Looks like no one added any tags here yet for you.
Subjective assessment
Definition: Gathering information about the client's feelings, perceptions, and experiences regarding their condition or occupation-related issues.
Purpose: Understand the client's perspective, emotions, and goals to tailor interventions effectively.
Example: Asking a client about their pain levels, daily routines, and challenges they face due to their condition.
Objective Assessment:
Definition: Collecting measurable and observable data through tests, measurements, and observations.
Purpose: Obtain quantifiable information about the client's physical abilities and limitations.
Example: Measuring range of motion, strength, or endurance through standardized assessments.
Basic Respiratory Assessment/Treatment:
Assessment: Evaluating a client's respiratory function, identifying any difficulties or abnormalities in breathing.
Treatment: Interventions aimed at improving respiratory function and promoting lung health.
Example: Teaching breathing exercises, postural techniques, and energy conservation strategies.
.SOAP Documentation:
Assessment: Analyzing the information to make clinical judgments about the client's condition and progress.
Recording the client's reported information, such as symptoms, concerns, and goals.
Objective
Documenting measurable data obtained from assessments and observations.
.Assessment:
.Analyzing the information to make clinical judgments about the client's condition and progress.
.Plan
Outlining the interventions, goals, and strategies for the client's ongoing care.
Procedural Reasoning:
.
Definition: Planning and selecting interventions based on knowledge of treatment techniques and their effectiveness.
Example: Choosing specific upper limb exercises to improve fine motor skills in a stroke patient.
Interactive Reasoning:
Definition: Collaborating with the client to understand their needs, preferences, and goals.
Example: Discussing with a stroke patient their desired level of independence in activities of daily living (ADLs) post-discharge.
Conditional Reasoning:
Definition: Considering how contextual factors and environment influence a client's performance and participation.
Example: Evaluating the stroke patient's home environment to recommend modifications that enhance safety and accessibility.
.Pragmatic Reasoning:
Definition: Integrating practical aspects such as reimbursement, resources, and time constraints into decision-making.
Example: Selecting assistive devices for the stroke patient based on insurance coverage and availability.
Narrative Reasoning:
Definition: Understanding the client's story, values, and life experiences to guide intervention planning.
Example: Learning about a stroke patient's hobbies and interests to incorporate meaningful activities into their therapy plan.
Diagnostic Reasoning:
Definition: Analyzing assessment data to identify the client's condition, impairments, and potential barriers.
Example: Identifying muscle weakness and sensory deficits in the stroke patient's affected arm through thorough assessment.
Scientific Reasoning:
Definition: Applying research evidence and scientific principles to support intervention choices.
Example: Using studies to determine the most effective interventions for improving gait in stroke patients.
Ethical Reasoning:
Definition: Considering ethical dilemmas and making decisions that respect the client's autonomy, confidentiality, and well-being.
Example: Balancing the stroke patient's right to make decisions about their treatment with safety concerns.
Conditional Reasoning:
Definition: Forecasting the potential outcomes of different interventions and making decisions based on likely results.
Example: Predicting how a stroke patient's balance and mobility may improve with intensive therapy versus a slower-paced approach.
SWOT analysis
.Strengths (S):
Clinical knowledge gained during studies.
Strong communication skills for patient interactions.
Ability to adapt to fast-paced acute care environment.
Experience in using various assessment tools.
Weaknesses (W):
Limited experience in acute stroke settings.
Less exposure to complex stroke cases.
May need more familiarity with specific hospital protocols.
Opportunities (O):
Learning from experienced therapists in the acute stroke unit.
Exposure to diverse stroke cases for skill enhancement.
Opportunities to observe and participate in interdisciplinary teamwork.
Threats (T):
High-pressure environment may impact decision-making.
Limited time for in-depth assessment and intervention.
Possibility of encountering emotionally challenging situations.
Understanding Hemiplegia in Acute Stroke: ( Steps to follow)
Hemiplegia: paralysis on one side from stroke damage.
Rapid intervention by OTs to minimize deficits.
Assessment in Acute Stroke: (Steps to follow)
Quick assessment of motor, sensory, cognitive issues.
Collaborate with medical team for brain damage insight.
Prioritize safety and basic self-care needs.
