Anti-inflammatories, Steroids
1/65
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
What is inflammation?
A protective physiological response intended to eliminate the initial cause of cell injury as well as the necrotic cells and tissues resulting from the original insult.
What can cause a inflammatory stimulus?
Infection
Mechanical/Trauma
Toxic (foreign substance)
Immunologic/Hypersensitive
Exogenous substances: allergies
Endogenous substances: autoimmune conditions
What is the goal of the inflammatory response?
To get as many white blood cells and other immune system components from the bloodstream into the tissues at the site of the inflammatory stimulus.
What is the physiological sequence of the inflammatory response.
Vasodilation to increase blood flow to site of origin
Increase vascular permeability to allow WBC to enter tissue
Chemotaxis: signals WBC where to go
What are the signs and symptoms from inflammatory response.
Rubor: redness form increased blood flow
Tumor: Swelling from increase vascular permeability
Calor: Heat from increased blood flow
Dolar: pain from increased cellular and fluid swelling, causing increase in pressure → stimulates pain nerves
What are the side effects of an aggressive or chronic inflammatory response?
Neovascularization
Tissue necrosis
Scar formation
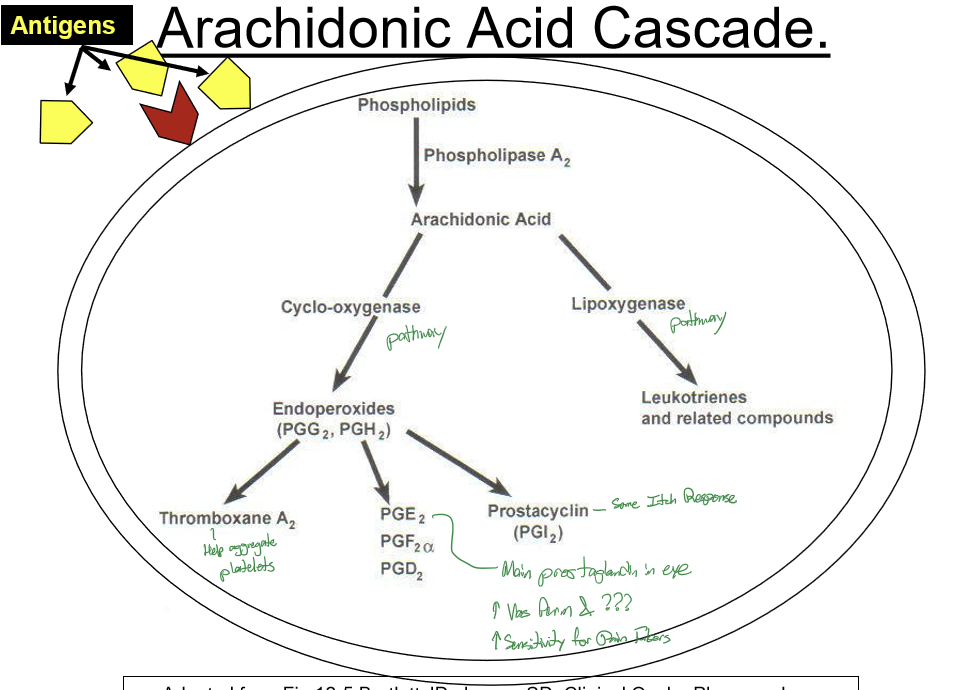
What is the arachidonic acid cascade a response to?
Antigens
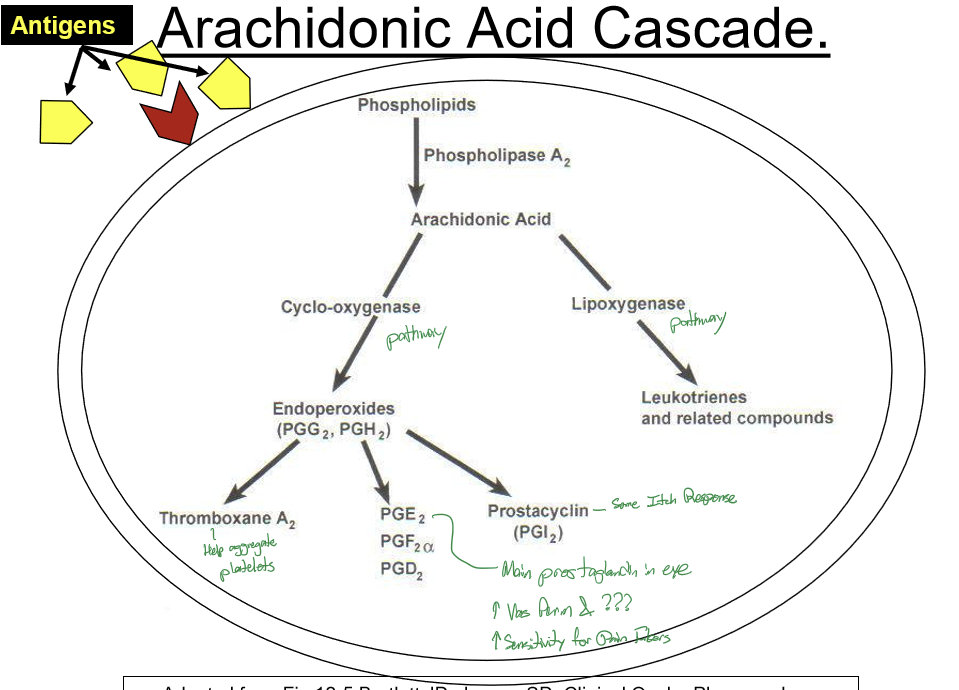
What does Phospholipase A2 do?
It converts phospholipids to arachidonic acid, initiating the arachidonic acid cascade.
What are the major products and effects of the arachidonic acid cascade?
COX pathway: transforms arachidonic acid into prostaglandins and thromboxanes (pain, fever, vasodilation, platelet effects). LOX pathway converts arachidonic acid into leukotrienes (bronchoconstriction, neutrophil recruitment, allergy/asthma).
What inhibits Phospholipase A2?
Corticosteriods
What is the MOA of steriods?
Bind to receptor and pass through cell membrane
Bind cytoplasmic receptor
Enter nuceus to alter protein synthesis: creating lipocortin-1
Lipocortin-1 inhibits Phospholipase A2, limiting the formation of arachidonic acid
What are the therapeutic effects of steroids on the arachidonic acid cycle?
Decrease vasodilation → Decrease redness from PGD2
Decrease vascular permeability to reduce swelling from decreased PGD2 and leukotrienes
Decrease chemotaxis to reduce swelling from decreased leukotrienes
Decrease pain from decreased PGE2
What are the therapeutic effects of steroids outside of the aracidonic acid cycle?
