Looks like no one added any tags here yet for you.
subjective and objective data: migraine with aura, migraine without aura, chronic migraine.
migraine with aura: migraine associated with visual symptoms (flashing lights and lines)
Migraine without aura: throbbing headache lasting 4-72 hours with at least 5 attacks in a lifetime
At least 2 of 4:
Unilateral location
Pulsating or throbbing quality
Moderate to severe intensity
Aggravation by/causing avoidance of routine physical activity
At least 1 of the following:
Nausea or vomiting
Photophobia
Phonophobia
Chronic migraine: >15 times per month
Triggers for migraines
Stress,
sleep deprivation,
hypoglycemia/fasting,
menses,
1st trimester pregnancy,
bright lights,
diet (cheese/cured meats, chocolate, MSG),
drugs (vasodilators (nitroglycerin, nifedipine),
OCs, alcohol, cocaine, analgesic overuse)
Goals of preventing & treating migraine
Treat headache pain quickly and prevent recurrence
Treat associated symptoms (N/V, photophobia)
Restore functional ability
Minimize use of rescue medications and avoid rebound headaches
Reduce migraine frequency, severity, and disability
Improve responsiveness of acute therapies
Improve functioning and quality of life
Prevent headache
Avoid escalation of headache medication use
Reduce headache-related distress and psychological symptoms
Treatment variables
severity
prior treatments
Women of childbearing age (teratogenic potential)
presence of nausea (affects ROA)
likely presence of depression
ROA
ADEs
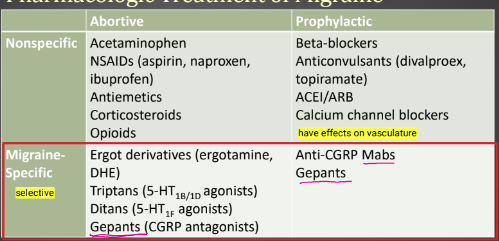
Abortive and prophylactic treatment modalities
Migraine abortive: triptans (triptans), ergot derivatives (DHE, ergotamine), OTC (APAP, naproxen), combinations (excedrin, treximet, cafergot), CGRP antagonist (ubrogepant), 5-HTf1 antagonist (lasmiditan)
Migraine prophylaxis: divalproex, topiramate, propranolol LA, amitriptyline, CGRP antagonists (erenumab, fremanezumab, galcanezumab)
Antinausea: ondansetron, prochlorperazine
Benefits and drawbacks for abortive pharmacologic (NSAIDs, Excedrin, triptans, gepants, lasmiditan, ergots) and prophylactic pharmacologic (BBs, divalproex, topiramate, Anti-CGRPs) treatments
Abortive: taken within 30 min or onset of aura phase
Prophylactic: consider only if 4 or more attacks per month, CIs, failure of therapy, or overuse of acute therapy.
Drug | Benefits | Drawbacks |
NSAIDs | OTC availability | Less effective for moderate to severe migraine |
Excedrin (APAP, caffeine, aspirin) | Proven efficacy in mild to moderate migraine | Less effective for moderate to severe migraine |
Triptans (5-HT1B agonists) | Migraine-specific, effective for aura and nausea | Ischemic cardiovascular effects (stroke risk) |
Gepants (CGRP antagonists) | Migraine specific, safe in CV disease | -- |
Lasmiditan (5-HT1F agonist) | Migraine-specific, safe in CV disease | Serotonin syndrome, sedation (C-V) |
Ergots | May be effective in resistant cases | Significant vascular and GI effects |
give 8wks to assess effectiveness
consider premenstrual prophylaxis (LA NSAID or triptan x 4-5 days during perimenstrual period
Drug | Benefits | Drawbacks |
Beta-blockers (propranolol) | DOC for post-MI and angina | Mild fatigue, CI in asthma, DM |
Divalproex | Effective for comorbid epilepsy and bipolar. Low dose for migraine | CI in pregnancy, potential hepatic toxicity |
Topiramate | Effective for comorbid epilepsy. Low doses for migraine. | Cognitive AEs, CNS depression, weight loss |
Anti-CGRP MAbs | Migraine-specific, highly effective | Hypersensitivity, upper respiratory effects, injection site reactions, $$$ |
Subjective and objective data consistent with major depressive disorder
S/sx lasting at least 2 weeks:
depressed mood
loss of pleasure or interest
insomnia or hypersomnia (frequently)
agitation or retardation (frequently)
fatigue/loss of energy (frequently)
significant weight loss
worthlessness or guilt
diminished concentration, indecisiveness
recurrent thoughts of death or recurrent suicidal ideation/attempt
Can be attributed to:
hormonal factors,
altered NT activity,
stress,
genetics,
comorbid condition (endocrine disorder, anemia, infection, lupus, SUD, anxiety, metabolic disorder, CVD, neurologic disease, malignant disease),
drug therapies (antihypertensives, OCs, steroids, etc)
Objective: PHQ-2/PHQ-9, suicide screening questions
Patient- and agent-related variables that impact the selection of antidepressant drug therapy.
