Cardiac Tumors & Masses
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
53 Terms
Moderator Band AKA:
Septomarginal Trabecula
Moderator Band (Septomarginal Trabecula)
thick bundle of muscle traversing the RV
variable size
often verifies RV in fetal scanning
seen in lower 1/3
more toward apex
not always visualized
may act as a protective mechanism to resist RV overdistension
Normal Variants:
Prominent RV Trabeculations
enhanced by RVH
atrial appendage lined w/ pectinate m
Ridge of Marshall
Ridge of Marshall AKA:
Coumadin Ridge
Warfarin Ridge
Ridge of Marshall
tissue separating LAA and LUPV
may be confused w/ clot

Fat
can be found anywhere in heart
appears echogenic
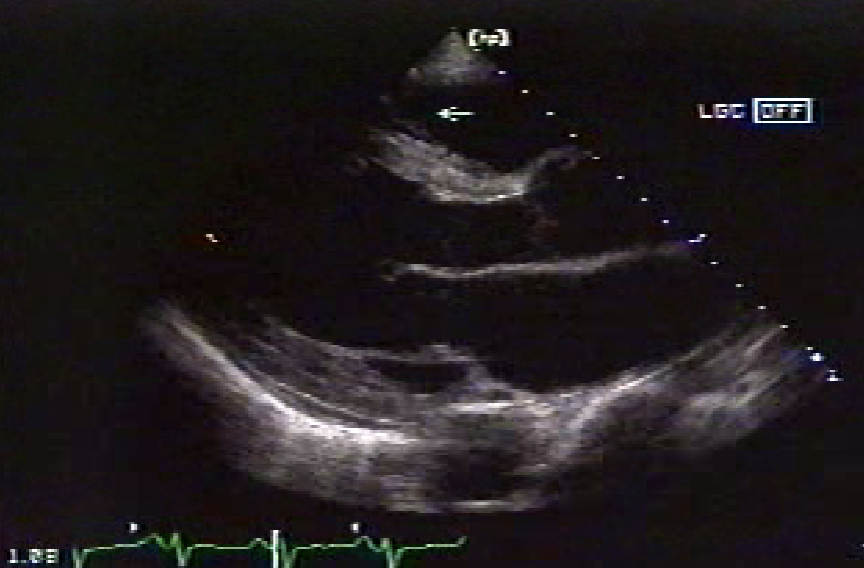
Epicardial Fat Pad
often located anteriorly
sandwiched between epicardium and myocardium
seen PLAX if anterior
appears anechoic in this location
can mimic loculated pericardial effusion
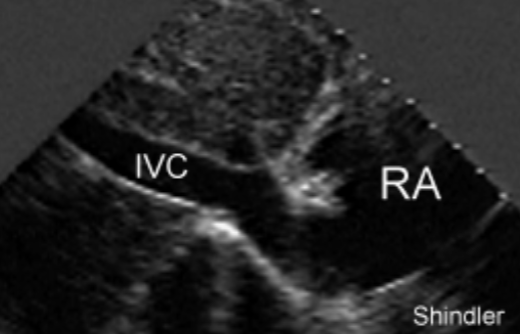
Eustachian Valve
a membranous, endocardial tissue flap
located at opening of the IVC into RA
may produce flow obstruction
IVC may become dilated
needs to be determined from pathological mass / tumor
Eustachian Valve during fetal circulation:
directs blood from RA to PFO (patent foramen ovale)
serves no significant purpose in adult
Thebesian Valve
a flap of endocardial tissue that guards the Coronary Sinus opening into the RA
often continuous w/ the Eustachian valve
not typically referenced in clinical practice

