After Midterm 2 Content
1/121
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
122 Terms
Obesity/Overweight Definitions (3)
Body weight above a defined standard relative to height.
Abnormally high % body fat which increases risk of health problems & mortality.
A negative social label.
(Current standards - normal = 18.5-25 BMI)
Association between BMI and all-cause mortality
Correlation between BMI and all causes mortality. Also a risk of heart disease, (dyslipidemia and HTN).
Other evidence suggests fitness and WC as better predictors of mortality.
What disease risks are increased with obesity and how much?
Greatly increased risk - more than 3 times non-obese
Type 2 diabetes, gallbladder disease, dyslipidemia, insulin resistance, breathlessness, sleep apnea.
Moderately increased risk - 2-3 times non obese
Coronary heart disease, hypertension, osteoarthritis, gout.
Slightly Increased Risk - 1-2 times non obese
Breast, endometrial, and colon cancer, reproductive hormone problems, pcos, impaired fertility, low back pain, fetal defects due to maternal obesity.
Waist to height ratio
A person’s weight to height ratio is a good way to measure the distribution of body fat. Higher values indicate higher risk of obesity related CVD. (Values >0.5).
BDNF
Brain derived neurotrophic factor. Regulates appetite. Dysfunction stops it from working.
Epigenetics
The study of heritable and stable alterations in gene expression potential that are not caused by changes in DNA sequence.
Fitness vs Fatness Studies
Puts people into categories based on their BMI, and VO2 (CV fitness).
Categories are normal weight fit (baseline), NW unfit, OW fit, OW unfit, OB fit, OB unfit.
RESULTS:
NW unfit has higher risk of mortality than NW fit.
NW unfit had a higher risk of mortality compared to OW fit.
OB fit has slightly better odds than OB unfit.
***Basically fitness is also a major predictor of mortality, not just weight.
7 Theories of Over-Nutrition
Genetic Theory (many genes involved in the regulation of food intake and body weight).
Lipostatic Theory (higher set point).
Thermogenetic theory (obese people have fewer brown fat cells).
Diabetes Associated Theory (excess food leads to hyperinsulinemia, hypertrophy, etc).
Psychological Causation Theory (obese individuals are vulnerable to external cues to eat).
Thermostatic Theory (A decrease in body temp below a given set point to stimulate appetite).
Sleep Deprivation Theory (Short sleep associated with high body weight).
Brown vs white fat cells.
Brown - Energy expenditure to be burned.
White - Storage.
Obese person would have a lot of white, little brown.
Genetic Theory of Over-Nutrition
Many genes are involved in the regulation of food intake and body weight - they are affected in obese individuals.
Lipostatic Theory of Over-Nutrition
Obese have a higher hypothalamic set point, difficult to maintain weight loss.
Thermogenetic Theory of Over-Nutrition
Obese have fewer brown fat cells and cannot burn off excess energy.
Body weight set point
A combination of hormonal signals, neural signals, and hypothalamic expressions to regulate body weight and maintain at defined set point.
When signals reflecting BW are higher than set point, feeding behaviour is inhibited.
When signals reflecting BW are lower than set point, feeding behaviour is initiated.
Impact of constant weight loss/gain on set point
When you loose and regain weight you get a new, higher set point. Yo-yoing is bad.
Diabetes associated theory of over-nutrition
Excess food leads to high blood glucose levels, hyperinsulinemia, and thus enhanced hypertrohpy and hyperplasia of fat cells.
Psychological causation theory of over-nutrition
Obese individuals are vulnerable to external cues to eat.
Thermostatic theory of over-nutrition
A decrease in body temperature below a given set point tends to stimulate appetite.
Sleep deprivation theory of over-nutrition
Short sleep is associated with higher body weight.
Energy equation balanced equation
E in - E out = change in body weight
Long term control is more precise than short term regulation.
Structural + Functional physiology of energy balance
Brain areas of control.
Organs.
Autonomic NS
Sympathetic NS - Overall decreases food intake.
Parasympathetic NS - Increases food intake (vagal nerve).
GI nutrients, hormones, and peptides.
Autonomic NS impact on appetite
Sympathetic NS - Overall decreases food intake.
Parasympathetic NS - Increases food intake (vagal nerve).
