Benign Scrotal and Testicular Disorders
1/8
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
9 Terms
What are the Layers of the Scrotum
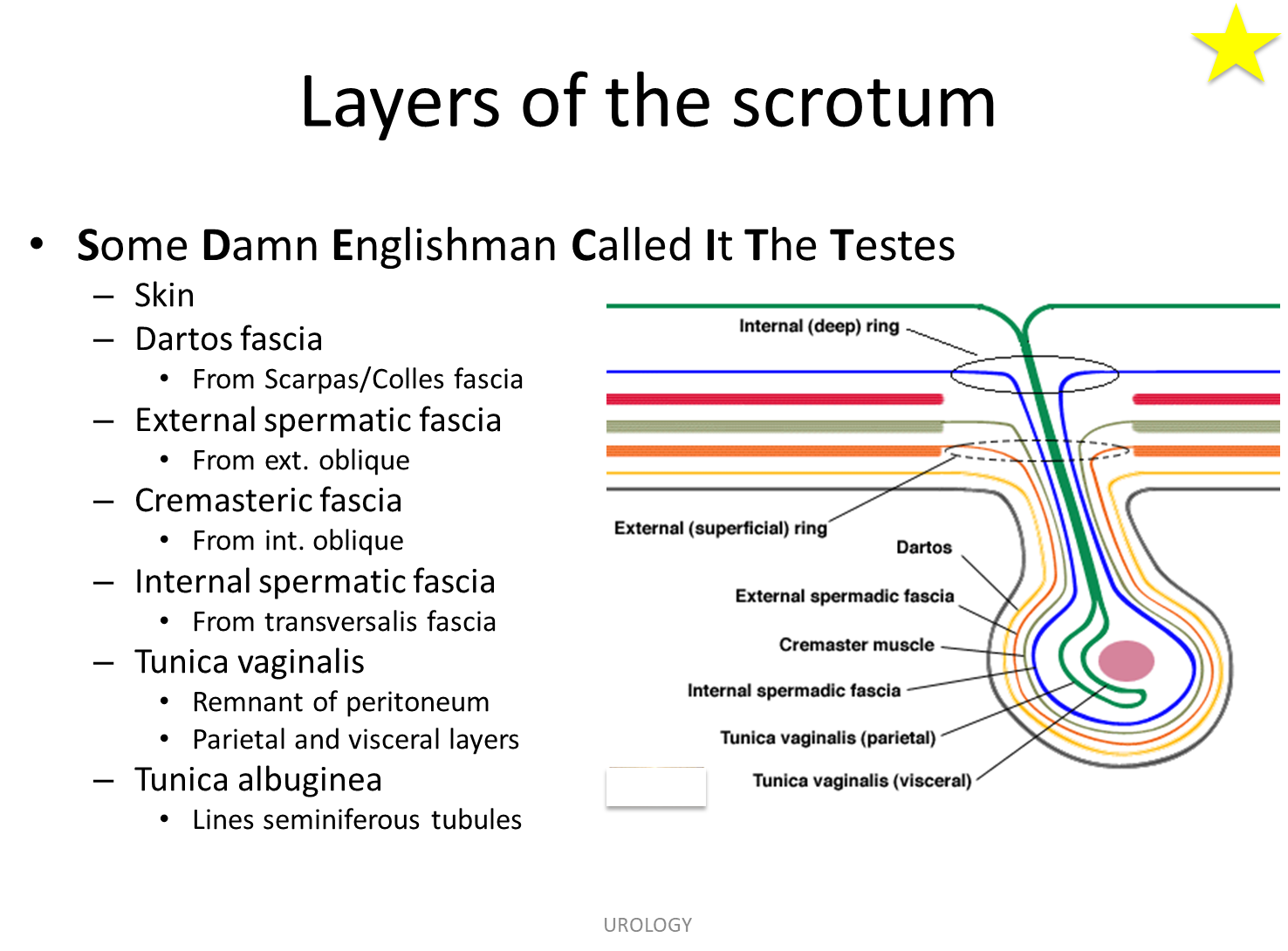
the layers of the scrotum can be named based on: Some Damn Englishman Called It The Testes
1) Skin
2) Dartos Fascia
→ an extension from the Scarpas Fascia into the Colles Fascia
3) External Spermatic Fascia
→ originates from the external oblique from the abdomen
4) Cremasteric Fascia
→ originates from the internal obliques from the abdomen
5) Internal Spermatic Fascia
→ from the transversalis fascia
6) Tunica Vaginalis
→ remnant of the peritoneum
7) Tunica Albuginea
0> lines the seminiferous tubules
What is the difference in nerve, vascular, and lymphatic supply to the testes vs scrotum?
