psychology final
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
Circadian rhythm
the regular bodily rhythm that occurs over a 24 hour period; the biological clock,
regulated by the suprachiasmatic nucleus (SCN) of the hypothalamus, which responds to morning light and triggers the pineal gland to decrease melatonin production
Pineal gland - pumps out melatonin
Melatonin - darkness hormone
EEG
electroencephalograph, electrodes are placed on the scalp to measure electrical activity in the cortex during sleep. Eye movements and muscle tension are also monitored
Measuring electrical activity in the brain and graphing it out
NREM 1 and 2 are light stages and you may move a little, lower heart rate
REM - no movement, higher heart rate
Sleep cycle
sleep consists of repeating patterns of distinct stages (NREM 1-3 and REM) that occur in 90-minute cycles
We spend more time in NREM-3 (deep, slow-wave sleep, extra groggy when waking up) during the first 3 hours of sleep (first 2 sleep cycles)
As sleep progresses into the latter half of the night, we begin to experience longer episodes of both NREM-2 and REM sleep
REM Sleep
We cycle through REM about 5 times per night
Most of our dreaming takes place during REM
Physiological arousal, (heart rate rises, breathing becomes rapid, genitals are aroused)
REM is referred to as paradoxical sleep because body muscles are immobile, but the brain and sympathetic nervous system are active
REM is associated with fast brain-wave activity that is similar to an alert, waking state
Several brain areas become active due to an increase in acetylcholine levels at the onset of REM
Prefrontal cortex remains deactivated
Sleep paralysis
occurs when the pons of the brainstem blocks the motor cortex’s messages to the somatic nervous system
- pons does not get the message that you are awake
People with REM sleep behavior disorder
act out their dreams because of degeneration of neurons in the pons, pons does not shut down motor signals physically acting out dreams while in body sleeping
Insomnia disorder
persistent difficulties with sleep quantity or quality associated with one or more of the following symptoms: Difficulty falling asleep (takes longer than 30 minutes), Difficulty maintaining sleep, Early-morning awakening and inability to return to sleep
Must occur at least 3 nights per week for at least 3 months
Insomnia often occurs with other psychological disorders
Hypersomnolence disorder
individuals with this disorder fall asleep quickly and have good sleep efficiency (sleep throughout the night)
Excessive nighttime sleep (10-12 hours or more) along with significant difficulty waking up (sleep inertia) - feel like a zombie when waking up
Excessive daytime sleepiness with long naps (>1 hour) nearly every day
Sleep is non-restorative - still feel sleepy when waking up
Delayed sleep phase type (Circadian Rhythm Sleep-wake disorder)
A lifelong disorder
A persistent inability to fall asleep and awaken at a desired or conveniently acceptable earlier time, often deviates 2-4 hours from desired sleep and wake-up time
Symptoms of sleep-onset insomnia, difficulty waking in the morning, and excessive sleepiness early in the day are prominent
Because these individuals have a history of difficulty falling asleep at a normal time, they often develop maladaptive behaviors (like doing work, playing games, watching TV, searching the internet) that further increase arousal and impair sleep
When allowed to set their own schedule, individuals exhibit normal sleep quality and duration
Non-REM Sleep Arousal Disorders
symptoms occur during NREM sleep; occur most commonly in childhood and diminish in frequency with increasing age
Sleep terrors
recurrent episodes of abrupt terror arousals while still sleeping, usually beginning with a panicky scream and sitting up in bed with eyes wide open. There is fear, rapid heartbeat and breathing, sweating, etc. Individuals are often unresponsive to the efforts of others trying to comfort them. If awakened, they do not report a story-like nightmare sequence
Amnesia: no memory of the episode
Sleepwalking
an individual has a blank, staring face; is relatively unresponsive to the efforts of others to communicate with him or her, and can be awakened only with great difficulty. They can even endure injuries without pain, until awakening. Can sometimes be accompanied by sleeptalking, eating or even ‘sexsomnia’ in adults.