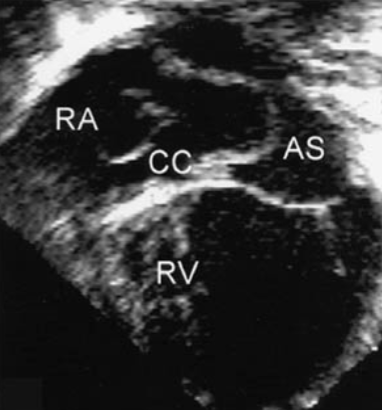
Chiari Network
a freely mobile, lace/mesh-like membrane
located in RA near orifice of coronary sinus
embryonic remnant
similar to Eustachian
seen in 2-3% of the pop
needs to be DDX’d from mass or tumor
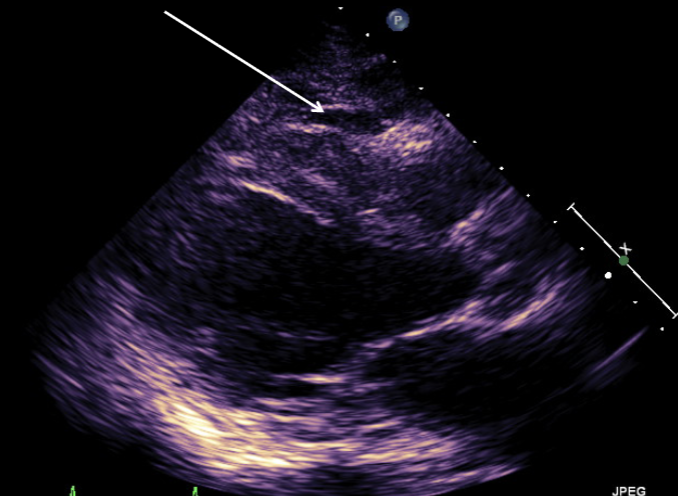
LV Bands or False Tendons
traverse the LV cavity
may be multiple
seen in any view of the LV
if prominent can produce confusing echos
clinical significance is unknown
rarely produce symptoms
What are other DDx’s for cardiac tumors / masses?
MAC
calcified papillary muscles
artifacts:
near field gain
main bang
side lobes
Cardiac Tumor Categories:
Primary
Metastatic / Secondary
Primary Cardiac Tumors
originate w/in the heart
classified as:
benign (75%)
malignant (25%)
Metastatic / Secondary Cardiac Tumors
originate from a primary malignancy located somewhere else in the body
more common than primary tumors
Types of Primary Benign Cardiac Tumors:
Myxoma
50% of primary benign tumors
Papilloma / Papillary Fibroelastoma
10%
Lipoma
10%
Fibroma
4% of primary benign tumors
Rhabdomyoma
What is the most common benign tumor of the adult population?
Myxoma
What is the most common benign tumor found in children?
Rhabdomyoma
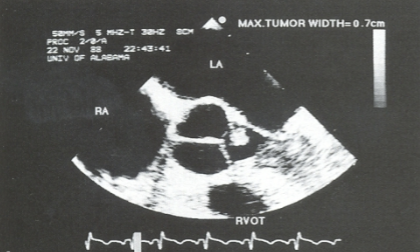
Myxoma
neoplasm that arises from endocardial tissue
80% located in LA
RA 2nd most common
usually attached by a stalk to the IAS
“pedunculated”
often arises from IAS
near region of fossa ovalis
Where might a Myxoma originate at?