Arterial Supply
→ testicles come directly from the aorta whereas the scrotum is supplied by the internal and external pudendal
Venous Drainage
→ the left testicle drains into the left gonadal vein to the left renal vein to the IVC
→ the right testicle drains into the right gonadal vein directly into the IVC
Nervous System
→ testicle is the genital branch of the genitofemoral nerve
→ scrotal skin is from the anterior and posterior scrotal nerves as well as the genital branch of the genitofemoral nerve
Lymphatic Drainage
→ testicles go to the para-aortic lymph nodes
→ scrotum go to the inguinal lymph nodes
What is Varicocele?
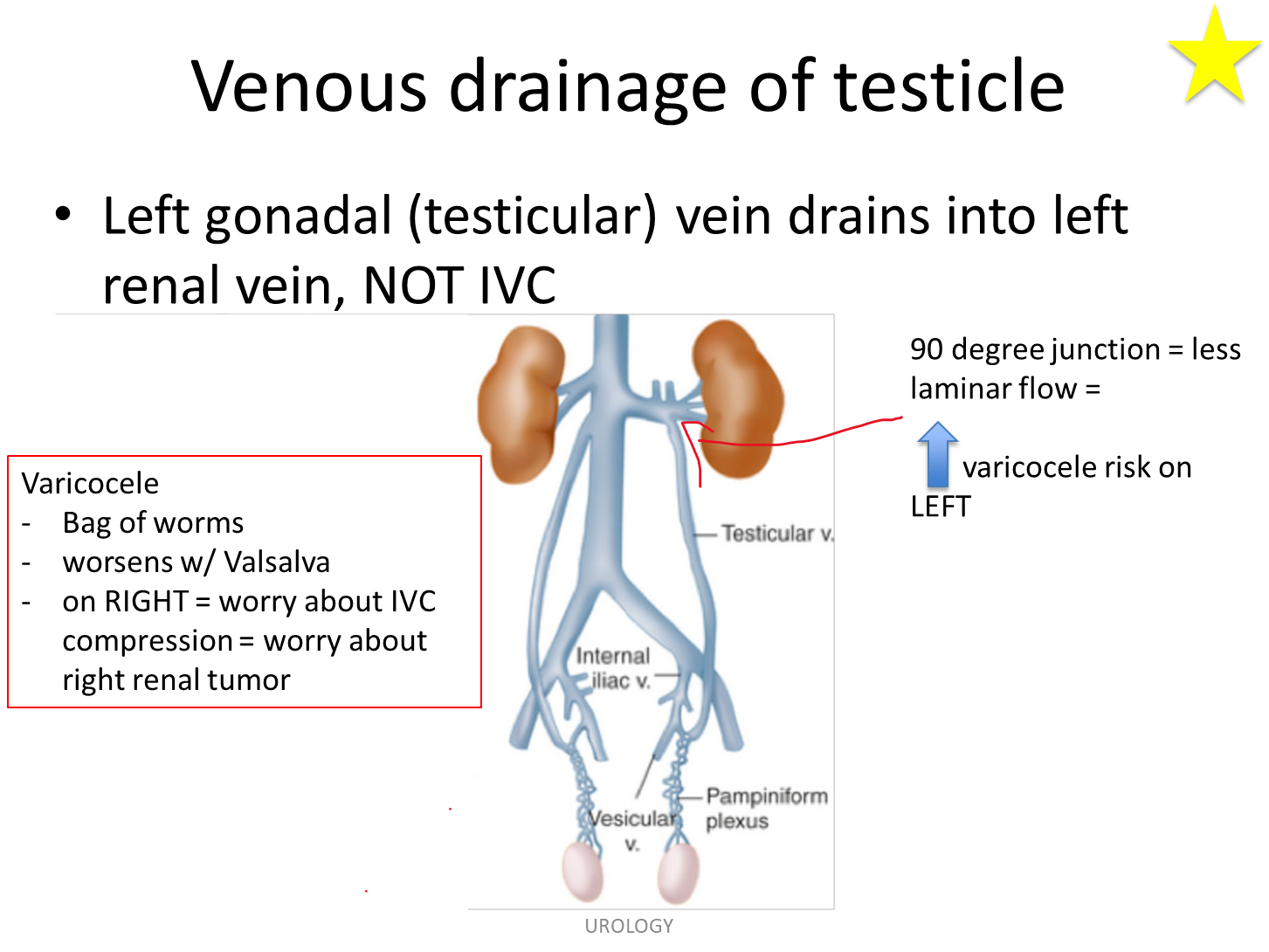
Varicoceles are dilation of the pampiniform venous plexus in the spermatic cord and is often described as a bag of worms above the testicle
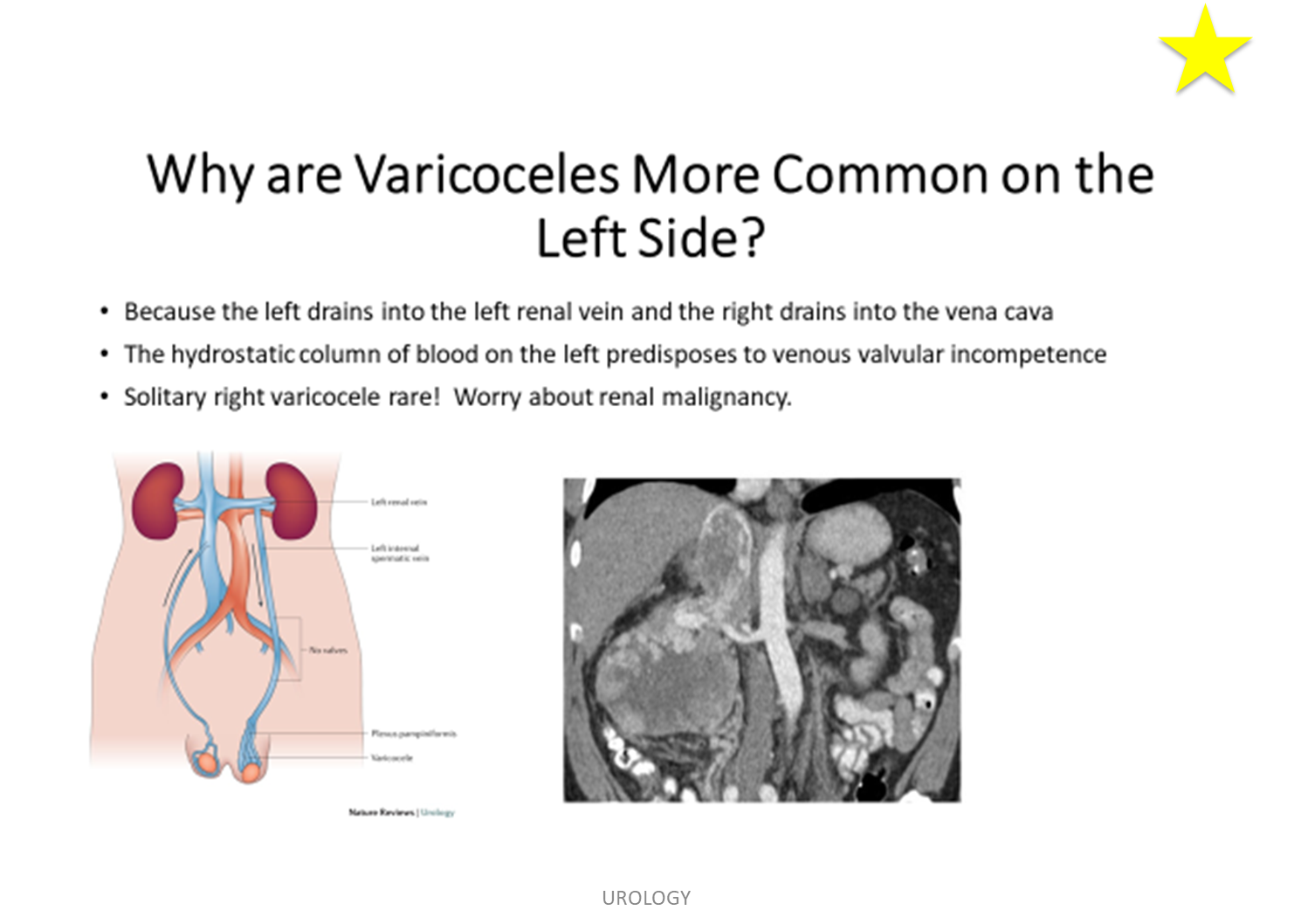
1) It is far more common on the left side due to the left gonadal vein’s drainage pattern into the left renal vein at a 90 degree angle
2) varicoceles on the right should raise concern for IVC compression often due to a right renal tumor
What is Hydrocele?
