Lecture 10: Joints
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
97 Terms
Normal Synovial Fluid
Hyaluronic acid (a non-sulfated proteoglycan) secreted by synovial cells acts as viscous lubricant
Clarity: Transparent
Color: Clear to pale yellow
0-150 WBC/mL
PMN < 25%
No RBCs
Glucose 0-10 mg/dL lower than blood glucose
Ankylosis
stiffening or immobility of a joint due to fusion of the bones
True intra-articular ankylosis is obliteration of the joint space by fibrosis or ossification between bony articular surfaces
Osteoarthritis (OA)
aka Degenerative Joint Disease (DJD)
Chronic, progressive degeneration of the articular cartilage → structural & functional failure of synovial joints
No systemic inflammatory response
usually Idiopathic (primary)
↑ after age 50
Secondary to previous injury, joint deformity, obesity
Joints affected: usually Oligoarticular, but may be polyarticular
Osteoarthritis Pathogenesis
Chondrocyte injury and death: wear & tear: Aging, metabolic (free radical damage, glycation) or mechanical injury (more common in weight bearing joints)
Chondrocyte reactive proliferation & secretion of inflammatory mediators activate degradative proteases
Early: Fibrillation (fraying & splitting) of cartilage
Chondrocyte reactive proliferation (“Cloning”) & secretion of inflammatory cytokines
Early attempts at repair
Proteolytic destruction of cartilage with full thickness sloughing
Dislodged pieces of cartilage & underlying subchondral bone tumble into the joint space → loose bodies” or “joint mice”
Friction of exposed bone with opposing surface “polishes” the bone giving it a smooth, ivory-like appearance (Eburnation) & underlying bone becomes thickened (sclerotic bone)
Synovial fluid leaks via cracks into the bone → fluid filled Subchondral bone cysts
Mushroom shaped bony outgrowths with cartilage caps form at edges of damaged articular surface (Osteophytes or “Bone Spurs”)
Osteoarthritis Morphology
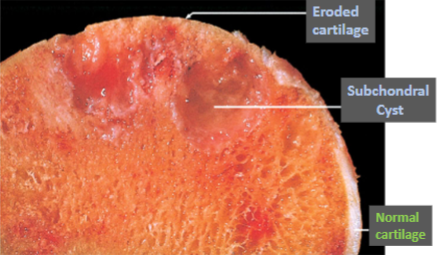
Destruction of cartilage
Fraying/fibrillation followed by erosion
Detached cartilage fragments in joint space
Eburnation of Bone: sclerotic (dense) bone with polished ivory-like surface
Cystic changes in subchondral bone
New bone formation: increased density of subchondral bone → Osteophyte (bone spur) formation
Joint mice/loose joint bodies are detached fragments of bone & cartilage in the synovial fluid/joint space
Synovium shows congestion, variable fibrosis & few inflammatory cells
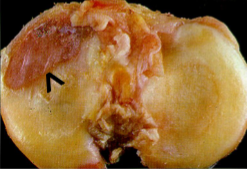
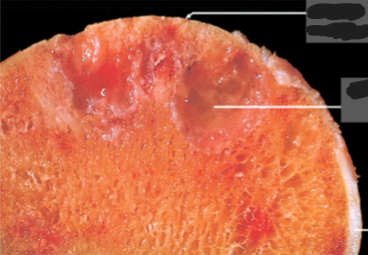
Osteoarthritis
Erosion of cartilage
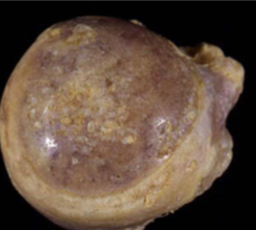
Osteoarthritis
Eburnation
Osteoarthritis
Subchondral bone sclerosis
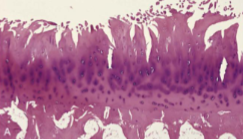
Osteoarthritis
Fibrillation
Osteoarthritis
Osteoarthritis
Osteoarthritis

