small animal med- GI objectives
1/260
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
261 Terms
what clinical signs are indications for in depth diagnostics?
-depression or weakness
-abdominal distension/organomegaly/mass
-anorexia, weight loss
-marked dehydration
-mucus membrane abnormalities (congestion, pallor, petechiation)
-tachycardia/poor pulse quality/arrhythmias
-fever
-melena/severe hematochezia
-pain
-chronicity
-lack of response to symptomatic therapy
-progression/worsening of clinical signs in face of symptomatic therapy
what are characteristics of large bowel diarrhea?
-hallmarks of large bowel: tenesmus, mucus in stool, hematochezia
-melena is absent
-normal to decreased stool volume
-increased defecation frequency
-weight loss is uncommon
-occasional vomiting
-stool quality: no undigested fat or food
what are characteristics of small bowel diarrhea?
-no tenesmus, mucus in stool, hematochezia
-melena may be present
-normal to increased stool volume
-normal to mildly increased defecation frequency
-weight loss is common with chronicity
-vomiting is common
-stool quality: fat, undigested food possible
what causes anemia of chronic disease?
caused by anything that increases cytokines (this causes suppression of RBC production)
what are characteristics of anemia of chronic disease?
mild, normocytic, normochromic nonregenerative anemia
what is a cause of regenerative anemia due to GI disease?
acute blood loss (like due to parvovirus, acute hemorrhagic diarrhea)
what are characteristics of regenerative anemia?
mild/moderate/severe macrocytic, hypochromic, regenerative anemia
what are GI causes of iron deficiency anemia?
due to chronic blood loss (chronic disease!!)
what are characteristics of iron deficiency anemia?
mild to severe microcytic hypochromic nonregenerative anemia (because iron is necessary for RBC production)
what abnormalities on a biochem profile can be found in pets with GI and/or pancreatic disease?
-elevated BUN
-hypocholesterolemia
-hypocalcemia
-panhypoproteinemia
what are causes of elevated BUN seen with GI/pancreatic disease?
-overt GI bleed (digested protein (hemoglobin) is converted to urea)
-dehydration
what are causes of hypocholesterolemia seen with GI/pancreatic disease?
due to malabsorption and maldigestion
what are causes of hypocalcemia seen with GI/pancreatic disease?
due to vitamin D malabsorption (dogs get all their vitamin D from the diet)
what are causes of panhypoproteinemia seen with GI/pancreatic disease?
hypoalbuminemia and hypoglobulinemia→ protein losing enteropathy (PLE)
what is the basic physiology behind hypochloremic metabolic alkalosis?
loss of hydrogen chloride (HCl)--> retention of bicarbonate to maintain electroneutrality
what are clinical signs that result in hypochloremic metabolic alkalosis?
severe, frequent vomiting
-->due to upper GI obstruction, and/or gastric stasis
what is the basic physiology behind hyperchloremic metabolic acidosis?
loss of bicarbonate -->retention of chloride with hydrogen to maintain electroneutrality
what are clinical signs that result in hyperchloremic metabolic acidosis?
1. diarrhea (most common) ---> diarrhea will be bicarbonate rich
2. vomiting pancreatic/intestinal secretions rich in bicarbonate
what are the 5 main bacterial enteropathogens in dogs and cats?
1. Clostridium perfringens
2. Clostridium difficile
3. Camplyobacter jejuni
4. salmonella
5. e. coli
how are clostridium perfringens infections diagnosed?
isolation alone (culture/PCR) cannot be used to diagnose
need PCR detection of c. perfringens toxin genes
how are clostridium difficile infections diagnosed?
isolation alone cannot be used for diagnosis
diagnosis requires positive result for both:
-organism detection (culture, antigen, ELISA, PCR)
-toxin A and B detection by ELISA/PCR
how are campylobacter jejuni infections diagnosed?
fecal culture or PCR
how are salmonella infections diagnosed?
fecal culture or PCR
when should testing for bacterial enteropathogens be considered?
