MIDI3 M2L2 : Local Anesthesia
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
What are some clinical indications to utilize topical anesthesia ?
Highly vascularized lacs <5cm
- best on face scalp
- can be liquid or gel
Topical Amide anesthetic (EMLA/LET) is used for intact skin anesthesia and (EMLA/LET) is used for non-intact skin anesthesia
- EMLA cream (Lido/Prilocaine)
- LET gel (lido, epi, and tetracaine))
What are the 3 main types of Local anesthesia?
1) Topical
2) Direct Infiltration/injection
3) Regional/entire extremity (i.e. digital blocks)
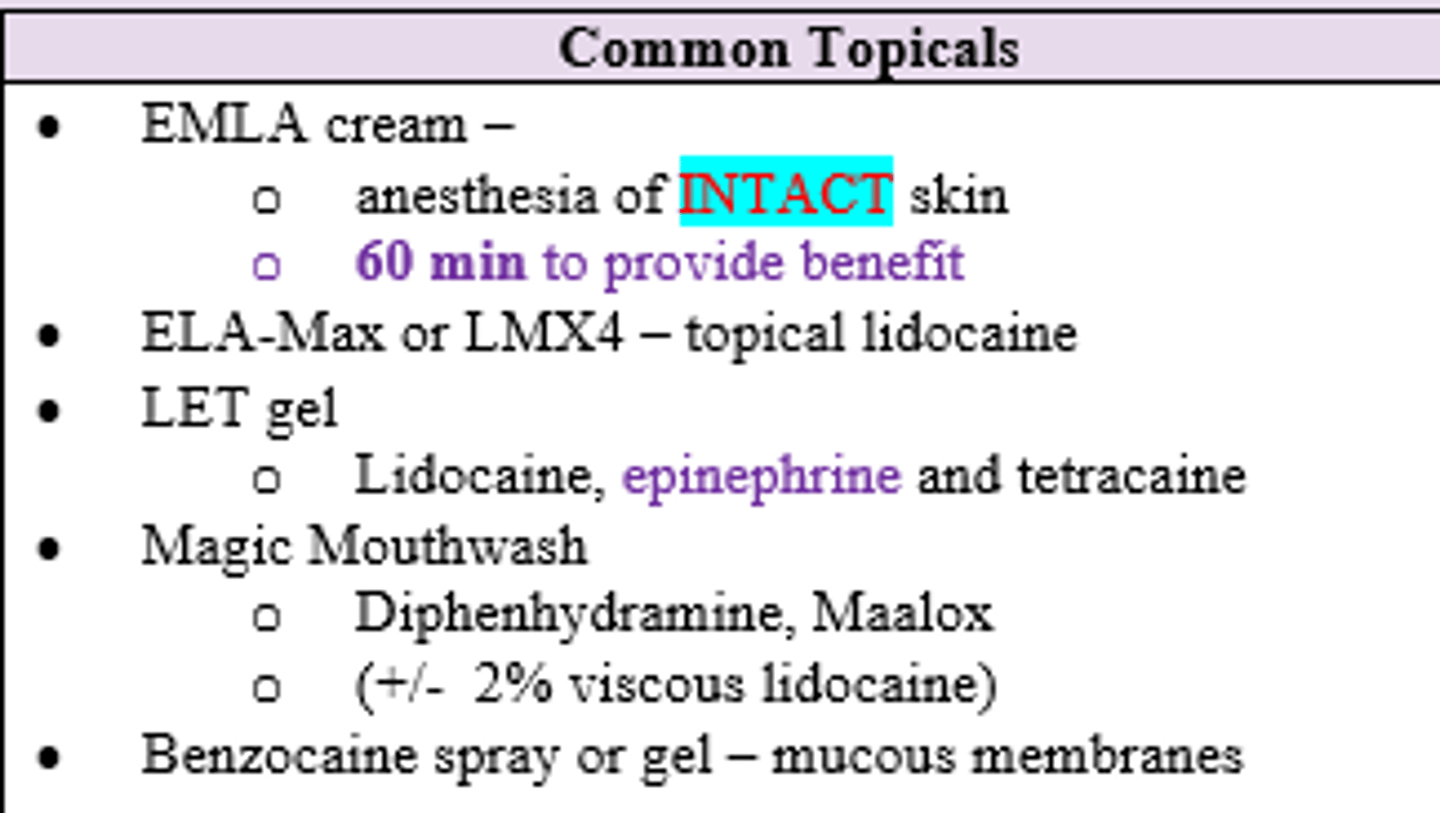
Which common topical anesthetic/analgesics are good for mucous membranes and throat/oral lesions?
- Benzocaine spray/gel
- Magic Mouthwash (Diphenhydramine, Maalox +/- lido)
When using LET as topical anesthetic, what is an indication that complete anesthesia is reached?
Zone of blanching around wound (d/t Epi)

Which topical anesthetic takes ~60 minutes for full benefit?
EMLA (Prilocaine / Lido) cream
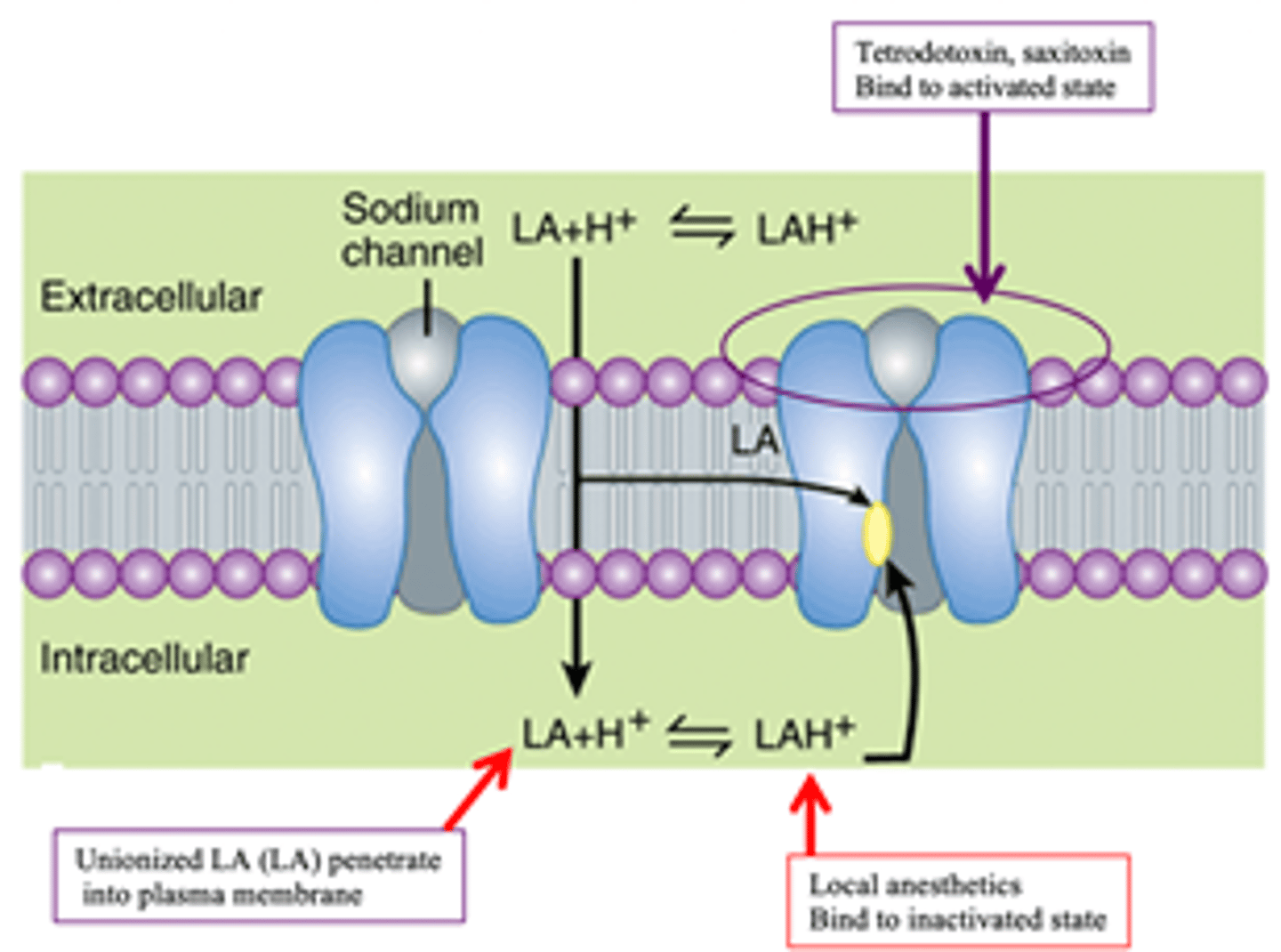
What is the MOA of Local anesthetics?