atrial appendage
origin of a pulmonary vein
Myxoma characteristics:
polypoid mass of gelatinous tissue
tumor is usually mobile + moves w/ blood flow
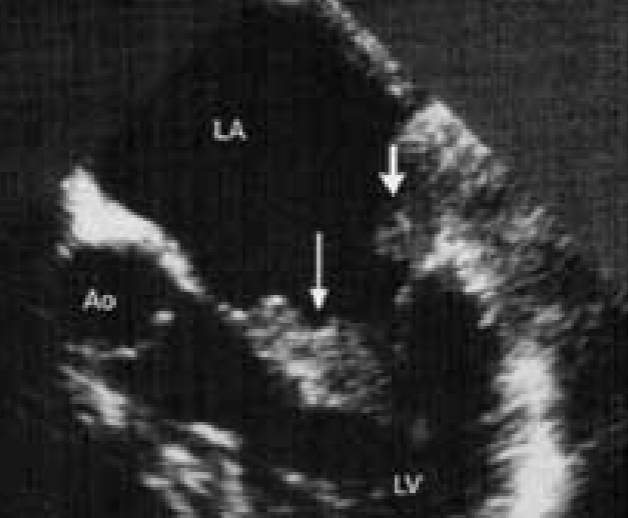
Classic LA Myxoma
echogenic mass located in the body of the LA in systole and prolapses through the mitral orifice in diastole
causes stenosis if large enough
narrowing of orifice
mimics MS
Potential risks of a Myxoma include:
pt’s are at high risk for embolization
systemic or pulmonary
death
d/t obstruction of flow, arrhythmia, emboli
tumor may re-occur
can grow back after surgical removal
if seed still remains
Myxoma symptoms:
asymptomatic → small
Systemic embolization
from possible tumor fragments
MV / TV obstruction
from tumor’s prolapsing motion into valve during diastole
CP
Dyspnea / DOE
Hemoptysis
Pulm edema
syncope
weakness / fatigue
cachexia
weight loss
Myxoma Auscultastion
New / acquired / “changing” cardiac murmur → tumor “plop”
Myxoma EKG findings:
conduction disturbances
arrhythmias
a-fib
atrial flutter
bundle branch blocks
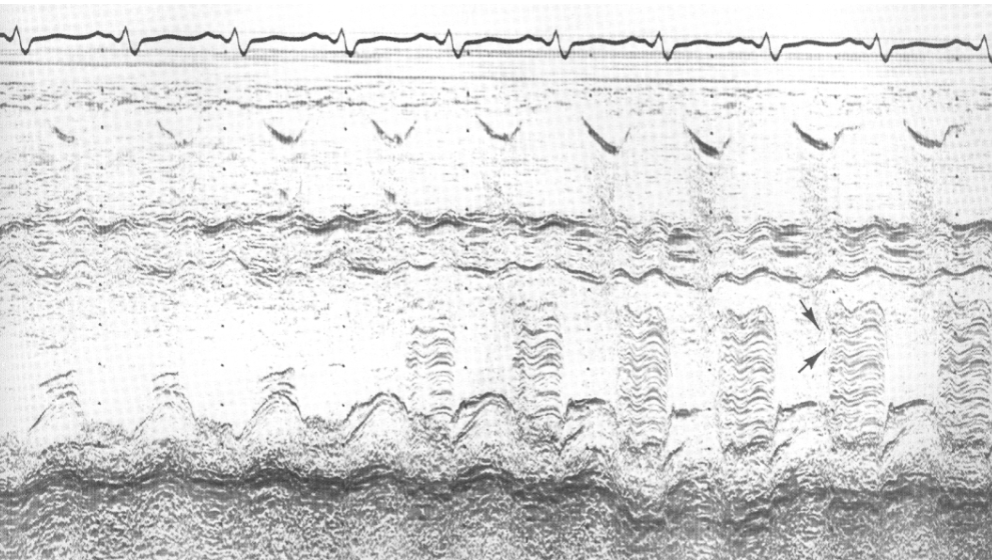
Myxoma m-mode findings:
blunted E-point of MV
reduced E-F slope
can mimic MS
heavy band of echoes behind AMVL in diastole
What does a Myxoma most closely mimic?
MS
Myxoma 2D findings:
visualization of myxoma
allows detection, location, + sizing
exaggerated motion of myxoma
d/t prolapsing from LA into the LV
Myxoma Doppler findings:
mimics valvular MS findings
MR may be noted
What is a new method of Myxoma diagnosis?
