PSAX Doppler Protocol
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Gain, scale, box size, centering
What do we adjust when optimizing for colour Doppler
Alignment, baseline, scale, gain, sweep speed
What do we adjust to optimize for spectral Doppler
AV colour, TV colour, TV CW, PV colour, MV level
What Doppler images do we take in PSAX
Zoom
What also do we do to the AV colour image besides add colour to it
False, should see a bit around the AV too
T/F: the zoom on the AV should be tightly around the valve without any space around the valve so you can see it really well
True
T/F: sometimes aliasing in the AV is normal because of the high velocity flow through the valve
Diastole
When does AR occur
Systole
When does AS occur
Make sure to see the valve opening and don't center over the rib
What are some tips for the PSAX RV inflow image
TR
What are we assessing for when sweeping through the TV
Annulus
The colour box over the TV should be just as wide as the _________
More medial
Does TR usually show up more medially closer to the Av or more laterally closer to the edge of the image in the PSAX TV colour image
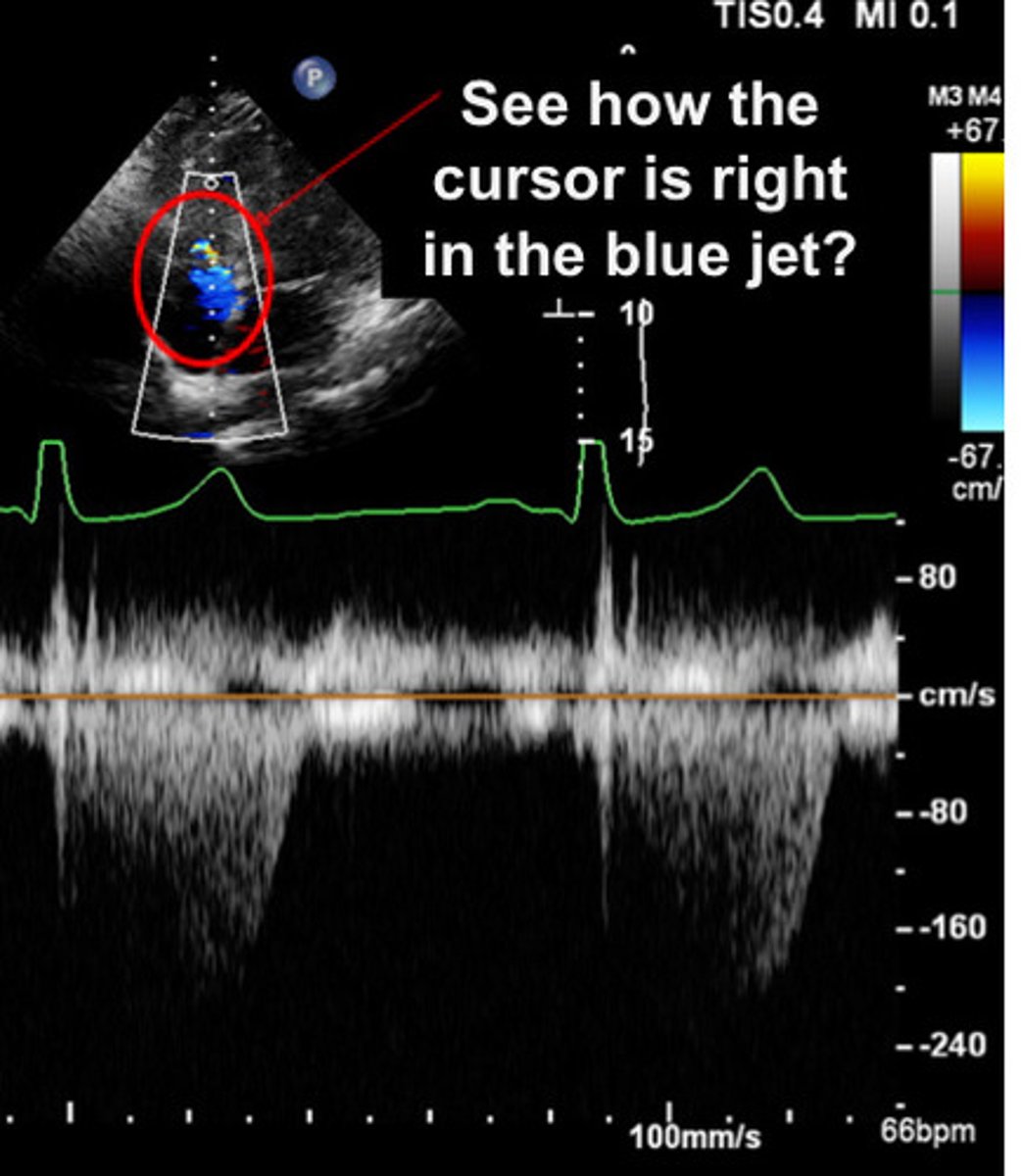
TR jet
What should the CW cursor be lined up to
2.4m/s
What should the scale be at for the TV CW
Parabolic jet
In the TV CW image, you will measure if a ____________ ____ is seen
