Rheumatology OSCE
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
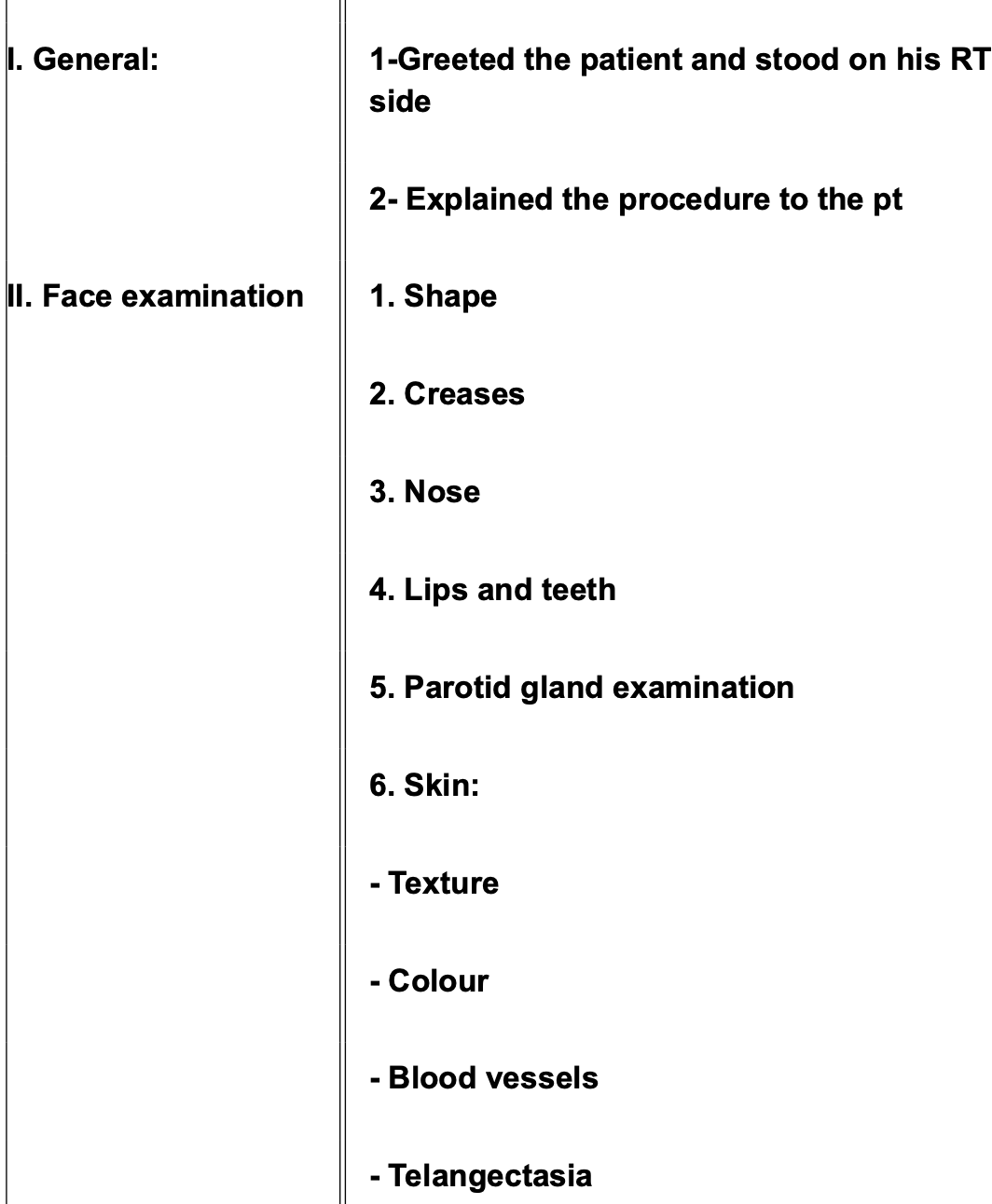
Mention items found in inspection of face of SSC.
Face elongated and younger than actual age
Hair: Alopecic patches
Forehead:
Loss of corrugations and smoothed out skin
(pinch test)
Attempt a normal pinch
unable to pinch skin = teathering
tethering to underlying structures by fibrous tissue
loss of elasticity/pliability
Loss of outer third of eye brows
Eyes:
Shrunken stony set inwards
dry eye + gritty sensation (feeling of sand/burning)
Ask the patient wether she cries or not
Nose:
Thin pinched like nose
Ask the patient did her nose shrunken in size over years or was it that size before the disease developed to
Flattened nasolabial folds
Mouth:
Perioral Skin = Purse-like lips (wrinkling/crumpling/radial
furrowing).
Lip Volume = Fish-like mouth (thin lips).
Oral Aperture
Test = 3-Finger Test (Ask patient to insert three fingers
vertically).
Finding = Narrow oral aperture (Microstomia) + Unable to introduce 3
fingers.
Intra-oral Exam
Findings = Poor oral hygiene + Loss of teeth.
Mechanism = Fibrosis causes gingival atrophy (teeth lost from
sockets) + Small mouth
prevents proper brushing.
Special skin features = telangiectasia + salt & pepper pigmentation
+ calcinosis
Mention mechanism of poor oral hygiene and loss of teeth in SSC.
Mechanism = Fibrosis causes gingival atrophy (teeth lost from
sockets) + Small mouth
prevents proper brushing.

