Local Anesthetic Complications and Management
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
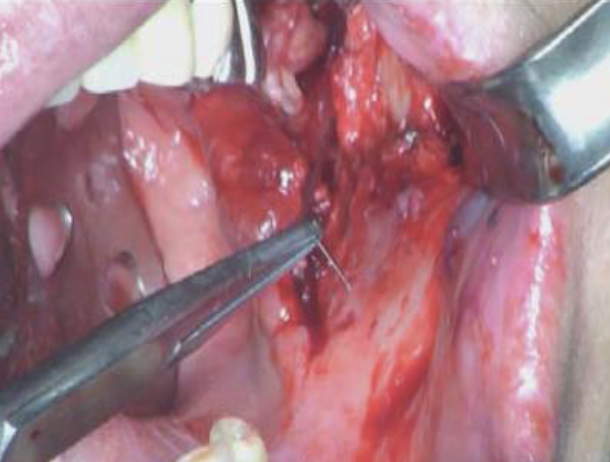
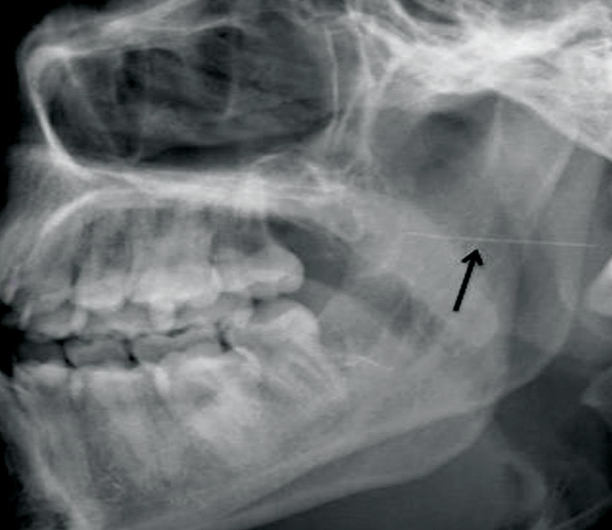
Complication – The needle breaks while administering local anesthetic to your pt
Management – If you can see the needle, you should attempt to retrieve it using a hemostat or cotton plier. If unable to retrieve, immediate referral to an oral surgeon for further evluation and/or surgical intervention if necessary
Prevention: Needle Breakage
Malamed reports that in most cases of a broken needle in the literature, almost all were while performing an IANB with a 30-gauge SHORT needle on an adult***
– Use appropriate length and gauge needles for the injection you are performing
– Don't pre-bend the needle if you don’t have to (some supplemental injections may be an exception)
– Avoid "burying to the hub“ of the needle if at all possible
– Replace needle with a new one after 3-4 injections
Complication – After administering local anesthetic to your pt, they report lingering paresthesia (numbness/tingling) that lasts for days/weeks
Management – First, you should determine what the cause of the paresthesia is. Remember, some paresthesia is a relatively common complication of certain surgical procedures such as extractions (especially mandibular 3rd molars). If paresthesia is a result of an injection (most likely due to the IANB), reassure the pt that most paresthesia will subside within a few days to several months. Follow up with the pt and RECORD EVERYTHING. Refer to specialist if unresolved
Prevention: Prolonged Anesthesia and/or Paresthesia
Most paresthesia involves trauma to a nerve. Avoid injecting directly into the nerve if at all possible, however in some instances it can be unavoidable (IANB)
– Avoid the use of Prilocaine with the IANB due to reportedly increased risk of paresthesia (per Malamed)
– Adhere to basic injection steps as closely as possible
– If a nerve is directly contacted (most likely the inferior alveolar or lingual nervesduring an IANB) avoid injecting directly into it. Move needle 1-2 mms away and/or reinject
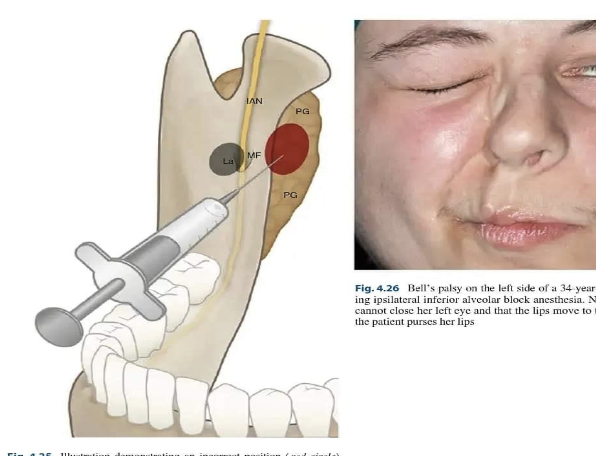
Complication – After administering an IANB, the pt's face on the side that was injected "droops" and the pt is unable to close their eyelid
Management – Most likely local anesthetic was administered into the pt's facial nerve (cranial nerve VII) which partly resides in the parotid gland. Reassure the pt that the numbness will be transitory and will wear off as the local anesthetic is metabolized. Instruct pt to manually close their eyelid and moisten with eye drops as needed until function is regained ***
Prevention: Facial Nerve Paralysis
In almost all cases, this complication is an operator error while giving the IANB (or Gow-Gates). Always contact bone before injecting! ***
Complication – Pt reports trismus (pain upon opening or closing) and difficulty chewing food a day or two after administration of local anesthe
Management – Trismus caused by local anesthetic deposition is usually caused by trauma to some of the muscles of mastication usually due to repeated injections (especially due to the IANB) or secondary due to swelling or hematoma formation