1. dogs and cats with acute onset bloody diarrhea that fails to respond to supportive care
2. dogs and cats with diarrhea and fever
3. diarrhea outbreaks occurring in multiple animals (+/- people) in densely populated shelter or kennel environment
when is treatment for bacterial enteropathogens warranted?
treat only when animals manifest systemic signs of illness that fail to respond to supportive care
why should you wait until animals manifest systemic signs of illness that fail supportive care to treat for bacterial enteropathogens?
most bacterial enteropathogens are associated with self-limiting diarrhea
injudicious administration of antimicrobials could be more harmful than beneficial
what is the recommended treatment for clostridium infections?
abx: metronidazole, amoxicillin
fecal transplants for c. difficile
what is the recommended treatment for camplyobacter infections?
fluoroquinolones
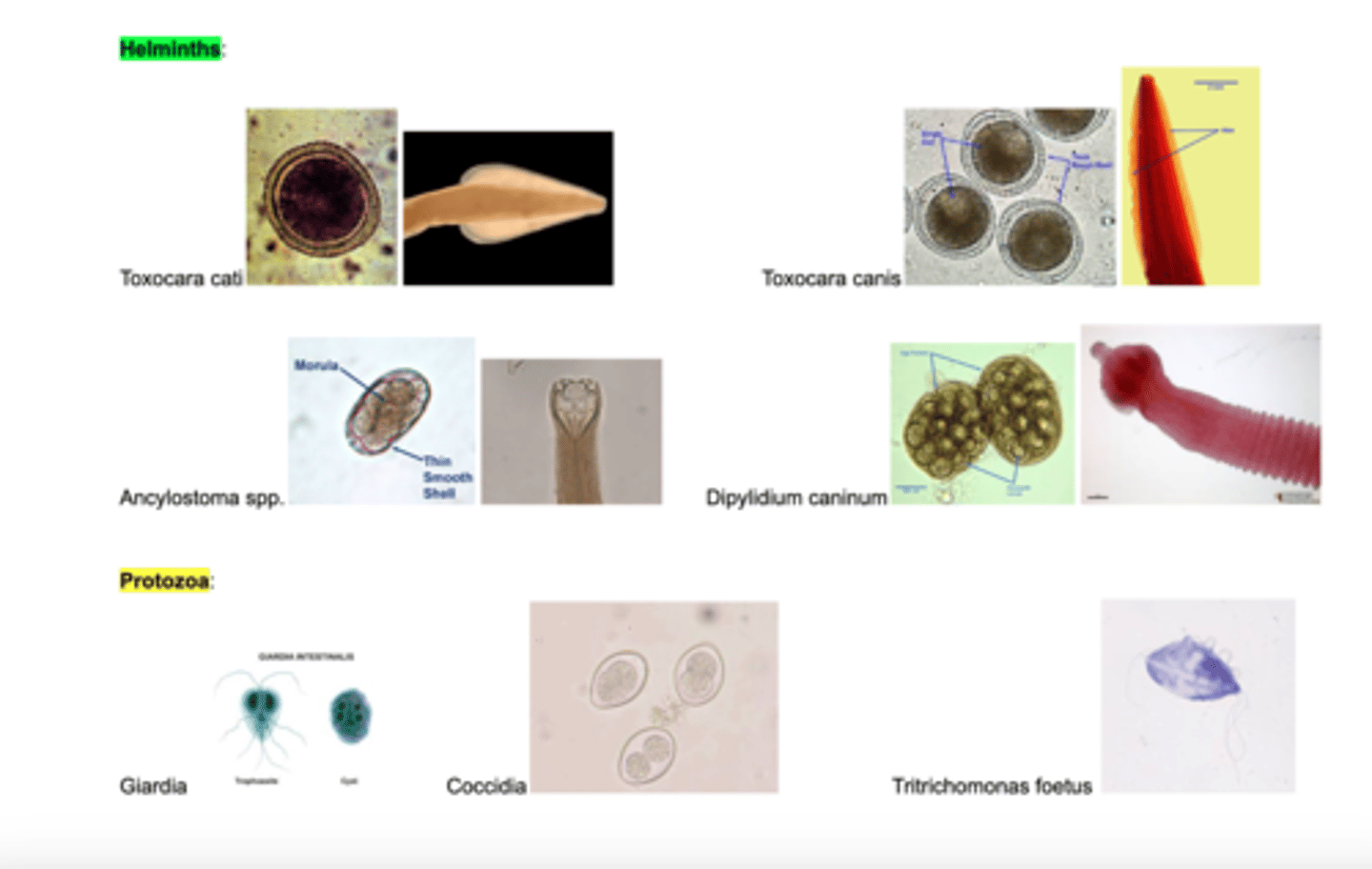
which endoparasites can fecal smears (wet mounts) ID?
