Traumatic Dental Injuries
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
types of dental trauma
-crown fracture
-root fracture
-alveolar fracture
-luxation
-avulsion
dental trauma- history
-when
-how
-where
-whom (many cases go somewhere else first (dentist, ER, etc.)
-is the patient alert?
-tetanus shot
-other meds
dental trauma- extra-oral exam
-extra-oral swelling
-lacerations- see if opposing incisors are fractured if lip laceration (fragment may be embedded)
-asymmetry
dental trauma- intra-oral exam
-displacement
-mobility of the tooth
-is crown intact?
-is pulp exposed?
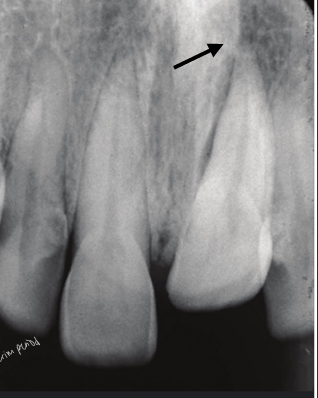
dental trauma- radiographs
-status of root development
-root displacement
-root fracture (take CBCT- likely to see transverse and narrow fractures that may not be caught on 2D radiograph)
dental trauma- clinical tests
-percussion
-palpation
-pulp sensibility tests- baseline→ checking for neural response, doesn’t really tell if vascular supply of pulp has been damaged (no way to assess this currently)
dental trauma- summarizing findings
-history of incident
-soft tissue exam
-status of tooth:
-mobility
-displaced
-pulp exposed
-root mature/immature
-baseline pulp testing
-baseline perio testing
dental trauma- concept #1
-do we need to preserve the pulp?
-radiograph is answer
-mature root: remove pulp (no need to preserve)
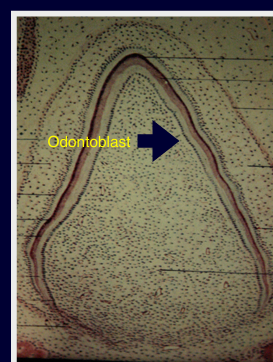
-immature root: will arrest further development of dentin if removed (will be removing odontoblasts), want to preserve the pulp
concept #2
-do we need to splint?
-no, unless there is mobility, displacement, or primary occlusal trauma
-always use flexible splints
splint time guidelines
-avulsions: 1 week
-luxation: 2 weeks
-root/alveolar fractures: 4 weeks
concept #3
-do we anticipate future complications?
-ankylosis: protracted splinting could lead to ankylosis, factor of the degree of damage to PDL and cementum- greater trauma = greater damage
-resorptions: replacement resorption from osteoclasts
-pulp necrosis: most common, osteoclasts accelerate resorptive process of reimplanted teeth by accelerating inflammatory process
crown fracture- concussion
-no response to cold test
-absence of neural response up to 3 months (can come back)
-do nothing, observe
uncomplicated crown fracture
-enamel-dentin
-restorative procedures to treat
complicated crown fracture
-enamel-dentin-pulp
-apply concept 1: if root mature then remove the pulp/RCT, if root immature then preserve radicular pulp tissue

apexogenesis
-vital pulp therapy performed to encourage continued physiological root development and apical closure
-do a pulpotomy by taking out coronal pulp tissue and placing bioceramic cement on pulp stump
-takes ~24-36 hours for bioceramic cement to set- does not irritate the pulp, medically seals the pulp from contaminatory saliva
-over 6-8 months, bring patient back for recall
-calcific bridge should form from immune competent cells → rest of root able to develop
-helps to preserve ridge
apexification
-a method to induce a calcified barrier in an immature root with a necrotic pulp
-place calcium hydroxide → promotes cells in PA space to grow in from the bottom, will get barrier to form at apex
-change calcium hydroxide a couple times, will require recall

horizontal root fractures
-the more apical the fracture, the better the prognosis
-more apical means being more walled-off from the oral environment
-apical segment: blood supply maintained, never a problem
-coronal segment at risk: mobility, splint required for 4 weeks, RCT not needed (just observe)
-when coronal pulp necroses, see if you can reposition the segment and splint, or can do RCT on the coronal segment only
-if apical segment starts trouble, just do apicoectomy to treat
cervical root fracture
-outcome/treatment will depend on age of patient
-adult: don’t worry, can extract and implant
-child/adolescent: don’t want to extract- could compromise the alveolus; want to preserve the root, extract coronal segment, bury root under bone and use retention (essix retainer) for esthetics, when pt turns 18 could do implant then since the ridge will have been preserved