Reversibly block sodium (Na+) channels, thus preventing depolarization (reduces influx of Na+) which will block conduction of nerve impulses
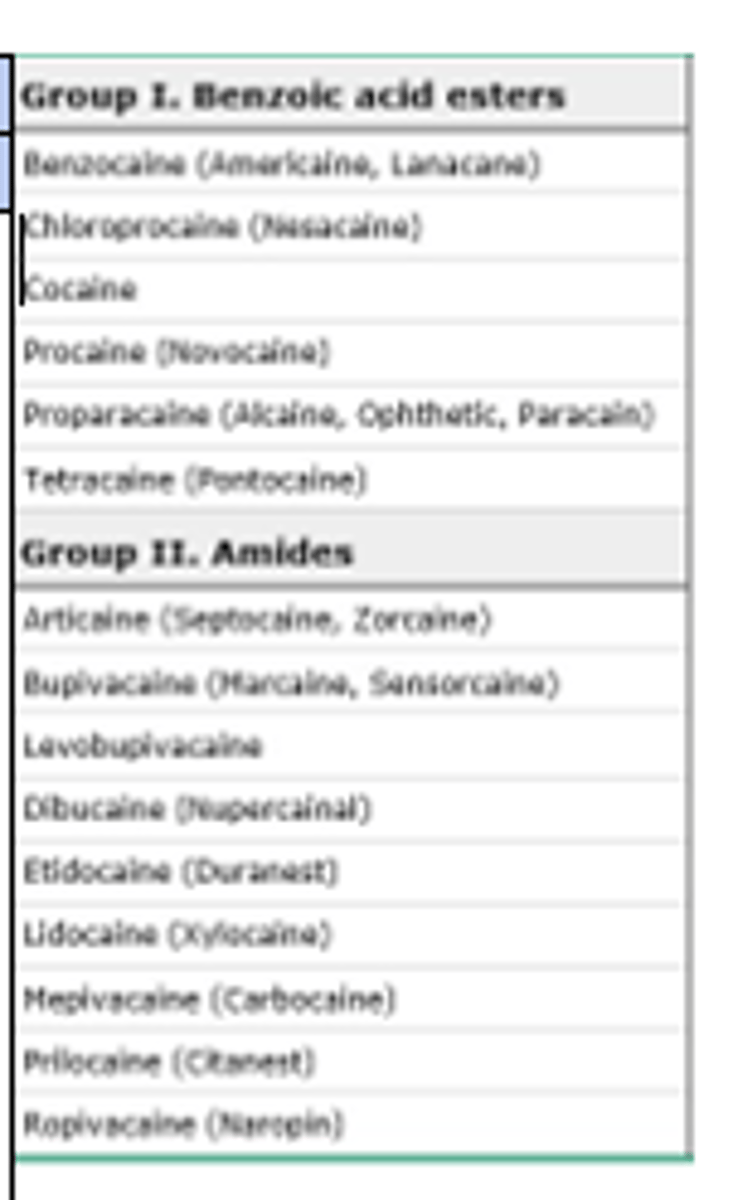
Cocaine, Procaine (Novacaine), Proparacaine, Tetracaine, and Benzocaine are all examples of (amides/esters) LA's
Esters
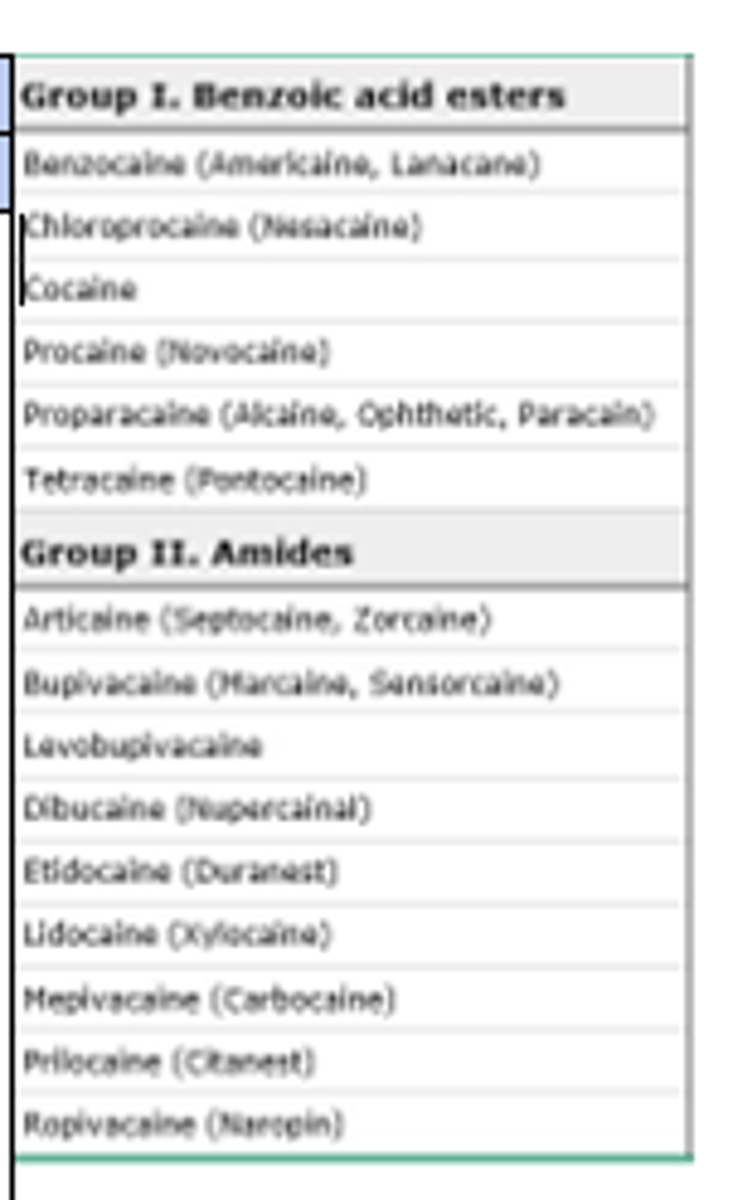
Lidocaine, Mepivacaine, Bupivacaine, and Prilocaine (EMLA) are all examples of (amides/esters) LA's
Amides
**extra i before -caine **
Esters have a (shorter/longer) t1/2 than amides
shorter (metabolized by tissue/excreted by kidneys vs amides which are metabolized by liver)
What clinical significance does the metabolism of Esters have?
Metabolized into PABA by pseudocholinesterase and excreted by the kidneys
PABA can cause contact dermatitis (thus Esters are more common to cause allergy-type reactions compared to Amides)
What are the 8 factors that affect the effectiveness of anesthesia?
- Rate of nerve conduction
- Size of nerve fiber diameter
- prescence of myelin
- anesthetic solution pKa and tissue pH
- Vascularity
- Use of Epinephrine
- Technique
- Concentration and dosing
- Metabolism
How does nerve size affect the effectiveness of anesthesia?
larger nerve = larger dose needed
Which nerve fibers are the most sensitive to local anesthesia?
smaller, unmyelinated pain fibers

LAs are more likely to bind to sodium (NA+) channels that have (rapid/slow) action potential
Rapid (i.e pain sensory nerve fibers anesthetize the quickest)
Bc Local Anesthetic is nonspecific it can act on all sensory nerves, however some nerves quicker than others. What nerve signals get blocked by LAs the fastest > slowest?