Osteoarthritis

Osteoarthritis
Joint mice
Osteoarthritis
Joint mice

Osteoarthritis
Joint mice
Osteoarthritis
Joint mice
Osteoarthritis Distribution
Joints subjected to mechanical trauma ("wear & tear"): hips, knees; lower lumbar & cervical vertebrae & hands
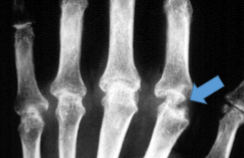
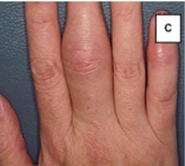
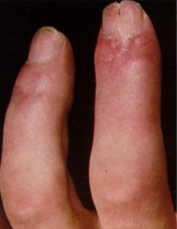
In the Hands:
Bouchard’s nodes: Proximal interphalangeal (PIP)
Heberden’s nodes: Distal interphalangeal joints (DIP)
common in women (but not in men)
First carpal-metacarpal joint (1st CMC)
In the Feet: First metatarsal-phalangeal joint as a complication of bunions (Hallux Valgus)
Usually spares wrists, elbows, shoulders
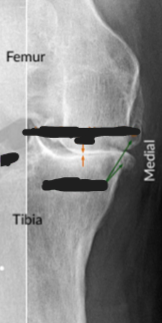
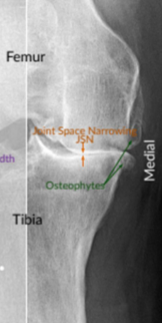
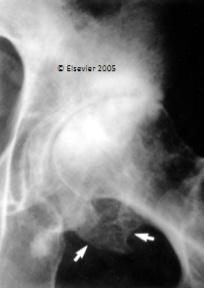
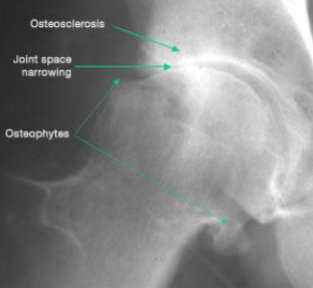
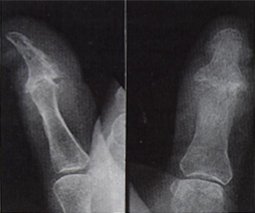
Osteoarthritis
Joint space is narrowed, but fusion (Ankylosis) does not occur
Subchondral bone sclerosis (Osteosclerosis)
Peripheral Osteophytes
Faint scattered radiolucent Subchondral Bone Cysts
Patellofemoral OA: Patella normally slides in the trochlear groove of the femur; cartilage along the trochlear groove & underside of the patella wear down
Knee OA: loss of cartilage in the Patellofemoral compartment or in the Lateral or Medial Tibiofemoral compartments
Heberden & Bouchard "nodes" are due to presence of Osteophytes
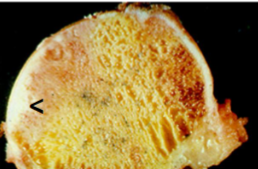
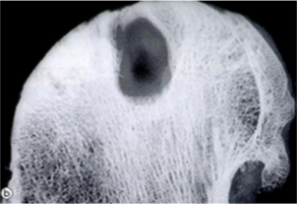
Osteoarthritis
Osteoarthritis
Subchondral Bone Cysts

