid %
What are the components and formulation of Zylet?
0.3% Tobramycin + 0.5% Loteprednol
Suspension only
Generic available
How does loteprednol in Zylet differ from dexamethasone in other combo agents?
Loteprednol has better penetration to target tissue and has lower risk of IOP elevation.
What is the typical dosing regimen for Zylet?
q2h for 2 days, then
QID for 5 days
Which antibiotic-steroid combinations are considered less desirable, and why?
Older formulations with:
Weaker antibiotics
Higher allergy risk (e.g., neomycin)
Inferior steroid choices (e.g., hydrocortisone)
Still used, but not first‑line compared to Tobradex or Zylet
What did the SCUT (Steroids for Cornela Ulcers Trail) study find?
Tested outcomes of adding 1% prednisolone acetate as adjunctive therapy 48 hours after treatment with moxifloxacin to culture positive bacterial corneal ulcers.
Results:
No overall difference in time to re-epithelialization, corneal perforation, or 3mos BCVA
No safety concerns with addition of steriods
No overall difference in scar size, except for:
Subgroup of pts who had finger counting entering VA had 0.17 logMAR better endoint acuity
Subgroup of pts with completely central ulcers had 0.20 logMAR better endpoint acuity.
What was the main take‑home message of the Steroids for Corneal Ulcers Trial (SCUT) regarding steroid use in microbial keratitis?
Steroids may be considered ONLY in select cases of bacterial keratitis, not routinely. They should be added cautiously and only after initial antibiotic response is demonstrated.
Under what specific conditions should a topical steroid be added to treatment for microbial (bacterial) keratitis per SCUT and AAO guidance?
Consider steroids only if ALL are met:
Risk of visually significant scarring (within the pupillary zone)
Treated on antibiotics alone for 24-48 hours first (48 h per 2023 AAO PPP)
Clear slit‑lamp improvement (↓ staining size, evidence of re‑epithelialization)
Preferably culture‑positive for bacteria to rule out fungal or protozoal keratitis