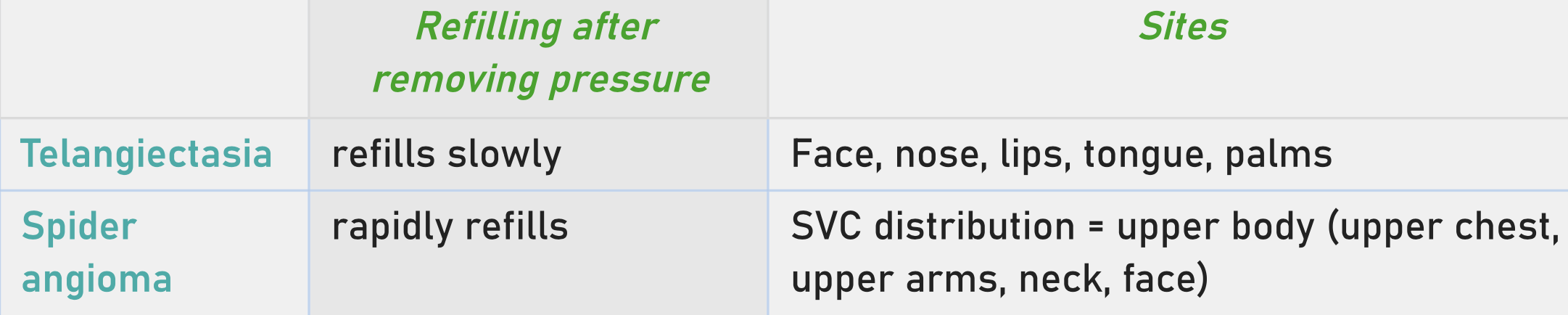
Telangiectasia
Mention appearance, technique, characteristics, and mechanism of telangiectasia.
Appearance = Red spots (visible vessels).
Technique = Must apply pressure to differentiate.
Characteristics:
1. Blanches on pressure = Differentiates from Petechiae/Purpura
(which do not
blanch/are bleeding).
2. Slow refill = Differentiates from Spider Angioma (rapid refill).
Mechanism = Abnormal new angiogenesis due to ischemia/fibrosis + Not
normal
capillaries.
Contrast: Spider Angioma = Dilated normal vessels due to
hyperestrogenemia (liver
failure) → rapid refill.
Mention sites of spider angioma and telangiectasia.
How to differentiate between salt and pepper pigmentation in SSC versus vitiligo?

Mention complications of Calcinosis.
cellulitis + compression on nerves, muscles, joints
Mention findings in SSC hand examination.
Skin Appearance = Shiny waxy skin (due to tightness/loss of matte
texture).
Skin Palpation = Tethering (cannot pinch) + Loss of elasticity
(can't stretch).
Special skin features = telangiectasia + salt & pepper pigmentation
+ calcinosis
Appendages = Loss of hair (on dorsum of fingers) + Loss of sweat
(ask patient does she
sweats in the summer).
Temperature = Assess with back of hand.
Raynaud's Phenomenon (Three Phases):
1. Pallor = Vasospasm (White).
2. Cyanosis = Accumulation of carboxyhemoglobin (Blue).
3. Hyperemia = Reperfusion (Red).
Note = Often not visible during exam unless cold/under AC. State:
"Patient is currently
not in Raynaud's."
Posture = Flexion contracture (hands fixed in flexion with no joint
destruction).
Fingertip Ulcers = Active lesions.
Pitting Scars = Healed ulcers (tissue perfusion poor).
Resorption of terminal phalanges = Tips "eaten away" (shortened
fingers).
Sclerodactyly:
Phase 1 = Edematous (puffy fingers).
Phase 2 = Indurated/Established (fibrosis).
Description = "Finger puffiness with sclerodactyly" (Note: It is not
arthritis/joint
swelling).
Advanced signs:
Tendon Rub = Palpate while patient moves joints.
Finding = Coarse crepitus (like sandpaper rubbing).
Joint Swelling = Usually absent (No synovitis, wrists/MCPs/PIPs not
swollen).
Palms = Palmar Erythema + Thin atrophic skin (tendons visible).
Palmar erythema:
Erythema in thenar & hypothenar muscles with pallor in the center of
the palm
Can be seen in liver disease + oral contraceptive pills + pregnancy
+ hyperthyroidism.
When does Contracture of fingers with destroyed joints in Scc occur?
Occurs in case of overlap with RA or OA or PsA or Septic arthritis

Discoid rash = chronic cutaneous manifestation + hyperpigmented
rim with lighter atrophic
center + can be seen in face, scalp, ears (specifically).

Urticarial rash = can be anywhere

Periungual erythema = inflammation & redness around the nail bed.

Livedo reticularis = A net-like, purple/mottled pattern on the skin,
usually on the legs
or arms. It suggests sluggish blood flow and is strongly linked to
Antiphospholipid
Syndrome.
Mention different SLE skin changes.
1. Malar rash = acute cutaneous manifestation + spares nasolabial
fold (because of nose
shadow) + increase by UV exposure.
malar rash
2. Discoid rash = chronic cutaneous manifestation + hyperpigmented
rim with lighter atrophic
center + can be seen in face, scalp, ears (specifically).
3. Photosensitive rash = acute cutaneous manifestation + look at sun
exposed regions as arms, V sign in the neck, dorsum of the hand.
4. Raynaud's = look for the 3 different colors (pale → cyanosis → redness)
5. Urticarial rash = can be anywhere
6. Periungual erythema = inflammation & redness around the nail bed.
7. Vasculitis:
Nail fold infarcts = Tiny black or brown dots in the nail fold or cuticle. These are small
areas of tissue death.
Palpable purpura = Non-blanching red/purple spots, usually on the
lower legs. "Palpable" means you can feel them raised above the skin surface
(unlike the flat petechiae of thrombocytopenia).
Digital ulcers = Open sores or crusts, typically on the fingertips, due to lack of blood flow.
Splinter hemorrhages = Vertical red/brown lines under the fingernails (looks like a
wood splinter).
Livedo reticularis = A net-like, purple/mottled pattern on the skin, usually on the legs or arms. It suggests sluggish blood flow and is strongly linked to Antiphospholipid Syndrome.
8. Oral & nasal ulcers = usually painless.

Non-scarring alopecia
Scarring alopecia
Compare between scarring and non scarring alopecia in SLE.
Diffuse Alopecia (Non-Scarring):
Appearance = General thinning of the hair. This reflects active systemic disease (a flare).
Lupus Hair = Look at the frontal hairline for short, broken, "frizzy" hairs.
These are fragile hairs that snap off easily.
Prognosis = It grows back when the disease is controlled.