Amnesia: no memory of the episode
Narcolepsy
at night individuals fall asleep and quickly enter REM sleep early
Excessive daytime sleepiness+increased need for sleep
Recurrent daytime sleep episodes (ex. Short naps) that mimic REM sleep
People with narcolepsy often have a deficiency in orexin/hypocretin; a neuropeptide which typically promotes wakefulness
Cataplexy- narcolepsy
sudden muscular weakness (loss of muscle tone) such as going weak in the knees, slumping in a chair, slurred speech, jaw dropping, etc. often triggered by positive emotion- laughter or joking
Sleep paralysis - narcolepsy
inability to move when waking from sleep
Hypnagogic hallucinations - narcolepsy
dreamlike sensations that occur with onset of sleep attack (ex. Seeing vivid static images, hearing voices, or phone ringing, or feel like they are falling or weightless)
Growth and Maintenance of Body and brain
sleep drive increases after strenuous physical activity and after long periods of wakeful activity (doing tiring stuff)
During sleep, the pituitary gland releases growth hormone so that's why babies and teenagers need the extra sleep. Older people release less of this hormone and sleep less
Sleep is important for immune cell production and improves immune response
Sleep restores and repairs the brain: helps reduce the levels of DNA damage in neurons, increased production of new glial cells that form myelin, maintenance of neurons in the hippocampus, amygdala, and prefrontal cortex; maintains functionality in those cortical circuits
Memory encoding and consolidation
sleep helps strengthen neural connections that build enduring memories
Getting memories you just learned into long-term storage
Sleep prior to learning enhances our ability to encode new experiences and information
Sleep after learning helps to consolidate those memories
Sleep and dreaming leads to improved performance: better for recall of list of words and etc. and faster, more accurate performance of procedural memories
Explicit memories
list of words, material for upcoming exam
Implicit memories
procedural memories such as playing an instrument, trying to beat a video game - muscle memory
Video with rats and sleep and memories
Sleep improves maze running activities
While you sleep, brain is receiving stuff + what you did wrong and you'll improve when waking up
Mapping rats thoughts
When rats sleep, the same pattern of brain activity is shown when they are running through the maze
Hippocampus cells are activated
Special navigation memories
Hippocampus cells reactivate in sleep
Freud's interpretation of dreams
argued that dreams are the disguised wishes and desires of our unconscious mind
He believe that images in dreams (‘manifest content’) are not what they appear to be
Instead, they are symbols of hidden wishes that require deeper interpretation to uncover their true meaning (‘latent content’)- manifested things to be similar to genitals
Freud's theory of drea, interpretation is not falsifiable and therefore lacks scientific support - claims can’t be validated
Dreams
Everybody dreams at night, but most of them are forgotten before we wake up
Dreams during NREM sleep are often extensions of wakeful experience (‘sleep thinking’)
Dreams during REM sleep are bizarre and vivid
Dreams sometimes include images from frequent experiences or particularly emotional experiences
The thoughts, emotions, and worries that precede sleep are the things most likely to be incorporated into our dream content
About 80% of dreams often include some negative event or emotion (ex. Failure dreams such as being pursued, attacked, rejected, or having bad luck)
Neurological components of emotion
Limbic system (amygdala, hippocampus): helps coordinate our emotions and encode emotional memories
Cortical areas (ex. ACC, insula, and prefrontal cortex): help guide our behavioral response to emotional stimuli
Autonomic nervous system and endocrine system: physiological response to emotional stimuli
6 universally recognized emotions
Happiness
Surprise
Sadness
Fear
Anger
Disgust
Emotions as evolved adaptations
Charles Darwin was the first to argue that the purpose of emotions is to facilitate adaptive behavior and decision making in response to salient events
They have been shaped by natural selection because they contributed to the survival and reproductive success of our phylogenetic succession of mammalian, primate, and hominid ancestors
Selye's General Adaptation Syndrome
Hans Selye, an early pioneer in stress research, coined the term ‘general adaptation syndrome’ to describe how all organisms respond to stress
Phase 1: Alarm reaction (mobilize resources), new acute stressor in life, ability to resist stress decreases
Phase 2: resistance (cope with stress) - ability to resist stressor increases
However, the body's resistance to stress can only last so long before exhaustion sets in
Phase 3: exhaustion (reserves depleted) - resistance decreases also tends to be more sick/immunocompromised
Problem-focused coping: confronting stressor
attempting to directly change the stressor or change the way we interact with it, ex. Confronting a hostile family member who is causing stress to directly address the issue
Emotion-focused coping
attempting to relieve or regulate the emotional impact of a stressful situation, ex. Seeking reassurance about the situation from a friend
Acute stress
sympathetic nervous system fight-or-flight response (epinephrine/adrenaline), sometimes oxytocin
Chronic stress
hypothalamus-pituitary-Adrenal (HPA) Axis (glucocorticoids/cortisol)
Telomere shortening
What is the HPA axis? What hormone is associated with HPA activity?