crown-root fractures
-poor restorative outcome

alveolar fracture
-refer to OMFS
-whole section moves in a mass
-splint 4 weeks
-don’t do RCT
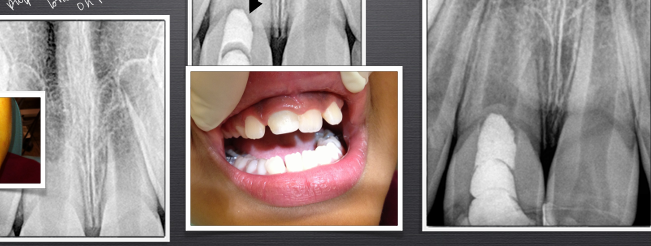
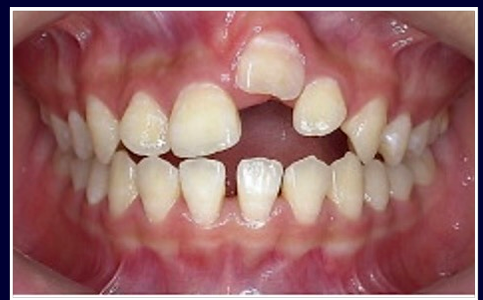
luxation injuries
-displacement of a tooth from its original position in the alveolus without total avulsion
-lateral luxation (buccal/palatal), intrusive luxation, extrusive luxation
-assess degree of displacement, reposition, splint, check vitality
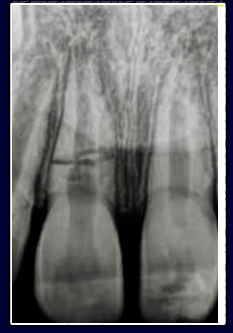
intrusive luxation
-can crush neurovascular bundle
-wait ~2-3 weeks to re-erupt
-get ortho consult right away in case re-eruption does not occur
intrusive luxation on primary teeth
-CBCT useful
-if no imminent damage to permanent tooth germ, wait 2-6 months to erupt
-if tooth germ damaged, must extract tooth
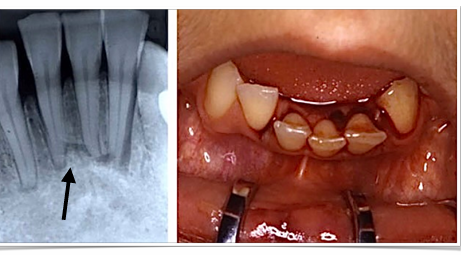
avulsion
-tooth completely out of socket
-unknown variables
-pulp necrosis, ankylosis, root resorption concerns
ankylosis following avulsion
-directly related to the damage of the PDL
replantation after avulsion
-extra-oral dry time <20 minutes
-critical to replant tooth into socket ASAP (doesn’t realistically happen)
-storage medium: saline, milk, saliva
-flexible splint 1-2 weeks
-may minimize ankylosis
avulsion in young permanent teeth
-replant and observe
-open apex = chance for revascularization to occur

avulsion with mature root
-replant, immobilize with flexible splint, then initiate RCT one week later
avulsion treatment goals
-preserve the PDL FIRST (minimizes resorption)
-then treat pulp
avulsion treatment
-initiate RCT one week later
-place calcium hydroxide (pH 12.4)
-calcium hydroxide alters the pH of the external root surface and may necrose the PDL fibers trying to re-attach themselves
-RCT one week later (fate of PDL decided in the first week after avulsion)
-minimum 1 week to 6 months in calcium hydroxide

avulsion- external inflammatory root resorption
-immediate complication

ankylosis
-decoronation
-remove anything in canal
-bury root 2-3mm into alveolus
-hoping to have blood clot form coronal to root and bone to form coronal to root
-hope bone will grow in tandem with adjacent teeth (height of gingiva/ridge maintained) so an implant can later be placed in site