Looks like no one added any tags here yet for you.
Problems w/ radiation (general)
1) direct clinical effects from high dose
2) delayed effects (induction/return of cancer)
3) genetic effects
We can minimize radiation but CAN’T remove it
Absorbed dose
-energy that stays in mass
-associated w/ physical effects in tissue
(Organ dose)
-mean dose in specific tissue/organ
-energy absorption per unit mass, avged over the organ
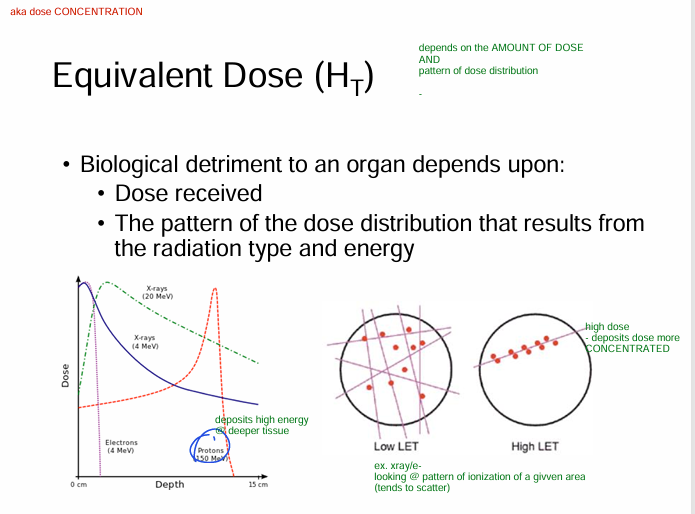
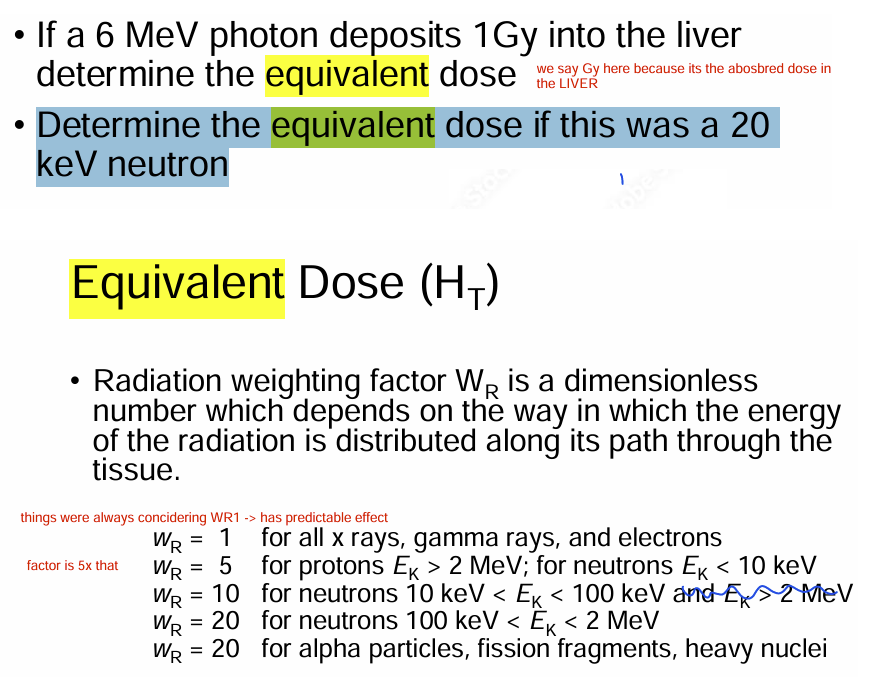
Equivalent dose (type of radiation; doesn’t account for tissue)
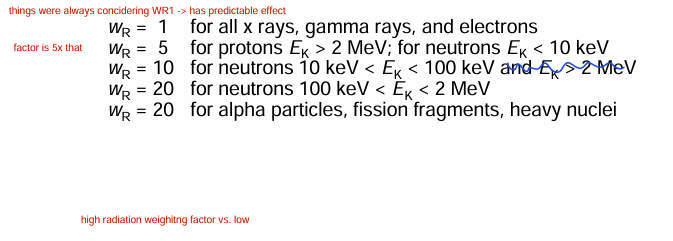
formula = organ dose*radiation weighing factor
-accounts that some radiation deposits more concentration than the other
-measure of BIOLOGICAL HARM to organ/tissue as a result of organ dose
(diff types of radiation have diff types of effects/potential to cause harm to tissue)
(ex. proton/neutron can damage more than xray, gamma, e-)
-if organ is irradiated by more than 1 type of radiation (e-,proton,neutron) equivalent dose = SUM
-units = J/kg = sieverts (NOT Gy)
(Equivalent dose)
- what does it depend on? (biological detriment)
1) Dose received
2) Dose distribution pattern (depends on radiation TYPE & energy)
Ex. proton = deeper
Ex. e- = surface
(Equivalent dose) (doubt yo uneed to know)
Radiation weighing factor
dimensionless #, depends on how energy of radiation is distributed along its path through the tissue
Effective dose (adjust equivalent dose & considers tissue sensitivity)
formula = SUM of tissue equivalent dose * appropriate tissue weighing factor
-units = J/kg = sieverts
-looks @ effects ON tissue
-measure of dose to reflect amt of radiation detriment (harm) likely to result from dose
-correlates well w/ stochastic effects (statistically could happne)
(takes equivalent dose * tissue weighing factor