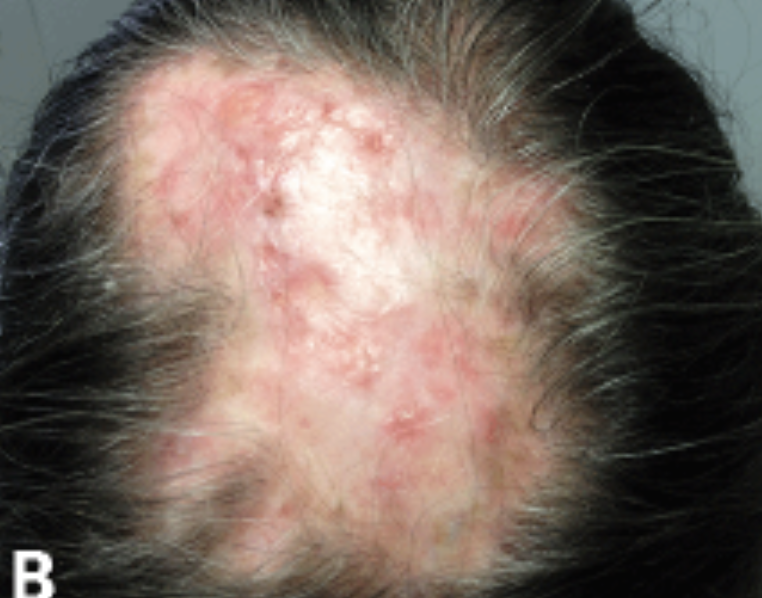
Discoid Alopecia (Scarring):
Appearance = Hair loss caused by a Discoid (DLE) plaque on the scalp.
Examination = Look for round, smooth, shiny white patches on the scalp with loss of follicular openings.
Prognosis = This hair loss is permanent.
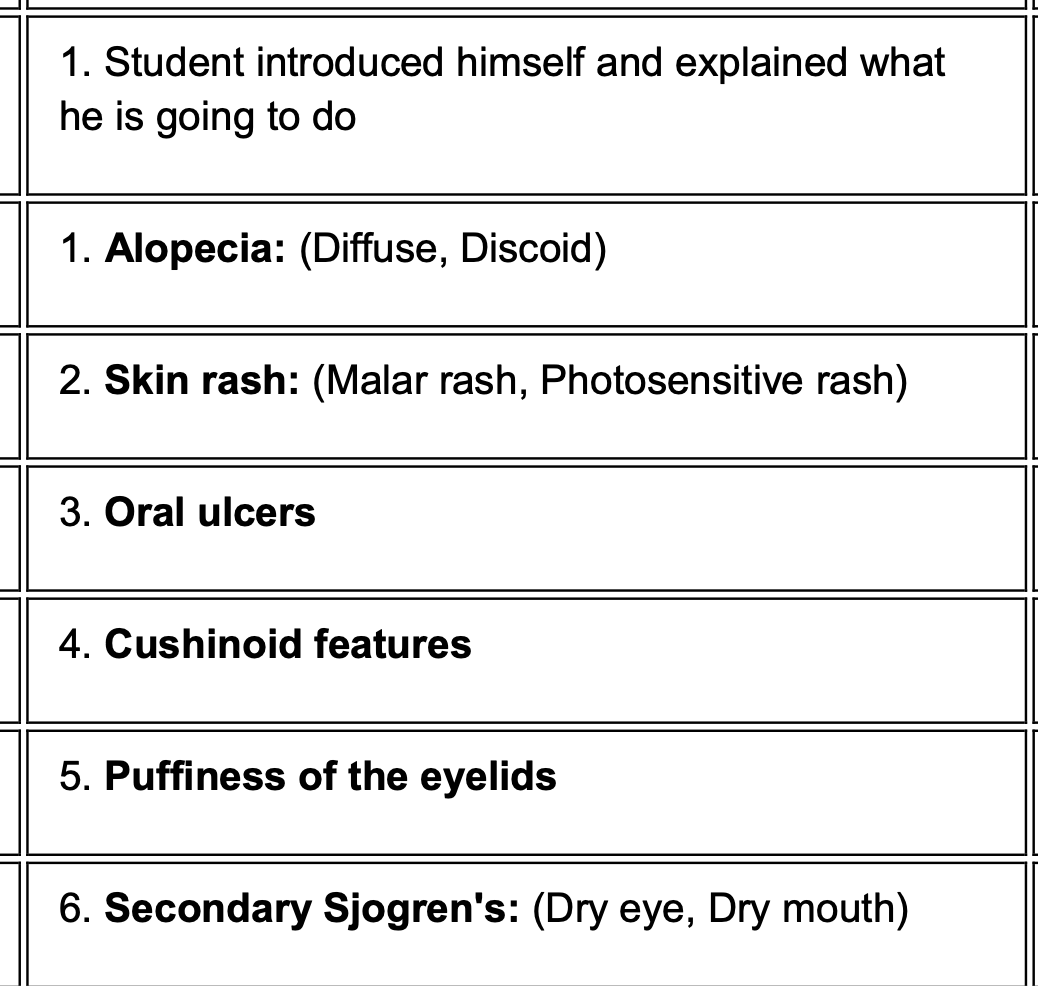
SLE head examination
Scarring alopecia and Diffuse Alopecia (Non-Scarring):
2. Skin Rash (Malar & Photosensitive)
Malar: Cheeks and nose. Photosensitive: Don't forget to look behind the ears and at the "V" of the neck (common
missed spots in head exams).
3. Oral Ulcers
Examination = Use a tongue depressor and light. You must look at the hard palate (roof of
the mouth). Key Feature = SLE ulcers are typically painless (unlike the painful aphthous ulcers of Behçet's or stress). They often look like red patches or shallow erosions on the palate.
4. Cushinoid Features
Cause = sign of Chronic Steroid Therapy (Prednisolone) as most SLE
patients are on
steroids.
Moon Face = Is the face round and plethoric (red)?
Buffalo Hump = A fat pad at the base of the neck (check this when
looking at the back
of the head/neck).
Hirsutism = Excess hair growth on the chin/upper lip.
Steroid Acne = Pustules on the face or chest.
5. Puffiness of the Eyelids
Cause = This is usually a sign of Lupus Nephritis (Nephrotic syndrome).
Examination = Look for edema (swelling) around the eyes, especially
if the patient mentions it's worse in the morning.
6. Secondary Sjögren's Syndrome
Cause = About 30% of SLE patients have secondary Sjögren's.
Dry Eye (Keratoconjunctivitis Sicca):
Ask if eyes feel "gritty" or like there is sand in them.