– Instruct the pt to use warm compresses for 20-30 minutes at a time
– NSAIDS
– Muscle relaxant Rx if needed
– Reassure pt that trismus will dissipate, usually within 48-72 hours
Prevention: Trismus
Use a new, SHARP, needle. Needles will have microscopic "burs" after repeated injections, ESPECIALLY if bone is contacted (IANB). If repeated injections in the same area are needed, consider using another approach or supplemental techniques

Complication – After administration of local anesthesia, the pt bites lip and/or tongue while anesthetized
Management – Soft tissue anesthesia typically lasts much longer than pulpal anesthesia and pts (especially children) can be unaware of injury caused by biting soft tissue.
– NSAIDS
– Warm saltwater rinse of affected area
– Ointment to minimize irritation
Prevention: Self Inflicted Soft Tissue Injury
Use a local anesthetic with an appropriate duration for the procedure you are doing. For pediatric pts, warn pt AND parent to avoid lip and tongue chewing after appt is over. Cotton roll may be placed in anterior mandibular vestibule. I've also seen stickers to place on pediatric pts to serve as a reminder to parents that they are anesthetized

Complication – After local anesthetic deposition, swelling around the site of injection develops and a hematoma is formed
Management – A hematoma is a collection of clotted or partially clotted blood that pools outside of blood vessels and can be a complication during local anesthesia delivery. It is usually formed by damaging a blood vessel with the needle. If noticed while administering local anesthetic, direct pressure should be placed on the bleeding site for a minimum of 2 mins. Warn the pt that discoloration (bruising) may occur and last for several weeks. Ice may be applied if it is noticed immediately. NSAID use for subsequent soreness ***
Prevention: Hematoma
Most often will occur with the PSA, IANB, or mental nerve block injections after inadvertent contact with a blood vessel in older or elderly pts due to loss of collagen and tissue rigidity. Use appropriate needle size and length. Avoid repeated injections into the same area if possible.

Complication – Your pt has an active infection and/or a painful symptomatic tooth and you need to anesthetize them in order to provide tx
Management – Pt's with active infection can be difficult to adequately anesthetize
– Regional blocks should be considered instead of infiltrating around infected tooth if at all possible
– Avoid injecting directly into infected tissue if possible (risk of spreading infection & relative inadequacy of anesthetic due to acidified tissue)
– Consider use of supplemental injection techniques in addition to traditional nerve blocks
– Pt's with generalized swelling should be administered antibiotics and warned of potentially catastrophic symptoms if infection progresses (trouble breathing, etc
Prevention: Active Infection
If prudent and pulpal anesthesia is unable to be obtained, infected area can be incised & drained and definitive tx be postponed until acute infection stage is over
Complication – Pt reports pain and/or burning while you are depositing local anesthetic solution