Early Mobilization and Functional Training: (Steps to follow)
Passive/active exercises for range of motion.
Prevent contractures with bed mobility techniques.
Focus on sitting, bed transfers in acute care.
4. Task-Specific Training: (Steps to follow)
Replicate vital daily tasks for independence.
Grasping, reaching, self-feeding for motor skills.
Problem-solving tasks to address cognition.
..5 Adaptive Equipment and Aids: (Steps to follow)
Temporary tools for self-care facilitation.
Modified utensils, grooming aids, dressing tools.
Train patients for effective tool use.
..6 Psychosocial Support and Coping: (Steps to follow)
Address emotional challenges post-stroke.
Therapeutic communication for anxiety, depression.
Stress management, social interaction promotion.
.7 Involving Caregivers: (Steps to follow)
Educate on care, safety, mobility assistance.
Balance support with encouraging independence.
Prepare caregivers for post-discharge roles.
.8. Preparation for Discharge and Transition:
Plan for rehab/home transition with team.
Recommend post-discharge adaptive equipment.
Share community resources, support groups.
.9. Documentation and Progress Tracking:
.
Document baseline, functional goals.
Update progress, intervention response.
Use objective measures for improvement.
.10. Interdisciplinary Collaboration:
Collaborate with physio, speech therapists.
Unified approach for optimal outcomes.
Comprehensive care plans for acute stroke.
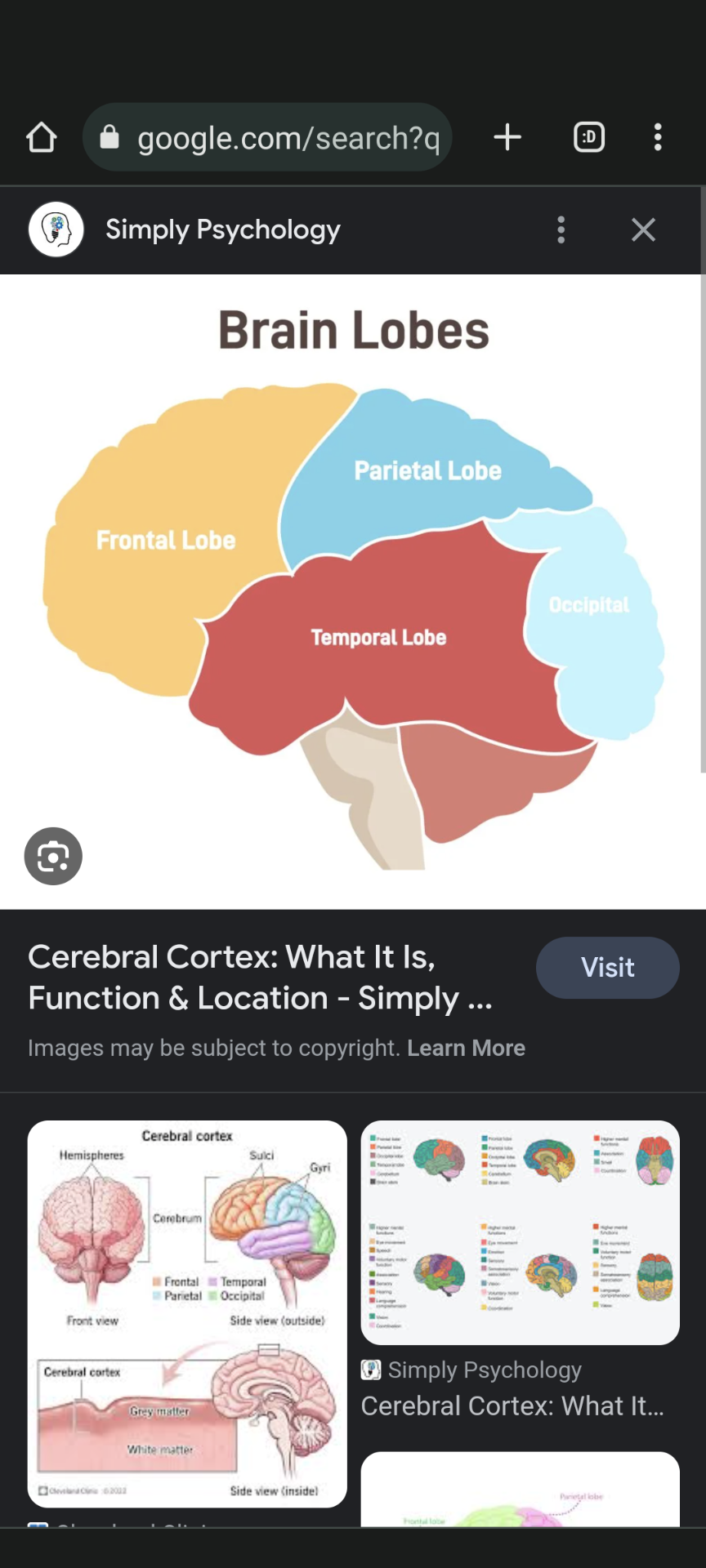
Term: Cerebral Cortex
Description: Divided into frontal, parietal, temporal, and occipital lobes.
