neoplasia 1 - definition and classification
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
what does neoplasia mean?
New growth
A tissue state characterised by a permanently altered growth pattern
Abnormal mass of tissue, the growth of which is uncoordinated with that of normal tissues and persists after the stimulus is removed
the term ‘neoplasm’ doesn’t give any insight on how exactly the tumour behaves
what is the definition of a tumour?
Swelling, generally without inflammation, caused by an abnormal growth of
tissue whether benign or malignant
how can you classify tumour behaviour?
benign/ malignant
how can you classify tumours pathologically? 4
consider the cell type of origin…
Epithelium
Connective tissue
Lymphoid / haematopoietic tissue
Germ cells
tumour differentiation / grade
The extent to which a tumour resembles its normal counterpart, both
morphologically and functionally
There are tumours for which no normal cell of origin can be determined: unable to comment therefore on differentiation
this relates more to malignant tumours - as benign tumours resemble their tissue of origin well
In general terms well differentiated lesions are
less proliferative and less aggressive with less potential for metastatic spread than their poorly differentiated counterparts
There are exceptions
grade 1 tumours
well differentiated
grade 2 tumours
moderately differentiated
grade 3 tumours
poorly differentiated
Hyperplasia
Increase in the number of cells in a tissue
Hypertrophy
Increased in the size of cells in a tissue
Atrophy
Reduction in the size of cells in a tissue
Involution
Decrease in the number of cells in a tissue
Metaplasia
A change from one to another normal differentiated cell type within a tissue - cellular instability - may increase risk of cancer developing
Dysplasia
A state in some tissues which denotes an increased risk of
malignant change (*)
*fibrous dysplasia: abnormal development
morphological abnormalities of cells seen in the microscope which are not yet cancerous
Neoplasia
A tissue state characterised by a permanently altered growth pattern
hyperplasia example
Bone marrow cells in people living at high altitudes
Hypertrophy example
Bodybuilders / athletes
Atrophy example
Muscle atrophy in a dis-used limb
Involution example
Breast tissue on cessation of breastfeeding
Metaplasia example
Barrett’s oesophagus
Dysplasia example
Cervical screening
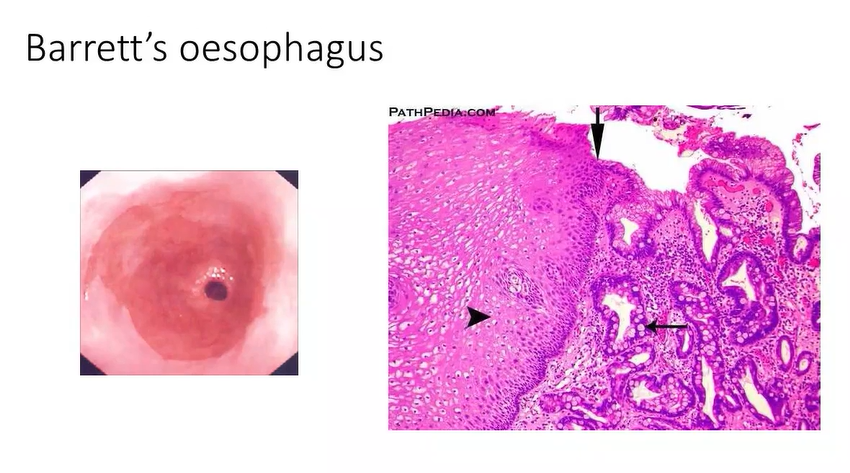
what is barretts oesophagus?
example of metaplasia
oesophagus is usually lined with squamous cell epithelium
stomach is lined by glandular epithelium- produces acids and enzymes - but is resistant to these products
squamous epithelium is easily damaged - so its therefore important to keep the stomach contents within the stomach via the lower oesophageal sphincter - but in reflux there is escape into lower oesophagus - damages the epithelium - the body can change the type of epithelium here to combat this - makes itself glandular - notice how the mucosa looks more red instead of paler
