Preventive (D1 Spring) Exam Two [Nutritional Assessment: Marshall]
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
You need to acknowledge the _____ health in order to be an effective dentist
nutritional
note
- or any conditions
Nutritional care can be divided into 4 areas
Assessment
Planning
Implementation (education)
Evaluation
Assessment
Identification if there is a problem and what is the problem
Planning
Determine the best method of treatment
Consider compliance and resources
Implementation
Putting the plan into action. Includes education of the patient
May never occur depends on the patients perspective of the problem
Evaluation
Review the plan assess the situation. Is it still appropriate. Modify and reinforce
Levels of nutritional assessment
Screening assessment
- most basic really identify who needs additional assessment.
Primary assessment
- Routinely conducted at WIC or public health clinic with basic treatment or referral. What you do for patients who fail their screen and or have obvious oral disease
Secondary assessment
- Generally at hospital level, with a dietitian, secondary level of care
Tertiary assessment
- At a specialty center for patients with significant needs. For example patient with eating disorders at an ED clinic
Nutritional assessment: Definition
Definition: Evaluation of a person's health from a nutritional perspective
Nutritional assessment: Objective
Objective: To identify individuals who are malnourished or at "risk" for malnutrition
Malnutrition is due to
Deficiency of nutrients/energy
Excess of nutrients/energy
Imbalance of nutrients
Clinical classification of malnutrition
Over: Physically obvious, visible
Subclinical: Before clinical signs or symptoms are apparent
Causes of Deficiencies (toxicity)
Primary: Due to inadequate dietary intake
- primary toxicity is due to excessive intake
Secondary: Due to altered 'other', adequate dietary intake
- secondary toxicity is associated with decreased need, utilization, excretion
Can't pick up a secondary concern with a diet screening because they could have adequate diet
Components of nutritional assessment
Histories- gathering subjective/objective information.. helps to establish rapport as well as identify patient's perspective of health/diet what they might be willing to change.
Anthropometric measures- Measuring the body
Clinical appearance- what do you see when you look at the patient
Biochemical measures- Lab values
Histories: Medical history
Assessment of high risk conditions that predispose or accompany malnutrition
- diagnosis
- infection history
- surgical history
- family history
- mental health status
- growth
Histories: Socioeconomic history
Assessment of social/environmental factors affecting ability to obtain proper nutrition