Arcuate Nucleus
Sits at the base of the hypothalamus and is a major controller of energy expenditure and energy consumption.
Ghrelin
Site of secretion: X/A like cells in the gastric fundus.
Effect on energy metabolism: Increased food intake, decreased energy expenditure.
Insulin
Site of secretion: Pancreatic b cells.
Effect on energy metabolism: Decreased food intake.
Amylin
Site of secretion: Pancreatic b cells.
Effect on energy metabolism: Decreased food intake.
CCK
Site of secretion: I cells of the small intestine.
Effect on energy metabolism: Decreased food intake.
PYY
Site of secretion: I cells of the small intestine.
Effect on energy metabolism: Decreased food intake.
Glucagon
Site of secretion: Pancreatic a cells.
Effect on energy metabolism: Decreased food intake, increased energy expenditure.
GLP-1
Site of secretion: L cells of small intestine.
Effect on energy metabolism: Decreased food intake.
Orexigeneic vs Anorexigenic
Orexigenic - Hormones that increase appetite.
Anorexigenic - Hormones that decrease appetite.
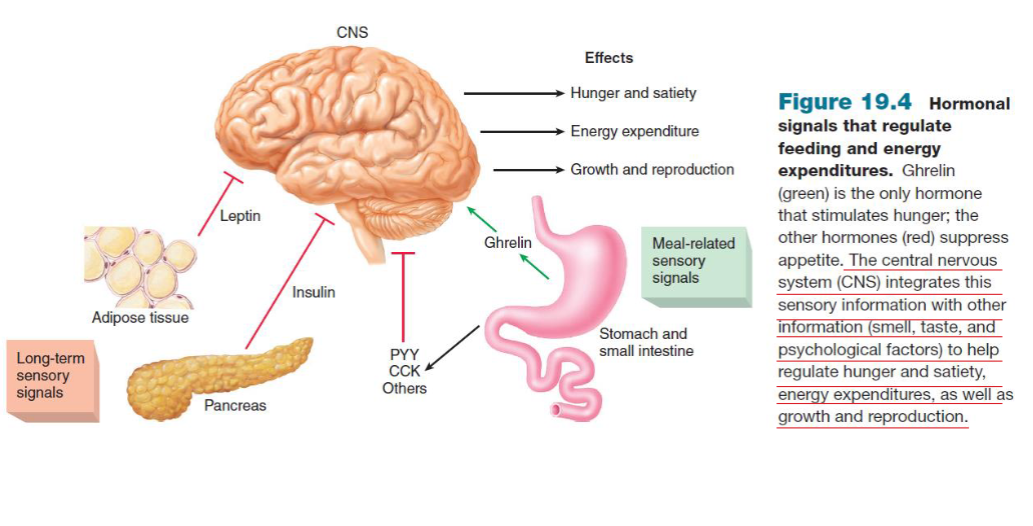
Hormone pathway when stomach is full/empty (short term/long term)
SHORT TERM
Stomach is empty: Ghrelin increases, signals to brain to increase appetite.
Stomach is full: PYY, CCK, and other increases, signals to brain to decrease appetite.
LONG TERM
When fat storage is high: leptin and insulin increases, signals to brain to decrease appetite.
What are the two types of primary neurons in the arcuate nucleus that produce different neuropeptides (two pathways)
Neuropeptide Y (NPY), and Agouti-related peptide (AgRP) - Increases food intake.
MSH (released by POMC/CART) - Increases food intake
NPY acronym
Neuropeptide Y
AgRP acronym
Agouti-related peptide
MSH acronym
Alpha melanocyte-stimulating hormone
CART acronym
Cocaine and amphetamine regulated transcript
POMC acronym
Proopiomelanocortin
Explain the NPY/AgRP pathway
NPY/AgRP neuron activates NPY/AgRP expression.
NPY and AgRP are released.
More food intake.
***As a secondary function, AgRP also inhibits a-MSH receptors
***Circulating insulin and leptin inhibit this pathway.
Explain the POMC/CART pathway
POMC/CART neuron activates a-MSH expression.
a-MSH binds to a-MSH receptors.
