Looks like no one added any tags here yet for you.
Response against helminths:
-Big giant worms so we need to use humurol response (extracellular).
-Mast cells, Eosinophils, and complement attack worms. Break them down and dedric cells pick up the pieces and present antigen (remember bc they are APC) on MHC II to Th2 (relate this to extracellular activation of adaptive WBC in notes)
-Th2 has interluekins Il4 (activates esoniphils and IgE production) IL5 (stim goblet cell to secrete mucus) and IL13 which (causes smooth muscle contractions)
response against protozoans
-small enough to be engulfed so use macrophages and neutrophils (Prof Phagocytes Protozoan—> all start w P)
-exocytis the parts, dendric cells pick up pieces and display antigen on MHC II and activate TH1 that activates NK or CTL to attach to infected cells and release proforin and granzymes. (relate this to intracellular inflammation activation of adaptive WBC)
Protozoa
first animal
eukaryote
no cell wall
single celled
cell membrane made of contracile fibers enabling movement in most
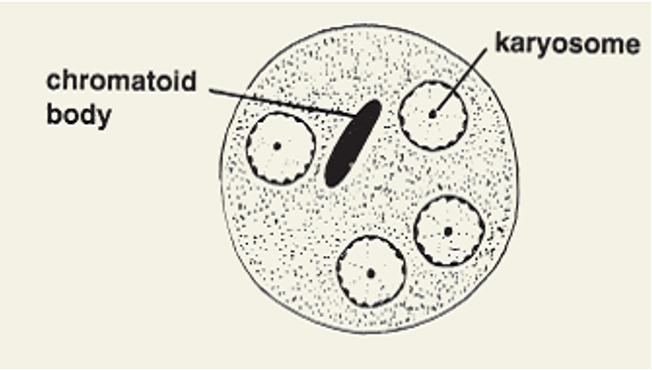
has nucleus, Chromatid body (extra DNA), Kinetoplast (nonnuclear DNA present in addition to host), karysome (DNA containing body close to or within nucleus), cytoplasm has 2 layers: Ectoplasm (outside layer, clear ring, aids locomotion, engulfment, respiration, excretion, and protection) and endoplasm (inside layer surrounding organelles).
Can reproduce sexually (rare) or asexually
- Binary fission
Division of nucleus followed by cytoplasm.
Longitudinally (Flagellates)
Transversally (Ciliates)
Any plane (Amoebas)
- Multiple fission (schizogony)
Nucleus undergoes multiple divisions
- Endodyogeny
Internal budding of daughter cells
- Asexual reproduction occurs in trophozoite stage.
- Sexual reproduction is rare: Conjugation: Reciprocal exchange of nuclear material. Only in Ciliates (B. coli). Gametogony or syngamy: Gametes are produced and fertilization results in a zygote. Occurs in sporozoans and gives rise to sporozoites by sporogony (Plasmodium). Exception: Cryptosporidium- Undergoes both asexual and sexual reproduction in humans.
two stages: Trophozite stage- active metabolic stage, actively growing, reproducing, and dividing. Cyst stage- dormant environmental stage, endures unfavorable conditions and has a resistant cyst coat.
most infections are intracellular few are extracellular
Balantidium coli
Blood Ciliate
Phylum: Chiliophora
Family: Balantididae
ONLY cilate that infects humans
Dysentary
rare
Globally distributed: more common in tropical and subtropical regions like brazil and places with farm animals or poor sanatation. rare in the U.S.
Niche: intestional track: caecal and sigmoid regions of the colon
Largest protozoan
Life cycle: Natural host- Pig, Accidental host- human, and resevior- pigs, monkeys, rat
2 stages: Trophozoite stage- invasive stage, active, ovoid cilliated cell, 2 nuclei (micro and macro), funnel shaped cytosome near anterior end, contracile vacuole, and encolsed w a pellicle showing longitudinal stiriations. Cyst stage- infectious stage, oval shaped, 2 nucli, and thick double cyst wall.