right image shows the interface between the pale and the red mucosa
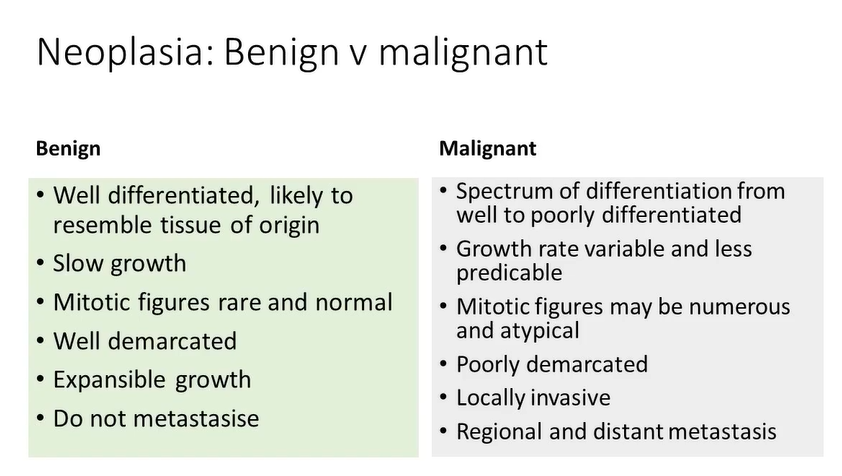
benign vs malignant - differentiation
benign- well differentiated, likely to resemble original tissue of origin
malignant - spectrum of differentiation from well to poorly differentiated
benign vs malignant - growth rate
benign - slow growth
malignant - growth rate variable and unpredictable
benign vs malignant - mitotic figures
benign - mitotic figures rare and normal
malignant - mitotic figures may be numerous and atypical
demarcation - benign vs malignant
benign - well demarcated
malignant - poorly demarcated
benign vs malignant - expansible growth vs locally invasive
benign - expansible growth
malignant - locally invasive
benign vs malignant - metastasis - spread to other parts of the body
benign - does not metastasise
malignant - regional and distant metastasis
compare benign and malignant tumours 6
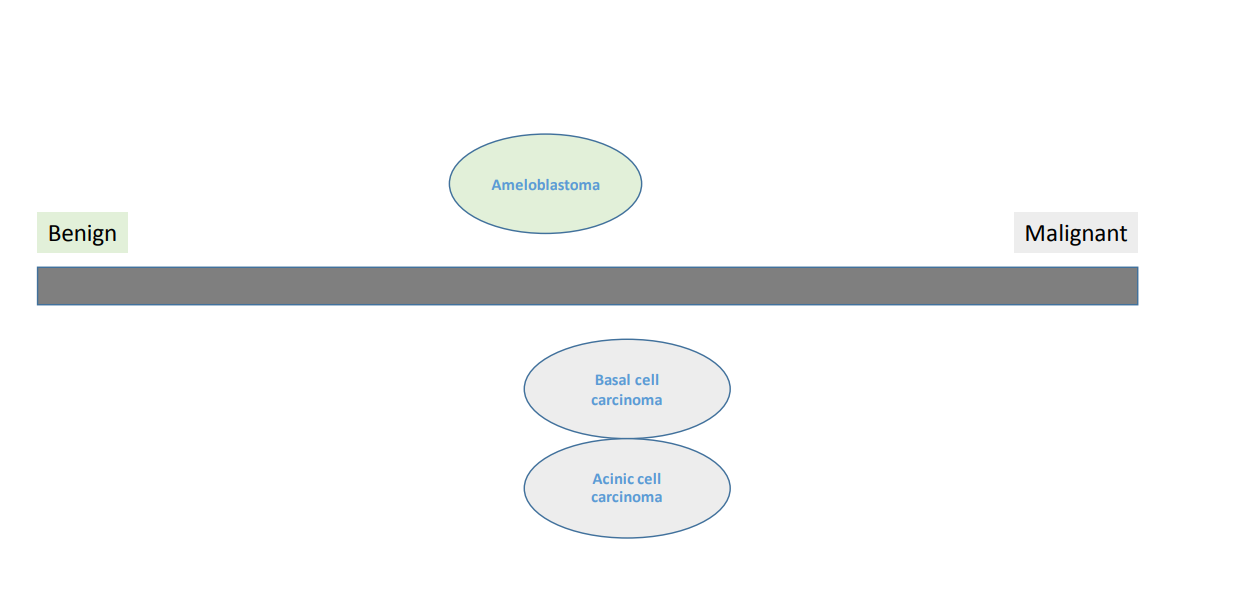
some benign tumours may be locally aggressive but can still be classified as benign - why?
because they don’t metastasise- but they may require more surgery than atypical benign tumour
consider benign and malignant to be a spectrum
two purple examples are malignant but at the benign end as they can metastasise but they rarely do
tumours can be three types - birds, rabbits and tortoises
cancer patients will survive if their tumours are contained - aim of cancer therapy is to fence them in
birds cant be fenced in - they will fly away - disseminated tumours - widespread at the time of diagnosis
rabbits can jump - can escape - can be contained - treat them aggressively
tortoises - all benign tumours, and indolent malignant tumours

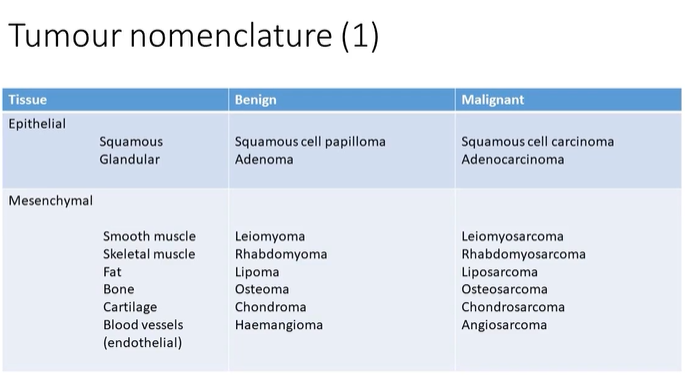
which is more common - epithelial tumours or mesenchymal tumours?
epithelial - with squamous tumours being more common than glandular tumours → arise from the mucosa
granular - salivary glands
wb the stomach?
epithelial squamous tumour B and M
B - squamous cell papilloma
M - squamous cell carcinoma
epithelial glandular tumour B and M
B - adenoma
M - adenocarcinoma
mesenchymal smooth muscle tumour
B - leiomyoma
M - leiomyosarcoma
mesencymal skeletal muscle tumour
B - rhabdomyoma
M - rhabdomyosarcoma
mesenchymal fat tumour
lipoma
liposarcoma
mesenchymal bone tumour
B - osteoma
M- osteosarcoma
mesenchymal cartilage tumour
B - chondroma
M - chondrosarcoma
mesenchymal endothelial tumour
haemangioma B vs angiosarcoma M
lymphoma
ALWAYS malignant - tumours of the lymphoid system
melanoma
always a malignant tumour of melanocytes
leukaemia
tumour of bone marrow cells - always malignant
teratoma
a tumour which includes elements of all 3 embryonic germ layers - rare
hamartoma
a developmental anomaly - not a tumour
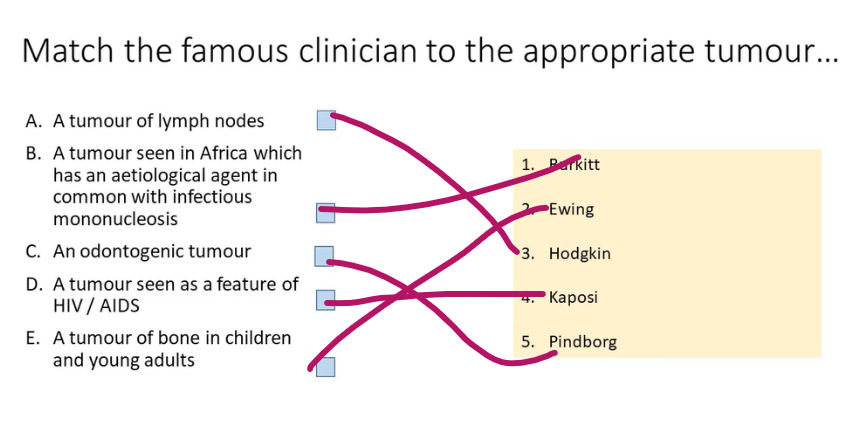
some tumours are named after the person who first described them
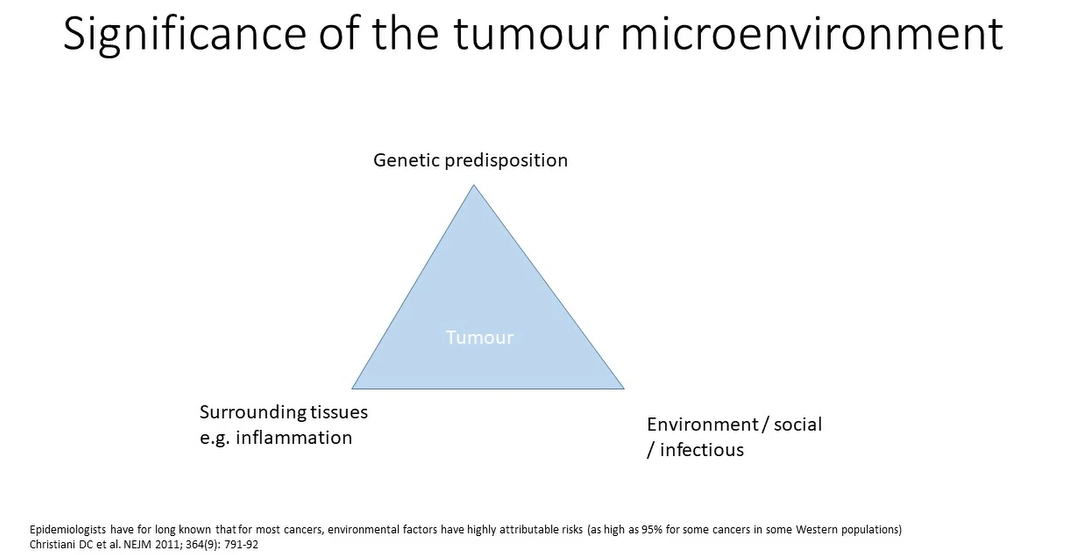
what causes tumours?