A major component of the homeostatic response is the hypothalamic-pituitary-adrenal (HPA) axis, an intricate, yet robust, neuroendocrine mechanism that mediates the effects of stressors by regulating numerous physiological processes, such as metabolism, immune responses, and the autonomic nervous system (ANS).
Chronic stress leading to the release of cortisol
Stress and the immune system
during stress, energy is mobilized away form the immune system making it vulnerable. People with the highest life stress scores were also the most vulnerable when exposed to an experimental cold virus
Emotional responsiveness to stressors
Classic ‘Type A’ individuals are competitive and hardworking, but also tend to be impatient and prone to anger and hostility.
Research suggests that these individuals are more susceptible to negative effects of stress, including vulnerability to heart disease and decreased life expectancy
The level of hostility expressed when confronted with stressors seems to be the biggest risk factor
Relation between chronic stress and social status - research in baboons
Baboons being stressed by each other
When animal escapes stress response turns off
Humans don't/cant turn off stress response
Baboons rank determined the level of stress hormones
Dominant males had a lower stress level
The lower a person is in their hierarchy → higher stress and heart disease risk
Results of the Dutch hunger winter study
Individuals didn’t have enough food, water, electricity
Data was analyzed from people born before and after the famine
Babies from the famine were more responsive to stress and had poorer health
Resulted in Metabolic syndrome → precursor to diabetes and cardiac disease
Maslow's hierarchy of needs
Maslow proposed that we are motivated by a hierarchy of needs. We must have needs lower on the hierarchy met before we can try to reach the state of self-actualization- fulfilling our potential
Order: top → bottom
Self-actualization
Status, esteem
Belonging, social activity
Safety, security, comfort, sex
Basic physiological needs, food, water, etc.
Carl Rogers humanistic approach (to therapy)
conditions of positive growth:
Genuineness and empathy - open with feelings, transparent and self disclosing, attuned to others’ emotions
Unconditional positive regard- an attitude of acceptance of oneself and others despite their failings and perceived limitations
Internal locus of control - the perception of that we can control our own fate
Personal control and learned helplessness
normally we try to escape or end a painful situation, but persistent external locus of control can make us lose hope
Accepting fate instead of leaving bad situations such as abusive relationships
Uncontrollable events → perceived lack of control → generalized helpless behavior
Long-term happiness set-point
how would winning the lottery change your life satisfaction and long-term happiness?
How would the death of a loved one change your life satisfaction and long-term happiness?
Personal happiness is typically stable throughout our lives
Can money buy happiness?
“emotional well-being” and income levels:
Measured by analyzing the rates of daily positive affect (smiling, laughter, joy) as well as rates of negative affect (worry, sadness, stress, anger)
Research indicates that there is an overall positive correlation between emotional well-being and income
However, beyond a certain threshold, higher income is neither associated with experienced happiness nor relief from worry, sadness, or anger
Other factors to consider: relative deprivation, the hedonic treadmill, how we spend our money
Relative deprivation
comparing selves to people who are more than them, focusing on trying to keep up with others
The hedonic treadmill
pleasure seeking, buying stuff, once you get it satisfaction eventually wears off
How we spend our money
on experiences, vacations, people usually report more satisfaction with these things
Meditation and well-being
when labeling emotions during mindfulness meditation, people show less activation in the amygdala and more activation in the left prefrontal cortex
There is also evidence that meditation:
Slows down areas of the brain associated with mind-wandering and self-judgment
Protects against a relapse in major depression
Reduces anxiety and sleep problems
Reduces glucocorticoid levels during and after
Reduces perceptions of pain (including chronic pain)
Boosts the immune system response (even in cancer patients)
Slows the aging process by protecting our telomeres from gradual decline
Genie’s Case study