Steps of infection: 1) ingest cyst from fecal oral matter. 2) Excystation (cyst—>trophozoite) in the small intestine. 3) trophozoite travel large intestine where they feed on bacteria and reproduce. 4) Can encyst or cause ulcerative pathology by causing inflammation in colon wall. 5) excretement. (cyst are viable for 2-3 days)
Diagnostic: Stool sample- wet mount slide and look under micro from stool sample or intestional scraping for trophozoite or cyst stage. Confirmed by PCR. Diarrheic feces- rotating cila and both nuclei. Firm stool- cyst may be observed based on size and macronucleus. Endoscopies and biopsies can be used if u think someone has it. Must collect mutiple samples due to infreq of organism outside infection.
Rx:Tetracycline, doxycycline, and metronidazole.
Prevention: sanatation, dont kiss pigs.
Disease it causes is Balanitis. No bias, and most ppl are asymptomatic, immunocomprormised are more prone to it.
Symptoms: Asymptomatic in healthy individs, acute colitis, or chronic infection. Acute colitis or chronic infection cause abdominal pain. Chronic infections cause alternation between diarrhea and constipation. Protracted infections can cause dysetery.
Amoeba
can be free living or intestional
Intestinal: entamoeba histolytica
free living/brain eating: Naegleria fowleri, Acanthamoeba, and Balamuthia.
rare
move by pseuodopodia and amoeboid movement
Phylum- sacromastigophora
class- sacrodina
order- amebida
morphology: plasma lema- thin and elastic limiting membrane. Ectoplasm- lies beneath plasma lema and free of granules. Endoplasm- has granules and moves. Pseudopodia- followed by ectoplasm and allows for movement.
reproduce by binary fission or budding
engulf prey and digest it in food vacuoles. DESTROY DESTROY DESTROY
Entamoeba histolytica
intestinal amoeba
can cause intestinal amebiasis or extraintestinal manifestations
amebic dysentary
liver abscses
amebic ulcerative pathology
like to eat RBC and neutrophils
Globally distributed: tropic areas but not limited to warm areas. More common in developing countries and areas of poor sanitation.
third leading cause of death
90% of those infected are asymptomatic
class b bioweapon
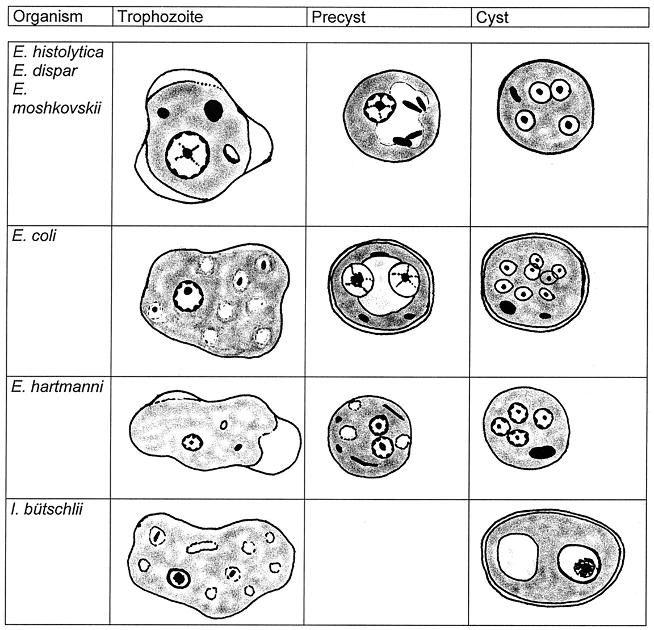
Morphology: Trophozoite (active)- only stage found in human, viable for 5 hours after infection, resistant to environmental changes. Pre-cyst stage (transitional)- can occur in lumen of gut or outside host, glycogen vacuole, 2 chromatid bars, begins dev cyst wall, trophozoites undergo encystment in feces. Cyst stage (infectious stage)- premature cyst has 1-4 chromatid bars, glycogen vacuole, and single nucleus. Mature cyst has no glycogen vacuole and is quidrinuclueated, resistant to high temp, acidity, ph, environmental conditions, and chlorine.
transmission: fecal-oral, anal, contaminated food/water, feet of flies can carry it, and poor sanitation.