Decrease circulating WBC and lymphocyte proliferation
Inhibit lymphocyte cell mediated response and cytokine synthesis
Inhibit migration of neutrophils
Inhibit Fibroblast proliferation
Inhibit Fibrin deposition
Inhibit Collagen deposition
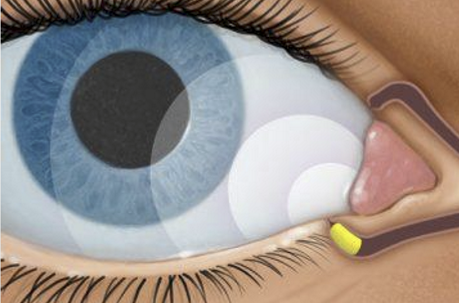
What are the ocular side effects of steroids?
IOP spike: 8-10 mmHg or greater
Posterior subcapsular cataracts
Increase risk of infection
Decrease healing/delayed wound healing
How many people are steriod responders?
7-8% o fgeneral population will have a IOP spike when given steroids.
What increases the risk of being a steroid responder?
If pt has primary open angle glaucoma.
How long does a patient have to be on steroids before there is a risk of an IOP spike?
At least 10 days/2 weeks
How does the risk of posterior subcapsular cataracts change with the route of administration?
Highest risk via intra-ocular injections
2nd highest risk getting PSE via oral administration
What are contraindication for topical ocular steroid use?
Presence or suspicion of infection, expecially of ocular dendritic keratitis
Unsure of diagnosis
Concurrent contact lens wear (must wear glasses when using topical steroids)
What are relative contraindications for topical ocular steroid use?
Epithelial defects. Depends on cause and size. If inflammation is cause, the OK. May need antibiotic/steroid combo for prophylaxis if risk of infection
Glaucoma. FHx of glaucoma increases risk of steroid responder. OK if short term (7-10 days). Can address IOP spike with glaucoma meds
Are there systemic side effects of topical ocular steroid use?
No systemic SE from topical ocular steroid use.
How is anti-inflammatory efficacy determined?
ocular absorption
Receptor affinity
Rate of metabolization
Ketone-based steroids vs ester-based steroids
What are the “…ates” formulation steroid characteristics?
Acetates, prednates, propionates, and etabonates have lipophilic structure and has higher hydrophobicity that leads to greatest tissue absorption and corneal absorption and penetrance.
What are alcohol steroid characteristics?
Have intermediate corneal penetrance.
What are Sodium phosphates (NaPh) steroid characteristics?
Hydrophilic in nature; significantly decrease tissue absorption and corneal penetrance. Is in a solution.
What is Pred Forte?
1.0% prednisolone acetate suspension
Considered the gold standard due to highest efficacy
Due to great absorption, high receptor affinity, ketone based steroid
FDA indications to treat ocular inflammation
Has highest risk for IOP spike d/t super efficacious nature

