Cancer Genetics - Hereditary Breast+Gyn
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
Breast Anatomy
15-20 Lobes per breast
20-40 Lobules per lobe
6-8 Ducts drain lobes to the nipple
Most breast cancers occur in the ducts
Nerves throughout the breast
Lymph Nodes and Blood Vessels: help fight infection
Gynecological System
Vagina: external to Uterus
Cervix: Opening and bottom portion of uterus
Uterus: Endometrial lining
Polyps
Fibroid
Fallopian Tubes
Ovary
Cysts
Non-Modifiable Risk Factors for Breast Cancer
Being female (prevalence 1/8 vs 1/700 men)
Aging
Ethnicity
Black women 4% lower incidence than white women, but 40% higher death rate
Certain breast conditions : (LCIS, atypical hyperplasia)
Hormone exposure: age at mensche/menopause, breast feeding
Fam Hx of cancer
Inherited gene mutations
Modifiable Risk Factors for Breast Cancer
Obesity
Alcohol use
Physical inactivity
Ionizing radiation exposure
Breast Finding: Not Cancer w/ Negligible Increased Cancer Risk
Cyst
Fibroadenoma
Hyperplasia
Papilloma
Calcifications
Radical Scar
Benign Phyllodes tumor
Breast Findings Not Cancer w Increased cancer risk
Lobular Carcinoma in situ (LCIS)
Atypical ductal hyperplasia (ADH)
Atypcial lobular hyperplasia (ALH)
Flat epithelia (FEA)
Breast Finding Cancer
Ducal carcinoma in situ
Invasive carcinoma
Ductal
Lobular
Tubular
Muscions (Colloid)
Medullary
Paget’s Disease
Malignant Phyllodes tumor
Inflammatory breast cancer
Breast Cancer Treatment- Chemotherapy
Anticancer drug used after radiation and surgery
Breast Cancer Treament Radtiaiton
straightforward: ionzing radtion to breast cancer tissue
Breast Cancer Therapy - Hormonal Therapy
Tamoxifen: targets estrogen and/or progesterone receptor positive cancers
Aromatase inhibitors: used in the tretment of breast cancer in postmenopausal women and men by stopping an enzyme in fat tissue (aromastase) from converting hormones into estrogren
Breast Cancer Therapy - Immunotherapy
uses body’s own immune system to help fight cancer
Breast Cancer therapy - PARP Inhibitors
Effective in BRCA1/2 mutation Cancers (Breast, Ovarian, prostate and Pancreatic)
These BRCA1/2 cancer rely heavily on PARP to fix single strand DNA breaks suppressing PARP leads to furthe double strand breaks that BRCA1/2 would normally repair
Lack of BRCA1/2 means double breaks cnnaot be repaired, leading to irrevserible DNA breakdown and cel ldeath
Breast Cancer - Surgical Options
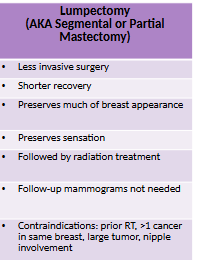
Lumpectomy
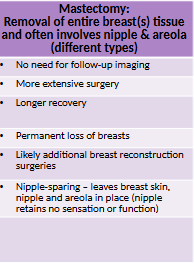
Masectromy / Bilateral Masetcomy
Lumpectomy
removal to trumo from breast plus neoadjuvant radtion
Masectomry