Look for redness (conjunctival injection).
Dry Mouth (Xerostomia):
Dental Caries = Dry mouth leads to rapid tooth decay near the gum
line.
Parotid Enlargement = Check the angle of the jaw for swelling of the
parotid gland
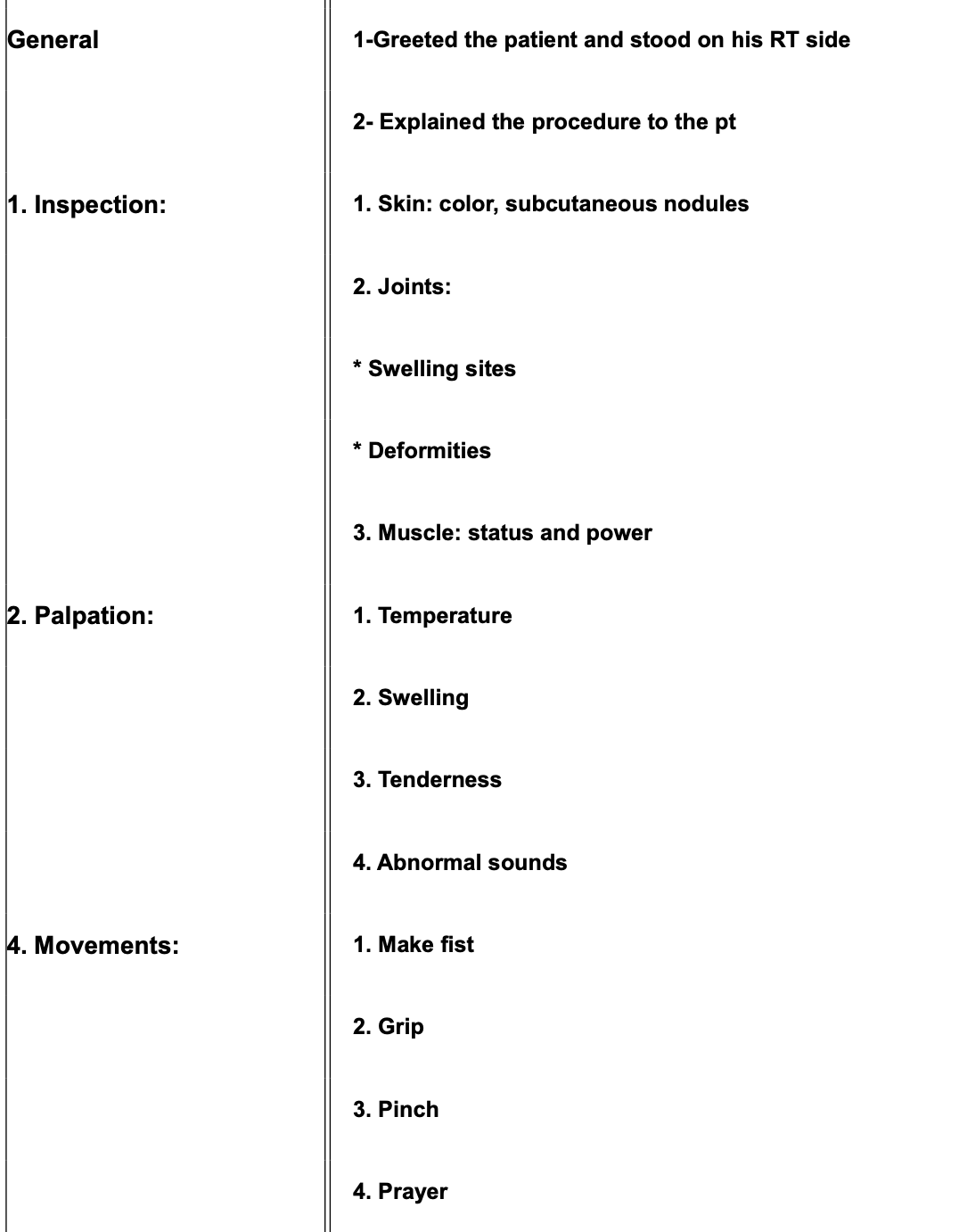
Mention inspection of Rh hand.
Skin:
1. Rash
2. Redness
3. Scar
4. Palmar erythema
5. Thin atrophic skin on dorsum of the hand
6. Nail = may contain nail pitting or psoriasis.
Subcutaneous tissue:
1. Rheumatoid nodules = well circumscribed + firm + around joint line (never on joint line) + usually on extensor surface
Muscle wasting:
1. Thenar & hypothenar wasting
2. Interossei wasting (guttering sign)
Joint:
1. Swelling:
MCPs = Ask patient to make a fist to count number of swellings on MCPs + trigger
finger can occur while patient trying to open his hand due to
tenosynovitis (loss of
lubrication in flexor tendons making them get stuck).
Interphalangeal joints = fusiform swellings (PIPs swollen) sparing DIPs.
Wrist = Boggy Synovium.
Causes of DIPs affection in RA:
1. Gout
2. OA
3. Psoriatic arthritis
4. Trauma
2. Bone (deformities):
Swan Neck Deformity = flexed DIP + extended PIP.
Boutonniere = extended DIP + flexed PIP
Z-shaped Thumb = flexed MCP + extended interphalangeal joint.
Zig-zag hand = wrist going to radial side + MCPs going to ulnar
side.
Caput Ulnae = Prominent ulnar head due to laxity of wrist ligaments.
Heerden's & Boucher's nodules = due to secondary OA + boucher's in
PIPs & Heerden's
in DIPs.
Caput ulna is the same as piano key sign in palpation
Mention causes of DIPs affection in RA:
Causes of DIPs affection in RA:
1. Gout
2. OA
3. Psoriatic arthritis
4. Trauma
Mention palpation items of rh hand.
Temp:
Technique = Back of hand, compare to forearm.
Finding = Warmth (inflammation) or Cold.
Crepitus:
Technique = Hand on joint, ask patient to open/close.
Finding = Fine Crepitus (creaking/grating).
Tenderness and swelling;
A. Wrist:
Technique = Bimanual.
8 fingers under the palm + 2 thumbs on dorsum.
Character of Swelling:
Soft = Cystic (Effusion).