Pain > Temp > Touch > Proprioception > Motor
(this is why you need to warn people irrigation will still feel cold even if they're numb to pain)
Most anesthetic solutions are (basic/acidic)
Acidic
- causes burning sensation with injection due to alkaline pH of tissue
- (+) Sodium Bicarb buffer can eliminate pain, increase onset of action, duration of blockade, and degrade Epi
Adding Epinephrine (increases/decreases) pH of an anesthetic
Decreases / makes more acidic
- thus increases burning sensation d/t becoming more acidic
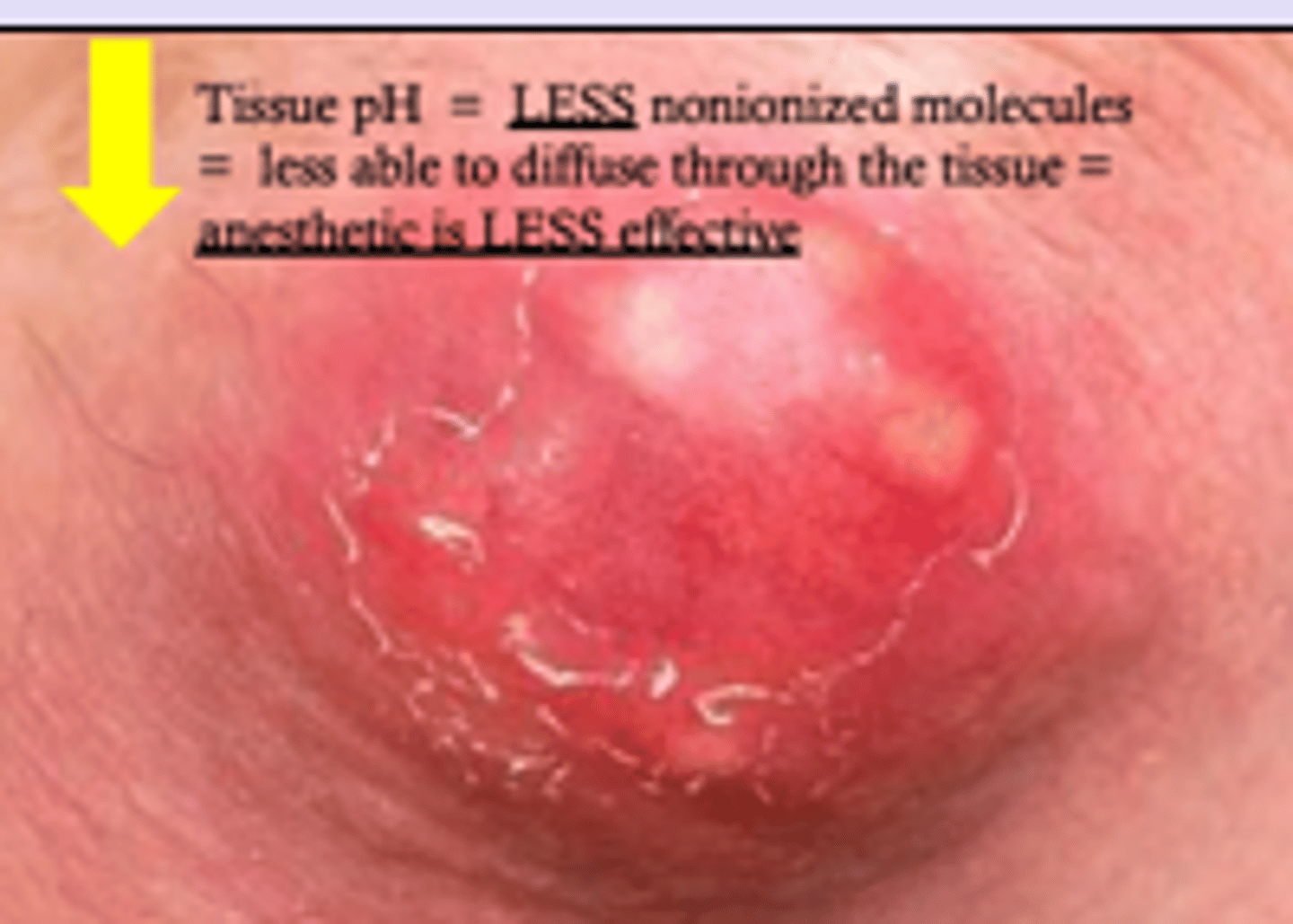
Why are anesthetics less effective in infected tissues (i.e. abscesses)?
Metabolic acidosis (lactic acid) occurring in tissue
- decreased pH keeps LA ionized
- preventing it's movement through tissue
**anesthetics work best at physiologic basic pH
What is the best indicator of the onset and duration of the anesthetic blockade?
pKa of anesthetic compared to the pH of the tissue

Which Ester Local Anesthetic is the only one not vasodilating and therefore doesn't ever need Epinephrine (vasoconstricting) added to it?
Cocaine (vasoconstricting)
What happens when you inject local anesthetic to highly vascularized area?
- it gets rapidly removed
- shorter duration of action
- either have to give more or add vasoconstricting agent like Epi
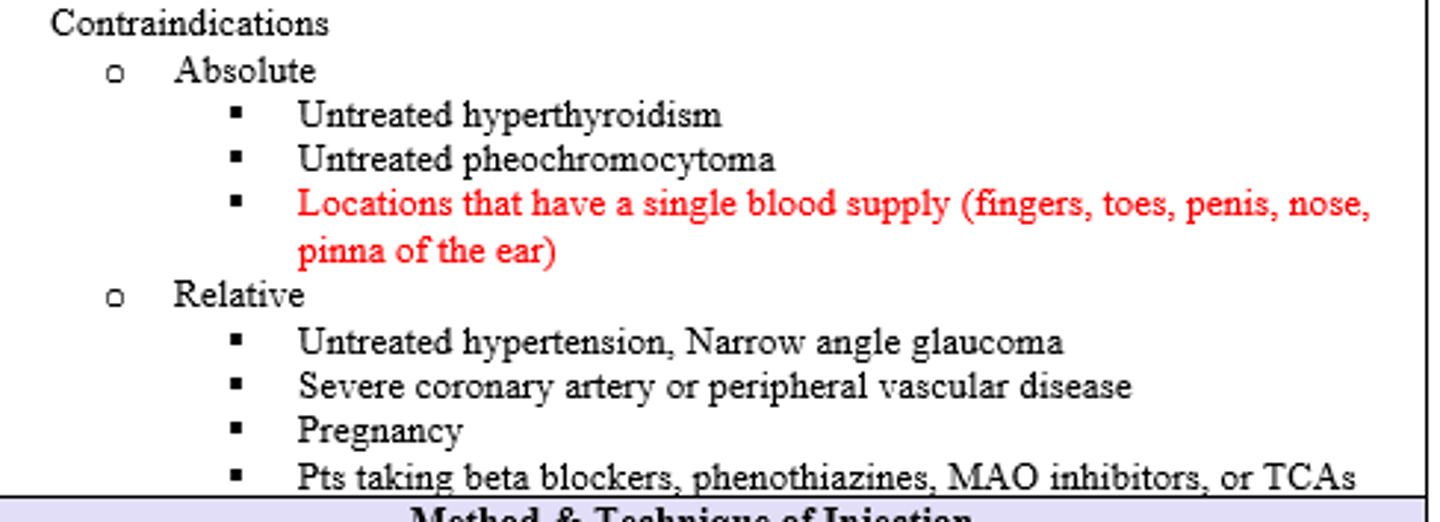
Which areas are contraindicated from receiving Lidocaine with Epi?
