Pupil Assessment
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
What is the pupil?
An opening in the centre of the iris
controlled by sphincter + dilator muscles
Which muscle causes pupil constriction?
iris sphincter contracts causing constriction → miosis
closest to pupil
Which muscle causes pupil dilation?
The radial dilator muscle contracts causing dilation→ mydriasis
What is the Relationship between sphincter and dilator muscles
They are antagonistic muscles working in opposition
What are the Three main pupillary reflexes?
1) Light/dark reflex
2) near reflex
3) and psychosensory reflex
What is the Light/dark reflex?
pupils constrict in response to bright light
pupils dilate in dark
What is the Near reflex?
Accommodation and convergence are linked with pupil constriction
(Near Triad)
What is the Psychosensory reflex?
can override light reflex + relates to emotional state
Pleasant emotions = pupil dilation (arousal,fear shock etc → fight or flight)
Unpleasant emotions = pupil constriction (anger, boredom)
What are the Functions of the pupil?
Controls depth of focus→ pupil constriction gives greater depth of focus
Signalling → pleasant emotional states or shocking stimuli → pupil dilation
controls how much light enters eye → protective effect e.g reducing UV
aids night vision by minimising amount of light adaptation that occurs → speeds up dark adaptation
minimising aberrations from peripheral cornea/lens
What is the Stiles–Crawford effect?
light appears brightest when entering centre of pupil
as cones in retina been directed towards centre of pupil
lower photoreceptor response from orthogonal rays
so large pupils dont limit our acuity vastly
Why large pupils do not greatly reduce acuity
Peripheral rays stimulate cones less effectively.
Parasympathetic innervation controls
iris sphincter controlled by parasympathetic nerves
responsible for constriciton
Sympathetic innervation controls
Pupil dilation via the dilator muscle
What is the Afferent pathway of pupillary light reflex
light enters + stimulates Retina → optic nerve → optic chiasm
fibres from nasal retina cross to opposite (contralateral side ) temporal fibres stay on same (ipsilateral )side
→ fibres project to pretectal nuclei in midbrain
→ pretectal nuclei project fibres to both ipsilateral + contralateral Edinger Westphal Nuclei
Crossing at optic chiasm (pupil reflex)
Nasal retinal fibres cross; temporal fibres remain ipsilateral.
Role of pretectal nuclei
Project to both Edinger–Westphal nuclei.
What is the Efferent pathway of light reflex (Parasympathetic Pathway)
Edinger–Westphal nucleus → CN III → ciliary ganglion → short ciliary nerves → sphincter
What is the Consensual response?
fibres from both eyes synapse onto both pretectal nuclei which innervate both Edinger Westphal nuclei
Light in one eye causes EQUAL constriction of both pupils
What is the Pupillary Dark reflex mechanism
pupils dilate in response to darkness
results from contraction of radial dilator muscle of iris + under control of sympathetic pathway
afferent pathway can be described as retina signalling an absence of light to hypothalamus in brain
What is the Sympathetic pathway → efferent pathway
originates in hypothalamus in brain → spinal cord → chest cavity → alongside carotid artery → enters eye via LONG ciliary nerves
What are the effects of problems that arise from the sympathetic pathway ?
Results in a miotic pupil because parasympathetic nerves which control constriction are unopposed
diseases arising in spinal cord, chest + neck → lung cancer + aneurysm can sometimes manifest with ocular sign
—> Horner’s syndrome
What does the Near response involve?
> Triad :
Pupillary constriction
Accommodation
Convergence
> response is automatic when an out of focus near object viewed
> stimulus = blurred retinal image + equal in both eyes
> occurs to maximise resolution acuity rather than to allow greater lag of accommodation
What is the normal adult pupil size range
Approximately 2–8 mm → varies with age + room illumination
Key features to assess on inspection of the pupil
Shape → should be round
Equality → do both pupils look equal
What is the Direct pupillary response (pen torch)
does pupil constrict when light shone directly into eye
What is the Consensual pupillary response (pen torch)
Constriction of the fellow eye when light shone onto other eye
What is the Near response assessment?
Pupils constrict when moving from distance to near target
What is the Relative afferent pupillary defect (RAPD)?
swinging flashlight test → alternate between both eyes
is there a relative difference in pupil cosntrcition
What is Heterochromia?
difference in colour of two irides
usually congenital
if acquired associated with:
Cataract
Glaucoma
Iridocylitis → type of uveitis
Iris melanoma (cancer)
What is a RAPD?