Osteoarthritis
Osteoarthritis Gender variation
Females: knees & hands more often involved
knees (tibiofemoral & patellofemoral)
hands include Distal interphalangeal joints (DIP)
Males: hips more commonly involved
Osteoarthritis Clinical course
Insidious onset; usually asymptomatic until 50’s
Morning stiffness (“gel”) that usually lasts < 30 minutes; stiffness/pain after periods of inactivity
Joint crepitus (grating sound or sensation); limitation of motion
Deep achy pain that “worsens with use”; worse at end of day
Spinal foramina stenosis with nerve root impingement by osteophytes: radicular pain; muscle spasm; neurologic deficits; muscle atrophy
Usually slowly progressive; produces disability
X-rays are characteristic & definitive but do not correlate well with Sx severity
Charcot Joint
Neuropathic Joint Disease
Progressive joint destruction from peripheral neuropathy
Foot joints in Diabetic Neuropathy
Knees in Tabes Dorsalis (tertiary syphilis)
Extremity joints in persons with Leprosy
Shoulder in Syringomyelia (most due to Chiari malformation)
Pathogenesis: lack of pain & proprioception leads to abnormal mechanics/repeated joint trauma
Rapidly progressive severe OA-like with joint fragmentation
Osteoarthritis Synovial Fluid
Group I; no crystals
Non-inflammatory
Clarity: Transparent
Color: Clear to pale yellow
WBC < 3000
PMN% < 20%
No RBCs
Glucose: blood/SF difference: 0 - 20
Rheumatoid Arthritis (RA)
Chronic systemic Autoimmune inflammatory disorder that primarily affects joints
Polyarthritis involves diarthrodial joints symmetrically & bilaterally
Most commonly involves: Small joints of the Hands & Feet: PIP & MCP in the hands & corresponding joints in the feet
Also, the Wrists, Elbows, Knees, Ankles & Cervical Spine
Produces a nonsuppurative chronic inflammatory proliferative synovitis which progresses to destruction of the articular cartilage & ankylosis of the joint
Rheumatoid Arthritis Risk Factors
Age: cumulative incidence ↑ with age; typical onset age 30-50
Women
HLA-DRB1 alleles of MHC II with similar binding sites to arthritogenic antigens
Smoking, including children of mothers who smoke
Nulliparity
Obesity
Rheumatoid Arthritis Pathogenesis
Autoimmune with genetic susceptibility
HLA allele variants of MHC II Ag presenting cells (APC) preferentially bind to neoautoantigens
Risk linked to a few genetic HLA-DRB1 alleles of MHC II on APCs
Endogenous neoantigen CCP (Cyclic Citrullinated Peptide), which are proteins that have had Arginine post-translationally converted to Citrulline via a Converting Enzyme that is activated by ↑ intracellular Ca++ during Necrosis or Apoptosis & normally marks proteins for destruction
In joints, Citrullination of extracellular structural proteins unfolds the proteins making them neoantigens
APC binding to Citrullinated proteins & presentation to Th cells activate of CD4+ Th cells (Th1 & Th2)
HLA-DR4
Rheumatoid Arthritis Labs
Rheumatoid factor (RF) is an IgM (or IgA) anti-IgG Fc
Often negative in early disease or at presentation
High titers associated with more severe disease & extra-articular manifestations
Not specific; High “False positive” rate: chronic infection, TB, aging
Anti-Citrullinated Peptide Antibodies (ACPAs/Anti-CCP)
May be negative in first months or may precede (predict) development of RA
More specific
Presence at disease onset is the strongest predictor of later radiographic joint damage
↑ C-reactive protein (CRP) or Erythrocyte Sedimentation Rate (ESR)
No RF or Anti CCP → Seronegative
Rheumatoid Arthritis Pathogenesis Model
Apoptosis/Necrosis results in activation of a Converting enzyme that Citrullinates extracellular proteins to form CCP → HLA-DRB1 allele of MHC II of APCs then binds CCP →
Activate Th1 cells make IFN-Ƴ → activates Macrophages → IL-1 & TNF
IL-1 & TNF → synovial cells & chondrocytes to secrete/activate proteases that destroy hyaline cartilage
IL-17 from Th17 cells recruits neutrophils & macrophages
RANKL (expressed by activated Th cells) → activates RANK receptor of osteoclasts → Bone Resorption/lysis
activation of Th2 cells → B-cell Humoral Ab response (anti-CCP, RF) with joint deposition of immune complexes
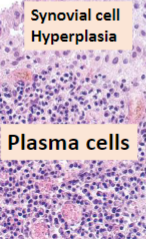
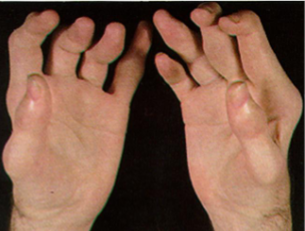
Rheumatoid Arthritis Morphology
Hyperplastic synovium creeps over the surface of the articular cartilage & is thrown into Papillary folds → PANNUS
Synovial cell hyperplasia, stromal edema, chronic inflammation (lymphocytes, lymphoid follicles & plasma cells)
Angiogenesis & fibroblastic proliferation (granulation tissue)
↑ Osteoclastic activity in underlying bone → juxta-articular erosions (lytic bone)
Fibrinopurulent exudate in joint surfaces & synovial fluid
Pannus grows over cartilage → fibrotic, followed by bony fusion (Ankylosis) & destructive inflammation of joint capsule, ligaments, tendons & bursae