What are the common uses for Pred Forte?
Uveitis
Keratitis
Post-op inflammation
Moderate-severe ocular surface inflammation

What is Pred Mild?
0.12% prednisolone acetate suspension
No generic available at this conc
FDA indications: open indication to treat ocular inflammation
Rarely used

What is 1.0% prednisolone NaPh?
A solution
Only available as generic
FDA indications: open indication to treat ocular inflammation

What are the common uses of 1.0% prednisolone NaPh?
External diseases of the ocular surface:
Pingueculitis
Allergic conjunctivitis
Episcleritis

What is Durezol?
0.05% difluprednate
Is an emulsion (no shaking required)
Generic version is a suspension
Is equally efficacious as Pred Forte with 50% less dosing
FDA indicated for: uveitis & post-op inflammation and pain
Induces IOP spike like Pred Forte, but not as often and higher in younger patients

What is the dosing of Durezol for post-op?
QID x14 days, then taper accordingly

What is Byqlovi?
0.05% clobestasol propionate suspension
FDA indicated for: post-op inflammation and pain following ocular surgery
Uses Acitve pharmaceutical nanoparticle technology to enhance ocular absorption
Dosage: BID x2wks following surgery
What is Loteprednol etabonate?
The only ester-based steroid
Rapidly metabolized
Nearly equal efficacy to Pred Forte while less likely to induce IOP spike
Good for pt with known steroid response
Good for protracted case of anti-inflammation

Why is Loteprednol etabonate less likely to induce IOP spike?
Natural tissue contains esterases in ocular tissue, therefore can break down drug → increase safety profile as excess drug is metabolized
What are the various formulations of loteprednol etabonate?
Lotemax suspension
Lotemax gel
Lotemax SM gel
Lotemax ointment
Alrex
Inveltys
Eysuvis
What is Lotemax suspension?
0.5% loteprednol etabonate
Open indications for ocular inflammation
Dosage: QID x2weeks, then taper accordingly
Preserved with BAK 0.01%

