Chapter 33: Trauma to Head, Neck, and Spine
1/47
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
48 Terms
Motor vs sensory neurons
Motor nerves from brain, sensory to brain
Cranium definition and parts
Cranium: portion of skull enclosing brain. Frontal, temporal (ears) , occipital (back), parietal (top of head), cranial floor is beneath the brain. Cranial bones fused to create sutures, immovable joints
Face bones
Face bones: mandible (lower jaw, only non suture of face), temporomandibular joint (joint of mandible), maxillae (upper jaw), nasal bones, malar/zygomatic (cheekbones), orbits (eye sockets), lacrimal (tear ducts)
Foramen Magnum
space where spinal cord meets brain
Meninges layers
Dura mater
Arachnoid
Pia mater
Spinous process
bumpy part of spinal column you feel along back
Atlas vs Axis
Atlas: C1, holds up head
Axis:C2 allows head to turn
5 sections of vertebrae and amounts
Cervical (C1-7)
Thoracic (T1-12)
Lumbar (L1-5)
Sacrum (S1-5)
Coccyx (CO1-4)
Scalp
has lots of vessels so injury causes bleeding, direct pressure and treat like soft tissue injury, tho careful if skull injury don't apply pressure if injury site shows bone fragments or depression of bone or brain exposed, just use loose gauze
Direct vs indirect injuries on brain
Direct: from open head injuries
Indirect: open or closed, shock of impact on skull transferred to brain
Traumatic brain injury
Traumatic brain injury: disrupts normal function of brain
Concussion
force transferred to the brain from fall or blunt force. May lose memory or have headache/lose consciousness for a few seconds, arms/groggy, sensitivity to light, nausea
Contusion
bruised brain, when force of blow great enough to rupture blood vessels, often caused by brain hitting skull and bouncing. Contrecoup injury: when bruising happens on side opposite of blow (coup opposite)
Laceration and Hematoma
Laceration: can occur from same thing contusion does since inside of skull has sharp ridges, or from penetrating object
Hematoma: can be subdural (between brain and dura) epidural (between dura and skull) intracerebral (blood within brain)
Process of interracial pressure
When hematoma happens pressure builds inside skull, causes neurologic issues, reduces blood to brain, can cause herniation which is when brain forced downward towards foramen magnus, compressing brainstem (causes ams dilated pupils, increased systolic, decreased pulse, abnormal respirations)
Abnormal respirations include cheynes stokes breathing (quick breathing then stops, quick stops), central neurogenic hyperventilation (rapid breathing), ataxic respirations (irregular/unpredictable)
Small subdural hematoma could take long for signs, epidural can instantly
Cushings reflex:Will see increased bp as brain tries to perfuse, slow heart rate from rest of body reacting or from compression of vagus nerve
Carbon dioxide will build causing pressure to increase more
As herniation continues may have decerebrate (extended, arched back) or decorticate posturing (arms look like gonna fight)
For significant hematoma sequence looks like
Strikes head, may have brief loc
After 10m slight ams
Ams worsens bp starts to increase
Seizure (can happen at any time from pressure or injury)
Unresponsive, cushing's reflex
Decorticate →decerebrate→death
Herniation
brain forced downwared towards foramen magnus from pressure buildup
Cheynes Stokes Breathing
(quick breathing then stops, quick stops),
Central neurogenic hyperventilation
rapid breathing
ataxic respirations
irregular/unpredictable
cvushings reflex
Will see increased bp as brain tries to perfuse, slow heart rate from rest of body reacting or from compression of vagus nerve
decerabrate vs decorticate posturing
As herniation continues may have decerebrate (extended, arched back) or decorticate posturing (arms look like gonna fight)
signs/care of interracial pressure
Ams, laceration/hematoma, goose egg, battles sign (late, bruise behind ear), pupils unequally/unreactive, raccoon eyes (late) CSF from ears/nose, irregular breathing, cushings, personality change, trouble balance, seizures, temp increase, vomiting.