Social isolation
Girl kept in so much isolation by her parents that she barely knew how to talk
She had a strange walk and other characteristics at first wouldn’t vocalize or make noise
She was first discovered at the age of 13
Weird walk, wouldn’t make eye contact or eat
She was able to speak a little “stop it” or “no more” lexacon, small vocabulary, phrases with few words
She never got to a higher grammatical complexity
This shows that there is a critical period that you need to be exposed to a language to learn it
Sensitive period of language development
if a child is not exposed to language early, the neurons in the left hemisphere of the brain which support these skills become pruned
Genie's case is an extreme example
Other evidence comes from individuals exposed to more than one language
Learning a second language
research on U.S. immigrants and their ESL (english as a second language) acquisition
What are the best predictors of mastery of this second language” age at immigration was the single best predictor of mastery of english
The earlier the better
Age of 7: you pick up just fine
Downward trend after that, especially after age of puberty
Bilingual brains
adults who learned a second language at 1-3 years of age showed the normal pattern of left-hemisphere activity in a test of grammatical knowledge
Those who learned the language later show more bilateral activation (ex. Increased right-hemisphere activity along with typical left activity)
Infants and language
babies are born with the capacity to learn any language
For a short period, babies have an ability to hear even the slightest of shifts in sounds
When a little older (a few months later), babies are able to only hear the distinctions from the language they are exposed to
Can no longer hear the fine differences in other languages
Milestones of language development
Prevocal learning - 2-4 months old: babies distinguish all phonemes they will later use for language
Babbling - 4-6 months: meaningless experimental sounds preceding actual language
Vocal turn taking - 7-8 months: basic understanding of the pragmatics of communication, back and forth turn taking
First words - 1 year old: simple words associated with objects or people, however kids’ language comprehension can be sophisticated at this time
Naming explosion - 18-24 months - mostly object words like car and dog
Telegraphic speech - begins at 18-24 months - two-word sentences omitting all but essential words, usually non-verb
Preschool period - 2.5-5 years: longer phrases/ sentences, start to use grammatical morphemes - modifiers that give more precise meaning to words/ sentences:
Adding ‘s’ for plurality; adding ‘ed; for past tense
Adding prepositions (in, on) and articles (the, a)
Infant directed speech
caregivers communications with infants
4 versions of melodies used during IDS: approval, prohibiting, comfort, attention
Semantic networks
Long-term memory
Words that have strong associative or semantic relations form larger networks of knowledge
These associated words can then act as anchors that help retrieve memory of other words, concepts, or schemas
Language production is essentially an app for converting a web of thoughts into a string of words
Areas in the brain involved in language
Speaking words: broca's area, M1-Mouth
Hearing words - auditory cortex, wernicke’s area
Seeing words - visual cortex
FOXP2
The KE family members with abnormal variants of FOXP2 have:
Reduced gray matter in Broca’s area, fewer neurons and connections between the neurons
Functional abnormalities in Broca’s area during language tasks
Wernicke’s aphasia
(receptive/fluent aphasia) impaired language comprehension due to damage of wernicke’s area
Difficulty understanding spoken and written speech (especially nouns and verbs)
Fluency of speech is normal; it lacks coherency and is therefore incomprehensible to others
A patient describing a picture of a child taking a cookie: “this and this and this. These things go in there like that. This one here, these two things here. And the other one here, back in this one”
Broca’s aphasia
(expressive/non-fluent aphasia) serious impairment in language production due to damage in Broca’s and related areas
Communication resembles telegraphic speech (ex. Simple noun verb combinations)
Can happen after a stroke , starting from nothing, used to be normal, unable to interact the same way with people
General intelligence
Charles Spearman first proposed the notion of general intelligence (g)
Based on research indicating that people who score high on one mental test tend to score high on others