chemical carcinogens - lung and mouth cancers - smoking
breast and ovarian cancers - genetic predisposition
can cancers be caused by viruses?
yes!
Cervical, oropharyngeal and anal squamous cell carcinoma: high risk HPV
“Oropharyngeal HPV associated squamous cell carcinoma”
Nasopharyngeal carcinoma and Burkitts lymphoma: EBV
Kaposi sarcoma: HHV-8 (human herpes virus 8)
can use in situ hybridisation techniques to detect viral DNA in tumour cells
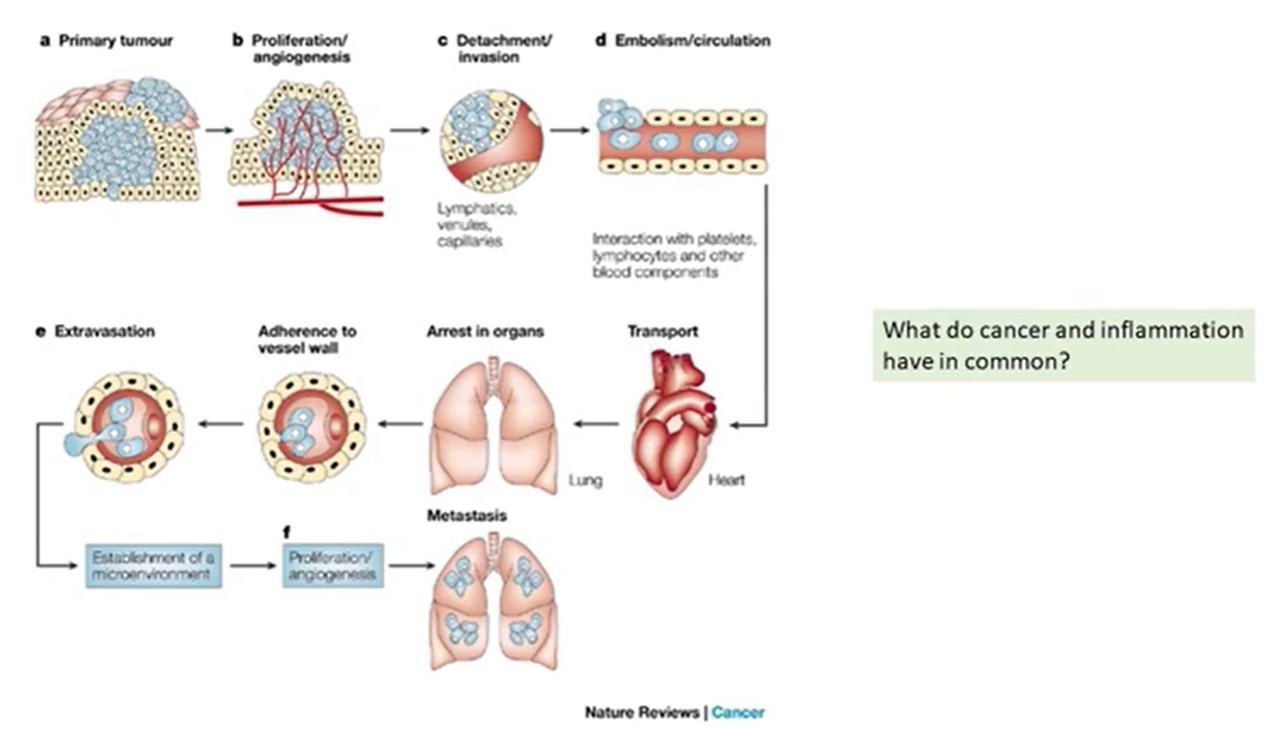
Cancers associated with infection / inflammation?