Removal of entire breast tissue and often involves nipple and areola
may include SLNB and ALND
Non-Modifiable Risk Factors for Gynecological Cancer
Again
Being female
chronic conditions (endometriosis, PCOS, diabetes)
Hormonal factors (early menarche, late menopause, nulliparity)
Infertility
Hereditary
Modifiable Risk Factors for Gynecological Cancer
Medications (excess estrogen exposure without adequate opposition by a progestin, tamoxifen)
Obesity
Smoking
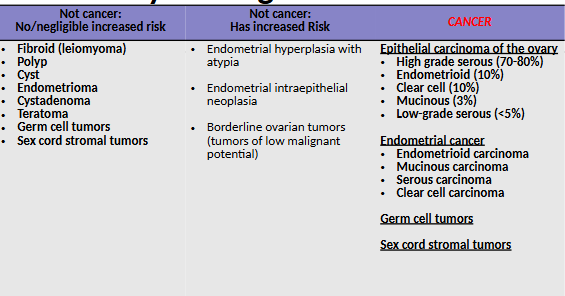
Gynecological Tumors
Screening Tests for Endometrial/Ovarian Cancers
Pelvic exam
Ultrasound/Sonogram
MRI
Tumor marker 9blood test)
Biopsy (usually follow finding by imaging or blood test)
Ovarian/Endometrial Surgical Treatment
Hysterectomy (TAH/TH)
Bilateral salpingo-oophorectom (BS)
LymphNodeBiopsy
OMental Biopsy
Pelvic Washing
Debulking cytoreduction: get all visible cancer out
Ovarian/Endometrial Cancer Radiation therapy
Only for Endometrial Cancer NOT Ovarian Cancer
Ovarian/Endometrial Cancer Hormonal Therapy
Alternative to hysterectomy to preserve fertility
Ex Progesterone
Synthetic forms of the naturally-occuring hormone porgesterone; Presnet ina llforms of hormonal birth control
Preveny pregnay by inhibiting ovulation
Unopposed Estrogen can cause an overgrowth of the endometrium, which may lead to endometrial canca becoming cancersours
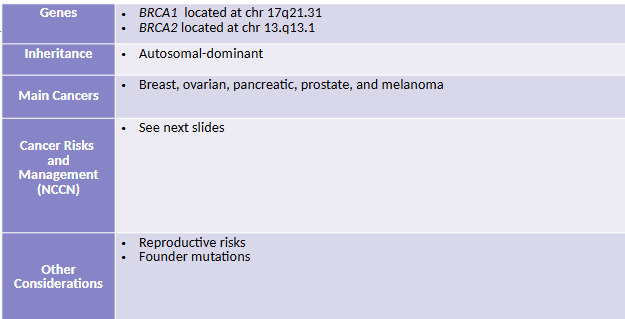
Hereditary Breas-Ovarian Cancer Syndrome (HBOC)
HBOC General Testing Criteria - Clinically indicated
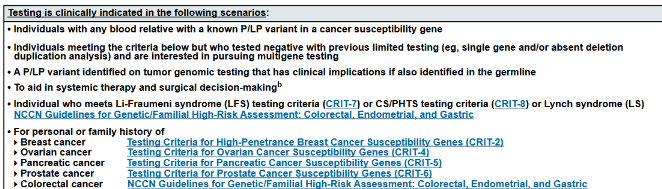
HBCO General Testing Criteria - Testing may be concidered

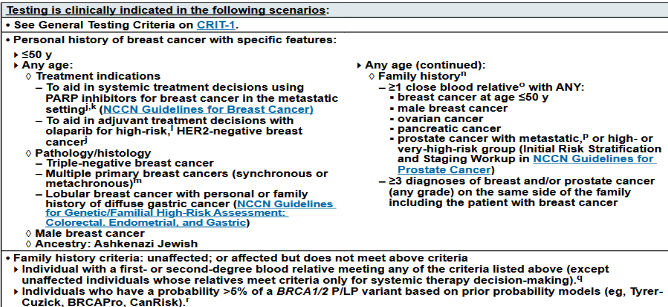
Breast Cancer Susceptibility Genes Testing Criteria
Less than 50yo at diagnosis
To aid in Systemic treatment decision: PARP (BRAC1/2), Olaparib (HER-2Negative)
Pathology/Histology:
Triple negative Breast Cancer (Estrogen, Progesterone, HER-2 receptors)
Lobular Breast Cancer w history of DIFFUSE GASTRIC CANCER
Multiple Primaries
Male Breast Cancer
Ashkenazi Jewish Ancestry
Family history
1 close blood relative with: <50yo Breast, male Breast, Ovarian, Pancreatic, Metastatic Prostate
3 Diagnosises of Breast and/or on same side of the family
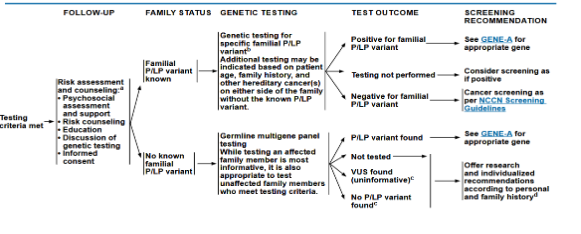
HBOC Guide Lines: Risks and Management
BRCA1 Cancer Risks
Breast:
Primary: 60-72%
Contralateral: 30-40%
Male: 0.2-1.2%
Epithelial Ovarian: 39-58%
Prostate: 7-26%
Pancreatic: <5%
BRCA2 Cancer Risks
Breast:
Primary: 55-69%
Contralateral: 25%
Male: 1.8-7.1%
Epithelial Ovarian: 13-29%
Prostate: 19-61%
Pancreatic: 5-10%
Melanoma: unknown
General Population Cancer Risks
Breast 12-13%
Ovarian 1-2%
Prostate 12-13%
Pancreatic 1-2%
ALWAYS compare to general population RISK!