Steps: 1) Humans become infected when they ingest contaminated food or water carrying mature cyst. 2) cyst undergoes cytoplasmic division and excyst 4 small amoeba in small intestine lumen. 3)These 4 undergo cytoplasmic division and produce 8 small amoebae. 4) these 8 trophozoites travel to large intestine where they feed on host, mature, and reproduce. (EAT EVERYTHING)
In 80% of infections, the trophozoites will encyst in the lumen of the large intestine and be excreted.
In 20% of infections, the trophozoites will invade the mucosa and submucosa of the large intestine.
In 1% of the cases the invasive trophozoites will cause extraintestinal disease by going to liver.
prevention: good hygeine, safe water and food especially when traveling, avoiding anal, and washing hands and fruits and veggies.
Diagnostic: Stool sample using wet mount and iodine and look for motile trophoziotes with phagocytosed RBC or cyst. E. dispar looks exactly like it so use PCR to distinguish. ELISA can also be used to differentiate but this is more expenisve but more accurate. U have to look at antibodies 2 weeks after infection.
screening: colonoscopy, CT scan, ultrasound
pathology: (attach, lyse, invade,, ulcer) use lectin glucose/ galactose to attach, release enzymes: phospholipase A and neuraminidase. Eat living cells (like RBC). Use CXCL8 to attract neutrophils to eat them and uses trogocytosis (nibbling of cells) to eat cells (like apoptosis).Use metacollagenase to spread through tissue and cause damage which causes inflammation and amebic ulercative pathology. (flask shaped ulcers are the hallmark)
Rx: cyst stage use paramycin and iodquinol. trophozoite stage use metronidazole.
Immune protection: secrete IgA to prevent lectin attachment and we release nitric oxide to protect.
Intestinal amebiasis- Diarrhea, dysenterya, chronic non dysentry diarrhea.
extraintestional amebiasis- liver abscess and brain damage.
amebic liver abscess- can cause fever and weight loss. Liver lesion produces anchovy past. Trophozoites present.
Amebic Dysentery is a “bloody” mucoid diarrhea caused by:
o bleeding into gut lumen and loss of overlying gut mucosa.
o resulting from adjacent deep ulcers joining (coalescing).
o undermining the overlying mucosal lining.
o Can be fatal. Third deadliest disease bc in colon and losing blood and electrolytes.
- Necrosis: pathological death of cells resulting from irreversible damage.
symptoms: diarrhea, dysentry, fatigue, fever, excessive gas, rectal pain, and vomiting.
Non-pathogenetic amoebae
- Entamoeba coli*
Commensal
Larger than E. histolytica does not eat RBC.
Non-invasive, only in lumen
- Entamoeba dispar*
Not distinguishable from E. histolytica
Non-pathogenic
- Entamoeba gingivalis*
Lives in mouth
No cyst stage.
Seen in people with gingivitis.
Leeuwenhoek described.
Naegleria flowleri
brain eating amoebae
opportunistic
Phylum: Percolozoa
Order: Schizophernia
genus: Naelgeria
shapeshifting amoebae flagellate
distributed globally
found in water and soil
have feeding cups to eat ur brains and blood vessels
Stages: cyst stage- withstand temp drop, temp up to 113, and chlorine up to 50 ppm. Amoebae trophozoite stage- infectious stage/invasive stage, found on surface of vegetation, mud, and water, feeding and reproducing, feeds on bacteria, replicates by binary fission during which nuclear membrane stays intact. Amoebae flagellate stage- biflagellate; can switch to this form when environmental conditions are unfavorable and switch back when out of harm.
Life cycle: 1) inhale through nose and they attach to olfactory bulb. 2)amoebae cause pathology by secreting enzymes to cause damage which triggers inflammatory responses.