The positive correlations between performance on a range of mental tests suggest that there is an underlying factor that contributes to success on each test
The global capacity is referred to as the ‘g-factor’
Fluid intelligence (gF)
reflects the ability to process information, particularly in novels of complex circumstances, ex. Reasoning and problem-solving
Crystallized intelligence (gC)
reflects on both the knowledge one acquires through experience and the ability to use that knowledge
Fluid and crystallized intelligence across the lifespan
cognitive aging, identification of synonyms (vocabulary) increases but these all tend to decrease:
Raven’s matrices (fluid intelligence)
Pattern comparison (mental speed)
Word span: (working memory)
Physical exercise can help prevent this
Thurstone’s theory of intelligence
based on statistical analysis of over fifty different cognitive tests, L.L / Thurstone found that test items tended to measure the following primary mental abilities:
Verbal fluency and verbal comprehension, reasoning and memory
Numerical and spatial performance ability
Perceptual speed
scoring high on one mental ability generally matched high scores on others, providing additional support for an underlying general intelligence factor
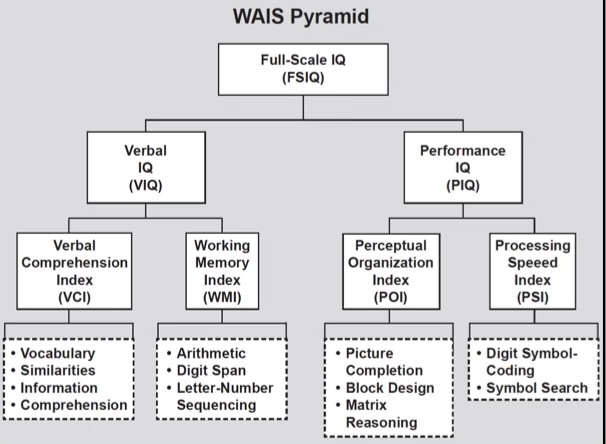
Modern intelligence testing
the WAIS (Wechsler Adult Intelligence Scale) is one of the most widely-used standardized IQ tests
IQ: an overall quantitative measure of an individual’s intelligence relative to that of other individuals
IQ distribution
About 95% of all people fall within 30 points of 100
13.5% between 70 and 85, and between 15 and 130, 34% between 85 and 100 and between 100 and 115
About 68% of people score 15 points above or below 100 (34% above and 34% below)
130 or greater = genuine
standard deviations from the mean who score below 70 can’t get death penalty
Reliability of intelligence test scores over the lifespan
test scores at age 11 predict the intelligence test score at age 80, (r=.66)
What does intelligence predict?
intelligence test scores are positively correlated with”
academic success
military performance - ASVAB score predicts subsequent performance in military services (ex. Qualifying for special forces, technical skills acquisition, performance ratings across career, medals earned)
Job success and income - the more complex the job, the more intelligence predicts success in that position
Health and longevity - higher score, better health and more long lived
What do twin and adoption studies tell about intelligence
identical twins reared together have similar intelligence scores
Lower correlations of identical twins reared apart shows that identical twins reared together shows some environmental effect
Intelligence correlation is lower between fraternal twins and other related siblings
Children and their birth parents have a much higher correlation in intelligence scores than children do with adoptive parents
Proposed theory of multiple intelligences
Howard Gardner argues that the deletion of intelligence is too narrow. He popularized the theory of multiple intelligences
Freud’s Conception of personality
argued that much of our personality is driven by unconscious processes.
The unconscious mind is a reservoir of thoughts, wishes, feelings, and memories that are hidden from awareness
He developed a therapy called psychoanalysis based on his theory of discovering one’s unconscious
Like an iceberg, most of the mind is hidden below the surface of our conscious awareness
Personality develops from the efforts of our Ego to resolve tension between our Id(unconscious energy) and our superego (internalized ideals)
Ego (mostly conscious; makes peace between the id and the superego)
Subconscious forces ego has defense mechanisms
Defense mechanisms: unconscious process employed to avoid anxiety-arousing thoughts or feelings
Big five traits of personality
Openness
Conscientiousness
Extraversion
Agreeableness
neuroticism

Fundamental attribution error
tendency to believe that someone else’s behavior is largely due to the person’s personality rather than the situation
Personality attributions are often made automatically, whereas situational attributions require more cognitive thought after weighing information about the context
Milgram’s study on obedience
Teacher was told that he was giving a test to a learner (who in this case was actually an actor). He was also told that he had to give them a shock whenever they got an answer wrong.