Risk REduction for HBOC - Breast
Hormonal Therapy: 50% reduction
Masectomry: 90% reduction
Bilateral Salpingo-Oophorectomy (removal of both sides fallopian tube and ovary): 50% reducation (in pre-menopausal women)
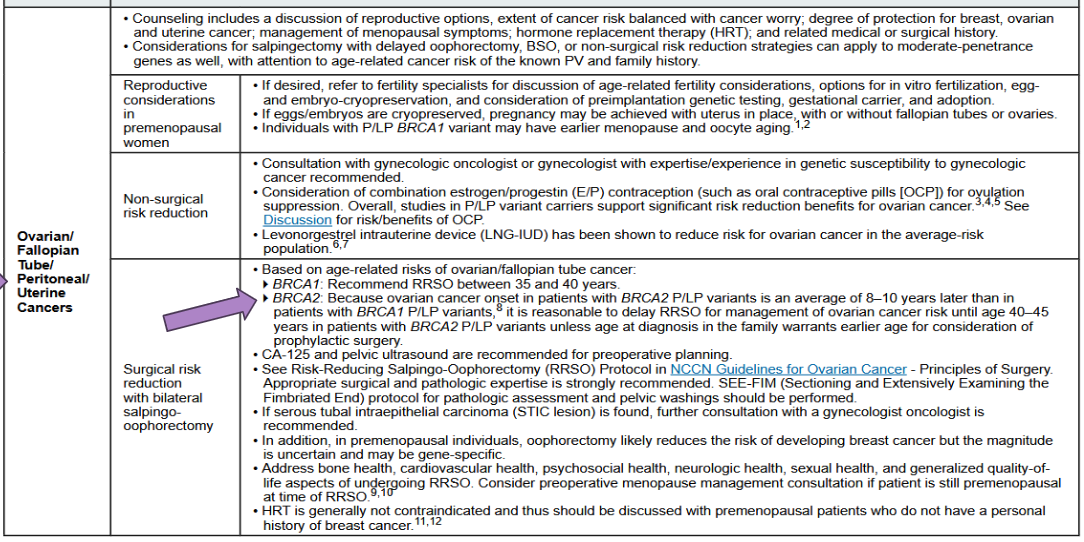
Risk Reduction for HBOC - Ovarian Cancer
Bilateral Salpingo-Oophorectomy (BSO): 96% reduction
Oral Contraceptive Pills (OCPs): 50% reduction (if taken for ~10years)
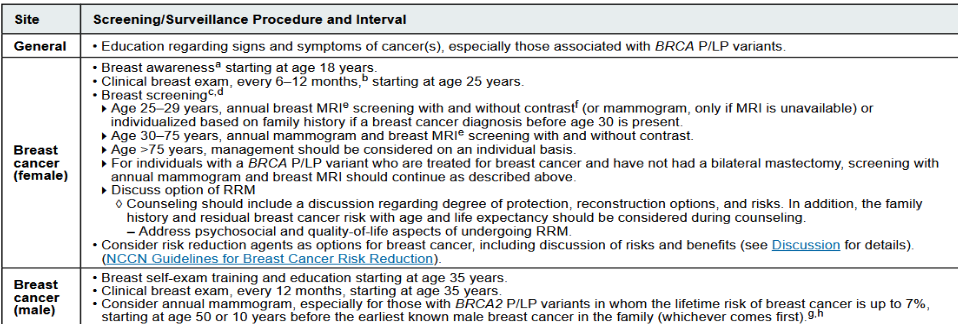
BRCA Positive Clinical Management - Breast Cancer
Women
At 25yo: Clinical Breast Exam 6-12 Months
25-29yo: MRI imaging
30-75yo: Annual mammogram and MRI
>75yo: management considered on an individual basis
Men
At 35yo: Self Exam + Annual Clincial Exam
50yo: consider mamogram
BRCA Positive Clinical Management - Ovarian/Fallopian/Perioneal/Uterine
Surgical risk reduction of Ovarian/Fallopian Cancer
BRCA1: Recommend Risk-Reducing Salpingo-Oophorectomy (RRSO) at 35-40yo
BRCA2: Recommend Risk-Reducing Salpingo-Oophorectomy (RRSO) at 40-45yo {Why? BRCA2 Ovarian cancer present 8-10 years later than BRCA1}
BRCA Psotive Clinical Managment - Prostate