What is Lotemax gel?
0.5% loteprednol etabonate
Only indicated for use following ocular surgery
Dosage: QID x2weeks, then taper accordingly
Preserved with BAK 0.003%

What is Lotemax SM gel?
0.38% loteprednol etabonate GEL
Only indicated for use following ocular surgery
Dosage: TID x2weeks, then taper accordingly
Preserved with BAK 0.003%

What is Lotemax ointment?
0.5% loteprednol etabone
Only indated for use following ocular surgery
Dosage: QID x2weeks, then taper accordingly
Non-preserved

What is Alrex?
0.2% loteprednol etabonate
Suspension
Only FDA indicated for allergic conjunctivitis
What is Inveltys?
1.0% loteprednol etabonate
Suspension
AMPPLIFY
FDA indicated for post-op inflammation
Dosage: 1gt BID x2weeks

What is Eysuvis?
0.25% loteprednol etabonate
Suspension
AMPPLIFY
FDA indicated for short-term treatment of signs and symptoms of inflammatory dry eye
Dosage: 1gt QID x up to 2wks

What is AMPPLIFY?
nanotech drug delivery with mucus-penetrating particles (MPP) to increase corneal and intraocular absorption
What are the common uses for loteprednol?
Dry eye (short-term use as diagnostic agent or management of flare-ups)
Inflammatory keratitis (DOC for Thygeson’s SPK)
Post-op inflammation (particularly refractive surgery)
Episcleritis (particularly nodular)
Allergic conjunctivitis
DOC for Giant Papillary Conjunctivitis (GPC)
and Vernal Keratoconjunctivitis (VKC)
Any inflammatory condition requiring long, protracted steriod therapy due to its safety profile
What is Maxidex?
0.1% dexsamethasone alcohol
Targets cells in Anterior chamber more than target tissues in cornea
Suspension
Also available in generic
FDA indicated for ocular inflammation
Has highest chance to induce IOP spike
Not as efficacious as Loteprednol etabonate

What is FML?
0.1% fluorometholone alcohol
Least to induce IOP spike
Suspension
Available in generic (preferred drug on insurance formularies)
FDA indicated for ocular inflammation
Commonly used for: episcleritis, superficial inflammation
What is FML Forte?
0.25% fluorometholone alcohol
FDA indicated for ocular inflammation
Rarely used, no generic available in 0.25%
What is Flarex?
0.1% fluorometholone acetate
Suspension
FDA indicated for ocular inflammation
Rarely used, no generic available
Possible benefit in treating protracted or recalcitrant Thygeson’s Keratits
Does not have high receptor affinity → weak therapeutic effect