The shock increased in pain and intensity after each time a question was answered incorrectly
It got to the point where the shocks were unbearable, so the teacher protested throughout the experiment, not wanting to continue shocking the man
However the lab scientist told him to keep going and since the scientist was an authority figure to the teacher, the teacher listened to him
This study shows that a lot of people do things, especially bad, if they are ordered by a person of authority to do them
Findings: 65% of participants actually went to the end of the shock generator
Situational factors that contributed to obedience rates
Perception of authority figure
Authority is seen as legitimate
when 2 experimenters were present and one expressed concern, obedience decreased
Limited sources of information in a novel situation
Which contributed to a reliance on the supposed expertise of the experimenter
When observing others’ refusal to continue the experiment, obedience was reduced
Responsibility not assigned or diffused
Responsibility placed on experimenter (“just following orders”)
When a confederate gave the actual shock and participant took on role as ‘assistant’, obedience increased
The proximity and salience of the learner
The closer the “teachers’ were to the learner, physically and psychologically, the less likely they were to administer the maximum shock
Stanford prison study
A man named Zimbardo was the head of it
24 normal males were examined and half were randomly assigned as prison guards, the other half prisoners
Hostility escalated quickly
Prisoners had mental breakdowns
The study eventually (well actually quite quickly) had to be shut down
The people who were in the study were not acting, it was real
Similar abuse occurred at Abu Ghraib prison, but this was real and a lot more intense
Psychological factors that contribute to cruelty
Obedience - order to help “break the will, bend the resistance of the inmates” set up a norm that legitimized brutality; guards obeyed authority’s norm
In-group conformity - ‘Us vs. Them’ perception; institutional/group pressures to conform; no incentive for whistleblowers; led to guards to be complicit in order to maintain group camaraderie
Depersonalization and dehumanization - prisoners were stripped of their identity. They were categorized as a group and were viewed as animals; their poor hygiene triggered attitudes of disgust
Deindividuation of guards - due to elevated group identification and general heightened arousal of the situation. This undermined self-restraint. Acting impulsively while observing others during the same trapped some guards into a Mardi gras moment - getting lost in the moment without considering consequences
Comorbidity
people diagnosed with one psychological disorder are often diagnosed with other disorders
DSM-5
diagnostic and statistical manual of mental disorders which describes psychological disorders
The most recent version describes about 100 psychological disorders and also many subcategories and specifiers exists the exact number of official diagnoses is much larger
Phobias
marked by a persistent and irrational fear of an object or situation that disrupts behavior and is out of proportion to the actual danger that the object or situation poses.
The fear, anxiety, or avoidance lasts for 6 months or more
Affects 10% of population
Women are more frequently affected than men (2:1)
It is common for individuals to have multiple specific phobias
Approximately 75% of individuals with specific phobia fear more than one situation or subject
Social anxiety disorder
The individual fears that they will act in a way that will be negatively evaluated
Usual social situations: speaking in meetings or classes; attending social events or parties; introducing yourself to others; having conversations; making requests of others; eating and working in public
The social situation)s) are avoided or endured with intense fear,and often trigger anticipatory anxiety
The fear, anxiety, or avoidance lasts for 6 months or more
Prevalence rates are about 7% of US population
Onlya minority (about 10%) of self-identified shy-introverted individuals have symptoms that meet diagnostic criteria for social anxiety disorder
Generalized Anxiety disorder
excessive and uncontrollable anxiety and worry, occurring most days for at least 6 months, about a number of events and/or can often occur without any known ‘trigger’
Associated with following symptoms:
Restlessness or feeling on edge
being easily fatigued
Difficulty concentrating
Irritability
Muscle tension
Sleep disturbances
The constant worry causes impairments in social, occupational, or other important areas of functioning
About 3% prevalence rate
More excessive, propounded, chronic and interferes significantly with daily psychosocial functioning and frequently occurs without precipitants
non pathological worries of everyday life are more transient, fluctuate from day-to-day, may include a narrower range of concern, feel more manageable, and may be put off when more pressing matters arise
Everyday worries are also much less likely to be accompanied by physical symptoms
Obsessive-Compulsive Disorder
persistence of obsessions - unwanted anxious thoughts, images, or urges - that the individual attempts to ignore, suppress, or neutralize by engaging in compulsive behavior-ritualistic, repetitive behaviors or mental acts