Rheumatoid Arthritis
Hyperplastic Synovium forming frond-like papillary folds
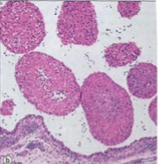
Rheumatoid Arthritis
Hyperplastic Synovium forming frond-like papillary folds

Rheumatoid Arthritis
Rheumatoid Arthritis

Rheumatoid Arthritis
Joint Fusion = Ankylosis
Subcutaneous Rheumatoid nodules
Rheumatoid Arthritis
Immune Complex activation of Macrophages
Occur in mostly “pressure areas” such as elbows, ulnar forearm, lumbosacral region, or periarticular; less commonly in visceral organs
Firm, freely moveable, nontender
more frequent in those with severe disease
Histology: palisaded granuloma with central fibrinoid necrosis

Rheumatoid nodules

Rheumatoid nodules
Rheumatoid nodules
Osteoarthritis
Sclerotic, dense bone
Joint space narrowed, but preserved

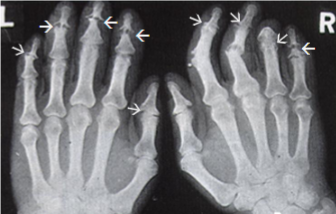
Rheumatoid Arthritis
Juxta-articular erosions (lysis of bone/osteopenia)
Joint ankylosis
Rheumatoid Arthritis
Juxta-articular bone erosions
Rheumatoid Arthritis
Juxta-articular bone erosions

Rheumatoid Arthritis
Late dislocations
Ulnar deviation
Rheumatoid Arthritis joint contractures & deformities
Ulnar deviation of the fingers
Radial deviation of wrist
Swan-neck, Boutonniere deformities of the fingers
Synovial cysts: Baker cyst (Popliteal Cyst) is a synovial lined herniation from the back of the knee into popliteal fossa 2° weakened joint capsule
Joint instabilities & restricted range of motion
Rheumatoid Arthritis Extra-articular manifestations
Lymphadenopathy; Thymic hyperplasia; Splenomegaly
Felty's Syndrome: RA + Splenomegaly with Neutropenia
Risk for Lymphoma; Multiple Myeloma
Anemia of chronic disease
Pulmonary involvement
Rheumatoid nodules; interstitial fibrosis, Caplan syndrome (RA + a Pneumoconiosis)
Vasculitis (RF immune complex or cryoglobulinemia) of small vessels of skin
Neurologic abnormalities due to vasculitis of vasa nervorum
Secondary reactive Amyloidosis (SAA type)
“Serositis”: pleural; pericardial effusions with fibrinous pleuritis/pericarditis
Eye: Scleritis/corneal perforation; uveitis
Heart: accelerates Atherosclerosis & ↑ risk CAD & cardiovascular mortality
Rheumatoid Arthritis Synovial Fluid
Inflammatory-noninfectious (Group II)
Clarity: transparent/opaque
Color: Cloudy, Pale yellow or white/bloody
3000-75,000 WBC/mL
PMN%: 50-90%
No RBCs
Glucose (blood/SF difference, mg/dL): 0-40
Rheumatoid Arthritis Clinical
Fatigue, malaise, anorexia, weight loss, fever, myalgia with joint involvement
Swelling of joints & stiffness, especially in morning or after inactivity → lasts at least 1 hour
Joints warm & painful
Small bones of hands & feet first
Swelling of the same joints on both sides of the body
Rheumatoid nodules of the skin
+ for RF and/or Anti-citrullinated Peptide Antibodies (ACPA)
Progressive joint involvement:
Deformity, greatest joint damage occurs during the first 4-5 years
Increasing numbers of joints involved
Rheumatoid Arthritis labs and Px
Clinical course tends to have remission/flare cycles
ESR & CRP elevated during active inflammation
Positive RF, anti-CCP ("Seropositive") predicts a more severe, progressive disease
Without therapy, life expectancy decreased by 10 years
Top causes of death are:
Ischemic heart disease (Atherosclerotic CAD)
Pulmonary Interstitial Fibrosis
Other causes of death include:
Vasculitis
Systemic amyloidosis, SAA type
Lymphoma
Juvenile Idiopathic Arthritis (JIA)
Arthritis before age 16 of unknown cause that persists > 6 weeks
Large joints more often affected than small joints
Usually Seronegative: Rheumatoid nodules, RF & anti-CCP are absent
Systemic disease is more frequent (serositis, myocarditis, growth retardation, glomerulonephritis, uveitis)
Seronegative Spondyloarthropathies
Seronegative
HLA-B27 (an HLA Class I Ag on all nucleated cells that present cytosolic peptides to CD8+ T Cells)
Sacroiliac joints & Spine
Inflammation of the Entheses (tendinous & ligamentous insertions)
Axial oligoarthritis or asymmetric peripheral arthritis
Achilles tendon involvement & Plantar Fasciitis
Immune mediated Pathogenesis (T-cell response to cross reacting arthritogen)
Ankylosing Spondylitis
AKA Axial Spondyloarthritis
Entheses of the Spine & the joint where sacrum joins the pelvis (Sacroiliac joint)
HLA-B27 positive
Late adolescence or early adulthood, in males
Inflammation of the sacroiliac joints (Sacroiliitis) → progressive low back pain or pain in gluteal region
Enthesitis of peripheral Annulus Fibrosus of discs & anterior/posterior Longitudinal ligaments (Spondylitis) damage tissue → calcifies → Syndesmophytes → vertebral fusion (Ankylosis or “bamboo spine”)
Affect the joints between spine & ribs, restricting breathing; prone to vertebral fractures
Acute Iritis → eye pain & photophobia
↑ incidence in inflammatory bowel disease (IBD)
Diagnose early with MRI of Sacroiliac joint