used to ID protozoan oocysts and trophozoites of giardia, and trichomonas foetus
which endoparasites can fecal flotations with centrifugation ID?
most commonly used test- detects giardia cysts and wide variety of helminths
centrifugation and zinc sulfate flotation improves sensitivity
which endoparasites can fecal sedimentation ID?
preferred test to look for trematode ova (heterobilharza)
what does the giardia/crypto ELISA/IFA test detect?
detects fecal antigen, high sensitivity and specificity
which test is used to ID tritrichomonas foetus?
visualization of trophozoite on direct wet mount
must differentiate from giardia→ only difference is how they move
also used: pouchTF culture, fecal PCR
how can tritrichomonas and giardia be differentiated?
giardia: moves like a falling leaf
trich: jerk-y movements
what are the most common endoparasites in dogs and cats?
1. helminths (roundworms, hookworms, tapeworms, whipworms)
2. protozoa (giardia, coccidia, tritrichomonas foetus)
where is folate (vitamin B9) absorbed in the GI?
proximal small intestine by folate carriers
what are GI causes of folate (vitamin B9) deficiencies?
chronic duodenal diseases leads to hypofolatemia (malabsorption, depleted folate stores)
what is elevated serum folate concentration a marker of?
dysbiosis (some bacterial species can synthesize folate)
where is cobalamin absorbed in the GI?
ileum (distal small intestine)
what are GI causes of serum cobalamin (vitamin B12) deficiencies (hypocobalaminemia)?
1. chronic distal small intestinal (ileum) disease
2. surgical removal of ileum
3. exocrine pancreatic insufficiency
what is the MOA of proton pump inhibitors?
binds irreversible to H+/K+ ATPase pump of parietal cell, most effective suppression of gastric acid
what are indications of proton pump inhibitor use?
-prevention of reflux esophagitis secondary to gastroesophageal reflux
-documented or strong suspicion for gastric or esophageal ulceration
what is the MOA of H2-blockers?
block histamine receptor on parietal cells (famotidine)
what are indications of H2-blocker use?
-prevention of reflux esophagitis secondary to gastroesophageal reflux
-documented or strong suspicion for gastric or esophageal ulceration
what is the MOA of sucralfate?
polymerizes with protein in damaged mucosa in presence of HCl
what is the MOA of misoprostol?
synthetic prostaglandin analogue. Inhibits gastric secretion by inhibiting cAMP
-increases production of gastric mucus and bicarb
-increases epithelial cell turnover to promote healing
-increases mucosal blood flow
what are indications for misoprostol use?
-NSAID associated ulcers
-ulcers refractory to PPIs
-not for effects of steroid-associated ulcers
what are contraindications of misoprostol use?
pregnant animals, caregivers that are pregnant
what is the MOA of maropitant?
inhibits substance P binding to NK-1 receptor in vomiting center, CTZ, and enteric plexus of gut
what are indications of maropitant use?
FDA approved as antiemetic in dogs, and motion sickness at high doses
what is the MOA of ondansetron?
serotonin 5HT3 receptor antagonists, antiemetic (blocks vomiting mediated at the CTZ), reduces signs of nausea
what is the MOA of metoclopramide?
blocks dopamine D2 receptors in CTZ, 5-HT3 antagonism at high doses, also a pro-kinetic/promotility
also a weak 5-HT4 receptor agonist
what are indications for metoclopramide use?
vomiting induced by a wide variety of blood-borne and peripheral causes
good for delayed-gastric emptying disorders
what is the MOA of cisapride?