Doughy = Marshmallow-like (Synovitis/Boggy Synovium).
Hard = Bone deformity.
B. Carpals and Carpo metacarpals
Technique = Squeeze Test.
Compress the row of joints.
Finding = Tenderness only (cannot assess swelling deep).
C. Metacarpophalangeal Joints:
Technique 1: Squeeze Test (across knuckles) → Tenderness.
Technique 2: Bimanual (Assessment of Joint Line).
Crucial Step = Flex fingers 30 degrees.
Why? = Joint line is closed in extension; groove appears in flexion.
Technique 3: Bi-digital (Four-Point Technique).
Thumbs and Index fingers
Hold sides + Push top/buttom ( check for effusion pulge )
D. PIPs and DIPs
Bi-digital ( four point technique )
Two fingers behind, two in front → slide to feel swelling
Mention items of movement, functional tests ( power ) and nerve tests.
Movement ( Range of Motion )
A. wrist:
Flexion test = Reverse Pryer position
Normal = 90 degrees ( forearm horizontals, wrists touching )
Abnormal ( problem in flexion ) Gap between wrists
Extension test: prayer test
Normal 90 degrees
B. Fingers:
Flexion = make a fist
check = are nails visible? if yes incomplete flexion
Thumb flexion: Thumb flexes across palm ( axis perpendicular to fingers )
Opposition = Tasbeeh (Count prayer beads )
Touch thumb to tip of every finger
C. Trigger finger
Observe for locking/catching upon straightening fingers
Functional Tests (Power )
Grip Strength = "Squeeze my fingers and don't let me slip it out."
Test Ulnar and Radial sides separately.
Observation = Ability to hold vs. slips easily.
Pinch Strength:
Patient makes ring (Index+Thumb), Doctor makes ring.
Instruction = "Don't let me break it."
Adduction/Abduction = Paper Test.
Place paper between extended fingers.
Instruction = "Don't let it slip."
Nerve Tests ( Carpel Tunnel Syndrome )
Tests for synovitis in Flexor Retinaculum compressing Median Nerve.
1. Tinel's Test
Technique = Repeated tapping on flexor retinaculum.
Positive = Tingling/Numbness in lateral 3.5 fingers.
2. Phalen's Test
Technique = Reverse Prayer Position (maintained for 30-60 seconds).
Mechanism = Compresses Median nerve.
Positive = Tingling/Numbness in lateral 3.5 fingers.
Anatomy = Palm sensation is spared (cutaneous branch arises before
tunnel); fingers affected.
3. Piano Key Sign
Target = Ulnar Styloid Process (Caput Ulnae).
Technique = Press down on styloid.
Positive = Moves down and pops up (instability) + Tenderness.
Mention knee inspection items.
Skin = Redness, Rash, Scars.
Muscle = Quadriceps Wasting.
Sign = Flattening or gutter formation above the knee (loss of bumpy
surface).
Joint Swelling = Unilateral vs. Bilateral (symmetrical?).
Bone Deformity (Must be done Standing)
Genu Valgum = Knock-knees ("Gum" = knees stuck together).
Genu Varum = Bow-legged ("Rum" = bottle of rum between legs).
Popliteal Fossa (Patient Turn Around)
Look for = Smooth swelling (Baker's Cyst).
Ruptured Baker's Cyst:
Mimics = DVT (Acute redness, swelling, calf pain).
Differentiation = Doppler Ultrasound (Veins patent = Cyst; Thrombus
= DVT).
Mention palpation items of knee.
Temp
Back of hand, compare knee to distal thigh.
Technique = Hand on knee, passive flexion/extension.
Crepitus
Type = Grinding Crepitus (Coarse) vs. Fine.Tenderness and swelling
Position = Knee flexed 30 degrees.
Landmarks for Palpation:
1. Joint Line = Around the patella (sides).
2. Quadriceps Tendon = Above patella.
3. Patellar tendon = below patellaCharacter of Swelling: Cystic = Effusion (Fluid). Doughy = Synovitis. Bony = Osteophytes.
Mention movement ( range of motion ) for knee.
Flexion
Normal Limit = Heel touches the buttocks.
Abnormal = Distance between heel and buttock indicates limitation.
Extension
Normal Limit = Knee is flat on the bed + Cannot insinuate hand
beneath the knee.
Abnormal (Flexion Deformity) = Gap exists between knee and bed (hand
passes
through).
Active Movement: Patient moves leg.
Passive Movement: Doctor moves leg.
Interpretation:
Limited Active + Improved Passive = Peri-articular issue or Pain.
Limited Active + Limited Passive = Articular pathology or Fixed
Deformity.
Mention Tests for effusion.
Tests for effusion: Different tests are used depending on the volume of fluid suspected.
1. Bulge Test (Swipe Test)
Indication = Mild to Moderate effusion.
Concept = Displace water from one compartment to another.
Technique:
1. Empty the Suprapatellar pouch = Milk fluid downwards from thigh
to knee.
2. Medial Upstrokes = Push fluid from medial side upwards to empty
the medial
compartment.
3. Lateral Push = Push on the lateral side of the patella.
Positive Result = A bulge/ripple of fluid appears on the medial
side.
2. Patellar Tap
Indication = Severe/Large effusion.
Concept = The patella is "floating" on a large volume of water.
Technique:
1. Suprapatellar Milking = Push down from thigh with one hand to
collect fluid under the
patella.
2. Tap = With two fingers, push the patella down.
Positive Result = Patella goes down, hits the femoral condyle, and
bounces back up ("Tap
positive").