Myocardial Contrast Echocardiography
contrast agent injection directly into the CA’s
shows normal myocardial perfusion
a myxoma will light up d/t contrast perfusion
thrombus will not absorb contrast
Other methods of Myxoma diagnosis:
coronary angiography
Myxoma Treatment:
prompt surgical excision
serial echocardiography to R/O reoccurrence after surgical removal
LA myxoma can reoccur if ‘seed’ is not removed
similar to a wart
some pt’s given anti-coag’s + rescanned within 1 month
to differentiate from a thrombus
Papilloma / Papillary Fibroelastoma
most common tumor of cardiac valves + valve apparatus
can arise from any endocardial surface
most common: AoV, MV, TV in children
small, pedunculated benign tumor
attached by a single stalk
very mobile
clinical significance is unclear
noted to be an emboli source d/t attracting platelets / fibrin
DDx: Endocarditis & Lambl’s excrescence
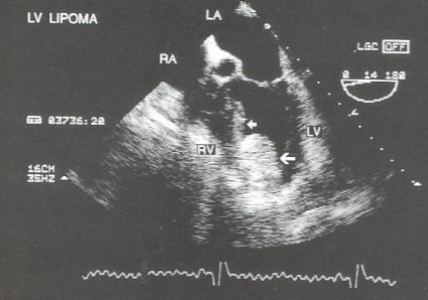
Lipoma
neoplasm of mature fat cells
well-defined, homogenous, dense mass
can invade all 3 heart layers
Types of Lipomas:
Fibrolipomas
contain fibrous connective tissue component along w/ fat
Myolipomas
contain muscular tissue along w/ fat
Where are Lipomas usually located?
LV
RA
IAS
termed: Lipomatous Hypertrophy of IAS
Lipomatous Hypertrophy of IAS
most common Lipoma location is IAS
“Dumbell” shaped IAS
d/t IAS thickening w/ sparing of fossa ovalis
may cause A-fib
associated w/ steroid use

Fibroma
most commonly arise from LV free wall or IVS
intramural
embedded in myocardium
can extend into chambers as they enlarge
does not invade the pericardium
malignant counterpart will → fibrosarcoma
Fibromas may cause:
obstruction to LV inflow or outflow
associated w/ sudden death
CHF
arrhythmias
Characteristics of Fibromas include:
isolated
slow growing
un-capsulated
well-circumscribed
highly echogenic
Rhabdomyoma
found at birth and <1 yr
70-90% have multiple tumors
associated w/ tuberous sclerosis
found in ventricular walls
more common in RV
solid, echo-dense mass protruding into ventricular cavity
mortality d/t blood flow obstruction
have been reported to recede over time

What is the most common tumor found in children?
Rhabdomyoma
Other primary benign heart tumors include:
hemangioma
teratoma
Hemangioma
vascular tumor
located in any chamber
right heart > lt
Teratoma
composed of skeletal, nerve, connective tissues
teeth, hair, skeletal components may be found
located in RA, RV, + septum
Angiosarcoma
RA location 80%
most common primary malignant tumor of the heart
may cause inflow obstruction
associated w/ pericardial effusion
Angiosarcoma note:
applies to a wide range of malignant endothelial vascular neoplasms that affect a variety of sites
skin, liver, bone, breast, spleen, heart
Other Primary Malignant Intracardiac Tumors in order of MOST to least common:
Rhabdomyosarcoma
Mesothelioma
Fibrosarcoma
Osteosarcoma
Mesothelioma
malignant intracardiac tumor d/t asbestos exposure
occur in pericardium of heart, but most commonly found in pleural lining (lungs)
Metastatic / Secondary Intracardiac Tumors
pericardial > myocardial involvement
pericardial effusion
often the 1st indication
heart invaded by:
malignancy of breast or lung
sarcoma
melanoma
lymphoma (can also invade myocardium)
Renal, Liver, Wilm’s tumors
extend from IVC to RA (1st) and RV (2nd)
rarely affects LV function
What extracardiac tumors may compress cardiac structures?
mediastinal tumors/cysts
thymus
lymphoma
pericardial tumors/cysts
pleural tumor
hematoma
teratoma
pancreatic cyst
diaphragmatic hernia