5-HT4 receptor agonist (increases motility from stomach to colon)
what are indications for cisapride use?
good choice for megacolon/constipated pets due to effects on colonic motility:
-gastroesophageal reflux
-megacolon/constipation
what is the MOA of mirtazapine?
antagonism of serotonin 5-HT3 receptors in CRTZ (antiemetic), MOA for appetite stimulation is unclear
what are indications of mirtazapine use?
management of weight loss in cats, appetite stimulant, antiemetic, sedative, anxiolytic
what is the MOA of capromorelin?
ghrelin analogue (growth hormone secretion and appetite stimulation)
-entyce in dogs
-elura in cats
what is the MOA of metronidazole?
bacteria need to activate intracellularly
-metabolite damages DNA
-activation only occurs in anaerobes and protozoa
what are indications for metronidazole use?
-anaerobic infections
-tritrichomonas
-giardia (?) → high doses required
-hepatic encephalopathy
-inflammatory bowel disease/abx responsive diarrhea (?)
Not recommended for acute diarrhea
what is the MOA of tylosin?
a macrolide antibiotic, bacteriostatic +/- cidal
inhibits 50S ribosome
what are indications for tylosin use?
-excellent for gram positive bacteria
-prokinetic
-motilin-like effect (helps with ileus)
-tylosin-responsive diarrhea
-pyoderma
-upper and lower respiratory infections
what is the MOA of polyethylene glycol 3350?
osmotic laxative or bowel cleanser prior to colonoscopy
what are indications for polyethylene glycol 3350 use?
-PEG3350 with added electrolytes: used for bowel cleansing or given as CRI for severe constipation
-PEG3350 oral powder (Miralax): used for management of constipation
what antibacterial drugs are used for GI disease?
tylosin, metronidazole, amoxicillin most common
should not be used routinely for uncomplicated acute diarrhea
what are indications of using antibiotics to treat GI disease?
-parvovirus infection with neutropenia
-acute hemorrhagic diarrhea syndrome (AHDS) with signs of sepsis
-antibiotics-responsive diarrhea trial (after appropriate workup and diet trial)
-e. coli associated granulomatous colitis (boxers and frenchies)--> based on FISH
-enteropathogenic bacteria with signs of systemic illness (ie, fever)
what are contraindications of using antibiotics to treat GI disease?
-uncomplicated acute diarrhea
-AHDS without signs of sepsis
-antibiotic-responsive diarrhea trial (before workup and diet trial)
-chronic large bowel diarrhea (instead of workup)
-enteropathogenic bacteria in nonclinical cases or mild, self-limiting disease
what are indications for probiotic use?
-acute uncomplicated diarrhea
-prevention and treatment of stress diarrhea
-prevention of antibiotic associated GI signs
-adjunct therapy for chronic enteropathies
what is the appropriate use of probiotics?
-prefer high dose, multi-strain probiotics for chronic enteropathies
-probiotics and antibiotics should be administered at least 4 hours apart
-need 1-3 days to infer a health benefit
what are the 3 clinically meaningful categories of fiber?
fermentability, solubility, and viscosity
what does fermentability of fiber describe?
readily metabolized by the gut bacteria (prebiotics)
what does solubility of fiber describe?
soluble fiber: dissolves in water
insoluble fiber: does not dissolve in water (non-fermentable, bulks stool)
what does viscosity of fiber describe?
thickens in the presence of water
what are the indications of fecal microbial transplantation (FMT)?
-antibiotic-associated diarrhea/dysbiosis
-acute diarrhea
-clostridium difficile infection
what are highly digestible, low residue foods (GI diets)?
relatively low in soluble fiber to promote stomach emptying and high in complex carbohydrates
low residue= low fecal bulk (very digestible)
what are indications for highly digestible, low residue foods (GI diets)?
-used for treatment of non-specific acute gastroenteritis cases
-pancreatitis
-gastric retention disorders
-lymphangiectasia (and hypertriglyceridemia)
what are 3 categories of elimination (hypoallergenic) diets?
1. hydrolyzed: protein source broken down into peptides
2. limited ingredient/novel protein: protein source the pet has never been exposed to
3. elemental: protein source consists of amino acids
what are indications for elimination (hypoallergenic) diets?