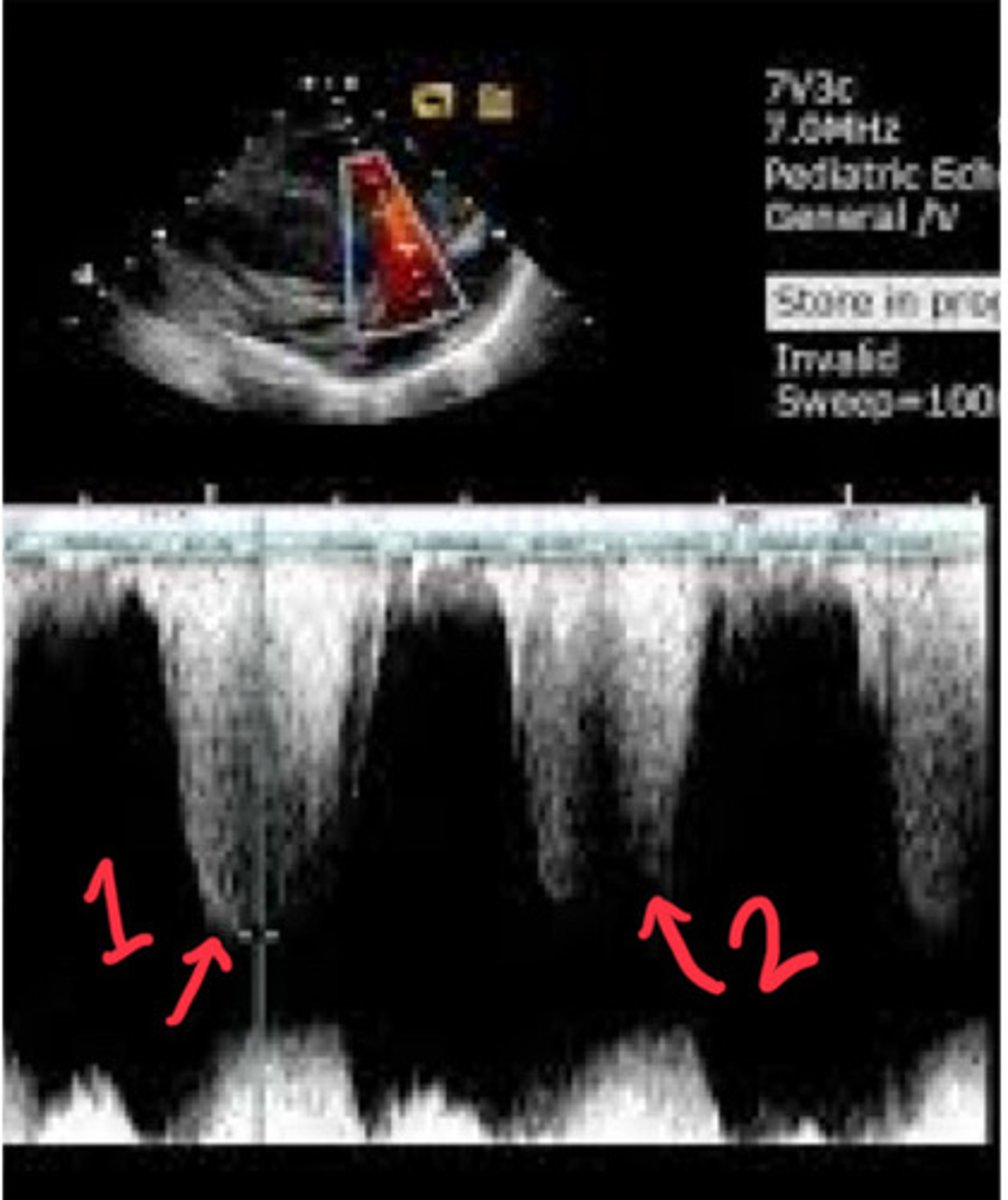
No
Would you measure this TR jet
No
Would you measure TR jet 2
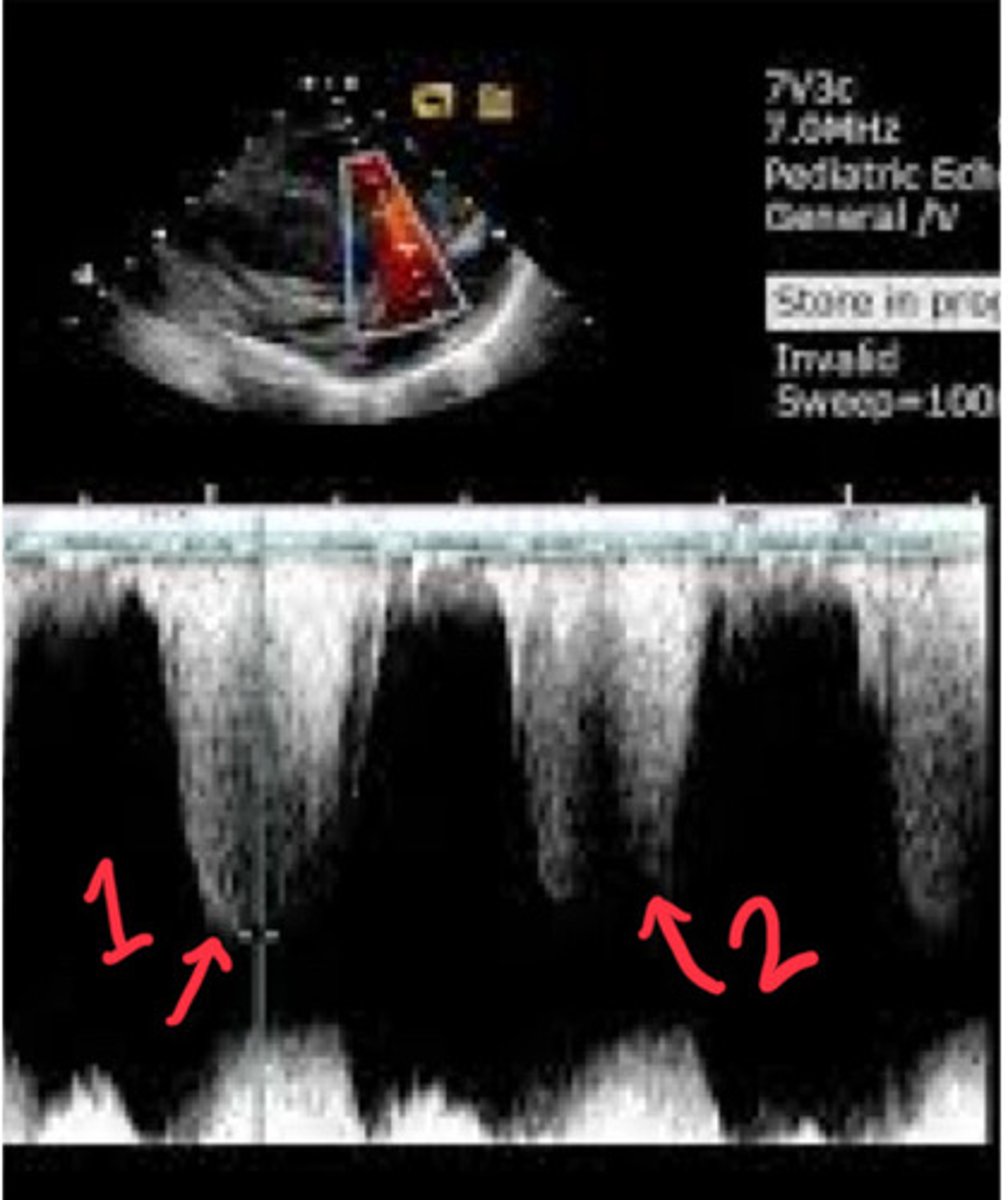
Because there difference in jets is just from the heart moving in and out of alignment
Why would you still measure jet 1 if the other jets are not measurable
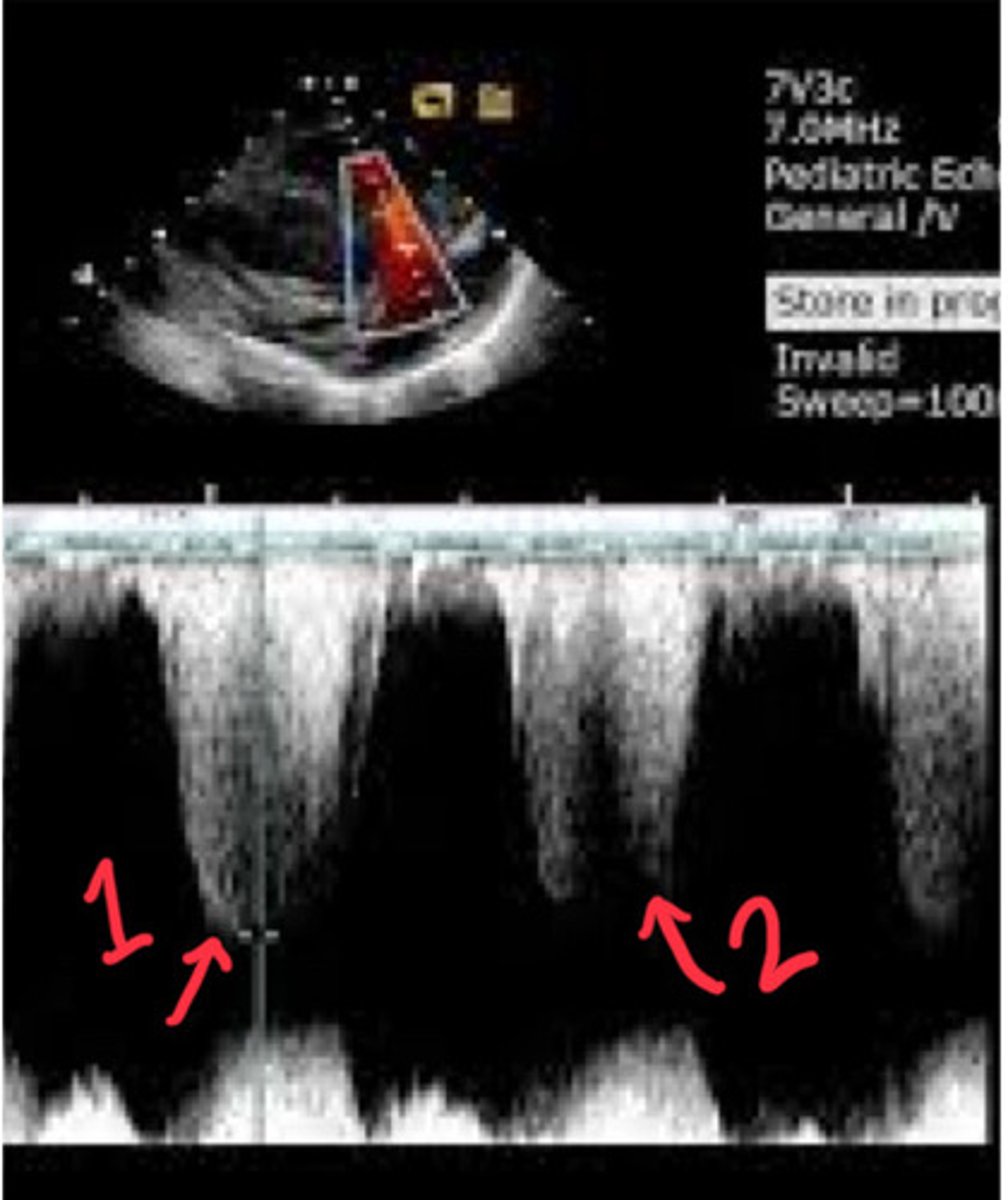
Yes
Would you measure TR jet 1
80%
Up to ____% of us have some TR
Just wide enough
The colour box for the PV should be _______ ________ _________ because the PV is a narrow valve
Red flame on the RVOT side of the PV
How is pulmonary regurgitation visualized on ultrasound in terms of colour Doppler
True