Disease it causes is PAM (primary amebic meningoencephalitis)
Rx: antibiotics given first, then primary antifungal drug amphotericin B. given intravenously or near spinal cord space. Investigational drug miltefosine along with using it with induced hypothermia. (coming in w symptoms less than 48 hours is better chance)
rare, deadly, not much known to treat
94% mortality w 4 survivors
symptoms: (2-9 days)- headache, fever, vomiting, nausea. (progressive)- stiff neck, hemorrhage, dazed and confused, loss of balance, seizures, hallucinations, coma, death,
Dx: spinal tap: trophozoites in CSF. Clear- viral, protozoan, or fungal. Cloudy- neutrophils. Can also do autopsy and look for trophozoites found in immunohistological preparations. PCR being dev.
Acanthamoeba spp
free living
found in dirt and water. cyst in dirt and trophozoites in water
Phylum: Amoebozoa
Family:Acanthamoebidae
Morphology: Cyst form: found in dirt, double walled, and highly resistant to environmental conditions. Trophozoite form- spine like pseudopodia.
Commonly associated w contact lens wearing—> can cause eye infections like Unilateral photophobia (tearing and redness)—> blurred vision and blindness
Can get into eye and go cause brain damage, can get into cut, can be inhaled/swallowed.
Causes GAE (granulomatous amebic encephalitis)
Symptoms: rash w aids patients, seizures, paresis, mental deteration. intracranial space lesions, death
symptoms are fatal
Long time for pathogenesis to occur and to present symptoms
occurs w dried cysts
Rx: Acanthamoeba Keratitis- Miltefosine and topical biguanide or chlorhexidine.
Dx: Acanthamoeba Keratitis- cornal scraping using calciflour white for rapid diagnostic. GAE- brain biopsie, culture, and immunofluroescence micro using monoclonal antibodies. CSF shows lymphocyte pleocystosis (increased cell count), and slight elevated protein levels.
Prevention- dont wash contact lense w water
no survivors of GAE
Balamuthia mandrillaris
free living ameobae
causes GAE
rare
direct pathology
DX: PCR and culture from skin lesions
RX: experimental combos (nothing set in stone)
Cyst found in soil and dust, trophozoite in water.
Entry site: cuts, inhalation.
Symptoms may present weeks to months later. Present in any months (warm and cold). Fever, headache, vomiting, lethargy, nausea. Progressive symptoms: Mental health changes, Seizures, Weakness, Confusion, Partial paralysis, Difficulty speaking, Difficulty walking swelling of brain.
After getting into a wound, B. mandrillaris causes a skin lesion. An asymptomatic granulomatous can occur where the amoeba enters: skin/face. Single or multiple lesions may be present. (rubbery in consistency) Then makes its way to CNS.
May see skin lesions and rashes worse in immunocompromised but effects anyone.
*Week or under symptoms is caused by PAM, 21 days or more GAE
Flagellates
intestinal, oral, and genital
Phylum- Sacromastigophora
subphylum- Mastigophora
Class- Zoomastigophora
Giardia lamblia
Flagellate
Distributed globally—> but more seen in areas up N that have MT and cold water
Water born pathogen—> likes COLD water
only protozoan pathogen seen in small intestine of hmans
Causative agent of giardias—> commonly known as daycare diarrhea, travelers diarrhea, and beaver fever.
Niche- duondem and upper jujenum
Morphology: Trophozoite stage- pear shaped, bilateral symmetry, owl face, 2 nuclei and 4 flagella (make it motile but slow), reproduce by binary fission, and ventral sucking disk for attachment. Cyst stage- oval shape, 4 nuclei to help differentiate from commensual, infective stage, found in hard stool, resistant to temp (freezing), ph, and chlorine
Transmission: Increased susceptibility is associated with Type A blood, achlorhydria, use of cannabis, chronic pancreatitis, malnutrition, IgA deficiency or hypogammaglobulinemia. Get it from fecal oral surfaces like diaper chagning places, get it from swimming in ponds rivers streams or lakes that have it, eating contaminated food or water/ice that has it, being around someone who has it, if u handle ur dog poop and they have it, and traveling to places where its common.
life cycle- 1) ingest (as little as 10 cyst and happens within 30 min) 2) excystation occurs in small intestine producing trophozoites (1 cyst = 2 trophozoites) 2) reproduce by longitudinal binary fission in lumen of small intestine 3) can be free living or attached to mucosa by ventral sucking disk and feed by phinocytosis 5) encystment occurs during unfavorable environmental conditions; cyst found in hard stool; 200,000 per gram of feces and can remain viable for weeks or months in cold water.
