Cardiac Excitability and Conductivity
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
52 Terms
Cardiac Excitability and Conductivity (3)
Common with other muscle tissues
Heart muscle cell membrane is an excitable membrane capable of transmitting an action potential
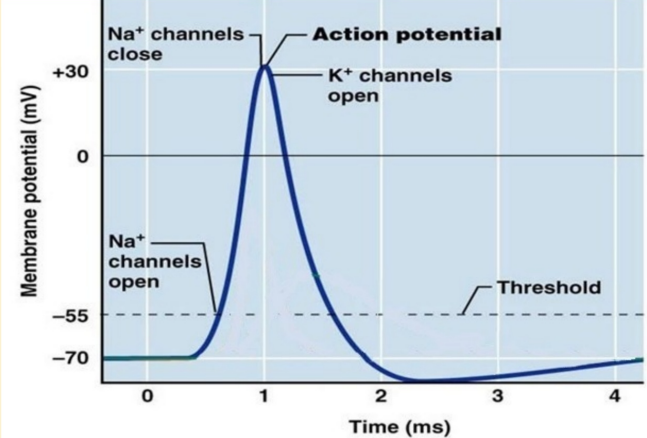
Depolarization occurs due to the opening of fast sodium channels
Skeletal Muscle (3)
No plateau phase
Depolarization is rapid, followed by quick repolarization
designed for rapid, repetitive contractions
Skeletal Muscle Action Potential (photo!)
Skeletal Muscle Excitation-Contraction Coupling
Relies on calcium from the sarcoplasmic reticulum only!
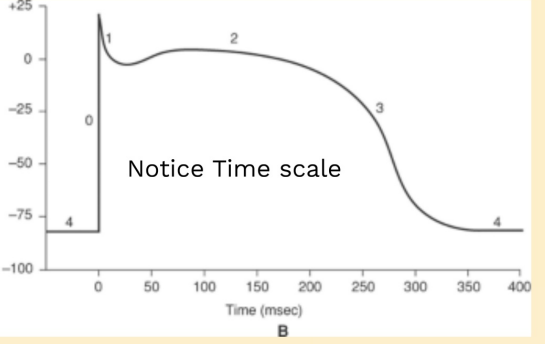
Skeletal Muscle Notice Time Scale (photo)

Ventricular Muscle (Cardiac Muscle) (4)
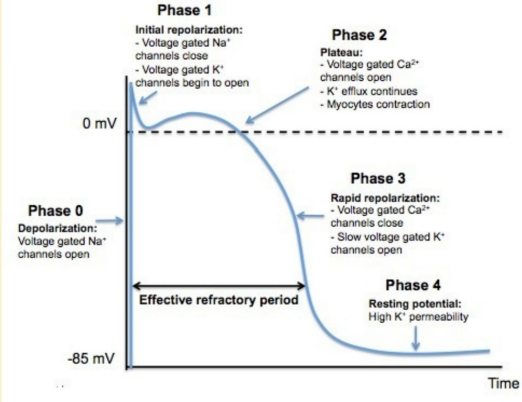
Has a plateau phase due to the prolonged opening of slow calcium channels
lasting several hundred milliseconds
Maintains the potential at a positive level during the action potential
needs rhythmic, sustained contractions to pump blood effectively
Ventricular muscle Prolonged Depolarization (3)
Leads to a longer absolute refractory period (ARP)
Prevents tetanization (continuous contraction)
Crucial for proper heart function
Ventricular Muscle Action Potential (photo!)