Hepatitis and liver cancer (hepatocellular carcinoma)
H pylori and gastric cancer (adenocarcinoma)
Pancreatitis and pancreatic cancer (adenocarcinoma)
cytokines may encourage proliferation in neighbouring cells
benign tumours tend to be
encapsulated, and grow slowly and expand rather than infiltrate
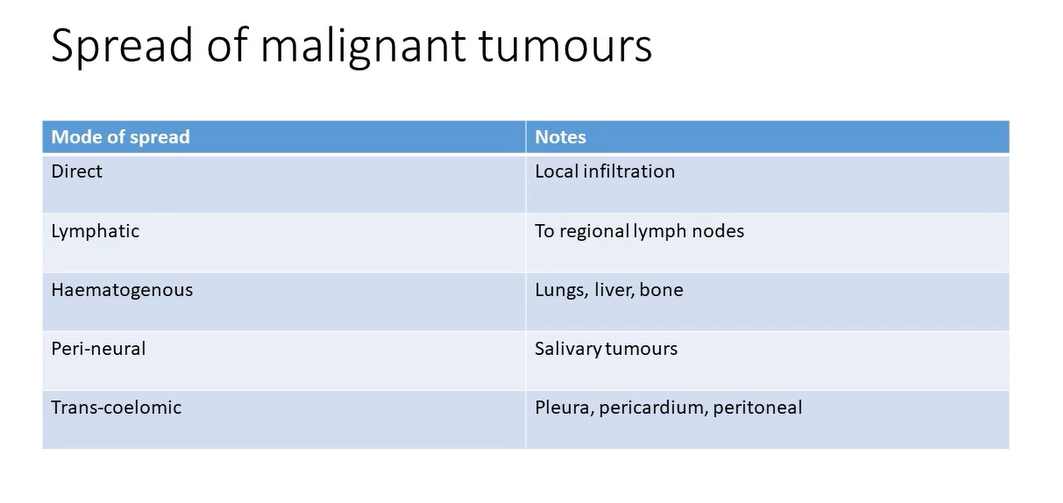
Spread of malignant tumours 5
infiltrate local tissues
may gain access to lymphatics
may gain access to venous circulation
may head straight to lungs liver bone etc
may spread along nerves
normal structure and function of squamous cell epithelium
forms lining of oral mucosa
barrier formation
multiple layers of cells
loose layer of keratin on the surface
epithelium sits on a layer of connective tissue called the lamina propria nd is well demarcated by the basement membrane
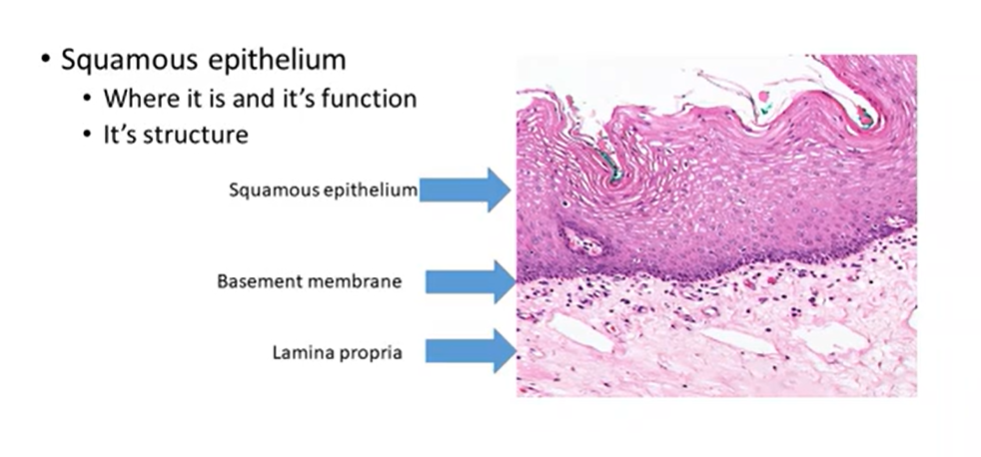
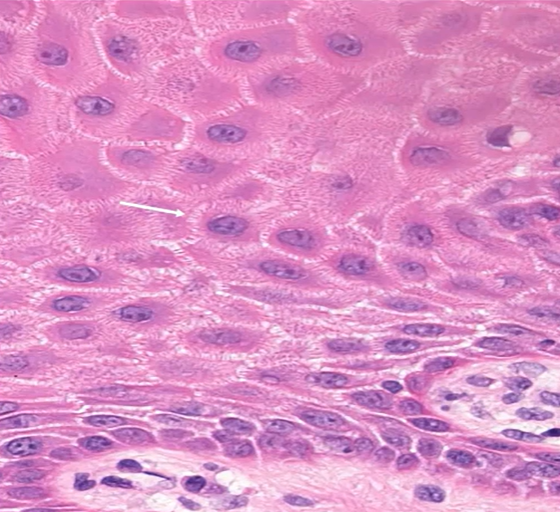
squamous cells
attached by intercellular bridges
spread of malignant squamous carcinoma local infiltration
undergo genetic changes - lose those tight attachments
Lose tight attachments
Disrupt / dissolve the basement membrane - no longer confined
Enter connective tissues / acquire mobility and gain destructive powers to damage the stromal tissues that are in their way
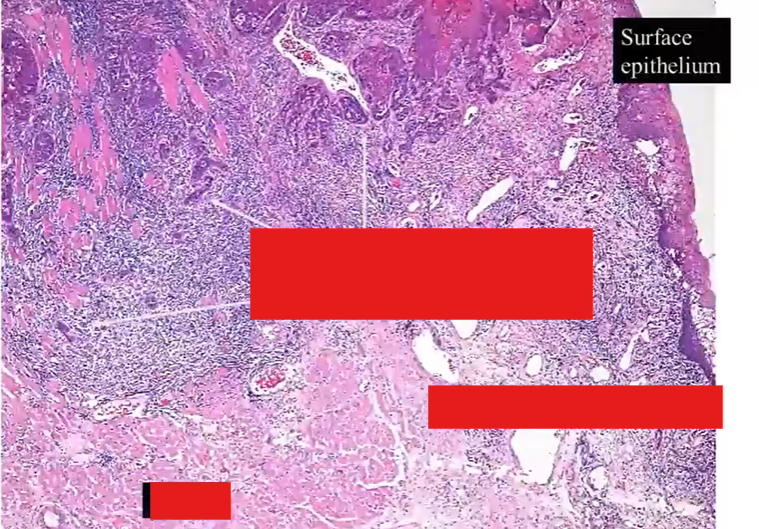
notice the infiltrating islands of cells that extend from the surface epithelium on the top right
they’re entering and breaking up the muscle layers - which still remain quite bright pink