Symptoms: most are asymptomatic. ( Acute Giardiasis )- cases present from 2-9 weeks; flatulence, burping, abdominal pain, fatty large volume watery foul smelling greasy non-bloody diarrhea. ( chronic giardiasis ) malunutrition and failure to thrive
effects children more commonly/ they are more at risk bc malnutrition and can lead to weight loss, vitamin/nutritional def, dev delay, and slows growth.
Patients with hypogammaglobulinemia (Ig A deficiency) suffer from prolonged, severe infections and are poorly responsive to treatment.
Dx: stool test- look for trophozoites and cyst in hard stool- trophozoites r dorsally convex, pear shaped, flat, 2 nuclei, and “smiley face”. RIA and ELISA. String test (swallow gelitin capsule on a string and let travel to small intestine, pull back out and run wet sample under micro of whatever is on string)
Immune evasion: use antigenetic variation- Antigenic variation—>VSG, alter our normal flora and microbiota, and induce apoptosis of brush boarder cells
Pathology- VSG, Trophozoites induce apoptosis leading of enterocytes leading to shortened flattened villi and apoptosis of brush boarder cells reults in malnutrition. Increase lymphocyte infiltration, and interrupt epithelial barrier dysfunction leading to diarrhea.
Prevention: use clean water sources, proper disposal of waste, no water sports 2 weeks after diarrhea, good hygiene, and be cautious in endemic areas.
doesn’t invade deeper tissues just stays in crypts of small intestine
Rx: metronidazole; used to give paromycin to prego ladies
Trichomonas
trophozoite form only
3 species in human: T. vaginalis, T. hominis, T. tenax
Trichomona tenax
Commensal of the oral cavity
smaller than T. vaginalis
“teeth”
Trichomona hominis
harmless—> commensal of the cecum
pear shaped w 5 anterior flagella and undulating membrane (full extent of body)
Trichonoma vaginalis
STI
transmitted through sexual acts
most common curable STI
underreported bc ppl don’t want to be said they have a STI or bc symptoms look like something else—> why men are more “commonly” infected than women bc symptoms in women can look like menstration cycle symptoms.
Can infect newborn (pass to child from vaginal birth)
Niche- Women- vagina and cervix. Men- anterior urethra. Vaginal ph facilitates infection and infection changes ph. Incubation takes about 10 days.
Morphology: Trophozoite form only: pear or ovoid shape, hydrogenosome, undulating mebrane that enxtends half way through body, 4 anterior flagellum and a fifth one that runs through the undulating mebrane, axostyle running through center of protozoan and looks like a tail, moves in a jerky twitching motion.
Pathology- infects squamous epithelim causing desquamation, secretes cysteine protease adhesions, lactic and acetic acid. Eats tissues and bacteria disrupt vag track and normal flora. Disrupt glycogen levels and lower ph.
Obligate parasite so needs tissue to survive
Symptoms: petechial hemorrhage caused by local blood vessel dilation (strawberry mucosa—> rash on cervix which are tiny dots) HALLMARK in women. Itching, burning, odor, redness, soreness, discomfort when peeing, frothy yellow green stinky discharge, Vulvar and cervical lesions, abdominal pain, dysuria, and dyspareunia in women. Itching burning and pain when peeing and discharge from penis in men. RARE neonatal pneumonia and conjunctivitis been reported
Dx: Microscope imaging of discharge to look for twitching trophozoites with an abundance of leukocytes. Stain to find trophozoites. Organisms gather in a “trich party”. Background of sqaumous cells often have a perinuclear halo and arent budding. Increased number of neutrophils. Culture if micro is negative, rapid diagnostic test- PCR.