→ reflects amount of radiation harm likely to result from the dose)
-aka: takes the equivalent dose *and multply by tissue weighing factor (of the tissues being HIT) as some tissues may bemore senestive than others or vice versa → takes into account of this → overall get a better idea of how much harm it will lead to in total)
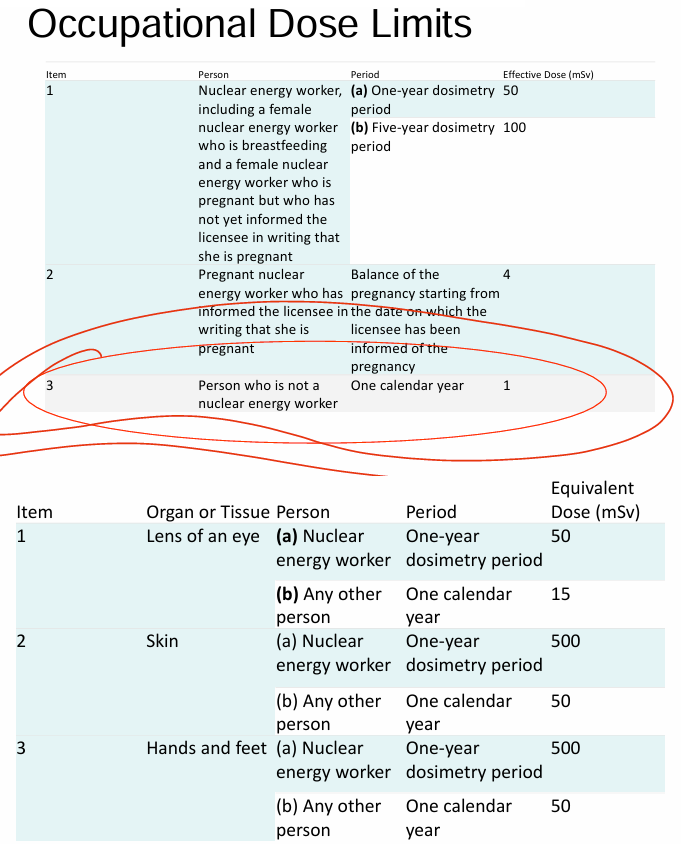
Annual dose limits for occupational and public exposure are given in terms of __
Annual effective dose
Who decides dose limits?
1) Canadian nculear safety commission (CNSC)
-regulates use of nuclear energy/materials
2) International commison on radiation protection (ICRP)
- recommend dose quantities/limits
3) International atomic energy agency (IAEA)
What are the natural sources of radiation?
1) cosmic
2) terrestrial (jake doens’t even know how to distinguihs)
3) ingestion
4) inhalation
What’s the major cause of increased radiation experiences by people in 2025?
man-made medical systems
What are the 3 categories of radiation exposure?
1) occupational exposure = workers
- exposures obtained in the course of their work
2) medical exposure = patients
- by patients as part of diagnosis
- individuals volunteering to support pts
- volunteers in research program involved in exposure
3) public exposure = members of public
- exposure by members of public
- EXCLUDES (everything else other than) medical/occupational exposure :)
Occupational dose limits (doubt you need to know)
mean radiation dose in ppl = 0.2mSv
1) in diagnostic medical exposure, the objective is to __
2) in therapeutic medical exposure, the objective is to __
optimize image quality; minimize dose
limit dose to normal tissue + deliver required dose to target volume
What is the CONCEPT to maintain low dose to healthy tissue?
ALARA - as low as reasonably achievable
What are the cornerstones of radiation protection?