- Finances
- Physical facilities
- Social support
- Community resources
- Education
Histories: Medication history
Assessment of food or nutrient-medication interactions
- nutrition supplements
- over-the-counter medications
- prescription medications
- street drugs
Histories: Dietary history
Assessment of intake and factors which influence intake
- Current intake- past intake
- Dietary habits
- Feeding skills development
- Psychosocial factors
- Prescribed/self-imposed diets
- activity patterns
- family/culture/environment
How do we asses current intake
24 hour/usual recall
Food records
Food frequencies
Observation
Questionnaires
24 hour/usual recall
List what ate yesterday...usually
1. memory dependent-but easy
2. Good for groups; need 3-21 recalls for accurate nutrient intake by an individual
Food records
3-7 days; > 3 loose compliance
1. record as eat- accurate; burdensome
2. Change eating with recording?
3. Increase awareness of usual habits
Food frequencies
questionnaires that assess frequency and/or quantity of foods contributing key nutrients/energy
1. Specific to population
Observations
Ideal but artificial
Questionnaires
Use with above to gather additional information
Not always feasible to assess current intake:
Patient with alcohol issues
history of traumatic brain injury as child
Intake evaluation
Food group analysis
- myplate
Nutrient analysis
Energy analysis
Anthropometric measures
Measurement of body size, weight or proportions
Indirect assessment of body composition
Weight = Fat mass + Fat-free mass
Reference populations
Anthropometric: basic components
Height
- generally think of standing height
Weight
Circumferences:
- head
- midarm
- waist
- hip
Skinfolds:
- triceps
- subscapular
- suprailiac
Anthropometric applications
Growth and development
- standards