Screening/Surveillance: at 40yo
BRCA1: consider prostate screening
BRCA2: recommend prostate screening
BRCA Positive Clinical Management - Pancreatic Cancer
only with Pos. BRCA AND with a Fam Hx of Pancreatic Ca
start at 50yo or 10years younger than relative’s diagnosis
Endoscopic Ultrasound ( )
Magnetic Resonance Cholangiopancreatography (a technique for viewing the bile ducts and pancreatic duct, pancreas gallbladder and liver)
PARP Inhibitor
Targets the Poly (ADP-Riobse) Polymerase enzyems: repair single strand breaks via base excsion repair
BRCA1/2 cancers have no Double Stranded Break repair system
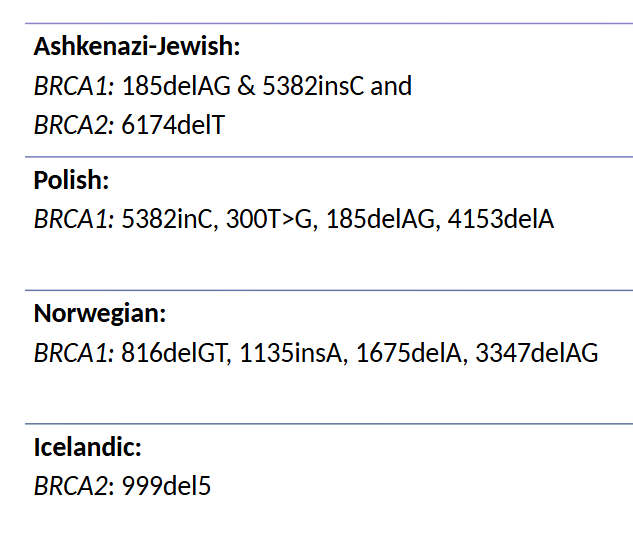
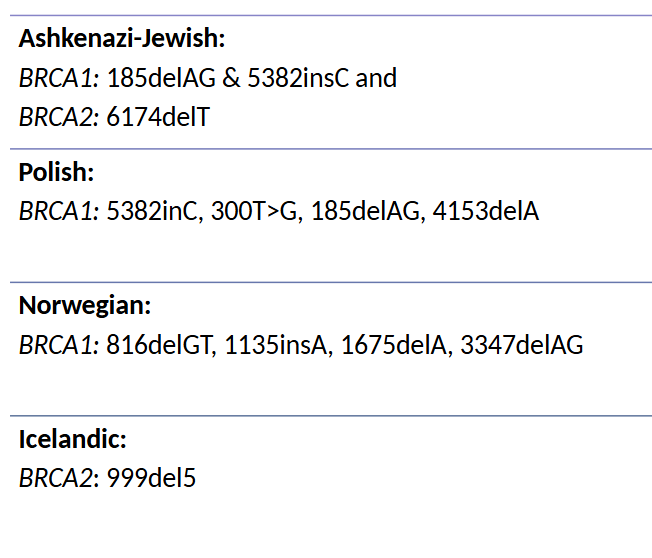
Founder Mutations in BRCA1/2
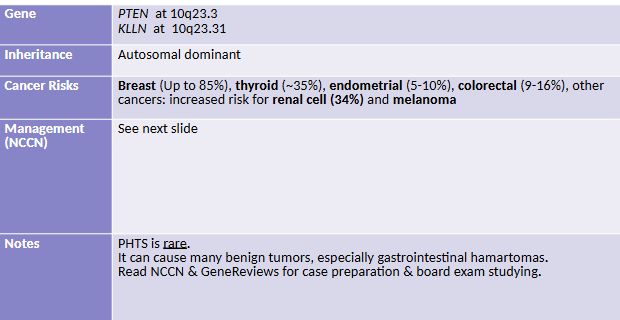
PTEN Hamartoma Tumor Syndrome (PHTS)
PHTS syndrome includes the following phenotypes:
Cowden Syndrome
Bannayan-Riley-Ruvalcaba
Adult L’hermite-Duclos disease
Protus-like syndrome
Autism spectrum disorder with Macrocephaly
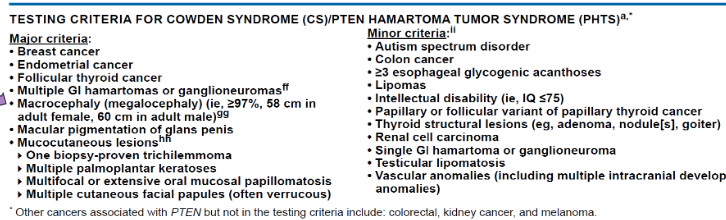
Diagnosing Cowden Syndrome
Major
Breast Cancer