Ankylosing Spondylitis
Ankylosis or “bamboo spine”

Ankylosing Spondylitis
Ankylosis or “bamboo spine”
Reactive Arthritis
Seronegative Polyarthritis
urethritis/cervicitis
Conjunctivitis/Uveitis
males in 20s, 30s
Post-Infectious Arthritis after an infection elsewhere in the body, from which the patient has recovered
Pathogenesis: Immune cross-reactivity reaction after infection with GU Chlamydia, GI Dysenteric infections (Salmonella, Shigella, Yersinia, Campylobacter, Clostridium difficile), Chlamydia pneumonia, or HIV related infections
Reactive Arthritis Clinical
Early: low back pain, joint stiffness, asymmetric oligoarthritis, usually of lower extremity
“Sausage” fingers or toes (synovitis of digital tendon sheath)
Enthesitis of Achiles tendon & plantar fascial insertions of calcaneous (swelling of heel)
chronic cases develop calcaneal bone spurs; ossification of other tendoligamentous insertion sites
Arthritic episodes wax & wane; most remit
Conjunctivitis/Uveitis/Urethritis/Balanitis/Cervicitis
Cardiac valvular disease (aortic regurgitation)
Erythematous, scaly plaques, usually affecting the palms, soles & toes (Keratoderma Blennorrhagicum)

Sausage left second toe in reactive arthritis

Erythematous, scaly plaques, usually affecting the palms, soles & toes (Keratoderma Blennorrhagicum) in Reactive Arthritis
Psoriatic Arthritis
Age 30-50
HLA-B27 & HLA-Cw6
Gradual onset of joint involvement, concurrent with or following skin disease
Conjunctivitis
Iritis
Asymmetric involvement of hands & feet
DIP joints most involved: “sausage” digits
Radiograph: "Pencil in cup deformity"
Sacroiliac & spinal disease
Histology like RA but Joint destruction less frequent

Psoriatic Arthritis
Dactylitis of third & fourth toes

Psoriatic Arthritis
Enthesitis of right Achilles' tendon
Psoriatic Arthritis
Dactylitis of middle finger