lots of associated inflammation
the tumour islands do bear some resemblance to the surface squamous epithelium - but more chaotic version of it
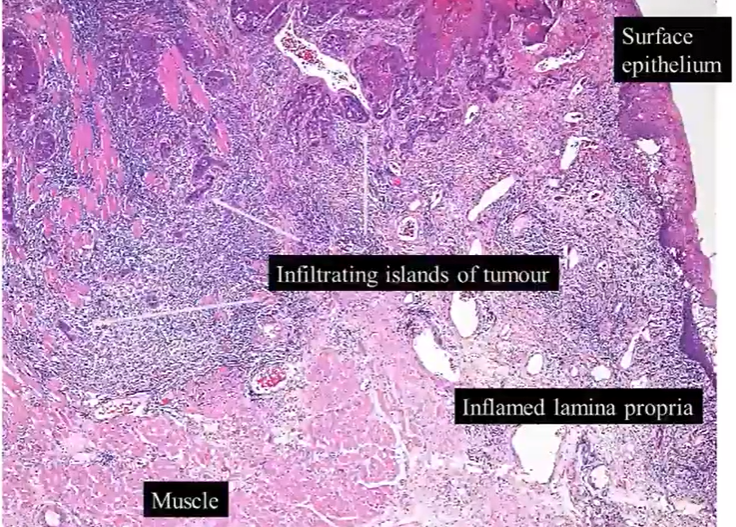
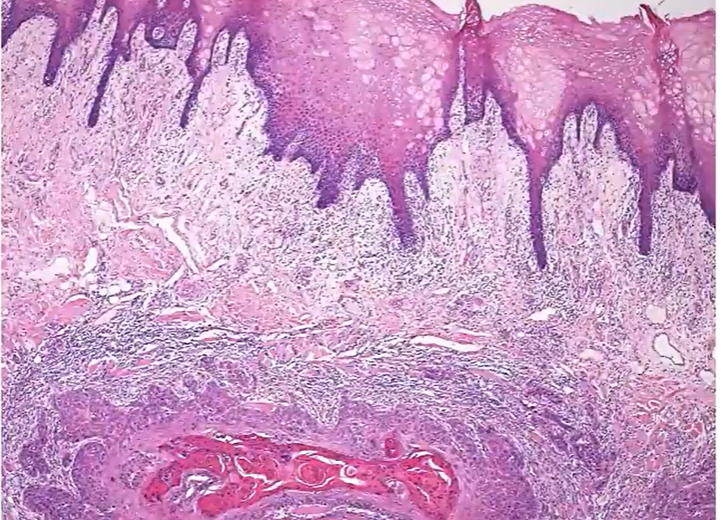
normal epithelium, beneath it, there’s a very similar looking island (tumour) - keratin pink centre - looks chaotic, atypical cells
invasive infiltrating squamous cell carcinoma
if the cells resemble the epithelium but theyre away from the basal cells - them why do they resemble epithelial cells? surely theyre in the lamina propria now and should resemble fibroblasts or adipocytes
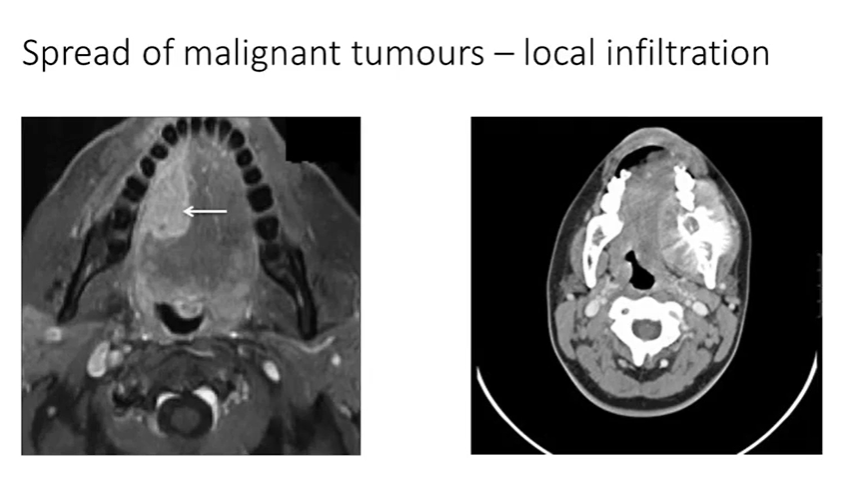
cant diagnose as a squamous cell carcinoma because you’d need a piece of tissue
mass with a different signal - measure size depth and extent - could be a carcinoma, sarcoma or lymphoma
white area - same signal as normal bone - bone tumour - osteosarcoma
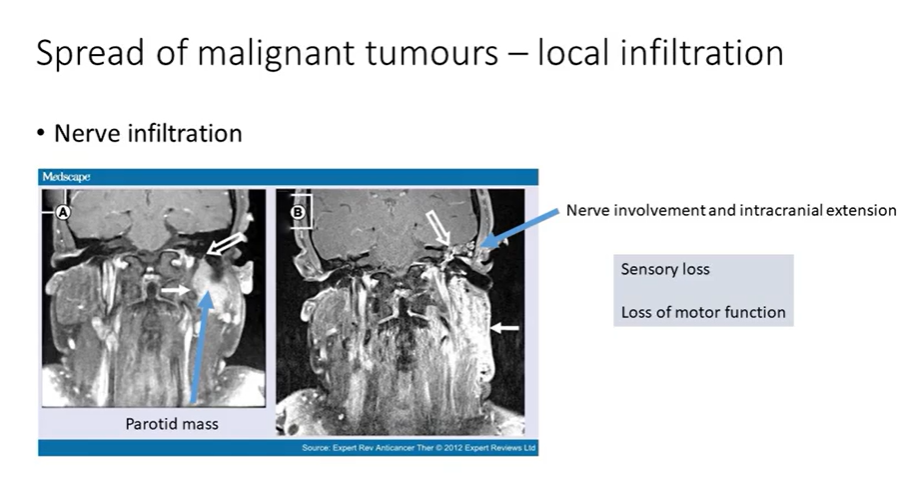
some salivary gland tumours have a propensity for neural spread - coronal MRI scans of a mass in the parotid
extension of this mass into the facial nerve - cranial fossa
symptoms may include sensory loss or loss of motor function
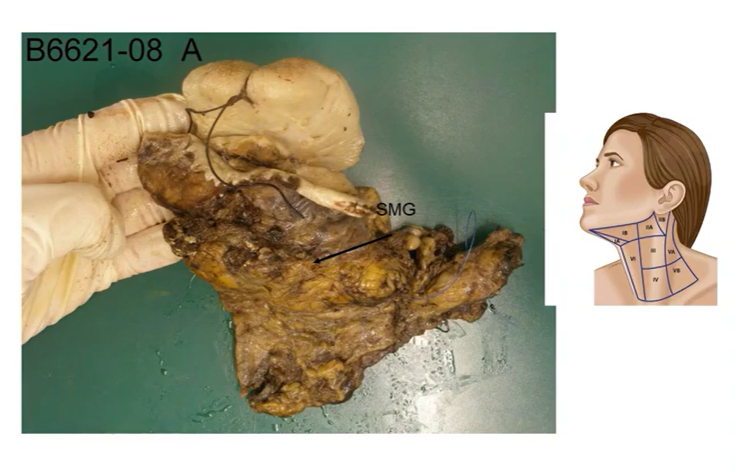
spread of malignant tumours - lymphatic spread
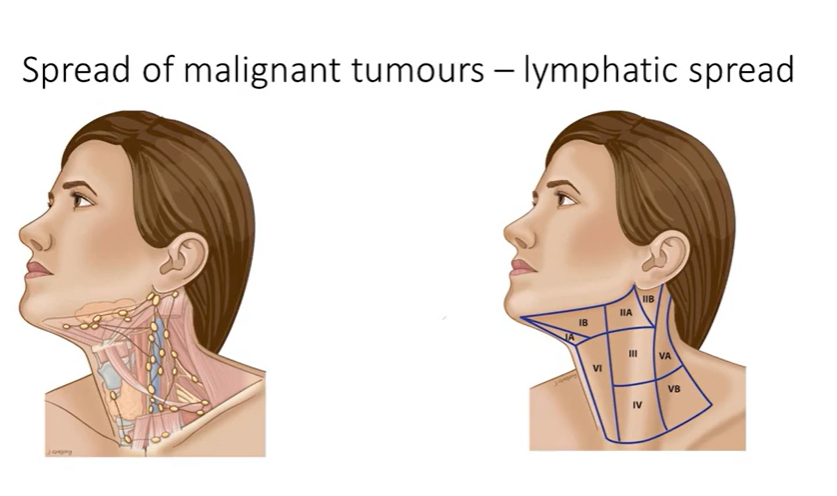
anterior tongue, floor of mouth and gingival mucoperiosteum
fibrofatty tissue of the upper central and left lateral neck 1,2,3,4 contain the tymph nodes - yellow-bown