T/F: you may need to take 2 images at the PV, one showing the PV and one showing the birfurcation
Inferior and lateral
How does the MPA bifurcation usually sit compared to the PV
Little bit of aliasing and narrow jet
How would normal PR look like
Lot of aliasing, goes farther back into RV, and wide jet
What would abnormal PR look like
CW
What kind of spectral Doppler do we use on PR and PS
PW
What kind of spectral Doppler do we use on the RVOT
PR is higher velocities and RVOT are slower velocities
Why do we use different spectral Doppler on PR and RVOT
Within 5mm of that PV in the RV
Where should the sample volume be placed for the RVOT PW
Higher than mid
How should the baseline be placed for the RVOT PW
Closing click
What aspect of the PW waveform would suggest you are aligned correctly in the RVOT for the RVOT PW
Peak velocity or trace VTI
What do you measure in the RVOT PW image
True
T/F: you ignore any PR that shows up in the RVOT PW image
RV outflow velocity
What does the RVOT PW image assess
Forward
Optimization on the RVOT PW spectral should be done for _________ flow
Congenital abnormalities
What can suggest high velocity in the RVOT suggest
RV stroke volume calculation
What else can the RVOT PW peak velocity be used for
Peak velocity
What does you measure in the PV CW
Pulmonary regurg
What is flow 1 from in this CW PV
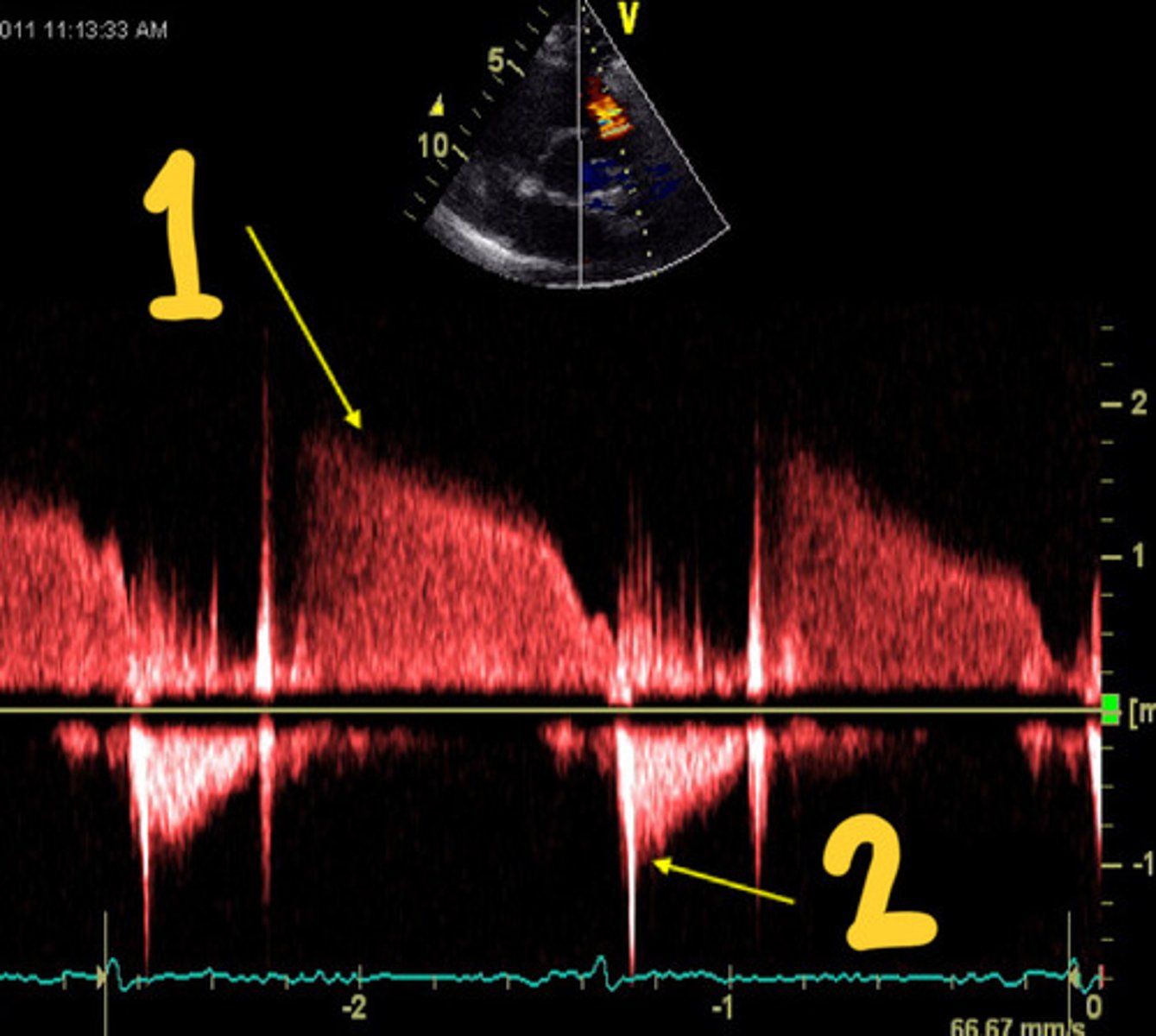
Pulmonary outflow