1) TIME = be short
2) DISTANCE = be far away
3) SHIELDING = protective barrier
What are operational quantities?
used for radiation protection purposes
-we can’t directly measure equivalent/effective dose.
-therefore ICRU came up w/ measurable operational quantities:
1) ambient dose equivalent (area monitoring)
- room (background)
2) directional dose equivalent (area monitoring)
-things happen around you
(xray source points @ wall → hits wall → what happens on the other side of the wall → that happens to person sitting i that room)
3) personal dose equivalent (personal monitoring)
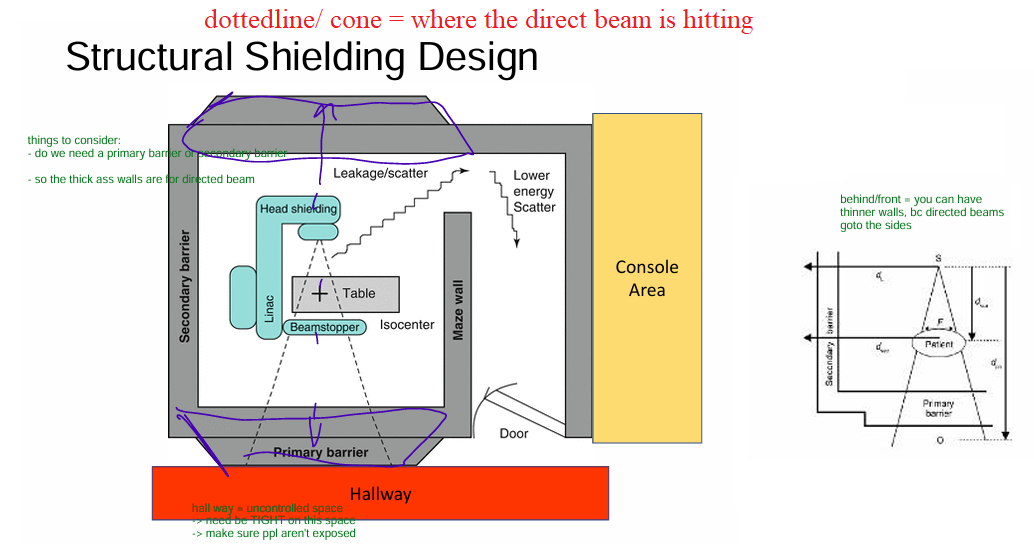
What is the STRUCTURAL SHIELDING design dependent on? (aka the room we are putting the linac in)
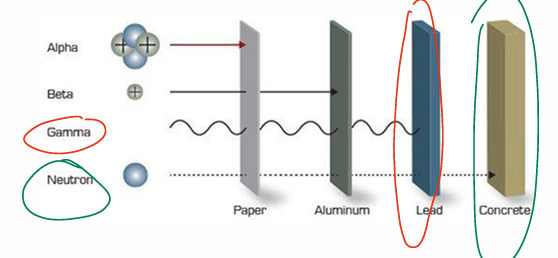
depends on QUALITY of beam (energy of beam)
aka: neutron will pass deeper → need better/stronger material
- whereas alpha won’t go through paper
Why do we need protection via structural shielding
Protect from 3 types of radiation:
1) primary
2) scattered
3) leakage radiation
What’s a:
1) Primary barrier
2) secondary barrier
1) barrier to attenuate useful beam
2) barrier against scattered radiation
Why do we have a MAZE DESIGN?
prevent direct incidence of radiation @ the door
- which can be photons or NEUTRONS (mainly focused on neutrons since they’re high energy)
- we want to reduce neutron fluence @ the door
- longer maze, hydrogenous material (polyethlyene @ door)
TLDR: make sure neutrons/scattered photons lose energy b4 they get to the door
beams w/ energies GREATER THAN __ result in _
1) 10Mv photonuclear interactions
2) neutron contamination
aka PHOTODISINTEGRATION (photons interact w/ components of head of machine)
TLDR: 10Mv or less; no neutrons produced
- 10Mv+ → high energy photon can hit nucleus of head of machine → neutrons produced an leak out (that small crevice of primary collimator)
Minimum shielding required for a door is __
6mm
After installation of radiation equipment, a qualified expert must carry out radiation protection survey.
What does this survey include?
1) equipment survey = check equipment specs + interlocks
2) area survey = evaluate potential radiation exposure to individuals + surrounding environment
- use GEIGER COUNTER
General - brachytherapy
Transfering = short paths (time)
Storage = proper sheilding (shielding)
Handling = long froceps (distance)