areas with single dependent or tiny vascular supply (i.e. fingers, toes, penis, nose, and pinna of ear)
Untreated Hyperthyroidism and untreated Pheochromocytoma are (absolute/relative) contraindications for Epinephrine with Lidocaine
ABSOLUTE
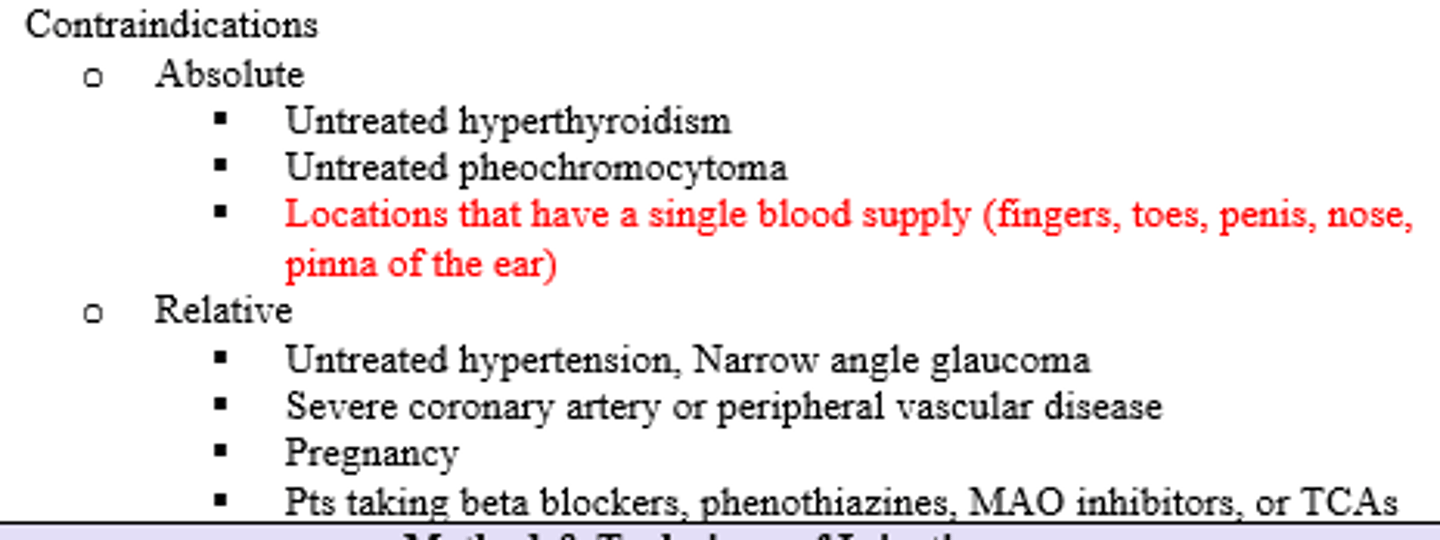
Untreated HTN, Narrow Angle Glaucoma, severe CAD/PVD, Pregnancy and use of Beta blockers, Phenothiazines, MAO-Is/TCAs are (absolute/relative) contraindications for Epinephrine with lidocaine
Relative
Where in the skin layer should local anesthetics be directed to achieve immediate blockade / pain relief ?
Junction of Dermis and Subcutaneous fat (fascia)
What are the max doses for the following:
Lido 1% without epi
Lido 1% with epi
Topical Lido
Lido 1% without epi: 4-4.5 mg/kg
Lido 1% with epi: 7 mg/kg
Topical Lido: 2-5mL of mixture
What are some clinical indications to utilize local anesthesia ?
indicated in ANY procedure confined to one area in which pain/discomfort is associated with the procedure
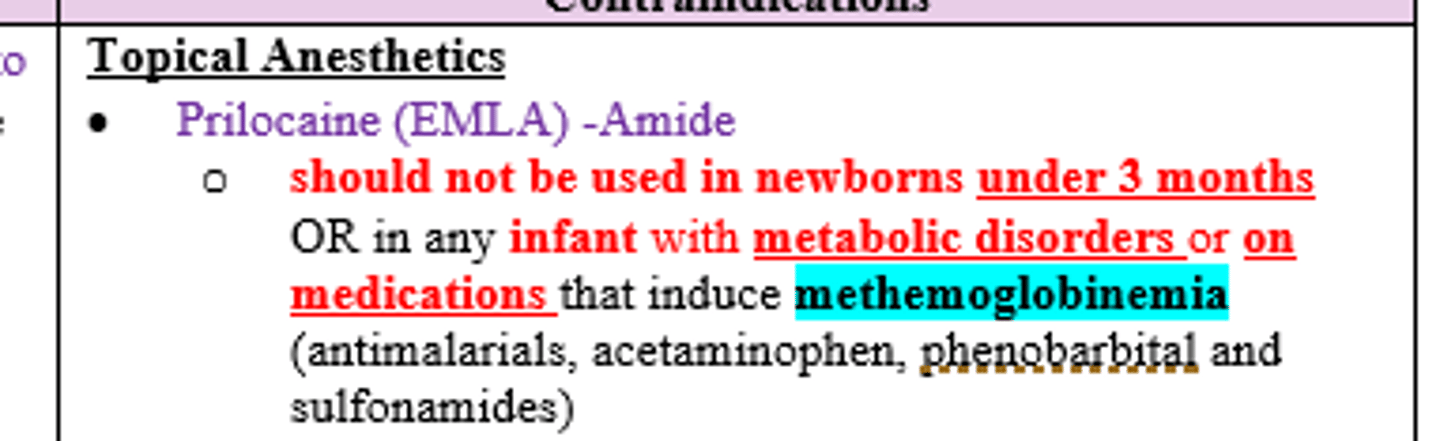
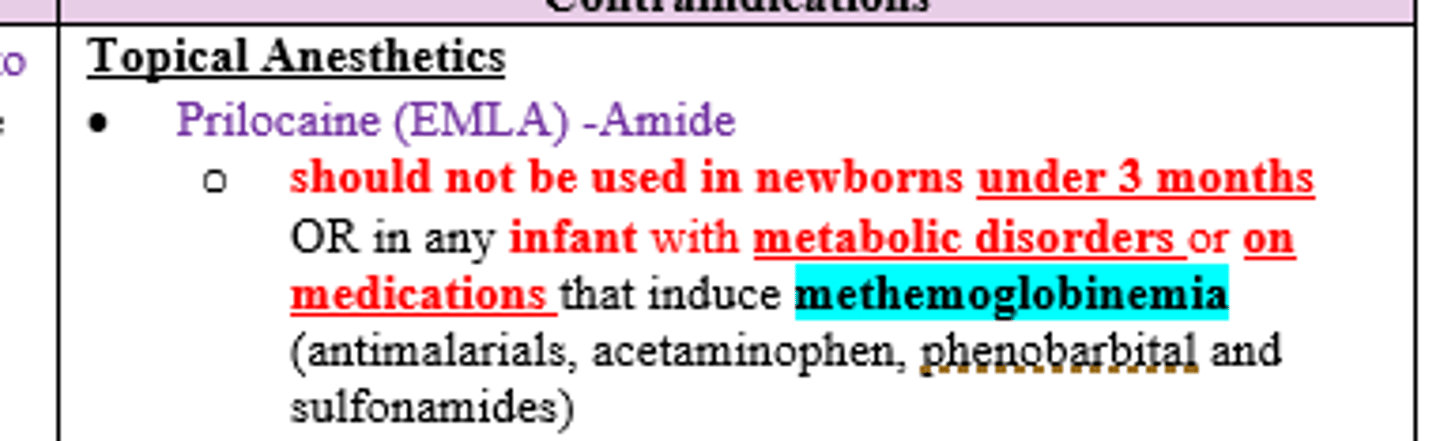
What are some contraindications to using Prilocaine (EMLA, amide) topical cream ?
Newborns <3 mos or any infant with metabolic disorders or on meds that induce methemoglobinemia (antimalarials, acetaminophen, phenobarbital, and sulfa)
What are some contraindications to using local anesthesia ?
- unstable BP
- True allergy (mc in ester)
- Severe Liver disease (for amides)
- Severe Renal disease (for esters)
- Mental instability
During dental procedure, patient experiences cocaine (an ester) toxicity. What physiological abnormality could have caused this?
Pseudocholinesterase Deficiency
- esters are metabolized by this enzyme and if decreased clearance occurs (i.e. severe liver disease, renal failure, pregnancy, and neonates) it will result in LA toxicity (seizures, hypotension, etc.)
Amide anesthetics are metabolized by what and where?
CYP450 enzyme degradation in the Liver
Patient with lac on hand needs numbing prior to sutures, what is the importance of patient preparation prior to administering local anesthesia ?
ALWAYS check neurovascular status before any anesthesia
What are the various techniques that can minimize the discomfort of the infiltration of local anesthetics ?
- Talk, explain, reassure
- Deep breaths
- Supine positioning
Procedure in which an electrical current is passed through skin soaked in tap water (not distilled water), normal saline (0.9%), or a solution containing an anticholinergic medication, which allows ionized (charged) particles to cross the normal skin barrier
Iontophoresis
What can be offered to a patient who needs LA but has a true allergy to both esters and amides?