Psoriatic Arthritis

Psoriatic Arthritis
Pencil in cup deformity
Psoriatic Arthritis
Pencil in cup deformity
Psoriatic Arthritis
Sausage Digits (nail changes)
Psoriatic Arthritis
Sausage Digits
Psoriatic Arthritis
Pencil in cup deformity
Septic (bacterial) arthritis
Pathogenesis: Hematogenous or direct inoculation
Sudden onset of painful swollen joint with decreased range of motion
Fever, leukocytosis, elevated ESR
Most monoarticular; knee most common
Septic (bacterial) arthritis Synovial Fluid
Group III: Septic joint
Clarity: opaque
Color: White
< 50,000 WBCs/mL
PMN%: >90%
RBCs
Glucose (blood/SF difference, mg/dL): 20-100
Lyme Arthritis
Infection by spirochete Borrelia (“Borreliosis”)
Inoculation via bite of deer tick
Erythema Migrans skin lesions
Erythematous margins with central fading +/- central “bull’s eye”
Untreated develop arthritis
Arthritis develops within weeks to up to 2 years after infection (main feature of late-stage disease)
Joint swelling- knees are affected most often
Involves large joints
Attacks last for weeks to months, then migrating to new sites
Usually, one or two joints affected at a time
Pathology: Synovitis, papillary
Viral Arthritis
Rubella; Parvovirus B19; Chronic hepatitis B, C; mosquito borne Alphaviruses
Pathogenesis: infection, autoimmune x-reactivity or immune complex deposition
Parvovirus B19 infection (Fifth Disease; Erythrovirus) in adults → self-limited arthritis (lasts days to weeks) that mimics RA
Gout
Precipitation of Monosodium Urate crystals, within & around joints → Arthritis
Uric acid: nitrogenous waste product from breakdown of DNA Purine nucleotides (Adenine & Guanine) & is excreted in Urine (2/3) & Feces (1/3)
Deficiency of HGPRT → cannot salvage → purines degraded into uric acid (↑ serum Uric Acid)
Value of > 7 = Hyperuricemia
Primary gout: idiopathic
Secondary gout:
↑ production due to nucleic acid turnover, as in acute Leukemia/Lymphoma, or release after chemotherapy (Tumor Lysis Syndrome)
↓ excretion in chronic renal disease
Congenital HGPRT deficiency (Lesch-Nyhan syndrome)- X-linked; manifests with neurologic symptoms, intellectual disability, self mutilation; some develop gout
Causes of Secondary Hyperuricemia/Gout
Drugs: Loop, Thiazide, & Thiazide-like Diuretics (↓ renal excretion)
Saturnine gout due to Lead poisoning
Gout Pathogenesis
Inflammatory arthritis triggered by the precipitation of MSU crystals in the joint
Macrophages phagocytose the crystals & produce cytokines that recruit additional Macrophages & neutrophils
Complement is also activated by the crystals
Transient attack of arthritis that typically remits spontaneously in days to weeks
Repeated attacks of acute arthritis eventually lead to chronic Tophaceous arthritis with severe cartilage damage & joint dysfunction
loss of joint space & juxta-articular bone erosions
Acute Gouty arthritis, clinical
Most common in older men
Sudden onset of joint pain with localized hyperemia, warmth
1st attack generally monoarticular:
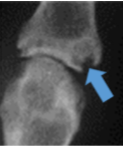
1st metatarsophalangeal joint "Podagra”
Flare lasts hours to weeks if untreated
Acute Gouty Arthritis Morphology
Dense neutrophilic infiltrate of synovium
Monosodium Urate crystals in neutrophils
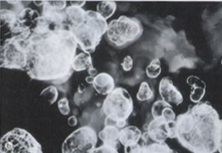
Synovial fluid shows long, slender, needle- shaped, negatively birefringent crystals by polarized light
Acute Gouty Arthritis Synovial Fluid
Group II: Inflammatory-noninfectious
Clarity: transparent/opaque
Color: Cloudy, Pale yellow or white/bloody
3000-75,000 WBC/mL
PMN%: 50-90%
No RBCs
Glucose (blood/SF difference, mg/dL): 0-40
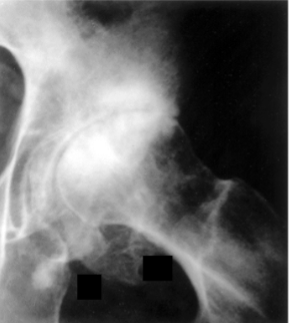
Chronic Tophaceous gout
Chronic gout: Tophaceous gout develops (chronic chalky white deposits of urate crystals in joints, around joints or in soft tissue)
>10 years after 1st attack
Podagra
Bone erosion, loss of joint spaces
Associated with hypertension; Renal disease
↑ risk of cardiovascular disease
Morphology of Chronic Tophaceous gout
Urates heavily encrust articular surfaces
form visible whitish, chalky deposits
Synovium hyperplastic, fibrotic & thickened
Pannus forms; destroys cartilage
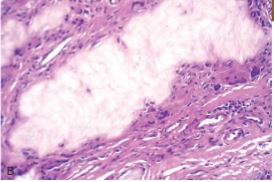
Tophi are the microscopic hallmark
Bone erosions develop adjacent to joints
Ankylosis occurs in severe cases