Rate the order of efficacy of the topical ophthalmic steroids. 1 being the most effective and 5 being the least.
a) Pred Forte
b) DurezolLotemax/Inveltys
Maxidex
Alrex/Eysuvis
FML/Flarex
Rate the risk of the topical ophthalmic steroids inducing an IOP spike. 1 being the most likely and 5 being the least likely.
Maxidex (* increase frequency)
a) Durezol
b) Pred ForteLotemax/Inveltys
Alrex/Eysuvis
FML/Flarex
What are the guidelines for dosing topical ophthalmic steroids?
Dosage and length of course of Tx is determined by severity of presentation
If condition warrants steroid Tx, initial dosage usually no less than QID
For mild to moderate inflammation, common dosage is QID x7 days
Initial dosage for significant cases of uveitis is commonly Q1h with Pred Forte or Q2h with Durezol
When is tapering topical ophthalmic steroids necessary?
High dosage (> QID)
Long duration of Tx (> 10-14 days)
When and how do you taper steroids?
Taper only when improvement is seen on a follow up at current dose
To taper: reduce dosage frequency by <50% of previous usage.
Typically, do not teed to taper after BID (to QD)
What is the purpose of pulse dosing? When would one pulse dose?
Purpose: rapidly reach peak drug conc in the target tissue to have an early impact on significant symptoms
Pulsing is done when more severe symptoms warrant it
Do ophthalmic formulations cause systemic side effects?
Almost never
Do short-term ocular use of topical steroids cause any ocular side effects?
Rarely. But can affect IOP or PSC, so it is best to treat aggressively to limit length of Tx.
Are there refills for topical steroids?
No. Have pt discard after use.
What is Dextenza?
0.4 mg dexamethasone intracanalicular insert
FDA approved for: inflammation and pain following ophthalmic surgery & allergic conjunctivitis
Sustained release for 30 days
Improved compliance vs. ~70 drops in 30 days
No need for removal, disintegrates and flushed thru nasolacrimal system
What is 0.1% triamcinolone cream?
Dermatological use
For short term use for acute dermatitis of periocular adnexa
Not for use on the ocular surface
10 times efficacy of OTC 1% hydrocortisone
Rx: TID x 3d, then BID x 3d
SE: high dose or chronic/excessive use on skin can lead to thinning and/or depigmentation of skin.
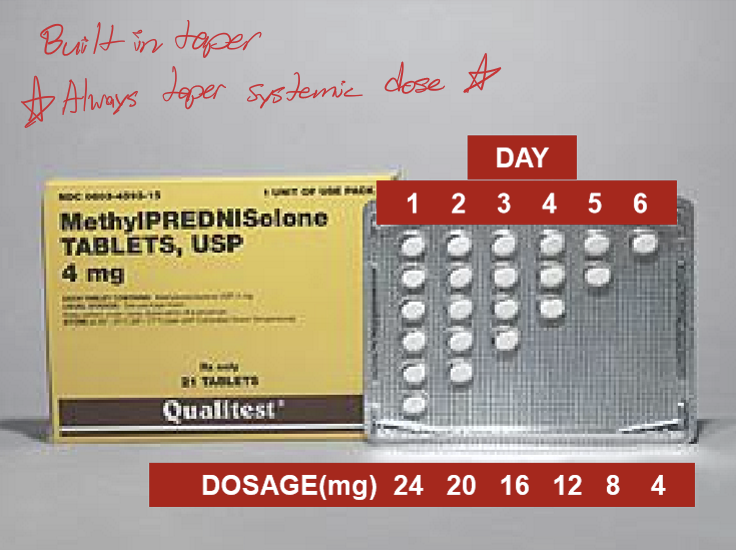
What are some systemic steroids?
Prednisone and Medrol (methylprednisolone)
What are the ocular indications for prescribing systemic steroids?
Allergic inflammation of the conjunctiva, lids, and adnexa (Only indication allowed for ODs in OH)
Graves Ophthalmopathy
Orbital Pseudotumor
Retinal Vasculitis
Uveitis
Myasthenia Gravis
Giant Cell Arteritis
What can cause allergic inflammation of the conjunctiva, lids, and adnexa.
Contact Dermatitis
Severe Allergic conjunctivitis/blepharitis
Poison Ivy
Bee stings

What are the restrictions for prescribing oral steroids in ohio?
Only for adults 18 years and older
Methylprednisolone only
Amount that does not exceed a single course of therapy (no refills)
single course of 6 day oral steroids per episode
Prescribed on basis of an individual’s particular episode of illness
What are the SE of chronic, long-term use of systemic steroid use?
Muscle wasting and altered fat distribution = Cushing’s syndrome
Suppress adreno-pituitary axis → adrenal insufficiency → malaise, myalgia, muscle atrophy, hypotension, increased risk of infection, decreased wound healing
Osteoporosis
Steroid psychosis
Thinning and depigmentation of the skin
What are the SE of short-term systemic steroid use?
Peptic uclers (from protective prostaglandins inhibited)
Recommended OTC proton-pump inhibitor to counter act upset stomach and nausea
Increased blood glucose (typically for out of control type 1 DM)
Pregnancy (not contraindication, but most consult w/ OB-GYN)