Direct infiltration w/ Diphenhydramine (Benadryl) or Saline (vs nothing vs conscious sedation)
- more painful
- cannot be reduced with buffering
How can you avoid systemic complications of local anesthesia?
aspirating (checking for accidental vessel penetration / blood) before injecting
Which ester commonly causes contact dermatitis when used topically (and found in lots of sunburn creams)?
Benzocaine
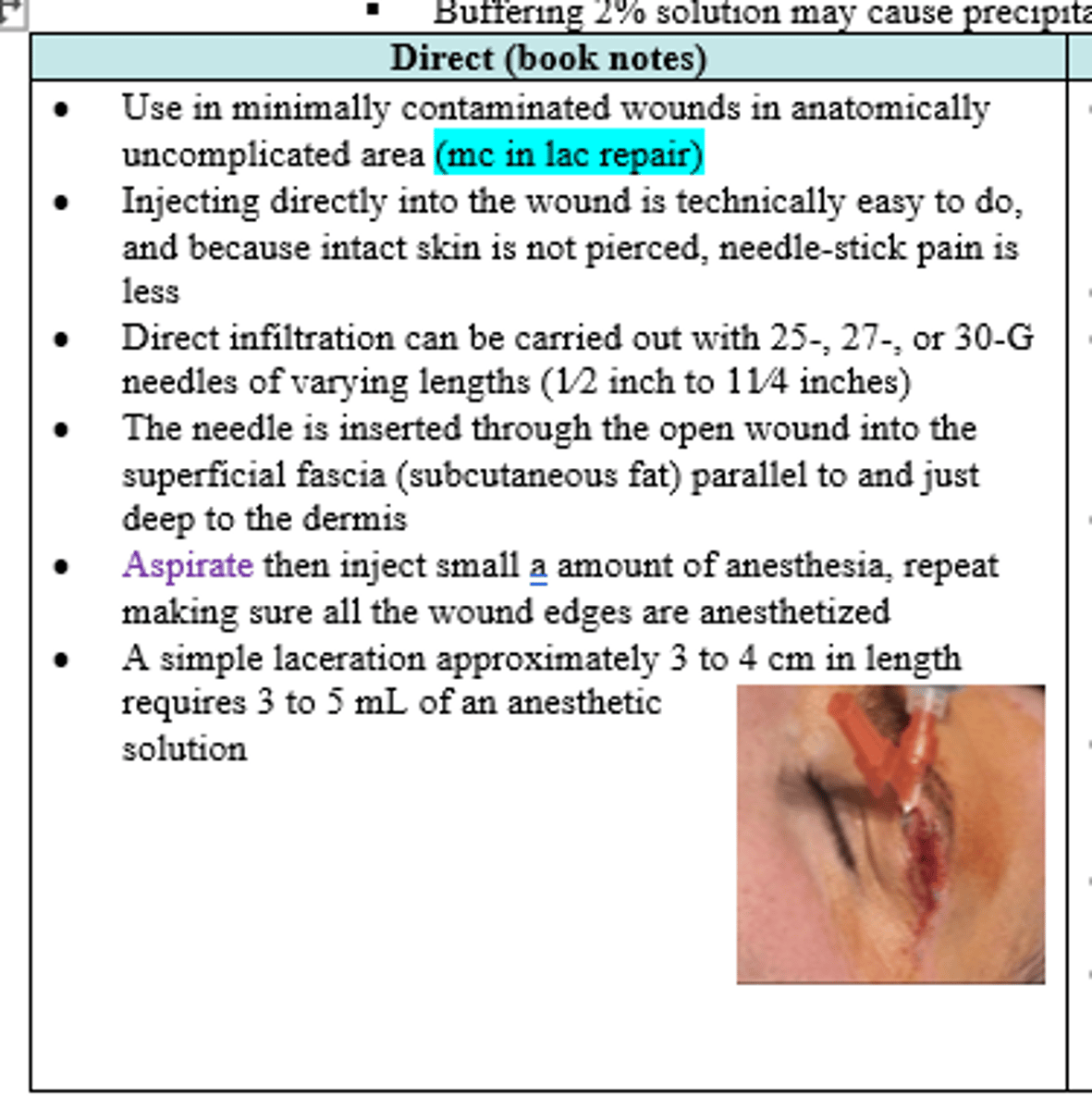
What type of local anesthetic injection is most commonly utilized in simple, clean laceration repair?
Direct (25,27,30g 1/2 to 11/4")
T/F Epi with lidocaine increases duration of action and improves local hemostasis
True
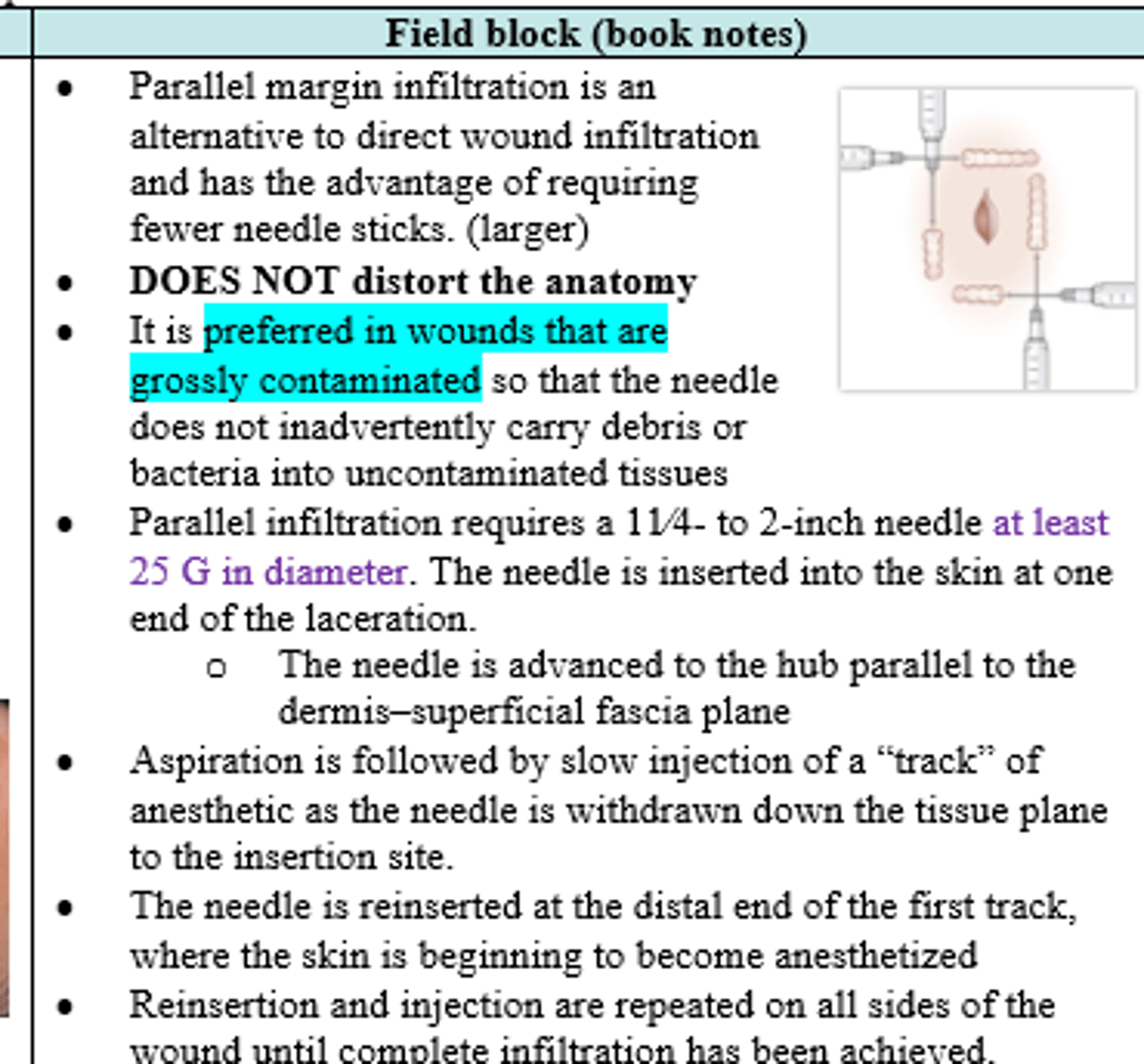
Field blocks (distort/ do not distort) anatomy (i.e. good for ear lacerations)