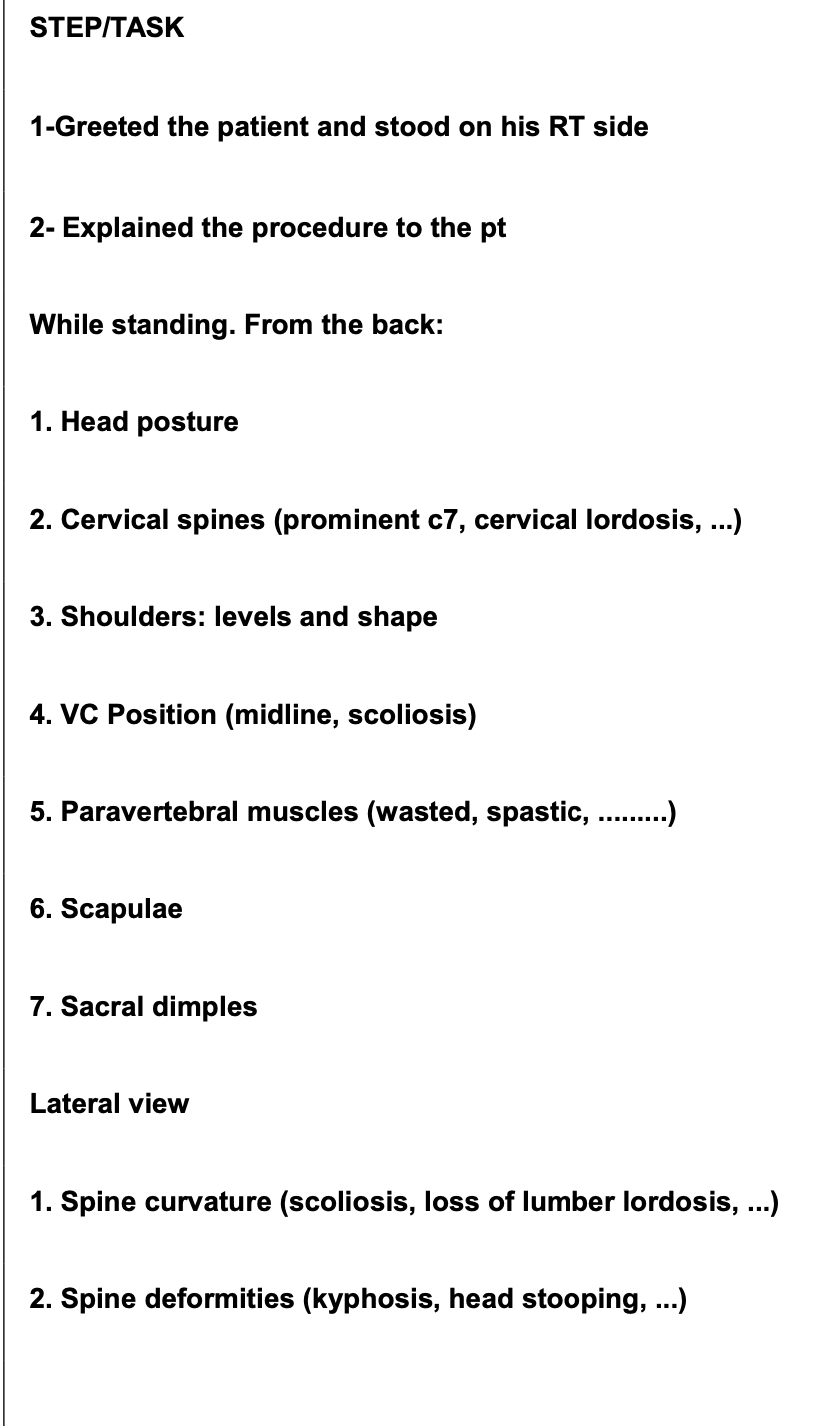
Mention inspection items of the back.
1. Skin (Psoriasis Check)
Must expose the whole back (front and back).
Relevance = Seronegative Spondyloarthropathies are a spectrum
(Psoriatic Arthritis
overlaps with AS).
Lesion Type = Psoriasis.
Appearance = Reddish plaques (raised) + Silver scales.
Location = Extensor surfaces (Elbows, Knees, Scalp, Dorsum of hands,
Buttocks).
2. Head & Neck Posture
Finding = Central Stooping (Head flexed forward).
3. Spinal Curvatures
Cervical Lordosis = Lost/Flat (Neck appears straight).
Thoracic Kyphosis = Exaggerated (Hunchback).
Lumbar Lordosis = Lost/Flat.
Scoliosis = Check for lateral curvature (uneven shoulder/nipple/rib
levels).
4. Muscle Status
Normal = Bulky (spine is in a groove).
Pathology (AS) = Atrophy/Wasting.
Result = Spine becomes prominent + Muscles form a gutter (went
inwards).
Causes of Wasting = Disuse + Inflammatory cytokines (cachexia).
Trapezius:
Finding = Trapezius Atrophy.
Appearance = Square shoulders (Loss of normal round contour around
the neck).
Landmarks:
Sacral Dimples of Venus = Normal landmark.
Significance = Guide to the Posterior Superior Iliac Spine (PSIS).
Sacroiliac Joint (SIJ) Location = 2.5 cm below and medial to the
sacral dimple.
Inspection (Side & Front Views)
igzag Posture (Late Stage):
Head flexed forward.
Exaggerated thoracic kyphosis.
Protruded abdomen (to adjust center of gravity).
Flexed Hips + Flexed Knees.
Chest:
Finding = Intercostal Muscle Atrophy.
Mechanism = Restrictive Lung Pattern.
Thoracic vertebrae/ribs stiffen → Chest expansion limited.
Accessory muscles (intercostals) atrophy due to disuse.
Clinical Correlation = Apical lung fibrosis may occur.
Mention segmental spine examination.
Cervical Spine:
Palpation:
Target = Spinous Processes.
Technique = Press thumb on each process (C2 to C7).
Finding = Tenderness (Enthesitis of ligaments).
Landmarks = C1 is not palpable. C2 is first palpable. C7 is most
prominent (vertebra
prominens).
Cervical (4 Movements)
1. Flexion = Chin to chest.
2. Extension = Neck back, forehead parallel to ceiling.
3. Lateral Bending = Ear to shoulder.
4. Lateral Rotation = Chin to shoulder.
fixate patient's shoulders while testing range of motion
Thoracic Spine:
Inspection = Exaggerated kyphosis + Paravertebral atrophy.
Palpation = Tenderness on spinous processes.
Movement (Rotation):
Technique = Patient seated (to eliminate lumbar/pelvic rotation).
Action = Patient crosses arms and rotates trunk.
Special Test: Chest Expansion:
Most Important Thoracic Test.
Level = Nipple line (Males) / Below breast (Females).
Method = Measure circumference at deep expiration vs. deep
inspiration.
Normal = > 5 cm.