Hypoperfusion Shock not normally sign except in infants cause not enough space in skull for bleeding
High priority, care like normal, keep person calm, don't stop cSD from flowing, lose gauze dressing
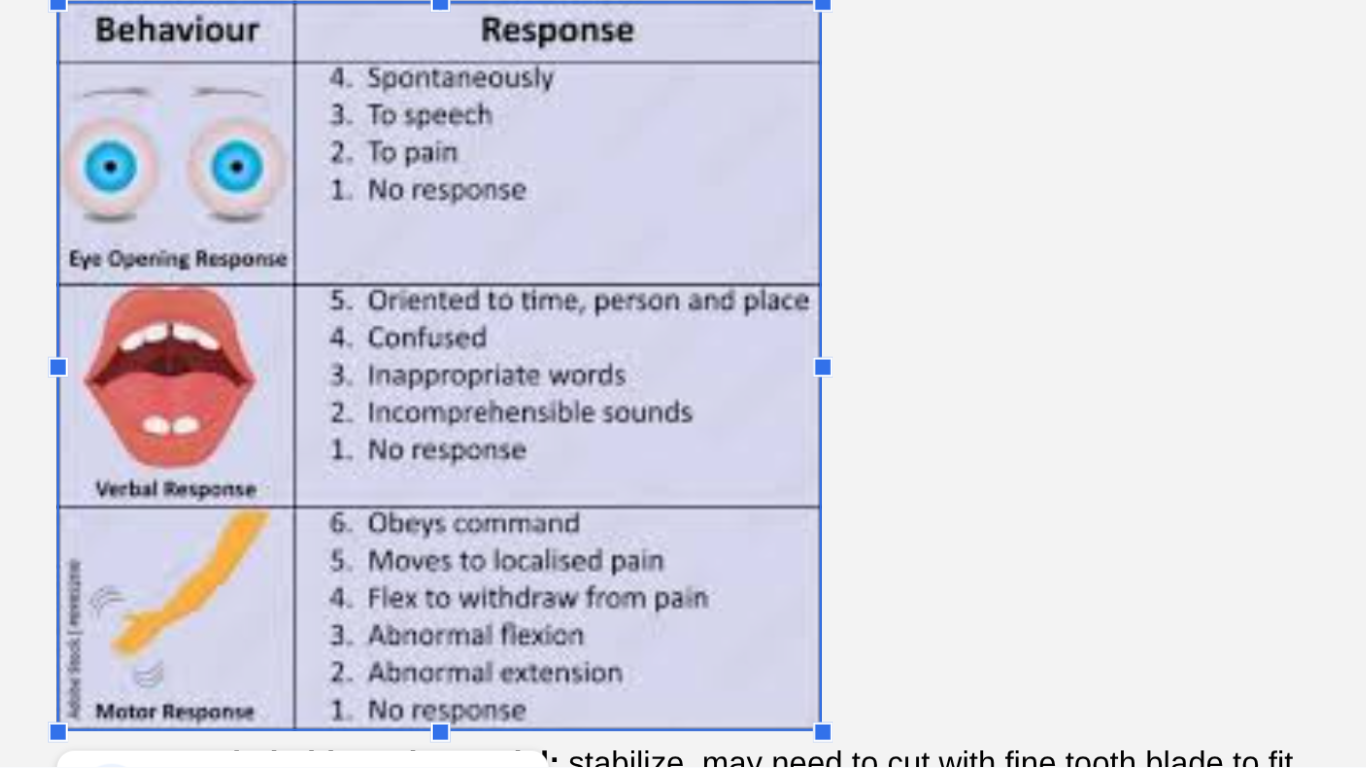
gcs
neck wounds + care
Lots of large vessels, pressure lower than atmosphere so could suck air and cause embolism,
Care: direct pressure, occlusive dressing (2 inches post wound), dressing over occlusive pressure as needed dont compress both carotid arteries at once, once bleeding stopped bandage dressing in place
primary vs secondary spine injuries
Primary injuries (occur immediately and from direct force, often irreversible since nerves dont heal well)
Secondary injuries: (after initial insult from things like hypoxia, shock, swelling of cord, hypoglycemia)
Always consider spine injuries when serious trauma to any part of body
whiplash vs axial loading vs distraction spinal injuries
:most often from energy that forces spine beyond normal range of motion like flexion or extension (whiplash) or from overrotation like twisting or compression (axial loading) or distraction (excessive pulling)
what makes you vulnerable/ what parts are most vulnerable of spine
:Thorax is typically well protected as well as sacrum. Cervical and lumbar susceptible, osteoporosis makes it more susceptible, ligament laxity from pregnancy/down syndrome as well. Fused vertebrae or fixed flexion deformities at higher risk. Ankylosing spondylitis causes vertebrae to fuse
high risk moi of spine
Falls over 3 ft or more than 5 stairs
Axial loading (compression) injuries like diving
High speed collisions
Atv crashes
Bicycle collisions
Geriatric more severe
low risk moi
penetrating trauma, low energy collisions
assessing spine
Pain and tenderness in injured area good sign
Pain with movement, changes in neurologic function or paresthesia, paralysis
Impaired breathing: if only slight movement of abdomen and no chest movement, diaphragmal breathing from damage to nerves commonly injured, as well as ribs collapsing on inhalation.