Do not distort
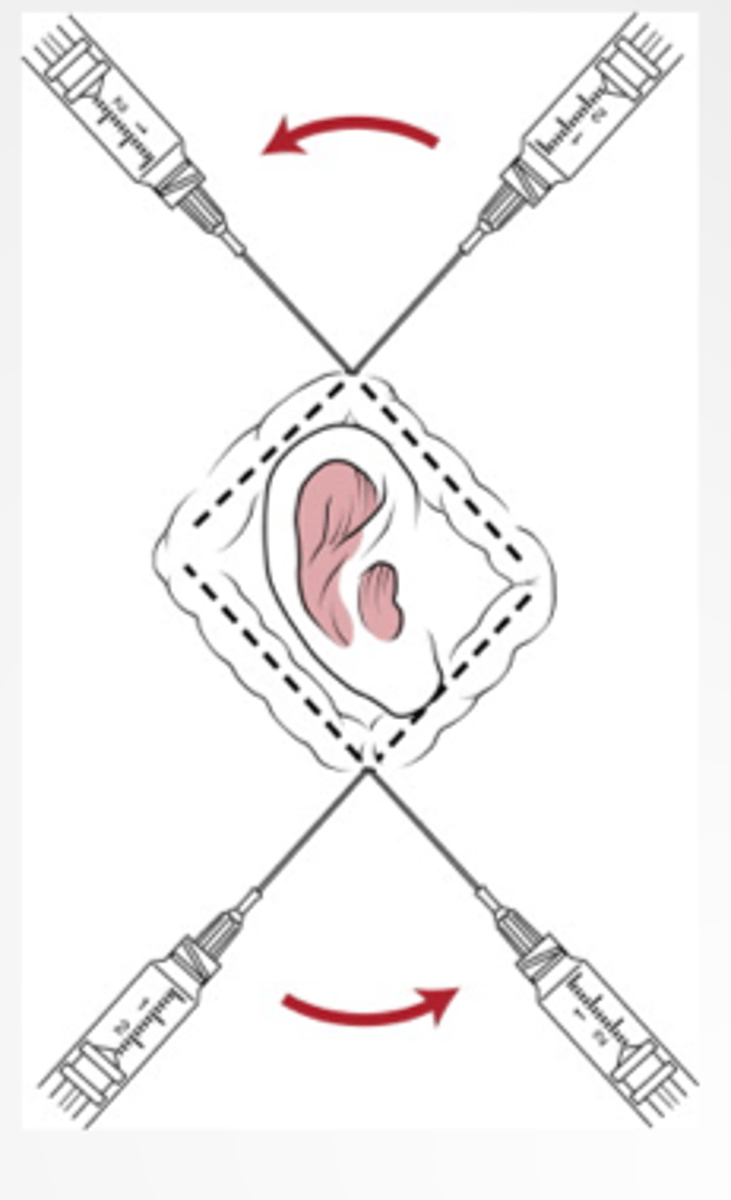
A grossly contaminated and large wound needs anesthesia prior to suturing. What is the preferred method for anesthesia?
Field block injection
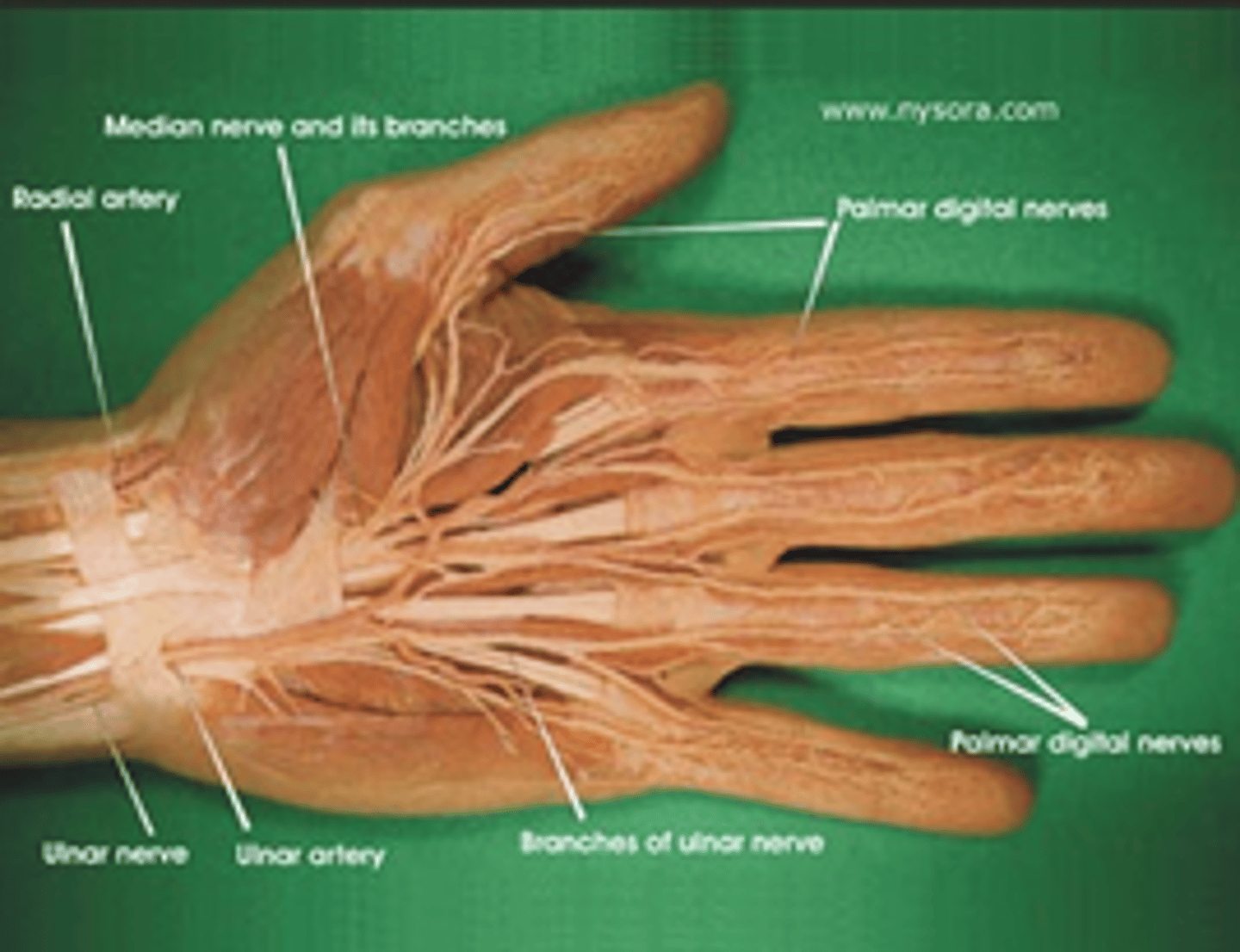
what are some clinical indications to perform a Digital (regional) block ?
- lacerations of fingers/toes
- drainage fo Paronychia
- Nail removal/repair
- reduction of Fractures or Dislocated fingers/toes
What should always be done before a Digital (regional) Block is performed?
Neurovascular status:
- Assessment of distal cap refill
- 2 point discrimination on volar pad
A patient has suffered a finger dislocation and needs reduction. What should be done for comfort?