Indication (psychiatric or medical comorbidity)
• Previous response or familial response
• Type of depression/severity of symptoms
• Pt. preference
• Financial considerations (brand vs. generic)
• Chronicity
• Side effect profile
• SI/risk of overdose
• Concurrent medical problems
• Potential drug interactions
• Adherence: Start low and go slow as side effects permit, Elderly pts.: 1⁄2 the usual adult dose
• Underlying anxiety disorder or suspected bipolar disorder: lower doses, ↓ initial anxiety and detect signs of switching
Therapeutic objectives for MDD
Minimize depressive symptoms (sad, anhedonia, feelings of helplessness, suicidal thoughts, diminished concentration, weight loss)
Reduce the depth and length of depression
Prevent suicide
Minimize disrupting effects on work
Induce remission of depression and achieve euthymia
Prevent recurrence
Time of onset of antidepressant effects & management
7-10 days: improved sleep and anxiety
7-21 days: improves self-care, thinking/concentration, energy lvl
2-6 weeks: improved mood, reduced suicidal ideation
Maintenance:
increase dose or use adjunct for partial responders (antipsychotics, lithium, buspirone)
Continue treatment for up to 1 year after remission is achieved
Maintenance treatment for patients with a history of recurrence (1-3 years or lifetime)
Migraine with comorbid depression (MID) therapeutic options: benefits and drawbacks
Drug/Drug Class | Benefits | Drawbacks |
TCAs | Dual transmitter | Toxicity in overdose, anticholinergic |
MAOIs | Option for treatment- resistant cases | Food and drug interactions |
SSRIs | Well-tolerated, evidence for efficacy for MID | Some CYP interactions (sertraline 3A4inh), bleeding risk, sexual dysfunction,
|
SNRI | Dual transmitter, evidence for efficacy for MID | BP elevation
|
Bupropion | Activating, effective for smoking cessation | Seizure risk, CI bulimia/anorexia, MAOI or another bupropion product use |
Mirtazapine | Helpful for insomnia and poor appetite | Metabolic syndrome |
fill in the blank:
Sumatriptan | |
Rizatriptan | |
Propranolol LA | |
Divalproex | |
Topiramate | |
Amitriptyline | |
Sertraline | |
Escitalopram | |
Venlafaxine extended release | |
Bupropion |
Sumatriptan | 50 to 100 mg as a single dose; Maximum dose: 100 mg/dose; 200 mg per 24 hours |
Rizatriptan | 5 to 10 mg as a single dose; maximum daily dose of 30 mg per 24 hours |
Propranolol LA | 40 to 80 mg/day |
Divalproex | 500 mg mg once daily; up to 1 g/day |
Topiramate | 25 mg once daily increase dose in 25 to 50 mg increments; up to 100-200 mg/day |
Amitriptyline | 10 to 25 mg once daily at bedtime; up to 150 mg/day |
Sertraline | 50 mg once daily |
Escitalopram | 10mg/day, titrate to 20mg/day |
Venlafaxine extended release | 37.5 to 75 mg once daily |
Bupropion | 12hr SR: 100 mg once daily; 24hr XR: 150 once daily; up to 450 mg |