Less food intake
***Circulating insulin and leptin activate this pathway.
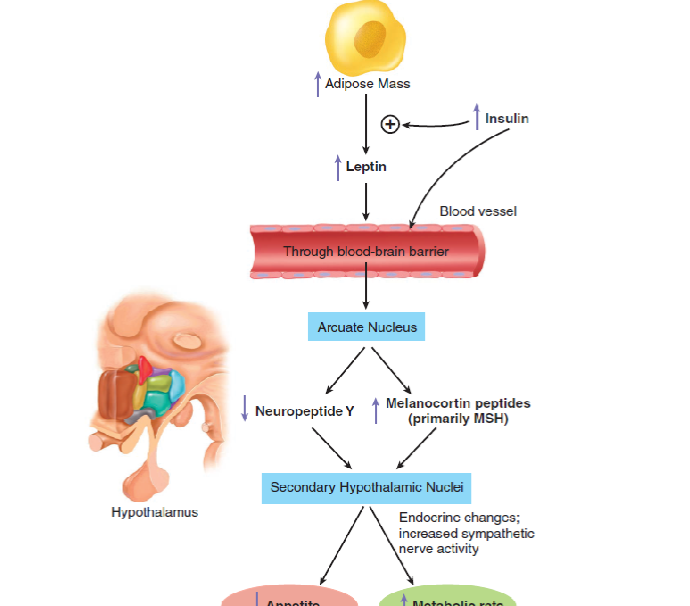
Explain the pathway of how increased adipose mass can decrease appetite through POMC/CART pathway
High adipose mass increases leptin release.
leptin crosses blood brain barrier.
leptin goes into arcuate nucleous.
Leptin suppresses NPY, and activates MSH (POMC/CART pathway).
MSH enters secondary hypothalamic nuclei.
Results in decreased appetite and increased metabolic rate.
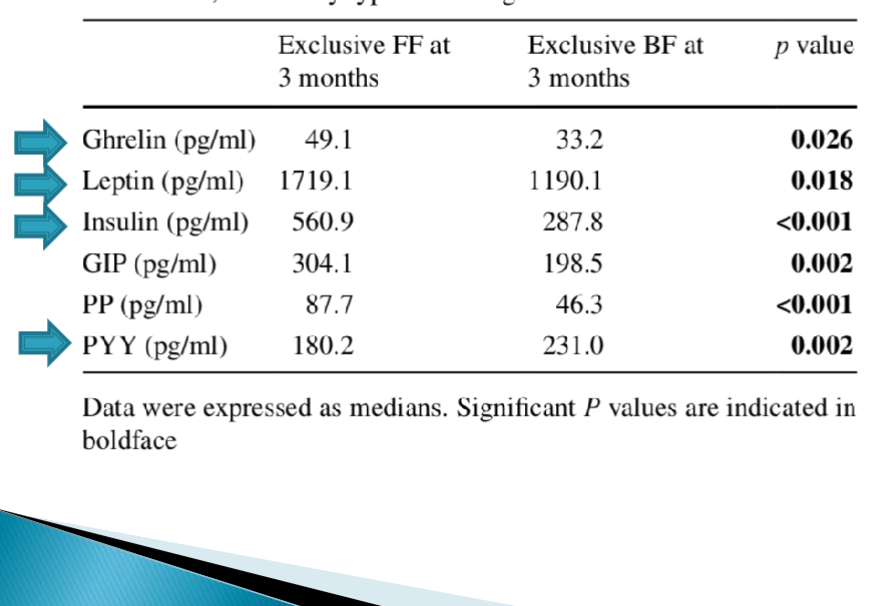
Impact of breastfeeding vs formula on appetite-regulating hormones.
Increased ghrelin, leptin, and insulin, decreased PYY.
Breastfed babies are more satiated.