Functions: Decision-making, sensory processing, memory, visual processing.
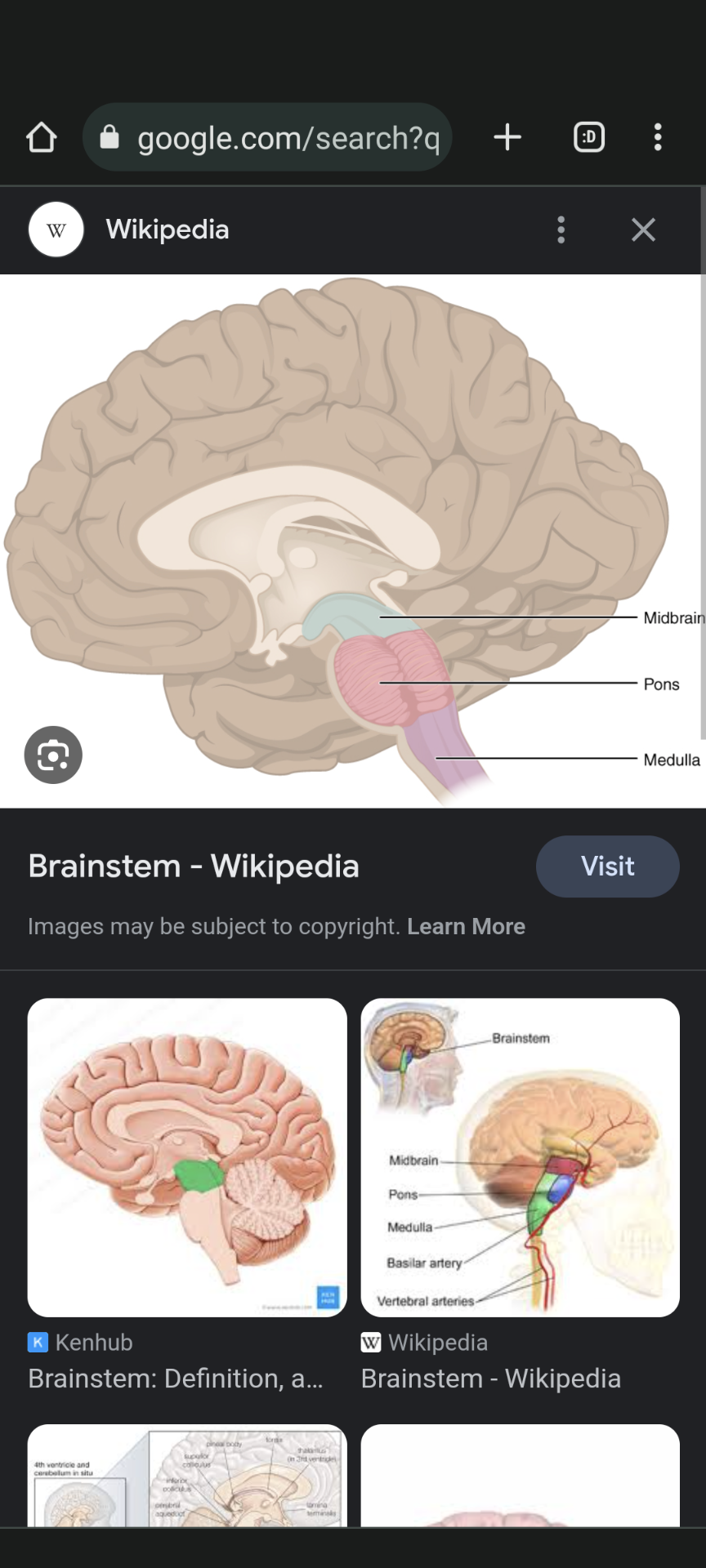
Term: Brainstem
Description: Connects brain to spinal cord, controls breathing, heart rate, consciousness.