Nutritional status
- change
Body composition
- body mass index
Body fat distribution
- waist to hip ratio
- Waist circumference
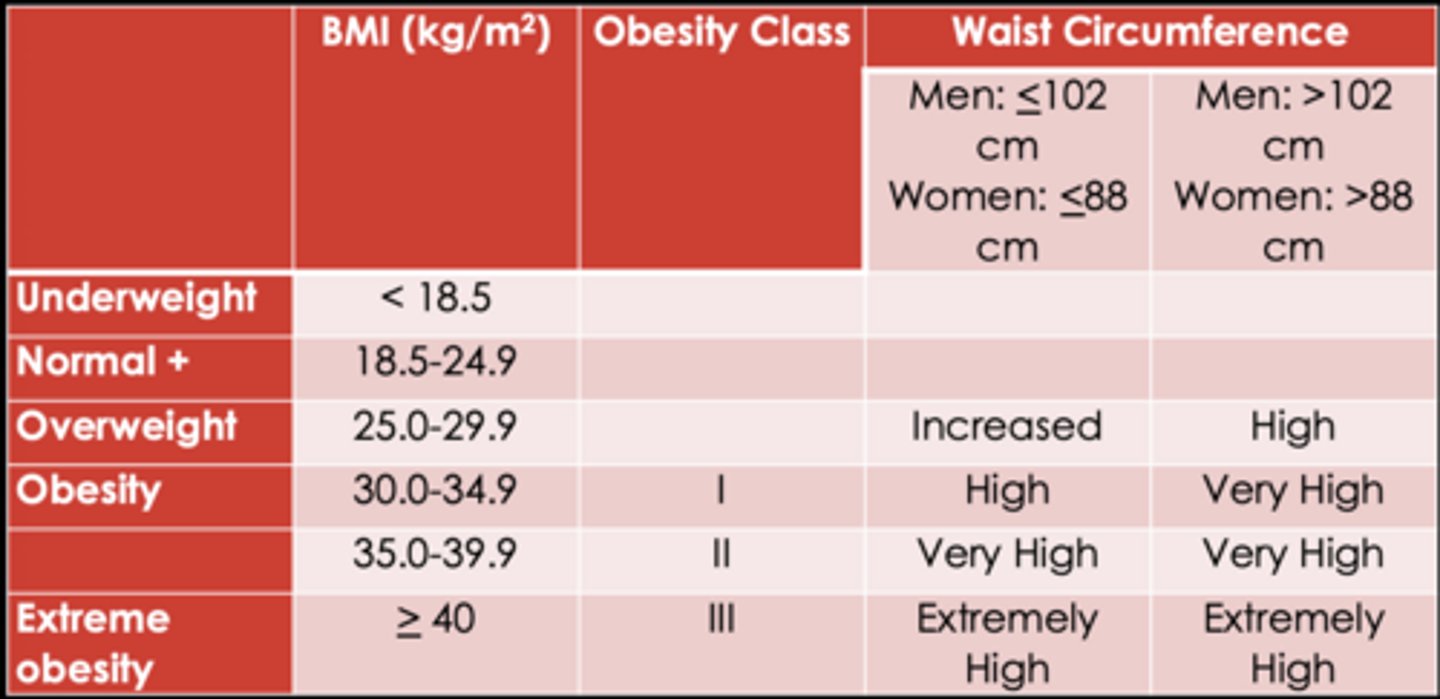
BMI + Waist circumference
- Disease risk
Disease risk: BMI x Waist circumference
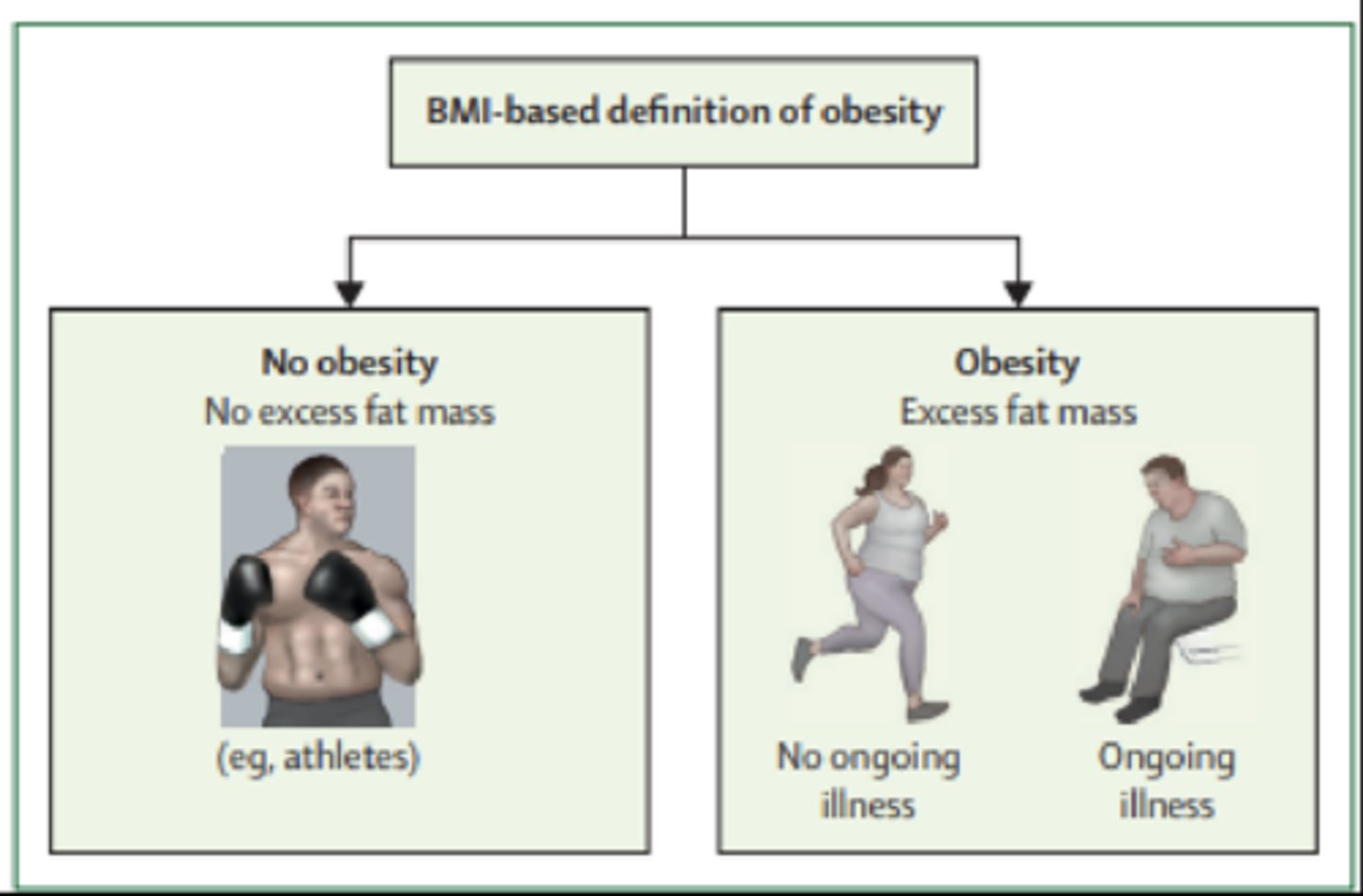
Obesity Definitions- BMI-based definition of obesity
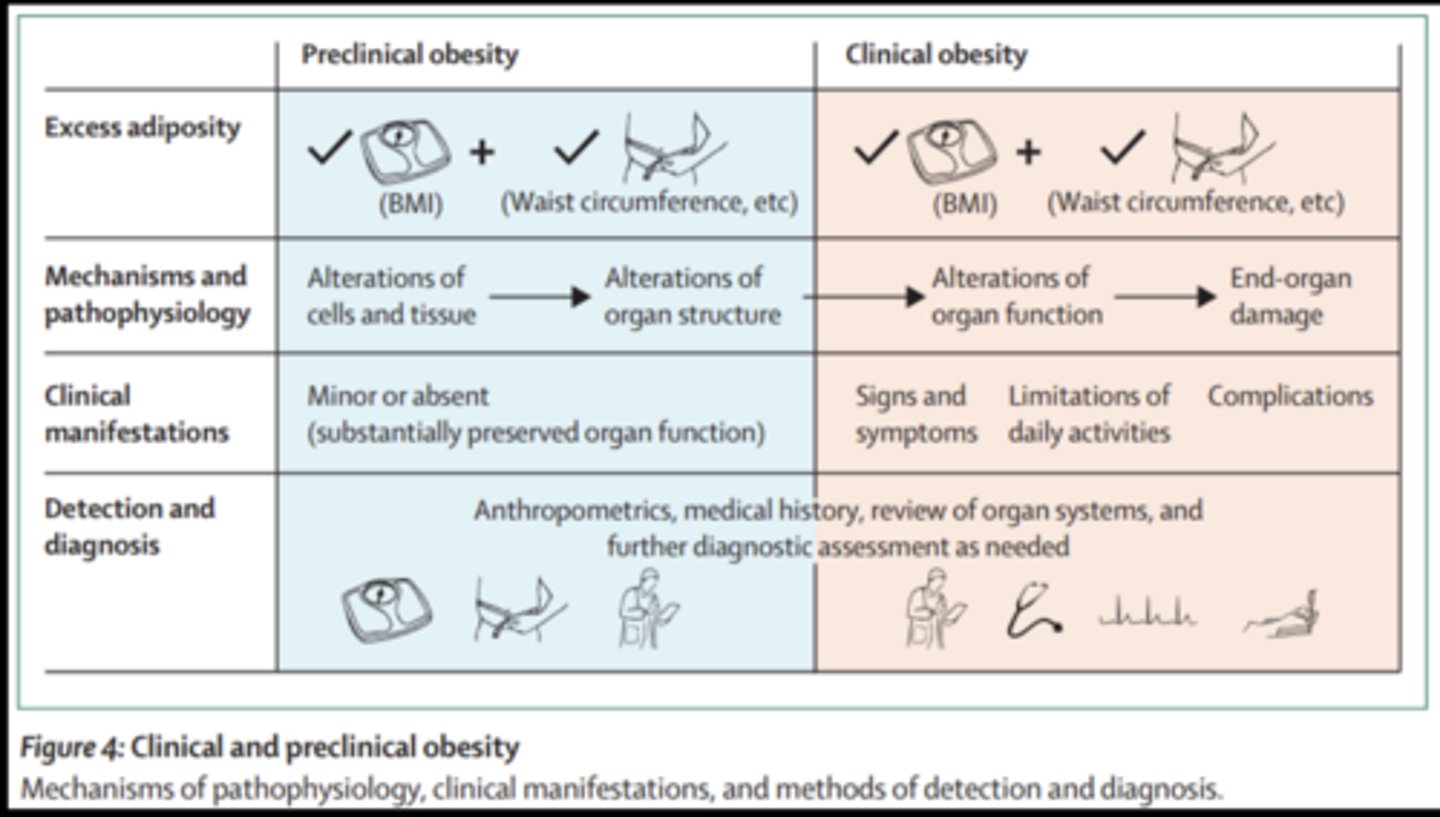
Obesity Definitions- preclinical vs clinical
Clinical Appearance
Signs and symptoms
Overt (visible) signs of malnutrition
- hair
- skin
- eyes
- oral tissue - tongue gums teeth lips
- nails
- muscles, skeletal system
Biochemical measures
Measurements of a nutrient or metabolite in blood urine or body tissue
Measures may be static or functional
Useful to detect subclinical and confirm clinical malnutrition
Problem
- nonspecific
- values influenced by nonnutritional factors such as disease, trauma, medications
Biochemical measures: Protein status
Visceral--serum albumin, prealbumin, transferrin
Somatic-- creatinine excretion, creatinine height index, 3-methylhistidine
Biochemical measures: Iron status
Serum ferritin, transferrin saturation, hemoglobin, mean corpuscular volume
Biochemical measures: Vitamin A status
Serum Vitamin A, dark adaptation, liver stores
Summary nutritional assessments
History --brief
- 24 hour/usual recall
Anthropometric
- weight, height
Clinical appearance --obvious
Biochemical measures
- screen specific (hematocrit, cholesterol)
Conclusion
Age determines focus assessment
- children- expect growth and development
- adult- expect maintenance of weight and height
Change is significant for individuals
Combination of tools
- no one tool is ideal
Treatment vs preventions
- cheaper higher cost effectiveness
- Less morbidity and morality
Go through case studies: NOT on slide video ~1:03:06