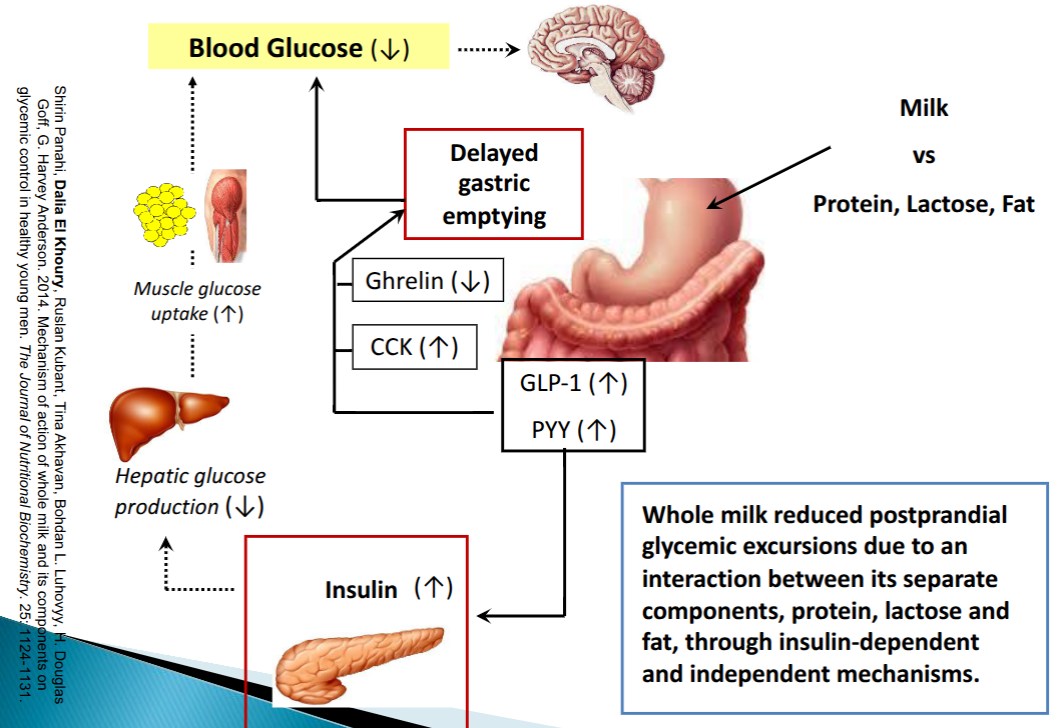
Impact of milk on appetite-regulating hormones.
Post-weight loss surgery vs regular weight loss impacts on appetite regulating hormones.
Hormones tend to bounce back to normal after regular weight loss.
Stay good after surgery.
What are the major predictors of weight loss?
Patient
Process
Treatment
Behaviour changes
What patient factors are predictors of weight loss?
Higher BMI, male, higher RMR, adipocyte hyperplasia, self-efficacy.
What process factors are predictors of weight loss?
Positive: Early weight loss, attendance of counselling sessions.
Negative: Repeated previous dieting attempts, experience of perceived stress.
Treatment predictors of weight loss
Increased length of support, social support.
Behaviour changes predictors of weight loss.
Self monitoring, goal-setting, slowing rate of eating, physical activity.
What are the five main mechanisms of weight regain?
Weight-loss induced changes in energy expenditure (EE).
Neuroendocrine pathways.
Nutrient metabolism.
Gut physiology.
Subjective appetite.
How is weight loss-induced changes in energy expenditure a mechanisms of weight regain?
EE is reduced after weight loss and returns to pre-weight loss level at about 24 months.
How are neuroendocrine pathways a mechanism of weight regain?
After weight loss, ghrelin is increased and satiety hormones are decreased up to a year later.
How is nutrient metabolism a mechanism of weight regain?
Weight regain differs to some extent by diet given. (Larsen et al).
How is gut physiology a mechanism of weight regain?
Delayed gastric emptying is often seen after weight loss, which may delay the release of satiety gut hormones and hence people will eat more.
How is subjective appetite a mechanism of weight regain?
Has biochemical, mechanical, neurological, and psychological basis. Preference for high kcal and reward aspects both increase.
Larsen et al 2010 findings
Took participants who had lost over 8% of BW on an 800 cal per day diet.
Added to 5 subgroups.
High protein, high GI.
Low protein, high GI.
High protein, low GI.
Low protein, low GI.
Control.
High protein, low GI gained the least weight back (no shiz sherlock).
What are the three main RD counselling approaches since the 1970s for weight loss?
Diet/calorie focus.
Counting calories, food records, exchanges, very low calorie diets. Ignored disordered eating.
Foods, exercise, and behaviour modifications.
Use points/exchanges or other counting systems to reduce kcal. Better mix of strategies, still have weight regain.