Components: Midbrain, pons, medulla oblongata.
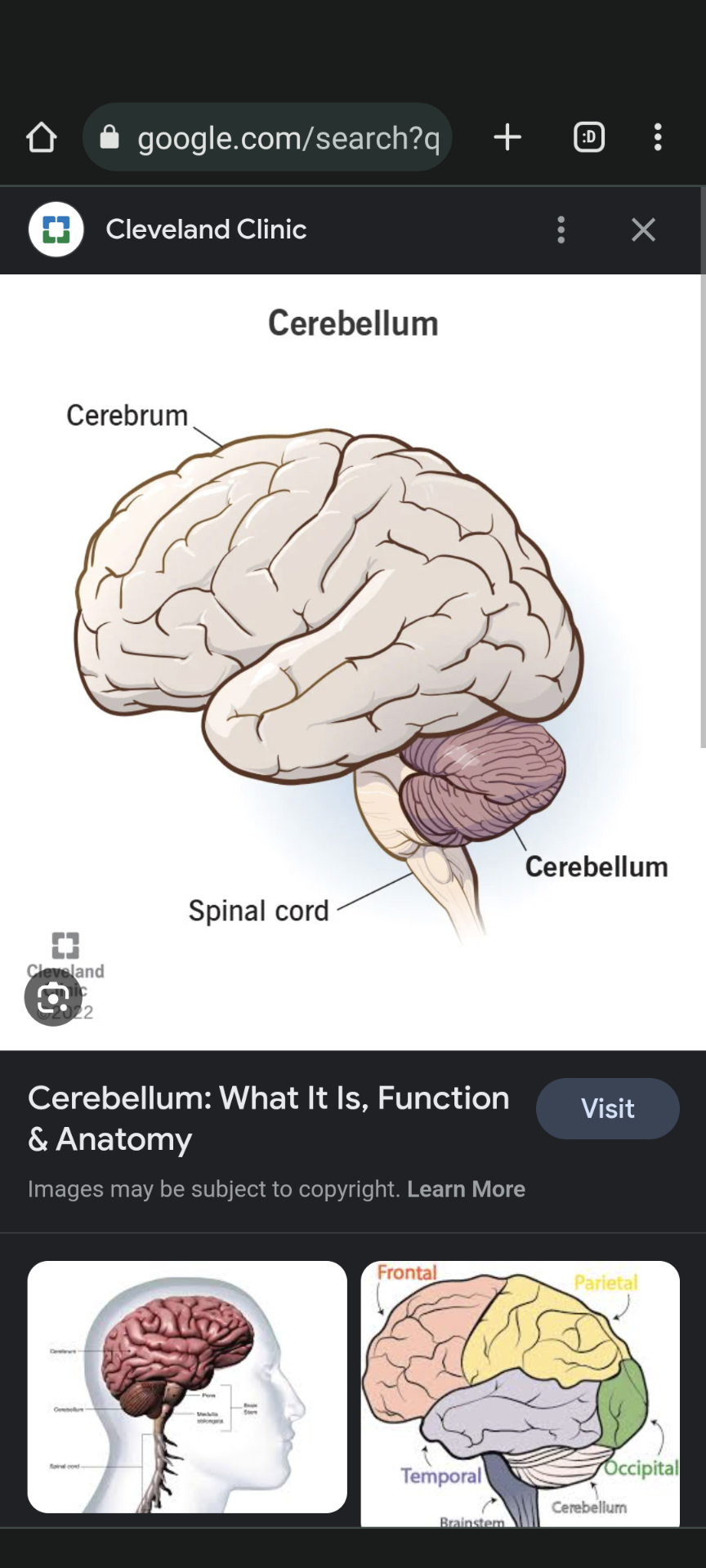
Term: Cerebellum
Description: Located at back of brain, coordinates movement, balance, posture.