Ventricular Muscle Functional Importance (2)
Heart muscle cells require diastole (relaxation phase) to fill with blood
Prolonged ARP ensures rhythmic contractions and prevents overlap of successive beats, maintaining efficient blood pumping
Ventricular Muscle Excitation-Contraction Coupling (2)
Calcium influx during the plateau phase triggers a stronger contraction
Uses extracellular calcium + from the sarcoplasmic reticulum
Ventricular Muscle Notice Time Scale (photo)
Increased Excitability meaning (2)
Refers to conditions or factors that make it easier for heart muscle cells to reach the threshold for generating an action potential
Increases the heart's sensitivity to stimuli, potentially leading to arrhythmias or abnormal heart rhythms
Increase Excitability (6)
Sympathetic stimulation
Mild hyperkalaemia (partial depolarization)
Adrenaline
Mild hypoxia (partial depolarization)
Ischaemia
Digitalis increases atrial muscle excitability
Decreased Excitability meaning (2)
Refers to conditions or factors that make it harder for heart muscle cells to reach the threshold for generating an action potential
Reduces the heart's ability to respond to stimuli
Decrease Excitability (7)
Parasympathetic stimulation (atrial muscle only)
Marked hyperkalaemia (marked depolarization)
Hypokalaemia (hyperpolarization)
Hyponatraemia
Acetylcholine
Marked hypoxia (marked depolarization)
Digitalis decreases ventricular muscle excitability
Pathological Conditions of Excitability (6)
Extrasystoles
Paroxysmal Tachycardia
Atrial Flutter
Atrial Fibrillation
Ventricular Flutter
Ventricular Fibrillation
Extrasystoles definition - Pathological Conditions of Excitability
Abnormal systoles occurring during early diastole due to impulses from an irritable ectopic focus other than the SA node
Extrasystoles types (3)
Atrial Extrasystoles
Nodal Extrasystoles
Ventricular Extrasystoles
Atrial Extrasystoles
Arising from the atrial muscle, followed by a normal diastole as the abnormal impulse resets the SA node
Nodal Extrasystoles
Arising from the AV node and AV bundle
Ventricular Extrasystoles
Arising from the ventricular muscle
Nodal Extrasystoles & Ventricular Extrasystoles ‘similarity’ (2)
Both followed by a "compensatory" pause due to a longer diastole
The extrasystole does not reset the SA node, thus:
Normal impulse is generated by the SA node but cannot be transmitted to the ventricles
The ventricular muscle is still in the absolute refractory period (ARP)
Paroxysmal Tachycardia (7) - Pathological Conditions of Excitability
High heart rate in short attacks (seconds to days)
due to Ectopic focus firing faster than SA node
Rate: Usually regular, atrial or ventricular origin
Dormant focus between attacks
Triggered by anxiety, anger, fear
These are factors that increase excitability - trigger condition
Symptoms: Palpitations or awareness of heartbeats
Tachycardia meaning
abnormally high heart rate
Atrial Flutter (5) - Pathological Conditions of Excitability
High atrial rate (200-300 beats/min)
Diminished pumping action of atria
due to the long refractory period of the AV node
AV node refractory period limits transmission to ventricles (max 200 impulses/min)
Creating Physiological heart block
Atrial Fibrillation (8) - Pathological Conditions of Excitability
Extremely high atrial rate (>350 beats/min)
Individual atrial fibres beat asynchronously
Complete loss of atrial pumping action
"Bag of worms" feeling of atrial beats
Heart block present
Irregular ventricular rhythm
Impulses transmitted randomly after reaching the necessary threshold
Not fatal: Ventricular pumping preserved
Ventricular Flutter (5) - Pathological Conditions of Excitability
High ventricular rate (200-350 beats/min)
Due to nodal/ectopic focus firing at a high rate
Markedly reduced cardiac output
due to shortened diastole
Fainting usually occurs
Ventricular Fibrillation (4) - Pathological Conditions of Excitability
Extremely high ventricular rate (>350 beats/min)
Asynchronous myocardial fibre activity