The compulsions are clearly excessive and cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
About 1% prevalence rate
Post Traumatic Stress Disorder
exposure to actual or threatened death, serious injury, or sexual violence
Four primary symptom clusters (you need to have a symptom in each to be diagnosed) :
Intrusive symptoms - recurrent distressing memories of event; nightmares; cue-triggered flashbacks; intense distress at exposure to cues that resemble any aspect of trauma
Avoidance - complete avoidance of stimuli/cues/reminders associated with the traumatic event; dissociation/suppressing distressing memories/thoughts; social withdrawal
Negative alterations in cognitions/mood - persistent anxiety/anger/guilt; feelings of detachment; derealization; inability to experience positive emotions
Altered behavior and emotional reactivity - self-destructive behavior; sleep disturbance; difficulty with concentration; jumpiness, irritability; angry outbursts
Symptoms from all 4 clusters must be present for more than 1 month (if all symptoms are met but don’t last a month, then the diagnosis is ‘acute stress’ disorder)
Symptoms usually begin within the first few months after the trauma, although may be delayed expression (greater than 6 months)
Sex difference prevalence rates: men 5%, women 10%
Highest rates (ranging from ⅓ to more than ½ of those exposed) found among survivors of rape, military combat, and captivity, and ethnically or politically motivated by internment and genocide
Major Depressive Disorder
a disorder in which an individual experiences recurrent ‘major depressive episodes’, symptoms must be at least 2 consecutive weeks and they must be present most of the day, nearly every day
Average episode is about 5 months
At least one of these symptoms must be present:
Depressed mood
Markedly diminished interest or pleasure
The individual must have at least four of the following symptoms as well:
Significant changes in weight or appetite
Sleep disturbances - insomnia or hypersomnia
Significant ‘psychomotor’ abilities - agitation, fidgetiness, slowed movement, heaviness
Persistent fatigue
Negative thoughts/rumination
Diminished ability to think or concentrate, or indecisiveness
Recurrent thoughts of death
Bipolar Disorder
an alternation between depression and mania
Bipolar I - full manic episodes
Bipolar II - hypomanic episodes
Manic episode: symptoms must last at least 1 week and are often experienced with such severity that they impact work/school performance and may even require hospitalization
A hypomanic episode typically lasts 4-6 days, often with fewer or less severe symptoms
Manic episode symptoms:
Inflated self-esteem or grandiosity
Decreased need for sleep
Flight of ideas and racing thoughts
More talkative than usual or pressure to keep talking
Increase in goal-directed activity and non-goal-directed activity (psychomotor agitation such as pacing around one room uncontrollably)
Distractibility and/or inability to disengage from a task
Excessive involvement in risky activities that have a high potential for negative consequences - excessive shopping sprees, gambling, sexual indiscretions
Prevalence rate of bipolar disorder is about 2%
Schizophrenia
defined by abnormalities in the following 5 domains:
Disorganized thinking and speech: switching rapidly and randomly from one topic to another, responds to questions with nonsensical answers, speech may be incomprehensible
Delusions: fixed beliefs that are not amenable to change despite clear or reasonable contradictory evidence regarding their veracity
Persecutory delusions - most common type of delusion; belief that one is going to be harmed by an individual, organization, or other entity
Grandiose delusions - believes that he or she has exceptional abilities, wealth or fame; think that they are a famous individual
Hallucinations: occur in any sensory modality, but auditory hallucinations are the most common,usually experienced as voices, whether familiar, that are perceived as distinct from the individual's own thoughts
Grossly disorganized or catatonic behavior: significant alteration in behavior and movement
Complete lack of verbal and motor responses
Purposeless and excessive motor activity; repeated stereotyped movements
Maintaining a rigid, inappropriate or bizarre posture
General resistance to instructions or requests from others
Negative symptoms: - an absence of normal emotional experiences
Flat affect - diminished emotional expression
Inappropriate affect - laughing at inappropriate times, etc.
Avolition - a decrease in motivation or interest in pursuing purposeful activities
Asociality - the apparent lack of interest in social interactions
Anhedonia - loss of pleasure
Dysphoria - depressed mood
For schizophrenia diagnosis - symptoms must continue for at least 6 months
Prevalence rate about 1%
Typically emerges between the late teens and mid 30s; onset prior to adolescence is rare
Slightly more common in males than females (7:5), and men tend to show higher rates of negative symptoms and increased symptom-severity
Some individuals have absent insight- lack of awareness of their disorder
Absent insight is the most common predictor of non-adherence to treatment and risk of relapse