How do they want us to apply the nutritional assessment to dental clinic
Consider medical history, drug history, anthropometrics, and clinical appearance with diet to consider implications for oral health
DIETARY ASSESSMENT OF PATIENTS
DIETARY ASSESSMENT OF PATIENTS
Practical assessment strategies
Screen: every patient
Assess: Those identified at caries risk or with other oral health red flags
- obvious disease- target assessment towards current disease
- healthy- target assessment towards prevention
Refer: Patients with dietary/systemic health red flags
Goals of screening process
Identify patients at risk due to marginal dietary habits
- caries risk
- periodontal disease risk
- systemic health risk
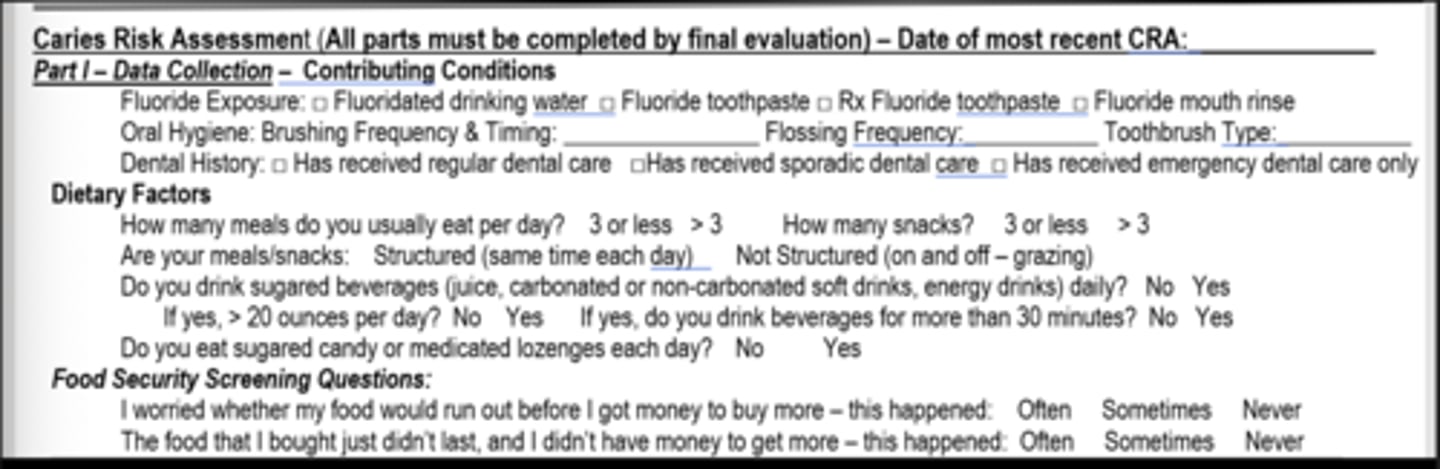
Screening process- caries
Dietary factors (worksheet)
Frequency
- eats more than 3 meals per day
- eats more than 3 snacks per day
- meals/snacks are not structured
Drinks sugared beverages (juice, soft drink, etc)
- drinks more than 20 oz sugared beverage daily
- drinks beverages for more than 30 minutes daily
Eats sugared candy or medicated lozenges daily
If nothing else what should be your three questions for screening
1. Unstructured meals
2. Daily sugared beverages
3. >30 minutes
Screening process- general
Compliance with MyPlate
- all food groups in adequate quantities
- all food groups consumed daily; inadequate quantities
- missing food groups
Unintentional weight loss or gain
- defined as weight change or more than 10 pounds in 6 months
- consider medical referral- not natural
Food security
Defined as access to enough food at all times for an active healthy lifestyle
- availability
- accessibility
- utilization
- stability
Food insecurity
Defined as limited or uncertain access to adequate food due to economic or social conditions