Healthy lifestyle approach/health at every size.
No focus on weight, promote lifelong habit changes. Improved self esteem, minimal weight loss. Still diet focused, mindful eating.
What are the four steps for nutrition assessment?
Current ABCDE.
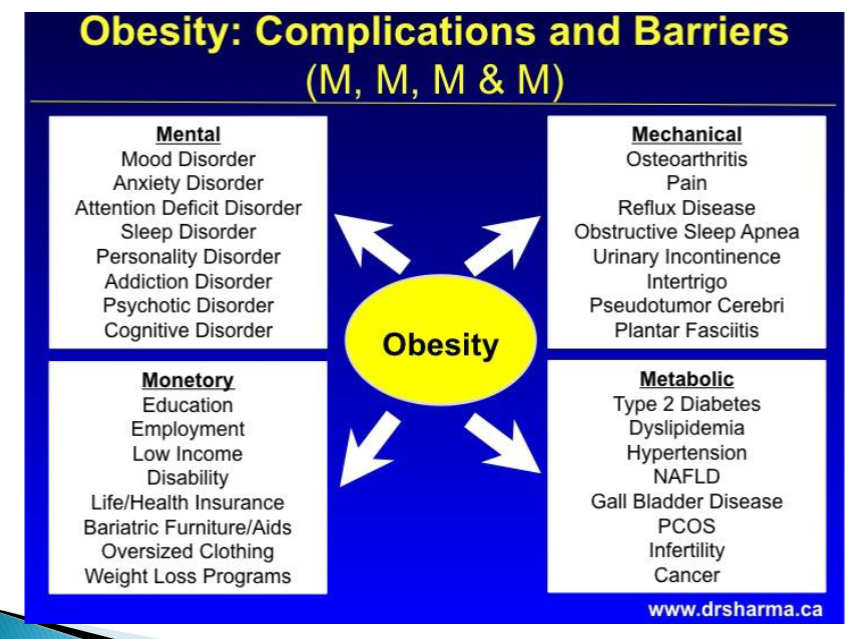
Assess 4 Ms.
Assess knowledge, obesity causes, goals, etc.
Unrealistic goals on weight loss are common, need teaching on current knowledge of diet role and options. Need to teach the importance of PA.
Diets for weight loss are only appropriate for some patients.
4 M’s for obesity barriers/complications.
How are kcal needs calculated for weight loss patients.
Current intake from food records or recall, weight history, food knowledge, portion knowledge, dieting experience, use both DRI and individual data.
How much of a deficit should be given to obese patients?
More deficit = faster weight loss, more hunger, greater decline in EE.
To loose 1 kg, 5000-7000 kcal deficit is needed.
500-1000 kcal deficit per day is practice guidelines, but difficult to manage.
100-200 per day via food is more manageable. (Would take 3.5 months to loose 3 kg).
What are some strategies to reduce the calories in food?
High intensity zero calorie sweetners.
Sugar substitutes, bulking agents.
Increase fibre content.
Reduce energy from fat or use fat replacers.
Olestra
Heat stable, not a fat but acts like one. Not used anymore because it causes major GI distress.
Pancreatic lipase inhibitors for weight loss
Excretes fat in stool.
Must be taken 3x daily.
Diet must have no more than 30% fat.
Most experience diarrhea/fatty stools.
What are orlistat and xenical examples of?
Pancreatic lipase inhibitors.
Metformin for weight loss
Metformin is a diabetes medication.
Decreases hepatic glucose synthesis, increases uptake of glucose in target muscle cells, and decreases glucose absorption in the gut.
GI side effects are common (nausea).
Hypoglycemia is not an issue.
Saxenda
type of GLP-1 receptor agonist
GLP-1 receptor agonists for weight loss.
Daily injectable.
40% have nausea, 20% diarrhea.
Potential risk of thyroid tumors.
Cessation causes you to gain more weight than you had lost.
If you go on it, you have to understand that you will have to pay for it forever.
Nasal PYY
Used nasally.
Adjustable gastric band
Adjustable band is placed on stomach, restricts it.