Management – Pain or burning upon injection can have multiple causes. Most commonly, some "burning" may be due to the lower pH of local anesthetic, especially anesthetics that contain a vasoconstrictor. Reassure pt that burning sensation should subside rapidly. If desired, a local anesthetic with a more NEUTRAL pH such as Mepivacaine plain can be given before injection with a local anesthetic with a vasoconstrictor which has a lower pH (more acidic) ***
Prevention: Pain and/or Burning on Injection
Adhere to basic injection protocol – INJECT SLOWLY. Use SHARP needles (may need to use multiple needles per appt). Consider use of a buffered local anesthetic solution. Don't soak anesthetic carpules in any disinfecting solution (alcohol) which may diffuse into the solution
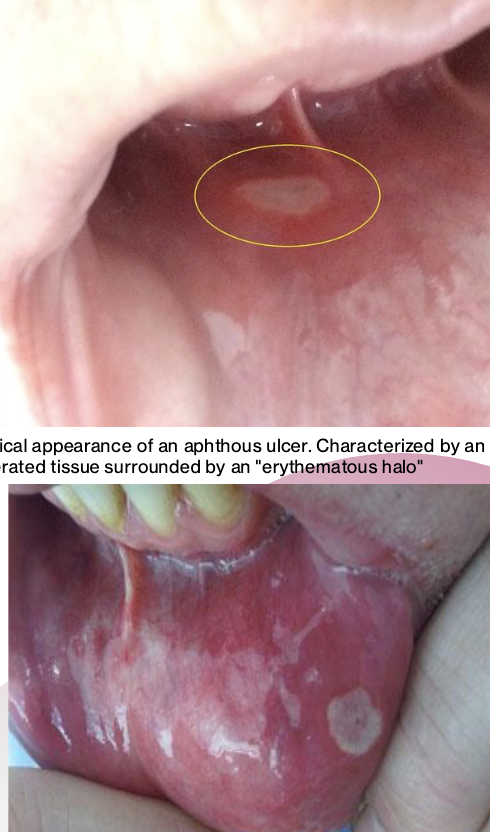
Complication – Pt develops an aphthous ulcer (canker sore) near site of local anesthetic deposition
Management – Soft tissue trauma from injection may instigate soft tissue pathologies such as aphthous ulcers and herpetic lesions if your pt is prone to them. Management of soft tissue ulcers is usually managing the symptoms with warm salt water, topical ointment, etc
Prevention: Aphthous Ulcer Formation
There is nothing that can be done to prevent this from happening, however if your pt is known to be prone to aphthous ulcer or herpetic lesion formation, warning them beforehand would be prudent
Complication – After administering local anesthetic, your pt develops one or more signs and symptoms of local anesthetic overdose including: slurred speech, drowsiness, dizziness, visual disturbances, loss of consciousness, or convulsions
Management – If your pt is conscious, seat them in a comfortable position and OBSERVE
– Consider placing pt on supplemental oxygen
– If symptoms progress or pt becomes unconscious/unresponsive, contact EMS immediately and begin BLS procedures ***
Prevention: Local Anesthetic Overdose
Always be aware of how much anesthetic you are giving your pts! ***
– Limit procedures to 1-2 quads and anesthetize ONE quad at a time
– Thoroughly check med hx
– Be ESPECIALLY cautious when administering local anesthetic to children and elderly pts (go by body weight and pay attention to the MRD) ***
Complication – Soon after local anesthetic is administered, the pt complains of fast heart rate, profuse sweating and begins to panic
Management – If a vasoconstrictor was used, most likely the local anesthetic was deposited intravenously. Seat pt in a comfortable position and reassure the pt that this effect should dissipate quickly and explain what is happening (epi used in drug is in bloodstream). Based on pt reaction, procedure might need to be rescheduled
– If heart rate does NOT slow down withing 20 minutes OR pt becomes unconscious, contact EMS IMMEDIATELY and begin BLS procedures
Prevention: Intravenous Administration of Vasoconstrictor
Aspirate before injecting
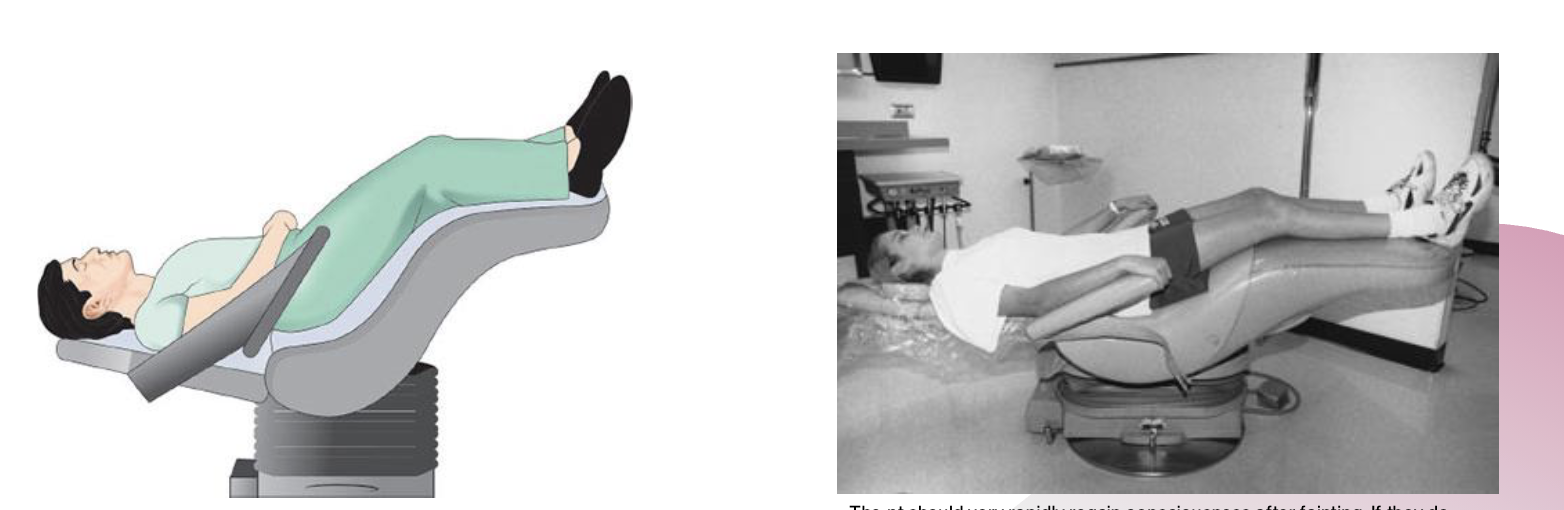
Complication – At some point during the process of administering local anesthetic (before, during, or after) your pt complains of lightheadedness and faints