Epithelial thyroid cancer (NON-MEDULLARY)
**** Macrocephaly *****
Endometrial carcinoma
Minor
other thyroid lesions
Intellectual disability
Hamartomas intestinal polyps
Lipomas
Fibromas
Genitourinary tumors
Uterine fibers
Bannayan-Riley-Ruvalcaba Syndrome (BRRS)
PTEN Hamartoma Variant
Macrocephaly
Intestinal hamartomous polyposis
Lipomas
Pigmented macules of the glans penis
Proteus Syndrome
CAN BE a PTEN Hamartoma Variant
Highly variable disorder—> clinical diagnosis hard, molecular diagnosis preferred
Hamartoma growth of multiple tissues
connective tissue nevi
epidermal nevi
hyperostoses
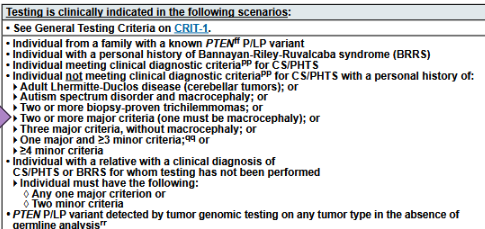
Testing Criteria for PTEN
Not meeting clinical criteria for CS/PHTS but with:
Autism AND Macrocephaly
Two or more Trichilemmomas
PTEN Hamartoma Tumor Syndrome Cancer Risks
Breast: 85%
Thyroid (NEVER MEDULLARY): 35%
Renal Cell: 34%
Endometrial: 28%
CS/PHTS (PTEN) Clinical Managment
Thyroid: US starting at 7yo
Breast: Screening at 25yo
Colorectal: Screening at 35yo
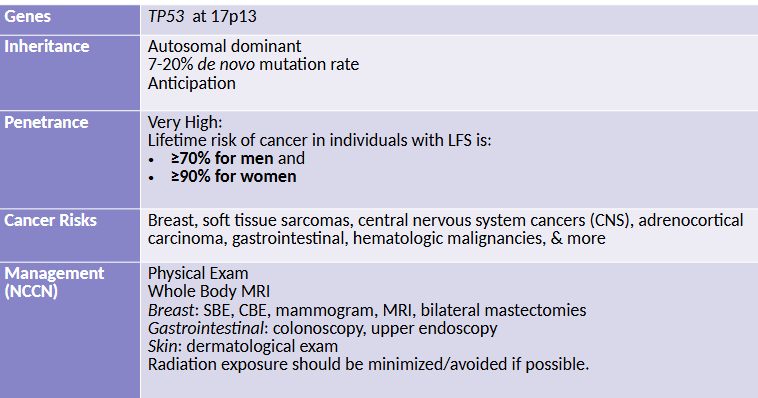
Li-Fraumeni Syndrome (LFS)
Li-Fraumeni Diagnosis/Testing Criteria