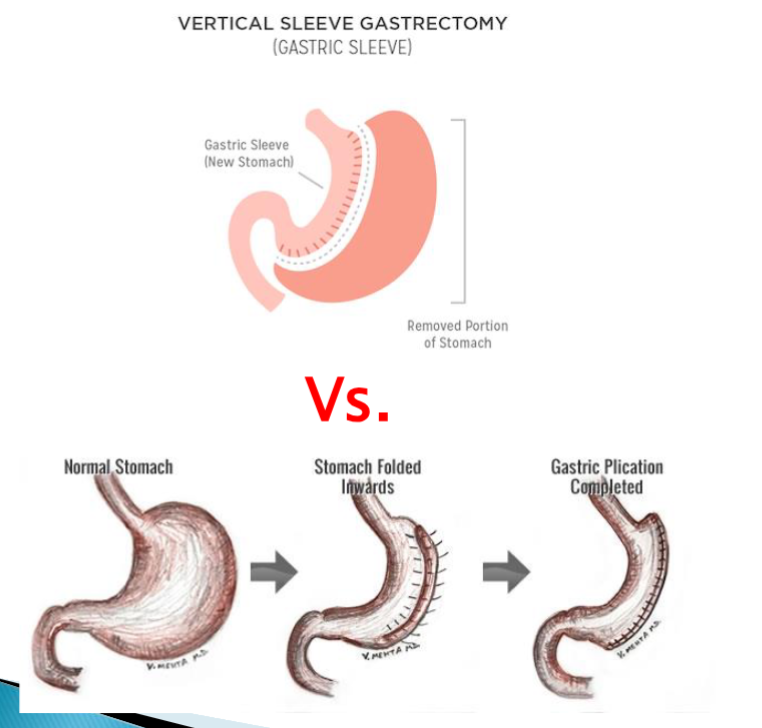
Sleeve gastrectomy
Cuts off a large portion of stomach, leaves behind 15%. Restriction + malabsorbtion.
Roux-en-Y gastric bypass surgery.

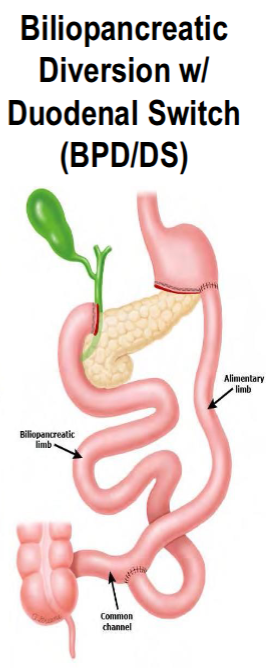
Biliopancreatic diversion with duodenal switch (BPD/DS)
Alternatives to sleeve gastrectomy
Fold stomach so it is reversible.
Nutrition care for bariatric surgery patients.
Pre-surgical assessment
Throughout assessment.
Treat deficiencies.
Pre-operation nutrition education
How is child growth monitored?
WHO Growth Standard - (Birth - 5 yrs).
Shows us how children should grow. No differences globally. Used in Canada because of diverse population.
WHO Growth References - (5-19 yrs).
How were the WHO Growth Standards created?
For birth-5yrs. Based on the multicentre growth references study.
n=8440 children from USA, Norway, Brazil, Ghana, Oman, and India.
Children lived in socioeconomic and environmental conditions favourable to growth (ie. smoke free homes, healthcare, nutrition).
All children were exclusively or predominantly breastfed for first 4-6 months of life, with feeding continuing for at least 12 months.
CDC vs WHO growth charts
WHO developed data from 6 countries, CDC is American.
WHO was longitudinal data (children measured repeatedly over 24 months), CDC was cross sectional.
WHO based off a breastfed population, CDC based on a predominantly non breastfed population.
WHO depicts optimal healthy rate of growth, CDC reported findings of how sample grew regardless of optimal.
WHO Growth References
5-19 years old.
Developed to help address childhood obesity.
Based on 1977 NCHS dataset.
Adjustments were made for smoother transitions between WHO growth standards and WHO growth references. Also makes a smooth transitions from 19 years old to adult BMI cutoffs.
Breastfed vs bottle fed obesity
Breast grows faster in first 6 months and slower in second 6 months.
Gut microbiome = less obesity.
Bioactive factors in breast milk = reduced ghrelin = reduced appetite.