If u have one sti most likely to have mutiple
Rx: metronidazole
Prevention: condoms
Move like amoeba but aren’t amoeba
Blastocystis hominis: anerobic protozoan of unknown taxonomic class —> previously classified as yeast. Niche- large intestine. Gi track symptoms. 3 forms: vacuolated (reproduces by binary fission and has large central vacuole), Amebiod (sporulates), and Granular form.
Dientamoeba fragilis: looks like amoeba but classified as flagella. Only trophozoite form. Niche-colon. Associated with diarrhea, flatulence, abdominal pain, nausea, and fatigue in young kids. Each trophozoite has 2 nuclei. Higher association w pin worms.
Hemoflagellates
trypanosomes and leishmania
Shared morphology: single nucleus, single flagellum, kinetoplast, deep stained basal body, orgininated in belpharoplasty, internal portion known as axoneme, free flagellum at anterior end traverses on the surface as a narrow undulating membrane.
4 forms: (this instead of trophozoites and cyst) 1)amastigote- no external flagellum, vertabrate host (intermediate). 3) promastigote- no undulating membrane, vector (definitive host). 3) epimastigote- flagellum runs in short undulating membrane, occurs in vector (definitive). 4) trypomastigote- occurs in vertabrate (intermediate), flagellum runs alongside entire body b4 emerging an external flagellum.
Trypanosomes
digenetic: 2 host
vertebrate host is intermediate host, fly is definitive host.
Vector is: Tsetse fly or Triatome bug
Classification: salivaria (spit) or stercoria (feces)
Distribution req presence of vectors. Commonly seen in Africa like Ehtiopia and Tasmania.
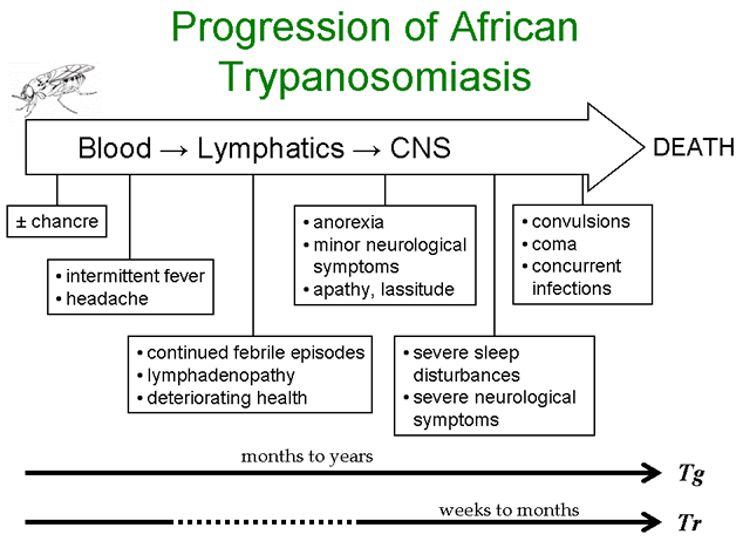
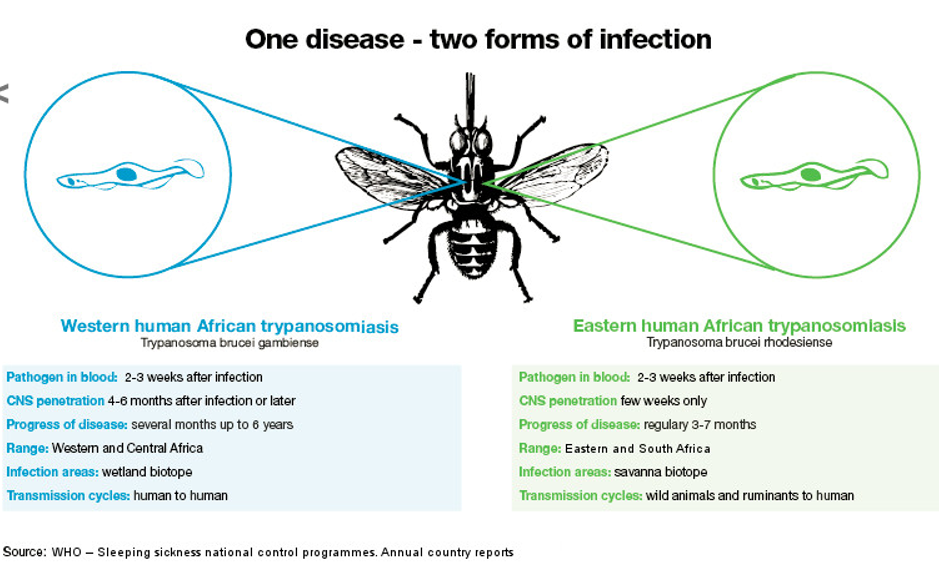
Causes HAT (human African trypanosomiasis)
T. brucei gambiense , T. brucei rhodensiense, T. cruzi
Tr and Tg VERY similar ( only diff is speed, location, and transmission cycle)
Life cycle: Only need 300-500 metacylic forms for infection; tsetse fly injects 40,000 of them into blood. Transforms in long slender trypomastigote form. This form goes into connective tissue and divides by binary fission (some go into lymph nodes and CNS). This form will cause surface antigen changes as it divides every 1-2 days and enters blood. They begin state change into short stumpy trypomastigotes that are taken up by tsetse fly during blood-meal.