- high food security (food security)
- Marginal food security (food security)
- Low food security (food insecurity without hunger)
- Very low food security (food insecurity with hunger)
Clinical form
Goals of assessment strategy
Identify dietary habits that increase disease risk
- educate as to rationale for 'better' dietary habits
- provide guidelines to achieve 'better' dietary habits
- focus recommendations
-- patient motivation
-- Reasonable changes
Practical perspective
- easy for clinician
- efficient for practice
- patient has to remember conversation when they get home
Chairside diet assessment of caries risk: Best practices
Defines key dietary areas for caries risk
Presents concept of anticipatory guidance
- recognize obstacles and provide advice before obstacle becomes problem
- no one food is consumed in isolation
-- what are ripple effects of consumption
-- what are ripple effects of lack of consumption
Examples
Foundation for brochure development
Brochure: Objectives
Facilitate patient education regarding dietary risk factors for caries
streamline caries risk assessment for patients identified at risk
Facilitate dietary recommendations targeting undesirable habits
Enables anticipatory guidance with respect to remainder of diet
Take home tool so patients remember conservation
Brochure: Components
Caries risk factor
- education
MyCavity Risk
- identify patient risk factor
- provide recommendations
MyPlate
- emphasize dietary foundation
- provide guidelines as to what should be eating
Additional recommendations
- reinforcement and extra guidelines
Fitting the pieces
- education
Brochure: general
Conversation with patient
- dietary change occur over time
- Document conversation and evolution of habits
Axium... screen shot
- forms
- caries risk assessment
- dietary assessment