TP53 positive
or
Three classic clinical positive
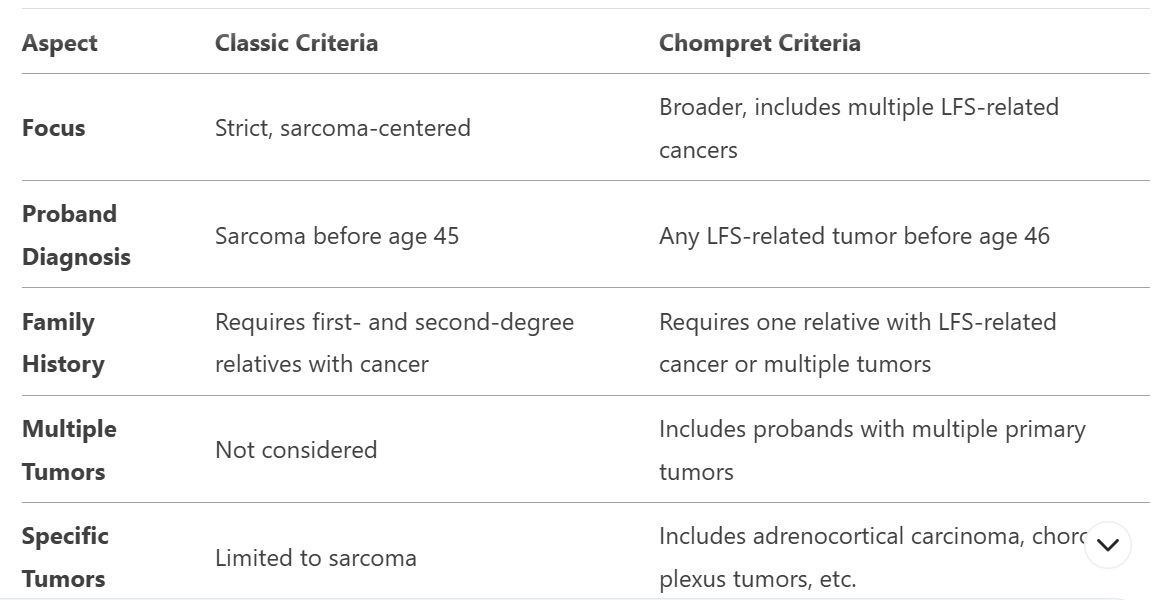
Li Fraumeni Chompret
LFS should be suspected in individuals who meet the chompret criteria
Has LFS tumor (breast, sarcoma, osteosarcoma, CNS tumor, adrenocortical tumor) AND realtive with LFS tumor before 56yo
Multiple tumors, two of which are LFS tumor before 46yo
Adrenocortical carcinoma, choroid plexus tumor, or rhabdomyosarcoma
Breast cancer before 31yo
Therapeutic Considerations for Lif Fraumeni
Radiation therapy should be minimized: potential for downstream malignancies
Li-Fraumeni Screening/Surveillance
Breast: 20yo every 6-12 months (Clinical+MRI)
Other Cancers: 25yo endoscopy, 18yo Skin exam
Pediatric
Annual Brain+Body MRI starting in infancy
Ultrasound every 3-4 months in infancy
Li-Fraumeni Testing Consideration
somatic TP53 detection can confound germline testing: can be detected in blood or slavia —> increase with age, NGS suspetiable
Must test tissue other than blood and salvia
Comepltle blood count nad perhihpal blood smear must also be done in TP53 postive detection