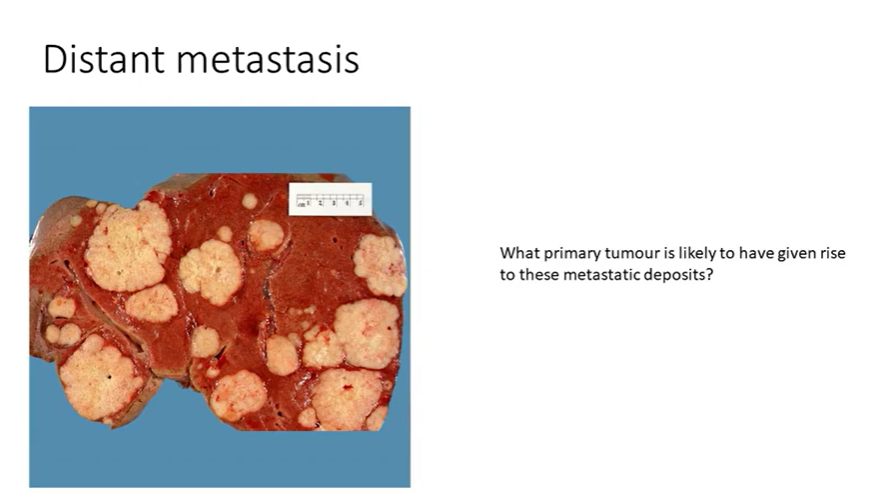
distant metastasis
liver - probably a post-mortem sample
contains multiple white nodules - consistent with metastasis
disseminated picture - likely from somewhere else compared to a lone, primary tumour - usually GI, breast and lung
how do you go from primary to a metastatic tumour?
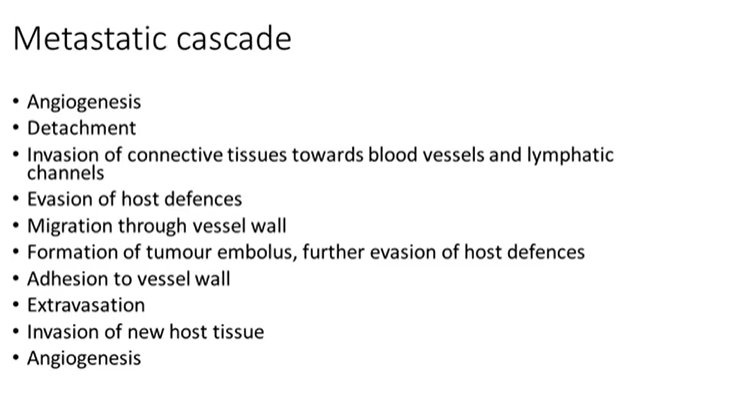
metastatic cascade
tumour cells have a tendency to secrete vascular growth factors - which encourages angiogenesis
a well vascularised tumour has a good supply of nutrients and oxygen - can keep growing
detach and dissociate spread away from each other by down regulating proteins that would normally mediate their connection
invasion requires involving mobility and possibly enzymatic destruction of stromal/connective tissues
host inflammatory cells are present in most tissues carrying out surveillance - ready to respond to tissue damage or infection
tumour cells will likely encounter CD8 T cells that could recognise them as foreign - tumour cells can develop complex pathways to downregulate T cells that could recognise them as foreign
once the migrating tumour cells reach the small calibre vessels - they can undergo a reverse of the process which allows inflammatory cells out of the vessels - gain access to the lumen
once they’re in the vessels they need to continue to evade host defences - macrophages lymphocytes
adhesion to vessel walls - but i thought immune cells also marginate?