Management – If your pt has a known dental phobia and faints during the local anesthetic procedure, lean pt as far back in the dental chair as possible (Trendelenburg Position), elevate their legs, and observe ABCs (Airway, Breathing, Circulation) ***
– Consciousness should be rapidly regained. If the pt does not regain consciousness quickly (within 10 seconds), have a staff member activate EMS and check for pulse/breathing
– Even if the pt rapidly recovers, it is recommended that the pt obtain a ride and be rescheduled for dental tx as the pt will be at a much greater risk for fainting again within the first 24 hours
Prevention: Patient Faints
Provide local anesthetic as atraumatically as possible. If pt has a needle phobia, avoid having the syringe in their eyesight. Reassure pt during procedure and provide positive feedback
– Pts should be leaned back in the chair in a supine position for the local anesthetic procedure (doing so may prevent fainting from occurring)
Complication – During medical and dental hx review, pt reports they are "allergic" to local anesthetic
Management – Follow-up questions must be asked to ascertain whether this is a "true" allergy or not
– Ask if they have been officially diagnosed by their MD
– Ask what kind of reaction they were having (was it an intravenous epi administration?). Did the pt break out into hives?
– Ask what specifically they are allergic to in the local anesthetic and what local anesthetic was given
– Ask what tx they received
Prevention: Pt claims they are allergic to local anesthetic
Per Malamed, allergy to amide local anesthetics is either extremely rare or non-existent. Most likely, the pt does NOT have a true allergy to local anesthetic and experienced an intravascular injection with a vasoconstrictor, HOWEVER if they insist then we must take them at their word. If tx requires the use of local anesthetic, the pt should be referred to their MD for allergy testing prior to any injections or topical use
Complication – Pt is extremely apprehensive about local anesthetic procedures
Management – Most people presenting for dental tx will have at least SOME anxiety and apprehension regarding local anesthesia. MOST of these people will get through the procedure without special considerations. For pts who are extremely apprehensive there are several strategies that can be considered, however not all strategies work on all people:
– Talk to the pt and get an understanding of why they are apprehensive. Is it fear of pain, needle, being numb, past experience, etc? Tailor your management to the cause of apprehension
– "Tell, Show, Do" - Explain what you are doing every step of the way. For some people, local anesthesia is frightening because they do not understand and/or cannot visualize what is happening. For these pts, showing them what is occurring (show the carpule, syringe, etc.) may be helpful. Others may not want to see the syringe at all
– Reassure pt that any discomfort is temporary
– Adhere to basic injection technique protocol – GO SLOW
– Distraction techniques
– Consider use of anxiolytic drugs (sedatives, nitrous, etc)
– Provide positive feedback throughout procedure
– For pts who still do not cooperate during local anesthetic procedure, refer to specialist for conscious sedation
– BE PROFESSIONAL!!!