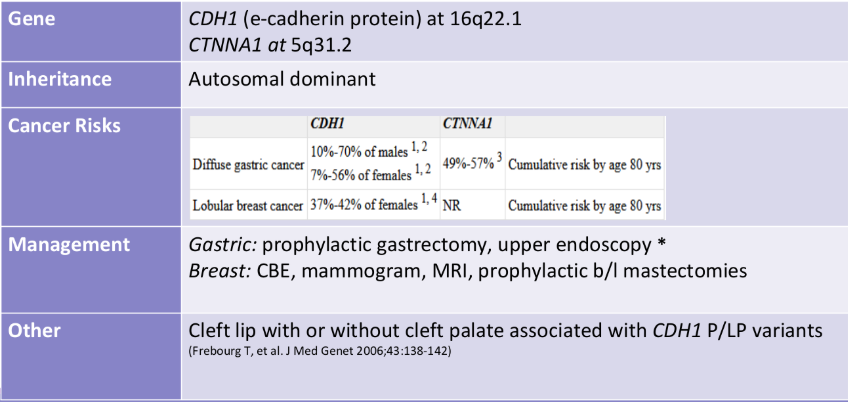
Hereditary Diffuse Gastric Cancer
Breast Cancer Genes
BRCA1 +2, CDH1, PALB2, PTEN, STK11, TP53
CLassic vs ChomperatCriteria for Diagonis of Li Fraumni
Skin Fibroblasts
the best option for germline testing tissue for TP53 mutations (Li Fraumeni)
Li Fraumni has alot of potenaitl for somatic mutation, blood samples can confound germline many times so skin fibroblasts are the best option
Hereditary Diffuse Gastric Cancer
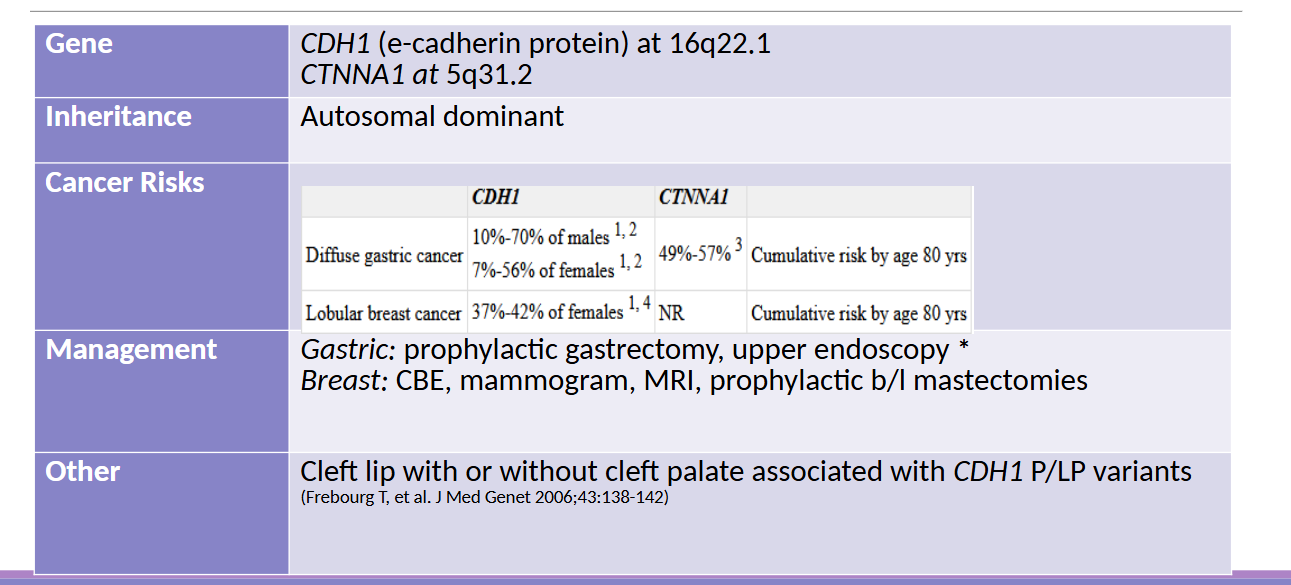
Signet Ring Cells
Associated with Diffuse Gastric Cancer syndrome: presence pathologically confirms diagnosis of DGCS
Controversy on Gastric Cancer Risk reduction surgery
Gastrectomy reduces risk <1%
But: Quality of life dramatically affected —> major dissatisfaction
Adult vs Child Hereditary Cancer syndromes
Adult syndromes: MonoAllelic mutatations
Childhood Syndromes: BiAllelic mutations
Francoi Anmeia
Bi allalic mutations in BRCA1, BRCA2, BRIP1, PALB2, RAD51C
Ataxia-Telangiectasis
Bi allelic pathogenic mutations in ATM gene
Bloom Syndrome
Bi allelic pathogenic mutations in BLM