Abnormal = < 2.5 cm (Severe restriction).
Lumbar Spine
Inspection = Loss of lordosis.
Palpation = Tenderness.
Mention special tests for lumbar spine motility.
Finger to Floor Test:
Assesses = Global spinal flexion + Hip flexion.
Technique = Patient stands neutral, knees extended, bends forward to
touch floor.
Measurement = Distance between tip of middle finger and floor.
Result = Greater distance = Worse limitation.
Normal = < 10 cm (debatable).
Limitations = Influenced by hamstring wasting, abdominal obesity,
etc.
Utility = Used for Follow Up (every 6 months).
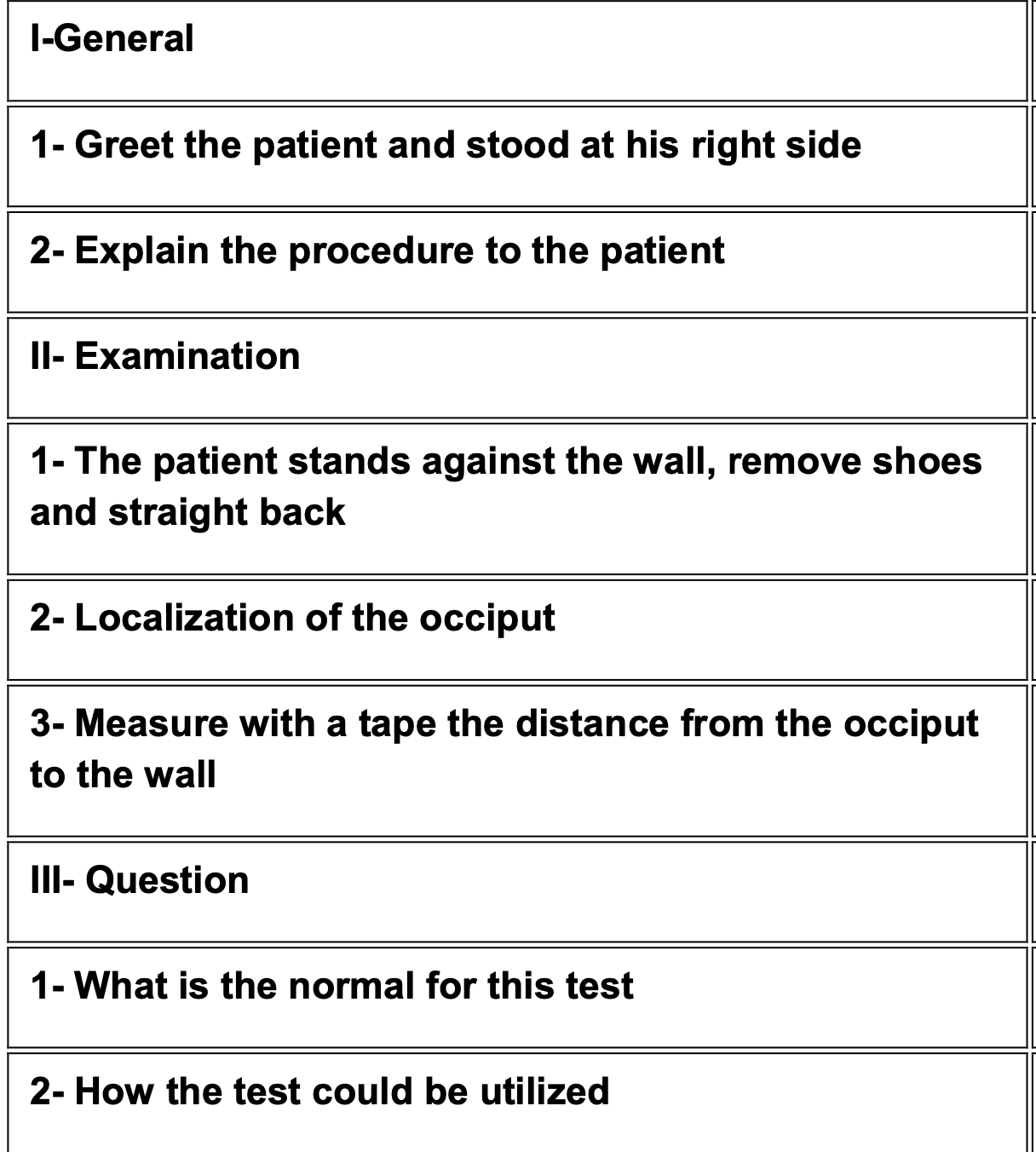
Occiput to Wall Test:
Assesses = Cervical/Thoracic deformity (kyphosis).
Technique = Patient stands in neutral position with Heels + Buttocks
+ Shoulders touching
the wall + Looks straight ahead + not wearing shoes.
Measurement = Distance from Occiput to Wall.
Normal = Zero cm + 0-3 cm in obese patients.
Importance = Excellent for follow-up (monitoring progression over
months).
C. Tragus to Wall Test
Assesses = Forward head posture.
Technique = Same stance as above. Measure Tragus (ear cartilage) to wall.
Normal = < 15 cm.
Shober Test:
Landmarks = Identify Sacral Dimples OR Posterior Superior Iliac
Spines (PSIS).
Setup:
1. Draw imaginary line between dimples/PSIS.
2. Mark a Midline point on this line.
3. Measure 10 cm ABOVE this point and mark it.
Action = Patient performs Hyper-flexion.
Concept = Skin stretches over lumbar spine.
Normal Result = Distance increases by > 5 cm (Total > 15 cm).
E. Modified Schober's Test (Flexion)
Assesses = Lumbar Flexion exclusively (eliminates hip movement).
Technique:
1. Mark L5/S1 (Dimples of Venus line).
2. Mark 10 cm above this point.
3. Patient bends forward (max flexion).
4. Measure the distance between marks again.
Normal = Increases from 10 cm →15 cm (Difference > 5 cm).
Positive = < 5 cm increase.
Lateral Shober Test:
Technique:
1. Mark midline at Mid-axillary line.
2. Mark 20 cm above it.
3. Patient bends laterally to the opposite side.
Normal = Increases from 20 cm →25 cm.
Positive = Does not reach 25 cm.