incubation period outside host: once inside fly midgut, the short stumpy trypomastigotes undergo binary fission and dev into long slender procyclic forms. After 2-3 weeks the procyclic forms migrate to the salivary glands and dev into epimastigotes. These then undergo binary fission and dev into the infectious metacyclic trypmastigote form. Takes ab 25-50 days to complete.
Pathology: parasite replicated in connective tissue. Can invade lymph nodes, blood, and CNS. Over exhaustes the immune system. Consumes glucose way faster than host cell.
Immune evasion: Uses antigenic variation(VSG), cause inflammation, make own cytokines, avoid complement, immune system causes pathology, shutdown immune cells.
Clinical presentation: parasitemia. Symptoms r broad so hard to diagnosis. Higher chance of survival if u catch b4 CNS evasion if u dont u will die.
2 stages: 1) hemolymphatic stage- (2-3 weeks), lives in liver and spleen, causes enlargement of liver and spleen Hepatosplenomegaly and lymphadenopathy. If in cervical lymph nodes- Winterbottom’s sign (hallmark). Myocardititis more often in T.b. rhodesiense. Leukocytosis and thrombocytopenia. Joint pain (observed with increased parasitemia). Inflammation of heart bc in blood system. Painless chancre at site of infection; More common in T.b. rhodesiense. Intermittent Fever (comes in episodes). Rash (itchy rash), anemia (bc eating more glucose aka sugar), and weight loss in some (no energy to eat or do anything). Cachexia -Extreme emaciation. Malaise. Overall blood cells stop reproducing bc they r tired. Stage 2: invades CNS, mental dullness, stiff neck, depression, sleepy, seizures, tremors, coma, and death (presents like meningitis).
Dx: Wet mount and look for Trichomastigotes. - With T. b. gambiense parasitemia levels are usually low and variable so much more difficult. May require concentration of blood to detect. With T. b. rhodesiense, parasitemia is usually higher than with T. b. gambiense and symptomatic patients typically have detectable parasites in the blood. Animal innoculation (old), seriodiagnostic for screening, Card aggulation trypanosomias test (CAT) and if antibodies clump test is positive, and IgM antigen specific antibodies; not reliable and only used for tbg.
Treatment- pentamidine or suramin (doesn’t cross BBB) in stage one. In stage 2 use mel-B (crosses BBB but not avaliable in US so will prolly give u antibiotics or miltefosine)
Prevention: wear long sleeves, use bug spray, use tsetse fly traps, check cars, avoid bushes and bright clothing.
Trypanaosoma brucei rhodesiense
- Similar to T.b. gambiense.
- Reservoir in cattle and vertebrate wild game animals.