Lower protein content vs infant formula = reduced insulin and IGF 1.
Tips to limit weight gain in children
Adopt family approaches to weight management.
Know portion sizes.
Eat meals and snacks at regular times and don’t skip meals.
Don’t keep high calorie snack foods around the house
Eat at table, not in front of screens.
Keep butter, salt, and margarine off the table.
Ellyn Satter Institute
Promotes healthy feeding habits.
Division of responsibility when feeding (parents vs children)
Parents: what, when, where.
Children: how much, whether.
How to manage/treat obesity in child.
Individual assessment, identify unusual eating patterns, assess growth, kcal needs, and compare to current intake.
Behaviours around family eating.
Goal is to maintain, not lose weight. (support healthy growth).
Qualitative food changes for the whole family.
Focus on reasonable limits on treats and increased activity. (Don’t put kids on diets).
Two main types of child weight management cases in clinical setting.
Lifestyle issues.
Receiving steroid treatment (ie. oncology).
Prednisone and child weight management.
Steroid. Interferes with a child’s ability to tell when they are full.
Side effects:
Increased appetite.
Weight gain.
High blood pressure.
Higher risk of osteoporosis and steroid induced diabetes.
What is malnutrition
Includes both the deficiency and excess (or imbalance) of energy, protein, and other nutrients. Under or overnutrition.
8 Causes of malnutrition
Increased nutrient needs (due to acute/chronic illness, or injury/trauma).
Alteration in GI tract function/structure (malabsorption).
Lack of or limited access to food.
Cultural or religious practices.
Limited environmental resources.
Food insecurity.
Lack of knowledge.
Psychological causes.
Cachexia
Metabolic response to inflammation and stress in the body.
7 Impacts of malnutrition
Low birth rates and infant mortality.
Affects growth and development.
Depressed immune systems (infectious diseases, mainly in undernourished children).
Diseases (due to excessive or unbalanced diet).
Illness or death.
Cachexia (metabolic response to inflammation and stress in the body.
Cycles of malnutrition (populations where undernutrition is a chronic problem).
What are the main impacts of undernutrition
Body tissues.
Functional ability
Overall health.
For hospitalised patients:
Complicated factors that cause inflammation (eg. trauma).
Can be more challenging to treat when the body undergoes extensive physiological changes and increased nutrient needs as appetite is decreased.
Main causes of undernutrition
Immediate causes
Poor diet.
Disease.
Underlying causes
Household food insecurity.
Inadequate care.
Limited access to health services.
Basic causes
Poverty.
War/natural disasters.
How is undernutrition diagnosed?
Identification of two or more of the following:
Insufficient energy intake.
Weight loss.
Loss of muscle mass.
Loss of subcutaneous fat.
Localized or generalised fluid accumulation that may mask weight loss.
Diminished functional status.
7 Potential outcomes of undernutrition
Specific nutrient deficiencies
Iron deficincy anemia.
PEM (Kwashiorkor & Marasmus).
Decrease in productivity.
Stunted growth.
Indicator of chronic undernutrition.
Increased susceptibility to disease.
Immune system compromised.
Sarcopenia
Abnormal loss of muscle mass in older adults.
Maternal undernutrition
Complications during pregnancy.
Poor fetal development.
Decreased body weight
Delayed dexual development.
Increased malnutrition in elderly.
Sarcopenia
Abnormal loss of muscle mass in older adults.
What is considered low body weight for height?
BMI below 18.5
% Usual body weight (UBW)
Non pregnant.
%UBW = (Current BW x 100)/UBW
85-95 - may indicate mild malnutrition.
75-84 - may indicate moderate malnutrition.
<74 - may indicate severe malnutrition.
Failure to thrive
Weight consistently under 2-5th percentile for age and sex.
Progressive decrease in weight to below 3rd to 5th percentile for age and sex.
On multiple occasions in the first 1-2 years of life.
Protein-energy metabolism
A form of malnutrition in which patients are not meeting their protein needs.
Marasmus or Kwashiorkor
Marasmus
Very low intakes of both protein and energy over a long period of time. Appear thin, old, dry nails and hair.
Kwashiorkor
Protein deficiency with sufficient kcal. Edema in feet, abdomen, and face.