For a positive SIJ test, the patient must report pain in the …
If pain is in the groin/thigh = …
For a positive SIJ test, the patient must report pain in the Lower
Back/Gluteal area
(Posterior).
If pain is in the groin/thigh = Hip joint pathology.
Mention sacroiliac joint tests.
1. Direct & Fist Percussion
Technique = Press on SIJ (dimples) with Thumb OR strike with Fist.
Positive = Pain in SIJ.
2. Pelvic Compression
Position = Supine or Lateral.
Technique = Compress the iliac crests towards each other.
Result = Compresses the SIJ.
Pelvic Distraction
Position = Supine. Technique = Push iliac crests apart/outward. Result = Stretches/opens the SIJ anteriorly.Patrick's Test (FABER)
Cross leg (ankle on opposite knee).
Stabilize opposite ASIS (pelvis) + Push down on the bent knee.
Mechanism = Opens the pelvis ("Opening a book") stressing the SIJ.Positive = Pain in the Lower Back. (Thigh pain = Hip issue).
Gaenslen's Test
Patient lies on the edge of the bed.
Hip Extension (Test Leg) = Outer leg dangles off the bed
(hyperextended).
Hip Flexion (Non-test Leg) = Inner leg flexed toward chest by
patient.
Mechanism = Torsion stress on SIJ (One innominate bone rotates
anteriorly, one
posteriorly).
Positive = Pain in the SIJ of the extended leg.Modified Gaenslen's
Indication = Patients with severe kyphosis who cannot lie flat/
supine comfortably.
Technique:
Patient lies on their side.
Bottom leg (on bed) is flexed to chest.
Top leg is hyperextended backwards by the doctor.Pump Handle Test
Indication = Patients with severe kyphosis who cannot lie flat/
supine comfortably.
Technique:
Patient lies on their side.
Bottom leg (on bed) is flexed to chest.
Top leg is hyperextended backwards by the doctor.Gillis Test
Indication = Patient has Kyphosis (cannot lie supine). Position = Prone (on stomach).Technique = Stabilize buttock + Lift leg into extension from the
other side.
Mention checklist of skin changes in SLE.

Examine Head checklist in SLE.
Examine sacroiliac joint in SLE.

Mention occiput to wall test checklist.
Mention checklist inspect back.
Examine Lumbar Spine Checklist.

Examine SSC hand checklist.

Examine SSC face checklist.
Mention RA hand examination checklist.
Mention knee examination checklist.
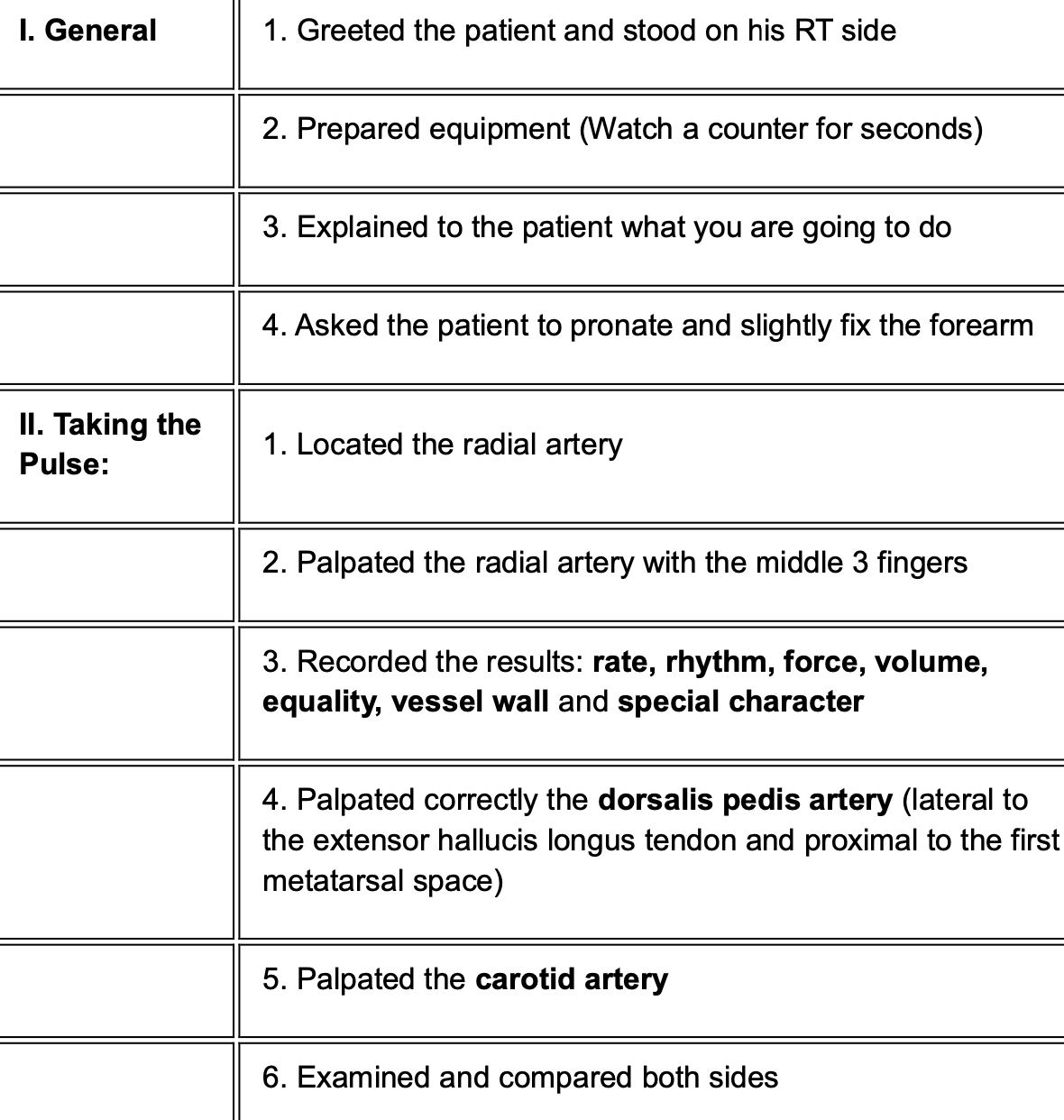
Pulse comment checklist.