What is flow 1 from in this CW PV

Near the top
Where should the baseline be for the PV CW
Below the base line
Where is normal flow from the PV found
Pulmonary stenosis and regurgitation
What are we assessing for in CW PV
No
Should you have any flow through the MV when the valve is closed
True
T/F: if you see regurge in PLAX, you should also see it in PSAX
Eccentric
What is the nature of MR flow usually
Abnormal flow across the IVS
What are you looking for in colour IVS sweep
VSD
What does this flow through the IVS indicate
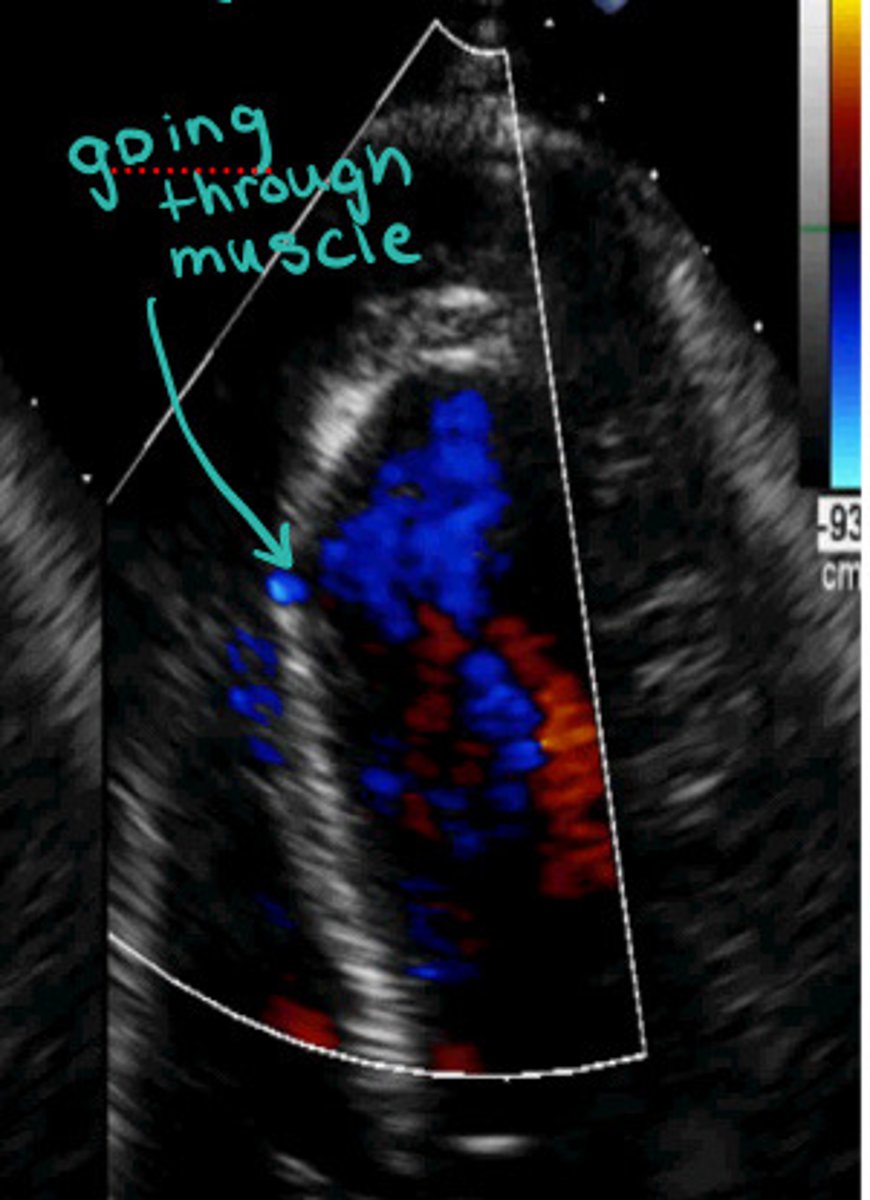
Ventricular septal defect
What does abnormal flow across the IVS indicate
Base to apex
How do you sweep the IVS