Priapism, peeing
Deformity (rare)
Neurogenic shock
key elements of nexus
key elements of nexus
Is the patient reliable?
Is there any pain or tenderness along the midline spine?
Are there focal or neurologic signs or symptoms?
Is there a distracting injury or circumstance?
What is the MOI in a pediatric patient?
what is bad when lung injury present/what negative effects of spine board
Flat immobilization of patients with lung injury bad
Even short periods on a spine board can cause hypothermia and pressure sores
3 centers of mass that when prevented from moving spine is stable
shoulder girdle, head, pelvis
what shape is spine naturally and what position should vertebrae stay in
s shaped, vertebrae stay in position of function known as inline neutral position
1st step of spinal care
manual stabilization of head first step (maintain neutral, if out of neutral can move unless complains of pain)
2nd step of spine care
Collar next to prevent movement (maintain manual until on backboard, check cms in extremities once restricted)
next step of spinal care
Once cervical spine done, can use ambulance stretchers (considered padded backboards) rigid less commonly used
when to use backboards/when not to
Backboards used when:
Transport time short
Likely needs cpr
Big splint for multiple injuries
Moving from backboard to stretcher causes excessive movement
Backboard contraindicated when respiratory distress, scoop helpful to move to stretcher
vacuum mattresses
Vacuum mattresses: more comfy, can lose rigidity over time and rob heat from patient
seated patients
can either place long spine board under butt and lower to supine or patient stands then sits on stretcher
If using flexible extrication device or short spine board secure torso first head last
special considerations for short board
Special considerations for short board (Study last)
Assess the back, shoulder blades, arms, and collarbones before placing the device
– The EMT applying the board must angle it to fit between the arms of the rescuer stabilizing the head
– The uppermost holes must be level with the patient’s shoulders; the base should not extend past the coccyx
Never place a chin cup or strap on the patient
– Avoid applying the first torso strap too tightly
– Some buckles have quick-release mechanisms
– Do not pad between the collar and the board; only pad to fill an occipital void
how to apply long backboard
log roll onto, pad voids between head and torso, secure head last, blankets for additional head immobilization, tilt pregnant to left after immobilization, strap across upper chest, pelvis, thighs
6 and under pad beneath shoulder blades
standing patients care
cervical collar and sit on stretcher, guide supine or semi-sitting, secure straps
helmet
if airway intact dont remove helmet if it causes pain or is difficult, when it fits snug, can immobilize with helmet, doesnt interfere with assessment, remove if cardiac arrest, don't remove just helmet or just shoulder pads
multiple trauma patients vs multi system trauma
Multiple Trauma patient: more than one serious injury
Multisystem trauma patient: one+ injuries serious enough to affect >1 body systems
When multi system trauma is severe
Severe if (physiologic)
Ams (gcs<14)
Head injury
Hypotension (systolic <90) shock, internal bleeding\
Abnormal respiratory rates (head injury, later stages of shock)
Severe if (anatomic)
Amputation proximal to wrist/ankle
Pelvic fractures
open/depressed skull fracture
Paralysis
Penetrating injuries to head, neck, torso, extremities proximal to elbow/knee
Chest wall instability/deformity
2+ proximal long bone fractures
Crushed, degloved, mangled, pulseless extremity
Severe if (MOI)
Falls
High risk auto crash (intrusion, ejection, death, telemetry data)
Severe if (Special)
Old cant compensate for shock
Children to pediatric facility
Patients taking anticoagulants/pregnant
golden hour
(need for critical patients to get to surgery within 1 hour of injury
trauma scoring
Includes systolic bp, respiratory rate, gcs, out of 12 lowest 0 rating system, objectively describes severity