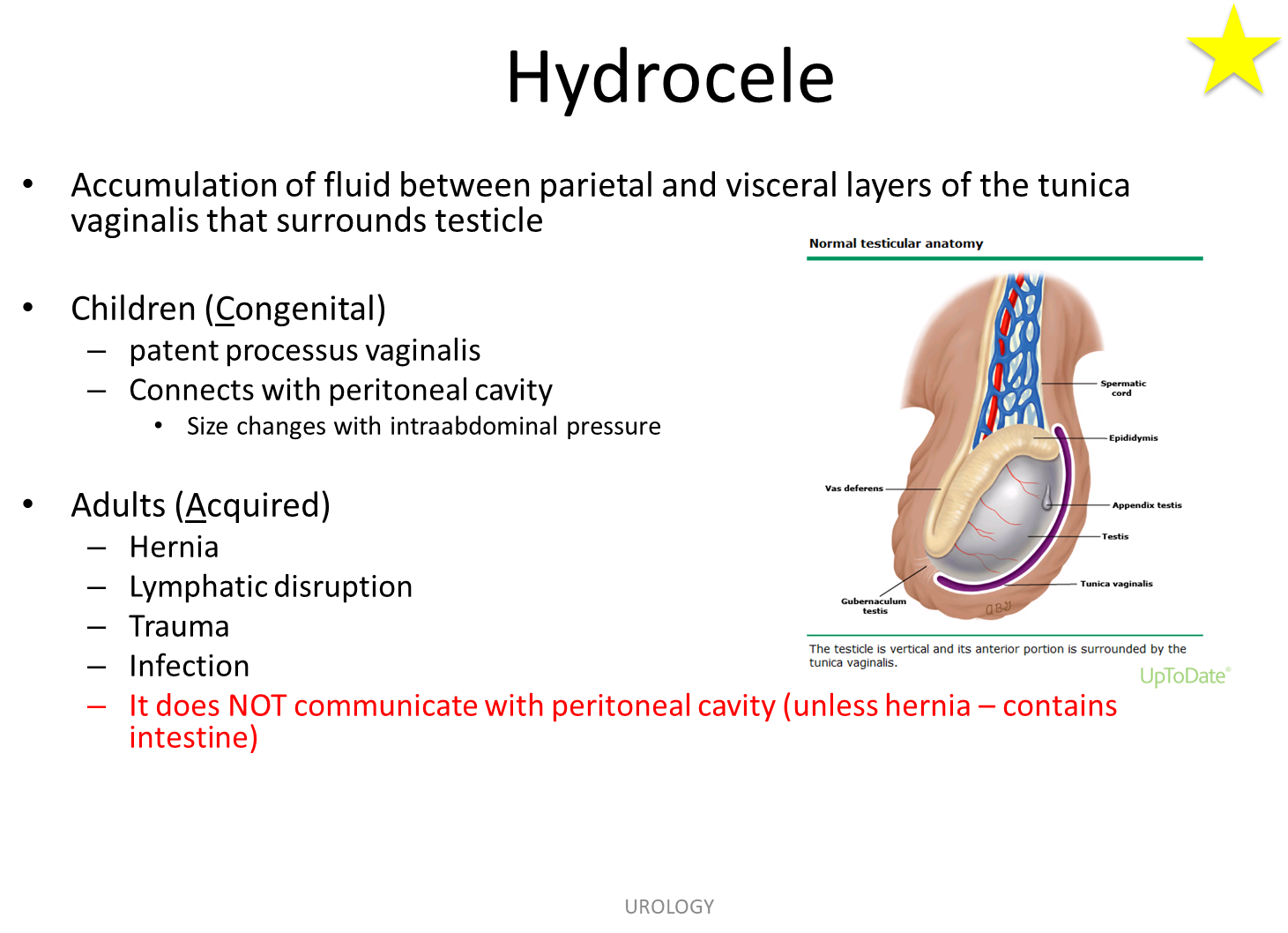
Hydrocele is accumulation of fluid between the parietal and visceral layers of the tunica vaginalis that surrounds the testicle
1) In children it is often congenital due to a patent processus vaginalis
→ it will often be communicating and will change in size with increased intrabdominal pressure
2) Adults are acquired often secondary to something like lymphatic drainage, trauma or infection
→ it does NOT communicate unless it is associated with a hernia
What is Fournier’s Gangrene?