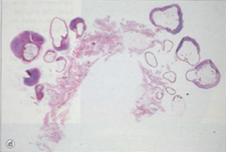
Chronic Tophaceous gout

Chronic Tophaceous gout
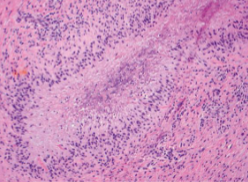
Tophi
Tophi are Pathognomonic of gout
Deposits of chalky white Uric acid crystals surrounded by giant cells
Joints: intra-articular, periarticular in soft tissues or bone
Helix & antihelix of the ear
Achilles tendon
Olecranon & prepatellar bursae
Skin may ulcerate over tophi

Tophi

Tophi
Tophi
Urate/Uric Acid Nephropathy
Obstruction of collecting tubules by crystals in Tumor Lysis Syndrome → Acute Renal Failure
Formation of Uric Acid & calcium oxalate Kidney Stones
Hyperuricosuria increases risk of calcium oxalate stone formation
Chronic Kidney Disease
Tenosynovial Giant Cell Tumors
Related neoplasms of the Synovium lining Joints, Tendon Sheaths or Bursae
Clonal neoplastic proliferations (Benign, but can be locally destructive)
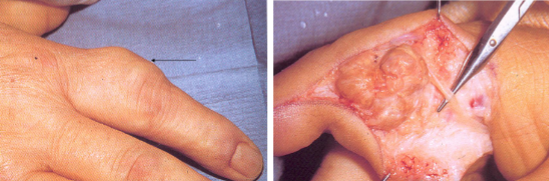
Giant Cell Tumor of Tendon Sheath
Diffuse type/Pigmented Villonodular Synovitis
Age 20-40; Male = female
Pathogenesis: Reciprocal chromosomal translocation, t(1;2) → fusion of type VI collagen promoter with coding sequence of Monocyte CSF gene → Overexpression of M-CSF stimulates production of macrophages
Neoplastic cells are minority of neoplasm
Majority of tumor is infiltrates of macrophages, with hemosiderin; foamy lipid; multinucleated giant cells; fibrosis may occur
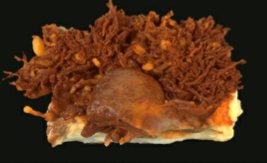
Giant cell tumor of Tendon Sheath
Most common mesenchymal neoplasm of the hand
Localized type of Tenosynovial Giant cell tumor
Involves tendon sheath of wrist, fingers, toe
Presents as a slow-growing, painless mass
May erode underlying bone
Can recur
Solid, golden/yellow nodule attached to synovium
Giant cell tumor of Tendon Sheath
Giant cell tumor of Tendon Sheath
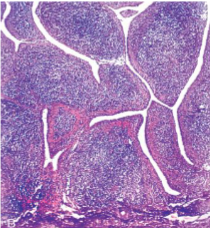
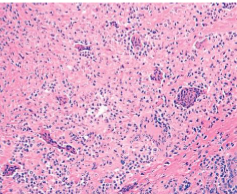
Diffuse Tenosynovial Giant Cell Tumor (Pigmented Villonodular Synovitis)
monoarticular arthritis: pain, locking & swelling of joint
Diffuse growth limits range of motion
Knee, Hip, Ankle
Benign, but tends to aggressive local growth with recurrence after excision
"Pigmented" due to Hemosiderin deposition
Diffuse Tenosynovial Giant Cell Tumor (Pigmented Villonodular Synovitis)
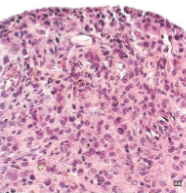
Diffuse Tenosynovial Giant Cell Tumor (Pigmented Villonodular Synovitis)
Diffuse Tenosynovial Giant Cell Tumor Synovial Fluid
Group IV: Hemorrhagic
Clarity: Opaque
Color: Red-brown or Xanthochromic
50-10,000 WBC/mL
PMNs, % < 50%
RNCs predominate
Glucose (blood/SF difference, mg/dL): 0-20