Complete loss of ventricular pumping action
Rapidly fatal (within minutes)
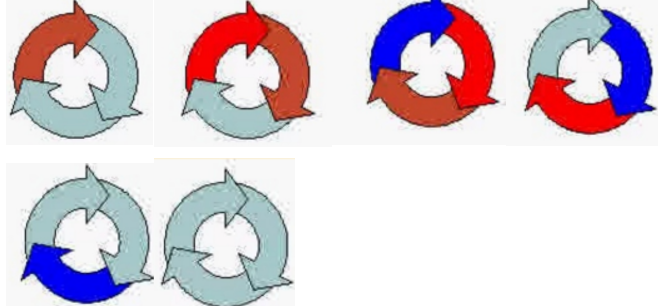
Resting Membrane Potential & Cardiac Impulse Types (4)
Resting Membrane Potential
Depolarising Membrane
Depolarised Membrane
Repolarising Membrane
Resting Membrane Potential (3)
The electrical charge across the membrane at rest
Inside the cell: negative relative to the outside
Maintained by ion gradients (sodium, potassium)
Depolarising Membrane (3)
The membrane potential becomes less negative (more positive)
Sodium ions (Na⁺) rush into the cell
Leads to the generation of an action potential
Depolarised Membrane (3)
The membrane potential reaches its peak (positive)
Action potential is propagated along the muscle
A phase where the cell is unresponsive to further stimulation (absolute refractory period)
Repolarising Membrane (3)
The membrane potential returns to resting negative state
Potassium ions (K⁺) leave the cell
The cell prepares for the next action potential
Circumstances for Re-entry & Circus Movement - Normal Conditions (2)
The depolarising wave travels through the muscle and eventually dies out
It encounters tissues in their absolute refractory period, preventing further action potential propagation
Circumstances for Re-entry & Circus Movement - Abnormal Conditions (2)
The depolarising wave reaches repolarised tissue (tissue that is no longer in the refractory period)
The tissue can be depolarised again, allowing the impulse to continue
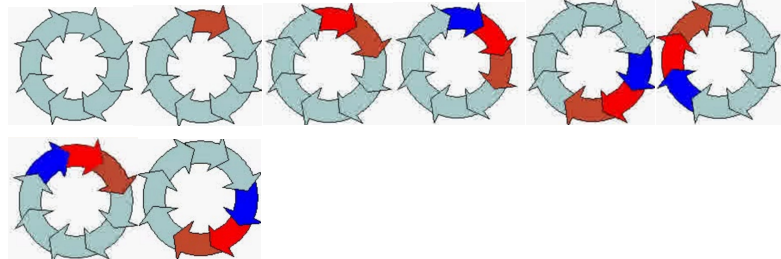
Circus or Re-entry Movement (4)
The impulse circulates around the tissue in a circular pattern, rather than dying out
This creates a self-sustaining loop of electrical activity
Leads to abnormal heart rhythms or arrhythmias
as the continuous re-entry disrupts the normal sequence of cardiac contraction
Conditions that can give rise to Circus Movement (3)
Decrease in the Velocity of the Impulse
Length of Pathway
Shortening of the Refractory Period
Decrease in the Velocity of the Impulse (4)
Blockage of the Purkinje fibres
Ischemia of the muscle
High blood potassium levels
Results in a decreased rate of conduction
Length of Pathway (3)
Impulse takes a longer pathway, returning to the origin and encountering muscle in the resting phase
Dilated Hearts
Increased size of the heart chambers leading to longer impulse travel time (long pathway)
Shortening of the Refractory Period (2)
Can occur due to factors like:
Adrenaline release
Electric AC shock
Importance of the Purkinje Fibres in Preventing Fibrillation (2)
Rapid Conduction
Longer Refractory Period
Rapid Conduction meaning
Purkinje fibres conduct impulses within a few 100ths of a second, ensuring that no part of the muscle is out of refractoriness
Longer Refractory Period (4)
The refractory period of Purkinje fibres is more than 25% longer than that of ventricular muscle fibres
This delay ensures that the impulse transmitted only after muscle fibre repolarisation
Prevents continuous or abnormal stimulation
could lead to fibrillation
Conductivity definition
Specialised conducting system ensures excitation travels to all heart muscle fibres in a specific pattern
Conducting Pathways (5+1)
Anterior, Middle, and Posterior Internodal Atrial Bundles
A-V Node
Only pathway from atria to AV bundle; slow conduction, long absolute refractory period
A-V Bundle
Right and Left Bundle Branches
Purkinje Fibres
Heart Block definition
Failure of impulses from the atria to reach the ventricles due to blockage at the AV node or Bundle
Types of Heart Block (2+2)
Partial
Regular
Irregular
Complete
Partial Heart Block
Some impulses fail to pass
Regular Partial Heart Block
Fixed ratio between atrial and ventricular rhythms
Irregular Partial Heart Block
NO fixed ratio between atrial and ventricular rhythms
Complete Heart Block
All atrial impulses fail to reach the ventricles, causing uncoordinated atrial and ventricular rhythms
Heart Block Classification (3)
1st Degree: Delay in conduction
2nd Degree: Partial block
3rd Degree: Complete block