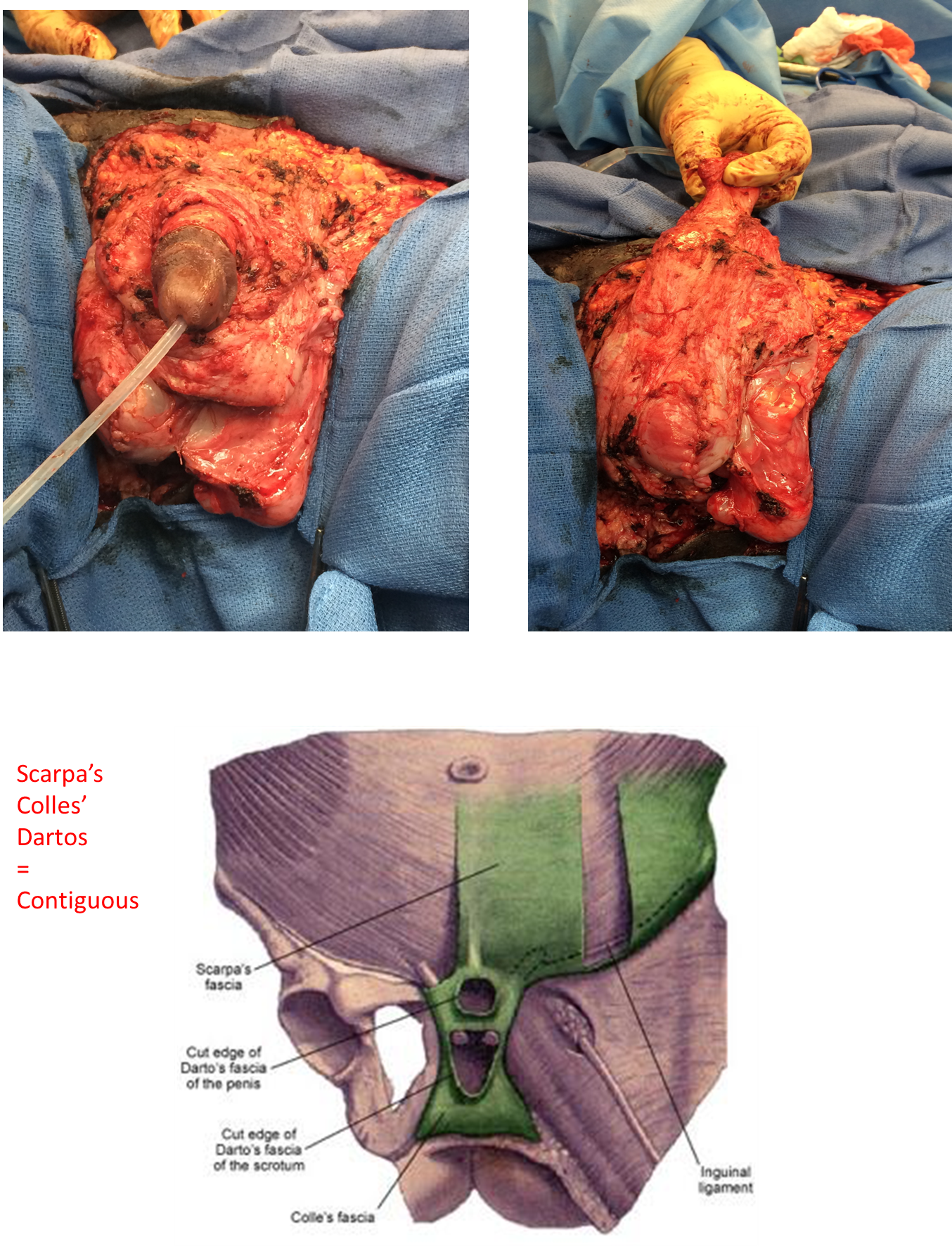
Fournier’s Gangrene is a rapidly progressive necrotizing fasciitis of the perineum, scrotum or penis due to polymicrobial infection of the soft-tissue
1) This disease is often seen in older men, diabetics and alcoholics
→ because it infects the superficial fascial layer, it can have contiguous spread along Colle’s, to Dartos, to Scarpa’s leading to infection spreading up the anterior abdominal wall
→ patients often have Crepitus due to gas forming organisms in the testis
2) Treated with emergent surgical debridement involving removal of affected skin and fascial layers
→ also treated with broad spectrum antibiotics
What is Epididymo-Orchitis?