Relative Afferent Pupillary Defect
tests for problems in afferent pathway → is there a asymmetrical defect in optic nerve or retina
affected eye will DILATE when light shone onto it as signals cant reach brain
under normal lighting conditions both pupils appear equal → consensual reponse
AKA Marcuss-Gunn Pupil
causes: Advanced glaucoma, retinal detachment , central retinal artery occlusion
How pupil reactions are recorded
Tick box grid → direct, consensual + near
Number scale → 0-4 where 0 is no relation and 4 is brisk normal reaction
PERRLA → Pupils equally round & Reactive to Light and Accommodation
generally write ‘no RAPD’ and ‘no Aniscocoria’ next to all of above if appropriate
What Is Physiological anisocoria?
one pupil naturally slightly larger than the other
What are the Key features of physiological anisocoria?
Size difference <1 mm + consistent in all lighting
present in ~15-20% of pop
present at birth
no visual side effects
Pupil appearance in Horner’s syndrome
Miotic → more noticeable in dim light

Pathway affected in Horner’s syndrome
Sympathetic pathway.
Other signs of Horner’s syndrome
Ptosis with normal light response
Why Horner’s syndrome is concerning
May indicate life threatening conditions such as stroke or lung tumour, spinal cord tumour
can be checked at hospital through instillation of a drop that block sympathetic pathway → 10% cocaine
causes pupils to dilate in physiological aniscocoria
but NO DILATION of affected eye in Horner;s syndrome
Adie’s pupil appearance
Dilated pupil and slow to react in reponse to light
Key feature of Adie’s pupil
Light–near dissociation → responds normally to near objects but slow to re-dilate at distance
rare neurological disorder → idiopathic
may indicate selective degeneration of nerves supplying parasympathetic pupil pathway → ciliary ganglion
non-progresive + unilateral
may also be called Tonic Pupil or Holmes-adie pupil
may complain of light sensitivity
Typical demographic for Adie’s pupil
More common in females + avg age of onset around 30 years
No Tx required
Long-term change in Adie’s pupil
May become miotic over time ('little old Adie')
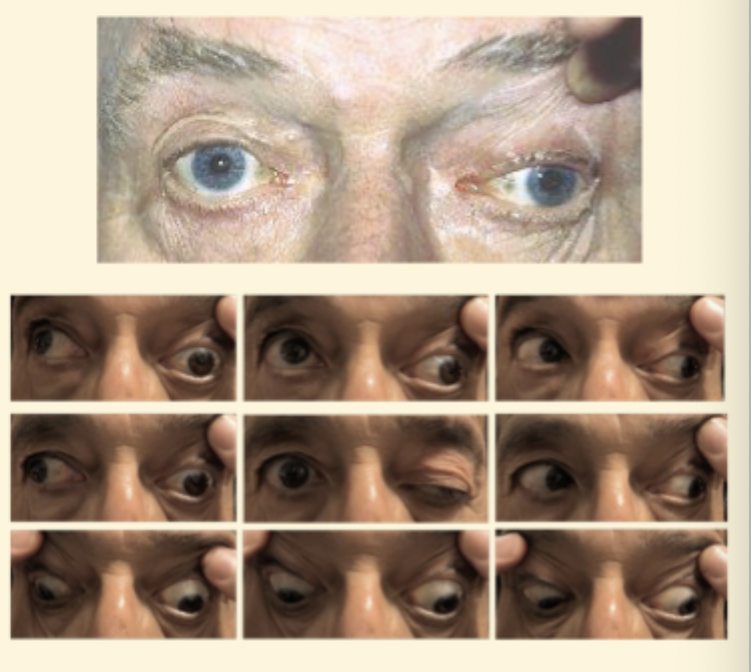
What are the Signs of third nerve palsy?
Ptosis
dilated pupil
eye positioned 'down and out'
Px likely to complain of diploma if acquired
Common causes of third nerve palsy
Ischaemia
aneurysm
tumour
What is an Iris coloboma?
Congenital abormaility where iris doesn’t form properly
can also affect retina + optic nerve
What is Persistent pupillary membrane?
Remnants of membrane that supplied blood to lens during development
Iris trauma after cataract surgery
clips used to hold pupil open
May result in irregular pupil shape