extravasation - leave the vessels - set up their own blood supply
metastatic cascade
what are some non malignant effects of tumours? 3
increased tendency to thrombosis
Cellular over activity e.g. overproduction of a hormone that would be expected to be produced by that particular tumour cell type, such as parathyroid adenoma or carcinoma - hypercalcaemic
Paraneoplastic phenomenon - Set of signs and symptoms that are a consequence of the presence of the tumour but not directly attributable to it e.g secretion of hormones and other substances that wouldn’t normally be secreted by the tumour cell type - eg raised parathyroid levels - but no parathyroid tumour - they have a lung cancer - lung cancer cells are producing parathyroid hormone
Factors affecting prognosis 8
Tumour type - some have an excellent prognosis such as a thyroid cancer called papillary carcinoma vs small cell carcinoma of lung - disseminates readily
Site and size; resectability - 1cm in brain is worse thana 5cm on finger
Differentiation - well differentiated tumours do better
Degree of cellular atypia
Depth and extent of invasion
Mitotic index and degree of mitotic atypia
Regional lymph node involvement
Distant metastasis - already metastasized - poor
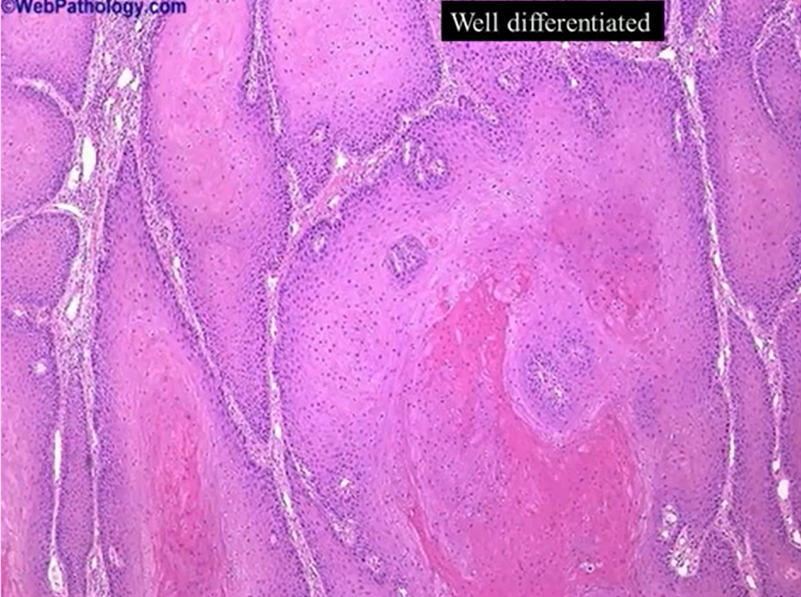
well differentiated - look almost identical to the cells you’d find in mucosal tissue - filling and invading the connective tissues - carcinoma - because they’re not where they’re meant to be
constituent cells are bland and monotonous and evenly spaced - normal - keratin formation
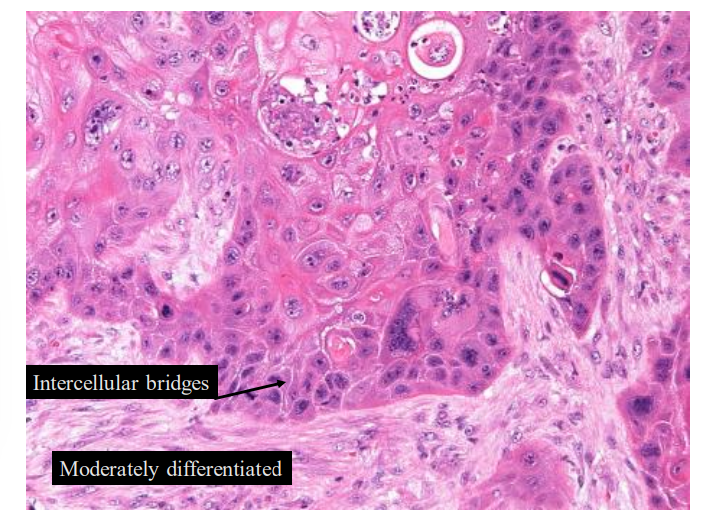
moderately differentiated tumour
intercellular bridges - normal characteristic of squamous cell
is some keratin
much uglier - cellular atypia
in the fibrous layer of the connective tissue of lamina propria - not in the surface - infiltrative - carcinoma
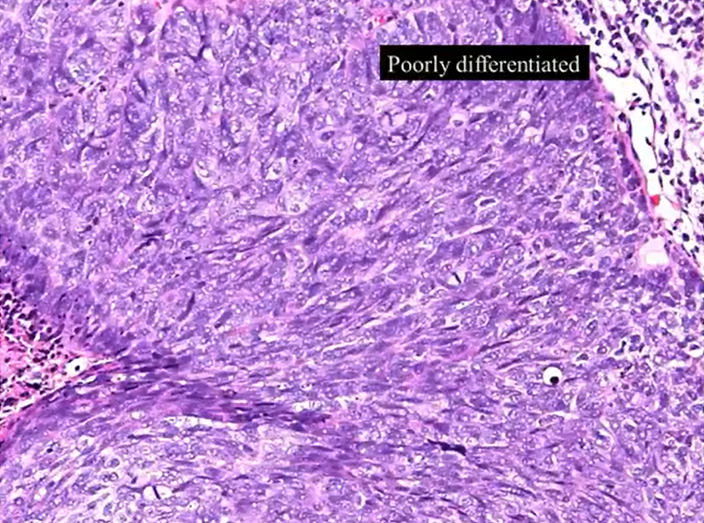
poorly differentiated - no intercellular bridges - no keratin - why squamous?