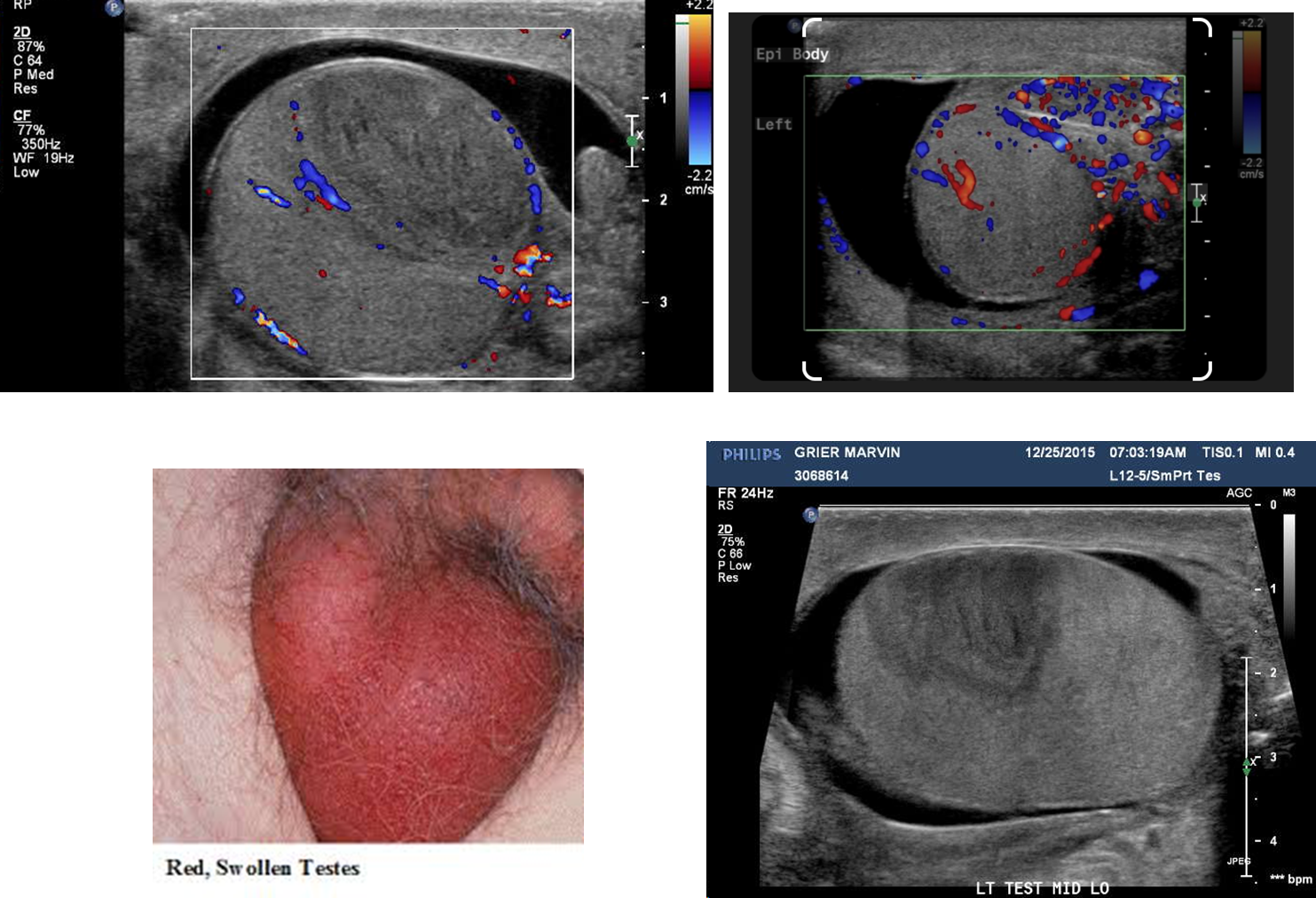
Epididmyo-Orchitis is inflammation of both the epididymis and testis and is often infectious in origin
1) Often presents with diffuse redness and swelling of the scrotum making it hard to differentiate the testicles and epididymis
→ when patients are less than 35 years old it is often Chlamydia or Neisseria
→ when older than 35 or children E.coli and Pseudomonas are primary concerns
2) Treated with Ceftriaxone (3rd generation cephalosporins) with the addition of doxycycline or azithromycin if you suspect it to be Neisseria or Chlamydia
→ if not then just use Levofloxacin