- Antigenic variation (how they get around the immune system): VSG: Variable Surface Glycoprotein surface coat. It’s a surface coat on outer side of plasma membrane of trypomastigotes composed of millions of identical molecules of one glycoprotein. VSG: Attached by Glycolipid linkage to surface of plasma membrane. This Glycolipid linkage allows parasite to rapidly clip off entire old VSG coat w/ only one specific enzyme: Phospholipase C. Parasite now has expressed a new and different VSG gene. Previous antibodies do not recognize new VSGs. (0 percent of their genome is dedicated to variable surface glycoproteins).
- T. b. rhodesiense is endemic in Eastern and Central Africa.
- Niche: connective tissues of vertebrates.
- Invade lymph nodes, blood, and finally CNS.
- Vector: tsetse fly (Glossina morsitans ) .
- Tsetse flies bite during daylight hours. Both male and female flies can transmit the infection.
- Disease: causes an acute progressing African trypanosomiasis (rapid and way more deadly).
- Kills quicker.
- Eastern African HAT
savannas
animal to human
- T. brucei rhodesiense
Salvivaria
East African Sleeping Sickness or east African HAT
Identical to T.b. gamiense.
American trypanosomiasis or Chaga’s disease
Faster acting so weeks later (on the road u go fast)
Transmitted animal to human
savannas
Trypanaosoma brucei gambiense
- T. b. gambiense is endemic in western and central Africa.
- Niche: connective tissues of vertebrates.
- Invade lymph nodes, blood, and finally CNS.
- Vector: tsetse fly (Glossina palpalis).
- Tsetse flies bite during daylight hours. Both male and female flies can transmit the infection.
- Disease: causes a slowly progressing African trypanosomiasis. Takes months to go from initial infection to CNS symptoms.
- Western HAT
- T. brucei gambiense
Salvivaria
West African Sleeping Sickness “we gamble.”
First isolated from a boat captain on the Gambia River
Identical to T.b. rhodesiense
Slower acting (months later)
Transmitted human to human
wetlands
Trypanosoma cruzi
intracellular infection—> live inside cell
cagas disease
definitive host: man
Intermediate host: kissing bug/ triatome bug (type of reduviid bug)
reservior: cats, dogs, pigs, armadillo
infective form: metacyclic trypomastigotes
Life cycle: bug bites u, and defecates by the bite. U scratch urself and feces enter bite site. Trypomastigotes in feces enter cell (heart and muscle) and fuse their vacuole w cell vacuole forming apimastigote stage which move around and burst out of cell into trypomastigote.
can be transmitted during blood or organ transfussions and from mother to fetus.
Was limited to S and central Africa but has seen spread
6-7 m ppl infected
Dx: Acute stage: Geimsa stain PCR, and skin biopsie (less common). Chronic: detection of IgG and imaging of heart or esophagus.
immune evasion: Antigenic variation, Delaying cell mediated immune resposnes, make u make Th1 in cell and Th2 in tissue, inflammation, prevent their own cytokines, increases ph in phagolysosome preventing proton pump, inhibits apoptosis, and down reg inflammatory cytokines after they get inside macrophage.
Rx: none. May use Nifurtimox and benznidazol but dont work against intracellular infections
prevention: bug spray, incestiside, places w cool air, bug traps, and eliminating breeding spots for these bugs.
Hallmark: swelling
if feces get into eye can cause Romanas sign.
leading cause of cardiomyopathy (swelling of heart)
Symptoms: Acute: (1-2 weeks after infection—> no swelling of heart or meningitis only contraction of muscles) last 1-4 months. chagoma may form at site of bite. Some people have more generalized infections like fever, lymphadenopathy, and hepatosplenomegaly. Rarely myocarditis or menigoencephalitis but if occurs results in death. Chronic: Occurs years after infection, Inflammatory response occurs with cellular destruction and fibrosis of smooth, skeletal, and cardio-muscular cells. They don’t function so you end up with cardiac myopathy, megaesophagus and megacolon (dilation of the smooth muscle)