we’d diagnose by looking a at a bigger sample and try and look for one that looks like a squamous cell/has a intercellular bridge
or immunohistochemical stains - antigens that correlate to squamous differentiation
factors affecting prognosis - subjective vs objective observation
subjective - differentiation/atypia
objective - depth and extent of invasion, mitotic count
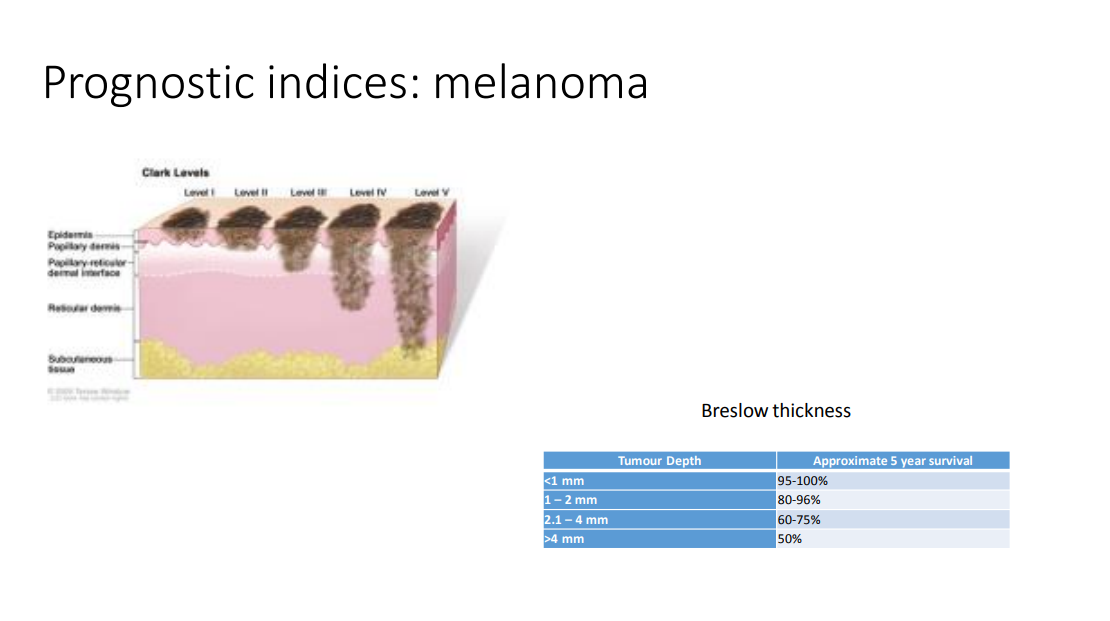
prognostic indices - melanoma
clack level - depth of invasion of melanoma
distance from basement membrane to the lowest down tumour cell - Breslow thickness - approximate 5 year survival
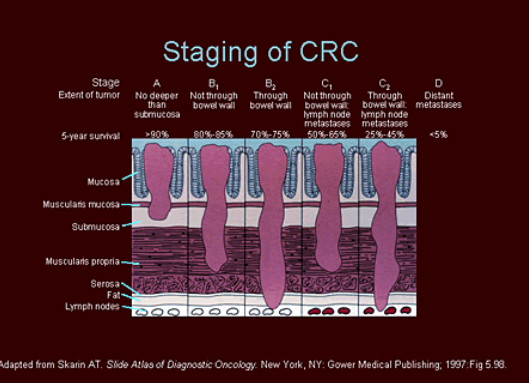
Prognostic indices: Dukes for colorectal cancer
Dukes A: Confined to bowel wall
Dukes B: Invading into the muscularis propria layer or beyond, lymph node negative
Dukes C: Lymph node metastases
Dukes D: Distant metastases
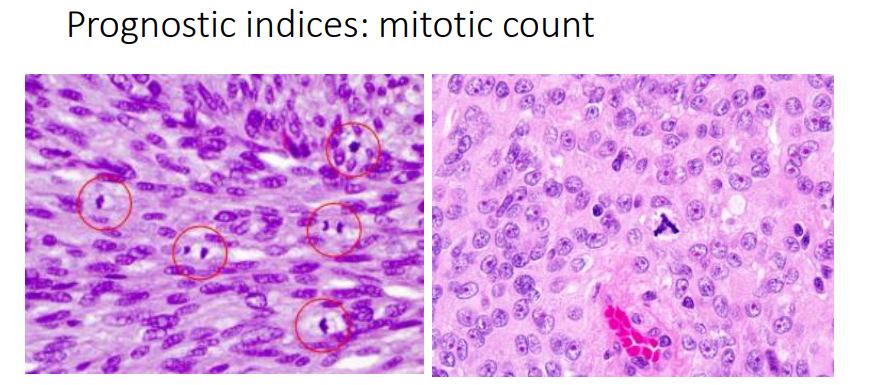
Prognostic indices: mitotic count
count how many mitosis there are - and atypical forms which may indicate greater level of genetic derangement
diagnosis - techniques
You need a tissue sample for diagnosis of presence of a tumour and also to sub-type it
Radiology can help to define size, extent and structures involved and might give some clues as to the tumour type
Tissue
Fine needle aspirate (FNA) - cells aspirated and placed on a slide - accurate subtyping not possible and prognostic indices also not possible - but may be required for assessing lymph nodes who has a positive tissue biopsy for squamous cell carcinoma
Histology (biopsy) - gold standard
Immunohistochemistry and genetic testing of tumours
Refer to laboratory diagnosis of disease lecture
Screening
The systematic search for cancer in people who have no signs or symptoms of cancer - find cancers early - treatment more simple
what are the two issues of screening?
False positives, Over diagnosis
Well established screening programs
Cervical, Breast ,Colorectal
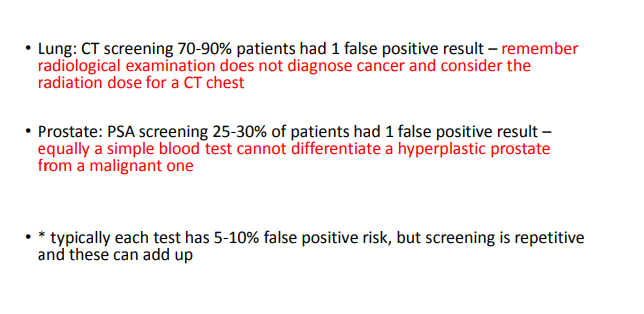
why is screening not a thing for lung, prostate or thyroid cancer?
Lung: CT screening 70-90% patients had 1 false positive result - also consider radiation dose of a CT
Prostate: PSA (protein in blood) screening 25-30% of patients had 1 false positive result
* typically each test has 5-10% false positive risk, but screening is repetitive and these can add up
campaigns for thyroid cancer
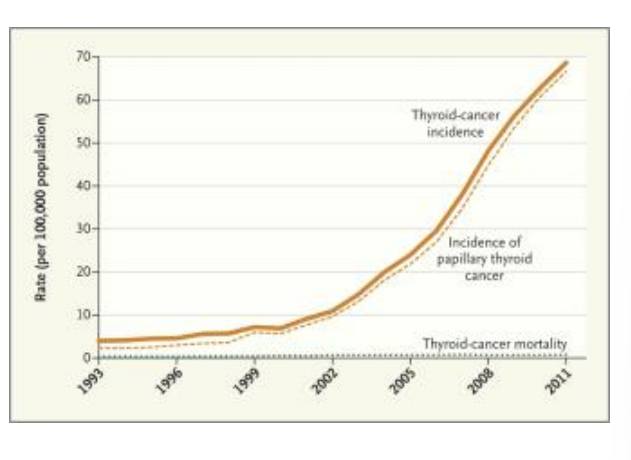
papillary thyroid cancer has a good prognosis - overdiagnosis - cancer may not have gievn them medical problems
are there any oral cancer screenings
no but examine mucosa in intraoral examination
staging vs grading
grading is assessing tumour differentiation- well/moderate. Poor
staging uses a TNM classification
T- tumour 1-4 - size and structure of tumour
N - lymph NODES 1-3 - number and type of lymph nodes invaded
M - metastasis 0 no, X yes
cancers have unique staging systems