What is Testicular Torsion
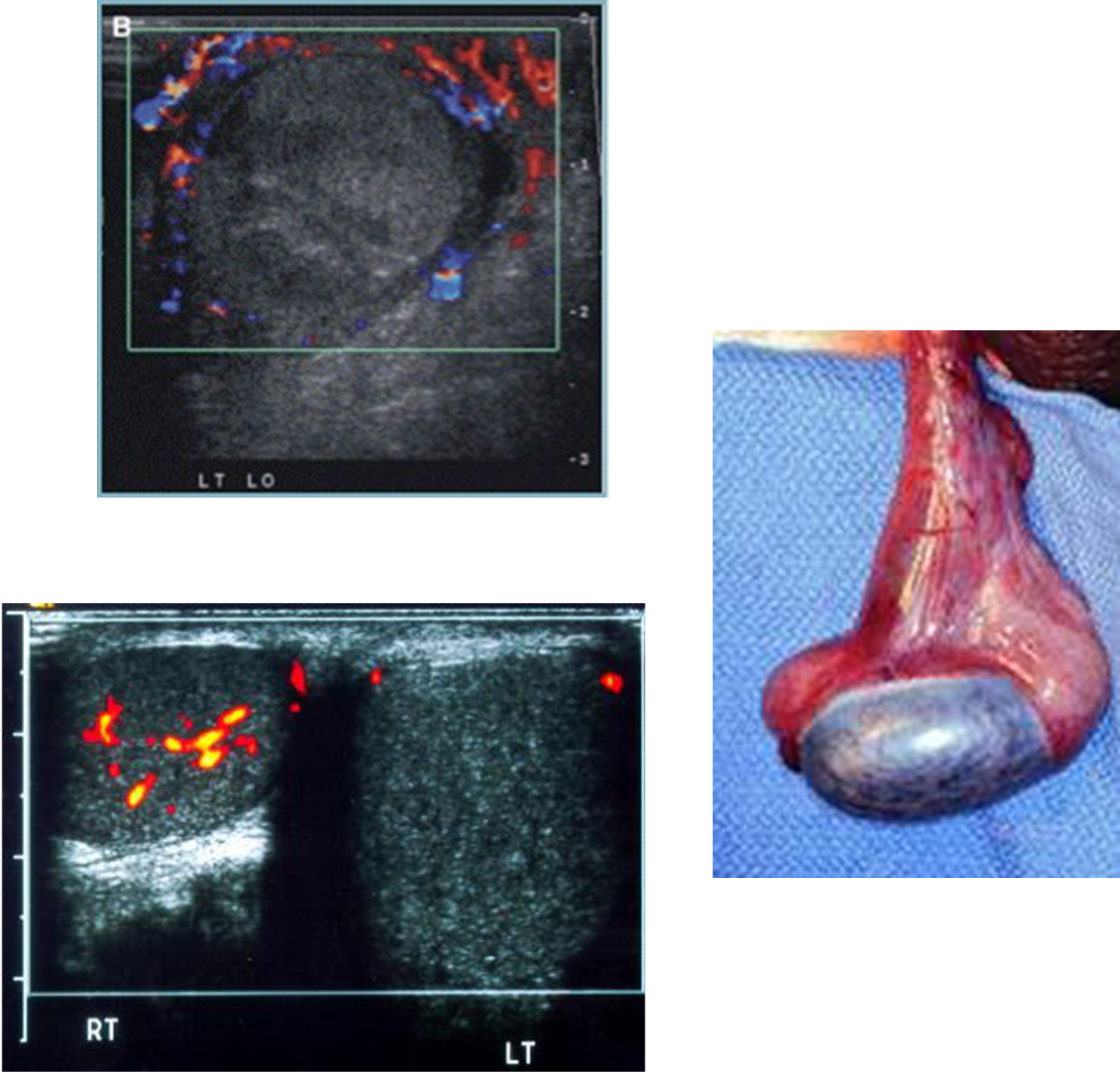
Testicular Torsion is twisting of the spermatic cord leading to ischemic damage of the testis
1) often occurring due to insufficient fixation of the testicle by the gubernaculum leading to it rotating “bell clapper deformity”
→ the testicle will lay horizontally instead of vertically and will have an absent Cremaster reflex
2) On examination will often see absent blood supply to the testis with abdominal pain and GI symptoms but have no fever or urinary complaints
→ it is considered a surgical emergency
What is a testicular mass in young males?