-chronic inflammatory entropathy
-atopy (skin allergies)
-feline triaditis (chronic pancreatitis, cholangitis, enteropathy)
what are fiber enhanced diets?
rich in insoluble or soluble fiber:
-soluble fiber preferred for small intestinal or pancreatic disease(helps improve microbiome)
-insoluble fiber preferred for weight loss, colitis, anal sack disease (bulks stool, helps express anal glands)
what are indications for fiber enhanced diets?
-hronic small bowel diarrhea (first choice is hypoallergenic diet)
-acute or chronic large bowel diarrhea
-constipation
what is the oropharynx?
caudal portion of oral cavity
what are the boundaries of the oropharynx?
Soft palate (dorsal)
Root of tongue (ventral)
Tonsillar fossae (lateral)
what is oropharyngeal dysphagia?
difficulty with prehension and abnormal transport through the upper esophageal sphincter
what are clinical signs of oropharyngeal dysphagia?
occur while eating:
-retching, gagging, repeat swallowing, food coming from nose
-exaggerated swallowing movements and foods will usually drop from mouth within seconds of prehension
what is esophageal dysphagia?
abnormal transport of bolus through the esophagus and lower esophageal sphincter into the stomach
what are functional causes of oropharyngeal dysphagia?
secondary to neurologic or muscular disturbance (neuromuscular disease)
if cannot keep down liquids, suspect functional disease
what are structural causes of oropharyngeal dysphagia?
stricture, traumatic injury, foreign bodies, neoplasia
if cannot keep down solids, suspect structural disease
what history should you obtain in patients with suspected dysphagia?
-age of onset (congenital vs acquired)
-frequency of signs (static vs progressive)
-duration of signs (acute vs subacute vs chronic)
-temporal pattern (if immediately after eating or hours after)
-difficulty with liquids vs solids
-recent doxycycline or anesthesia
-weakness, painful or stiff gait, exercise intolerance (polymyositis)
what should you include in your PE in patients with suspected dysphagia?
-palpation of pharynx and neck for masses, asymmetry, pain
-thoracic auscultation (aspiration pneumonia?)
-look for muscle atrophy, especially around head
-full neuro exam
-sedated laryngeal exam with doxapram (respiratory stimulant) and sedated oral exam
-watch pet eat food/liquid
what are abnormal findings on radiographs that may suggest dysphagia?
-dilated esophagus
-mass effect
-metallic foreign body
-air pockets (anaerobic bacteria)
normal: air filled pharynx
how is contrast radiography helpful for diagnosing dysphagia?
looks for structural causes of dysphagia in esophagus
start with lateral cervical and 3-view chest rads, then give contrast (avoid sedation)
--> repeat right lateral views soon after swallowing contrast
what is the best and only test to evaluate functional causes of dysphagia?
barium contrast videofluoroscopy
how are barium contrast videofluoroscopy studies performed?
-fast for 12 hours
-survey rads of thorax/cervical region to rule out gross abnormalities
-give 3 foods with contrast: liquid, slurry, kibble
-visualize prehension of food, swallowing, esophageal motility
how is endoscopy used to diagnose causes of dysphagia?
look for esophageal disease, foreign bodies, strictures
what is cricopharyngeal dysphagia?
congenital or acquired neuromuscular disorder of upper esophageal sphincter
what is the pathophysiology of cricopharyngeal dysphagia (achalasia vs asynchrony)?
failure of the UES to relax (achalasia) OR
lack of coordination between the UES relaxation and pharyngeal contraction (asynchrony)
can clinical signs distinguish between achalasia and asynchrony?
no
how is the cause of cricopharyngeal dysphagia diagnosed?
swallow contrast videofluoroscopy
when diagnosed, rule out myopathy or polyneuropathy:
-Myasthenia gravis
-Autoimmune myositis and muscular dystrophy
-Exclude hypothyroidism
what is the treatment for cricopharyngeal dysphagia?
-surgical myotomy of cricopharyngeal muscle (unilateral)
-injection of botulinum toxin into muscle
-gastrotomy tube
what are the key features of vomiting?
-disease in stomach or upper small intestine (or non-GI)
-forceful expulsion of stomach contents
-preceded by retching, vocalization, abdominal heaving