1. Assess cap refill & 2 point discrimination on volar pad (prior to block) THEN ->
2. Digital block (regional) anesthesia
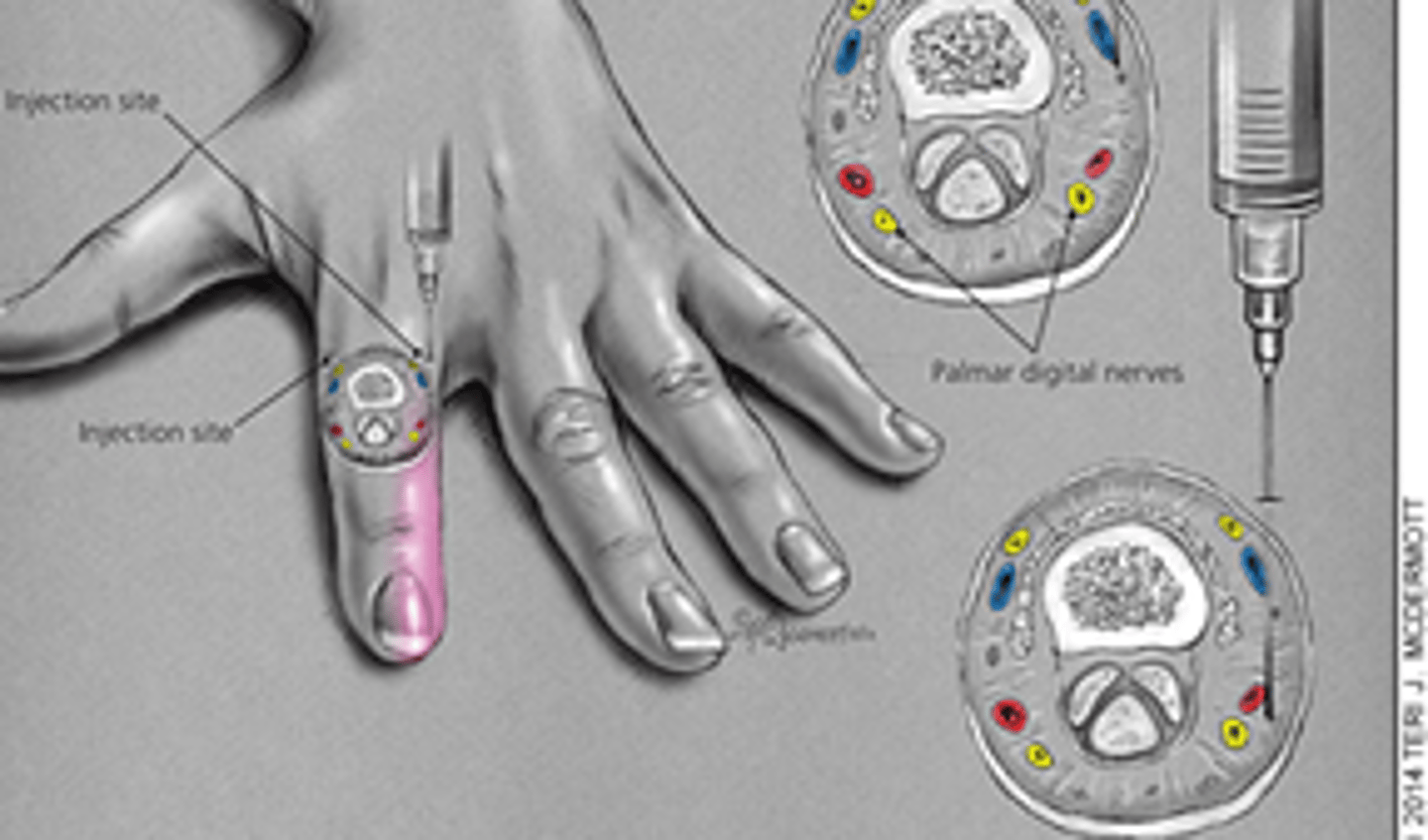
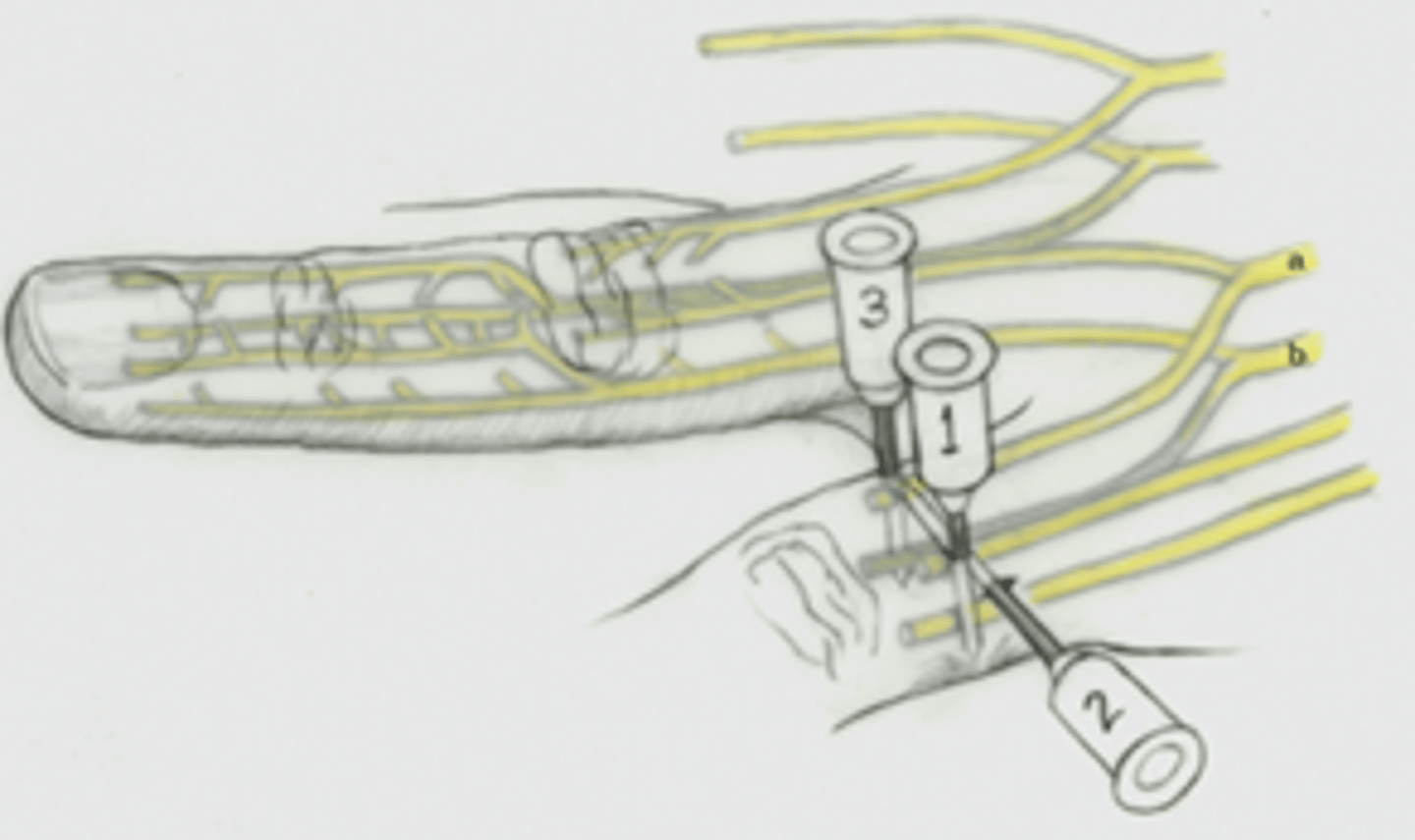
Procedure for Digital (regional) nerve block technique 1:
1) Assess neuromuscular status
2) find web space
3)direct needle toward bone, don't hit it!
4) go all the way to ulnar surface
5) aspirate
6) inject while slowly withdrawing needle
Which digital blocking technique only involves one stick?
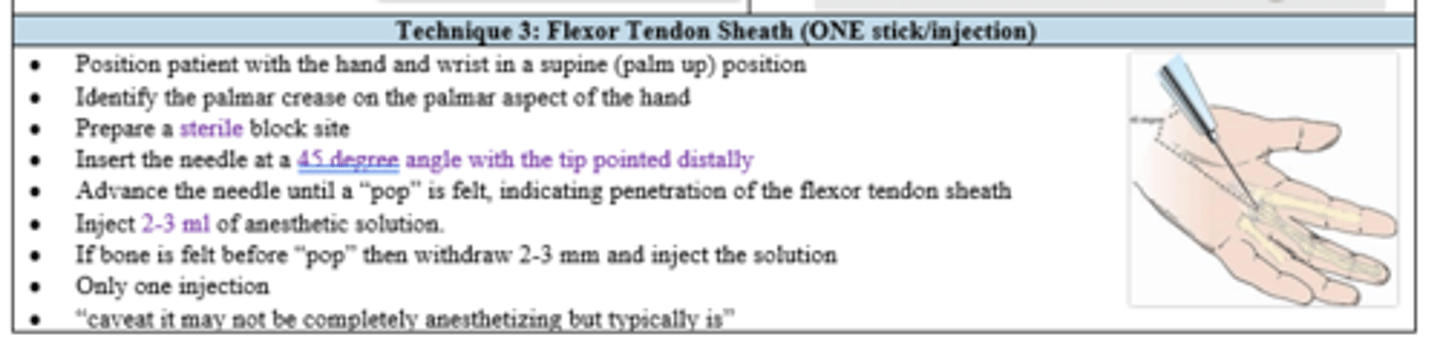
Flexor tendon sheath (technique 3)
- palm up
- identify palmer crease
- inject at 45 deg until "pop"
In a digital nerve block (both technique 1 & 2), where is the needle inserted in relation to the webspace?