Testicular mass in younger males is always considered cancer unless proven otherwise and is often not an acute issue with no pain
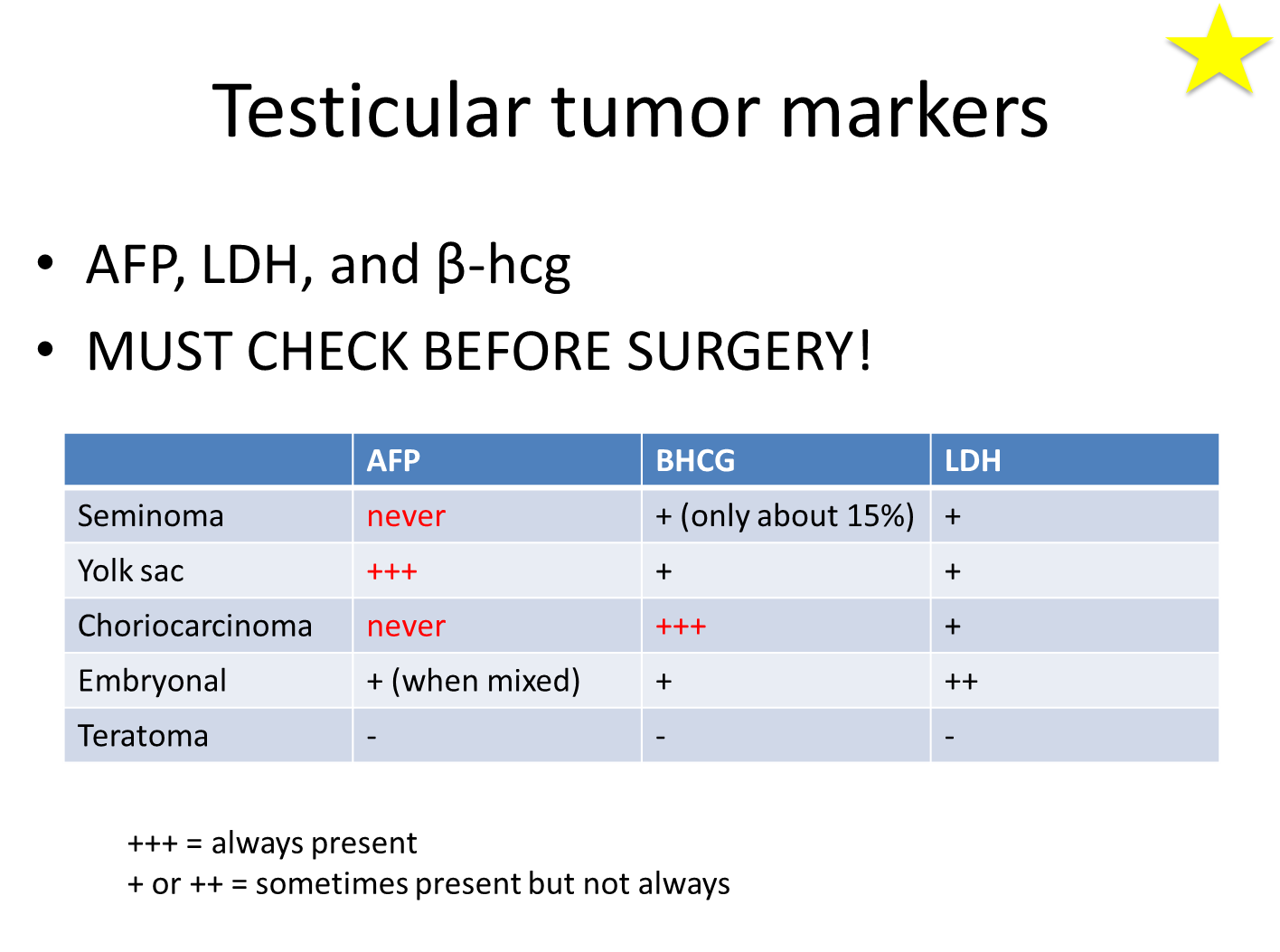
1) The majority of testicular masses in young males is testicular cancer with the majority being germ cell in origin with the most common form being a seminoma
2) seminoma will not have any elevated serum tumor marker except for maybe bHCG or LDH
3) Yolk sac tumors will have elevated Alpha-fetoprotein
4) Choriocarcinoma have elevated beta-HCG
→ are commonly hematogenous spreading (hematogenous spreading cancers reign foolishly)
What is important to remember for surgery in the scrotal area for cancer?

1) Radial Orchiectomy is where a surgeon makes a inguinal or gronial incision to remove the entire testis and spermatic cord
→ importantly the cut is NOT AT THE SCROTUM when you are concerned about cancer
2) Make sure to check tumor markers before and after as well as doing a CT scan and chest X-ray
→ make sure to bank sperm in order to make sure that these patients can become fathers if they wish to do so