Distal to webspace
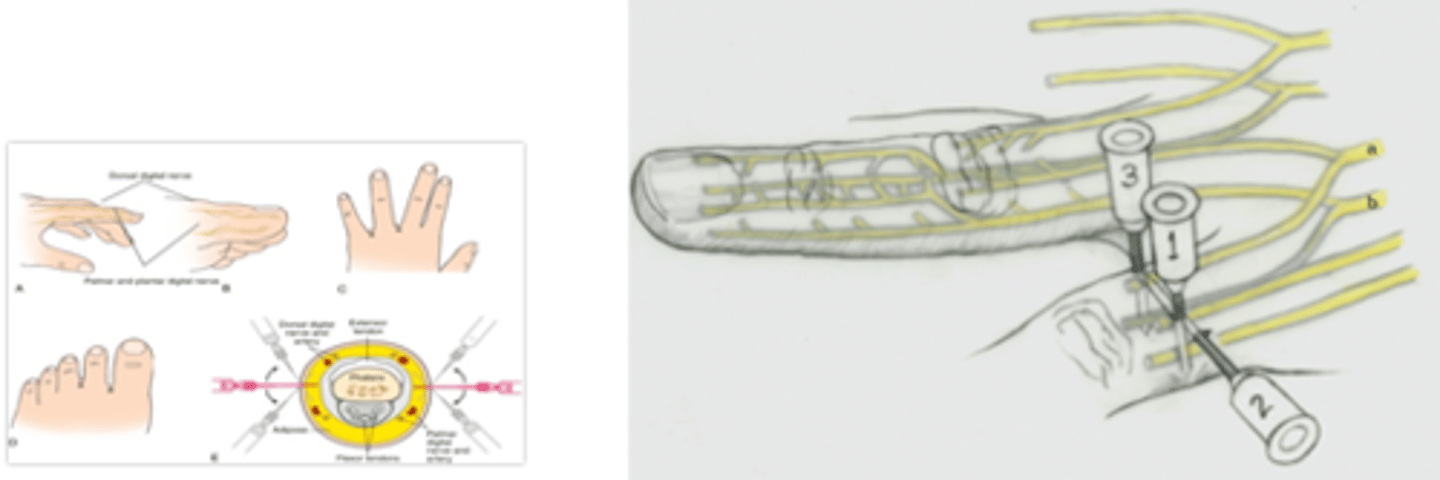
What is different about the 2nd technique for digital nerve blocks (vs. 1 and 3)?
Direct needle across dorsum of digit
- typically only done for thumb or great toe
What is the advantage and disadvantage of Flexor Tendon Sheath approach (technique 3) vs Digital nerve blocks (techniques 1 & 2)?
Pro: one stick
Con: does not always completely anesthetize
As you were performing a Flexor Tendon Sheath digital nerve block, the bone is felt before the "pop". How do you proceed?
Withdraw 2-3mm and inject
During flexor tendon sheath nerve digital nerve block, needle should be positioned at a ____ degree angle
45

With correct technique, what is the onset of action for Lidocaine in direct infiltration?
immediate
What is the onset of action of Lidocaine in nerve blocks?
5-10 minutes
After LA admin, patient develops LA toxicity d/t some underlying condition causing delayed clearance. What s/sx might they be showing?
- Hypotension
- Bradycardia
- CNS depression/stimulation: Seizures
what can be added to reduce pain of infiltration upon an injection of an LAs (acidic) into tissue (basic) ?
Bicarbonate buffer
(T/F) Nerve Digital Field blocks create larger areas of anesthesia and do not cause tissue distortion
True
Always check and document the (neurovascular /cardio/ respiratory) status before admin of LA, especially Facial nerve blocks and Digital block LA?
Neurovascular
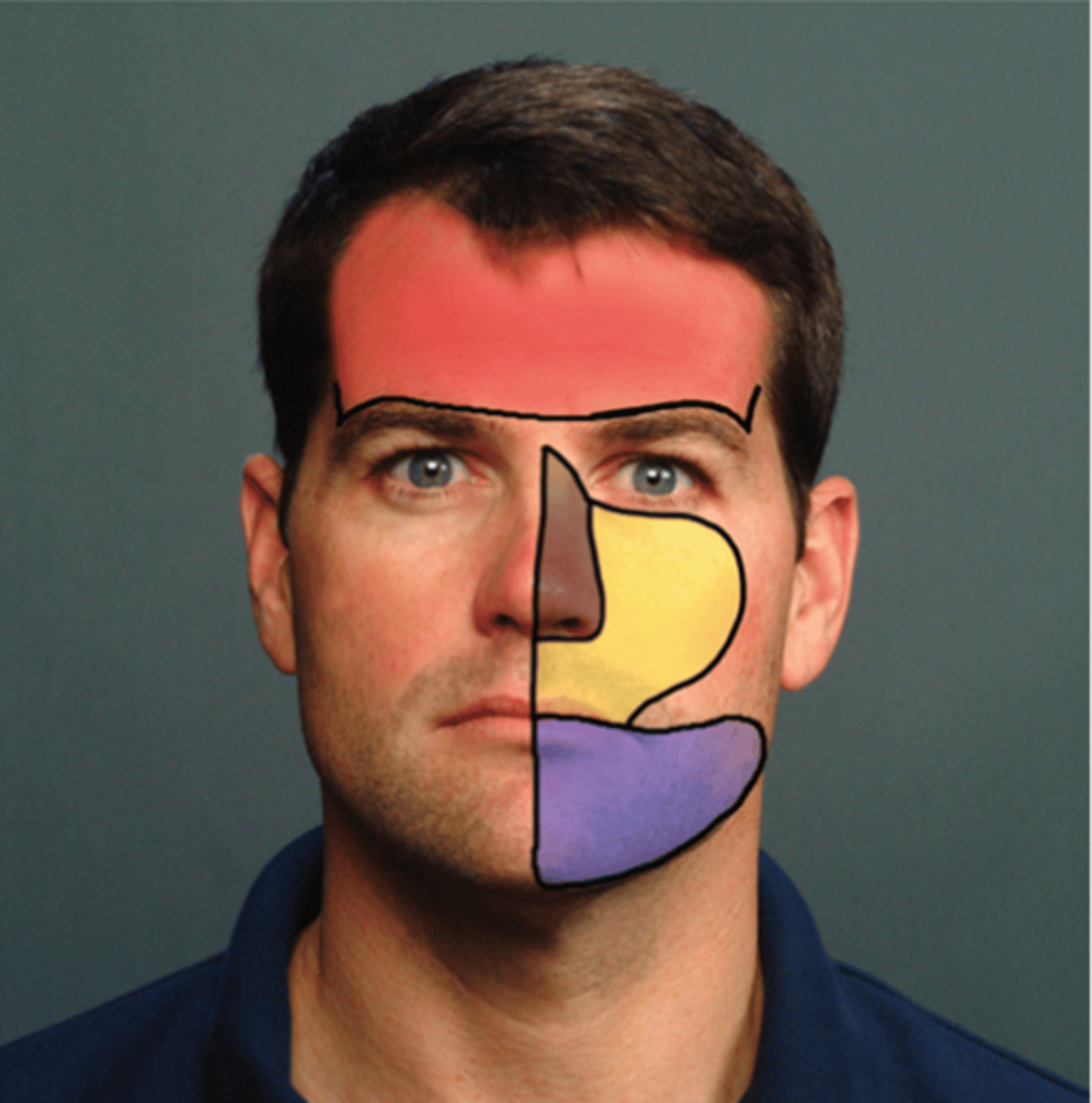
What Facial Nerve blocks and their associated landmarks:
- Supraorbital block: superior to eyebrow/ inline with pupil
- Infraorbital block: below eye/ maxillary canine or 2nd bicuspid teeth
- Mental block: lower lip adjacent to incisors and canines