Functions: Motor learning, cognitive functions.
Left Hemisphere Back of card
Description: Controls right side of body.
Functions: Language processing, speech production, logical reasoning.
Areas: Wernicke's (comprehension), Broca's (production).
Right Hemisphere
Description: Controls left side of body.
Functions: Spatial perception, emotions, creativity.
Abilities: Nonverbal cues, metaphorical language.
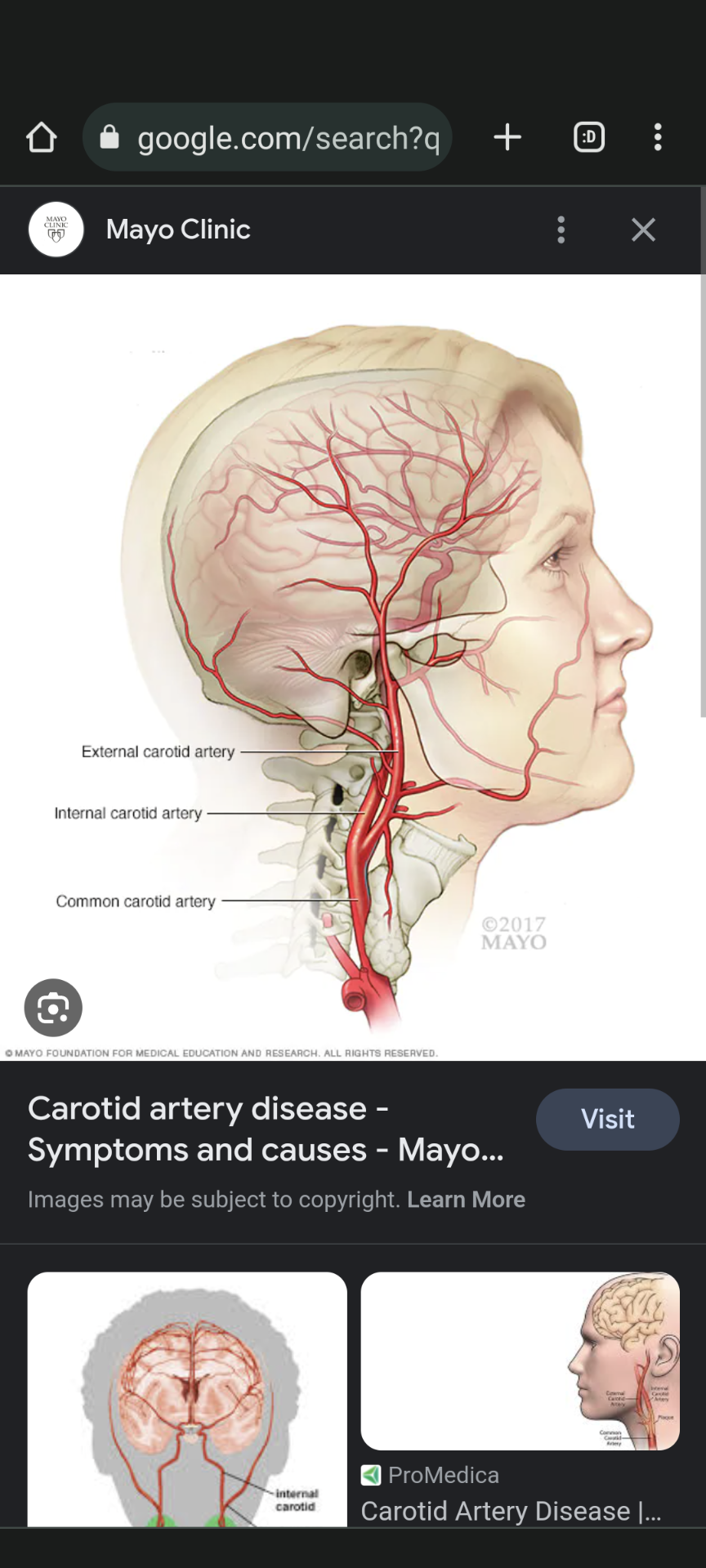
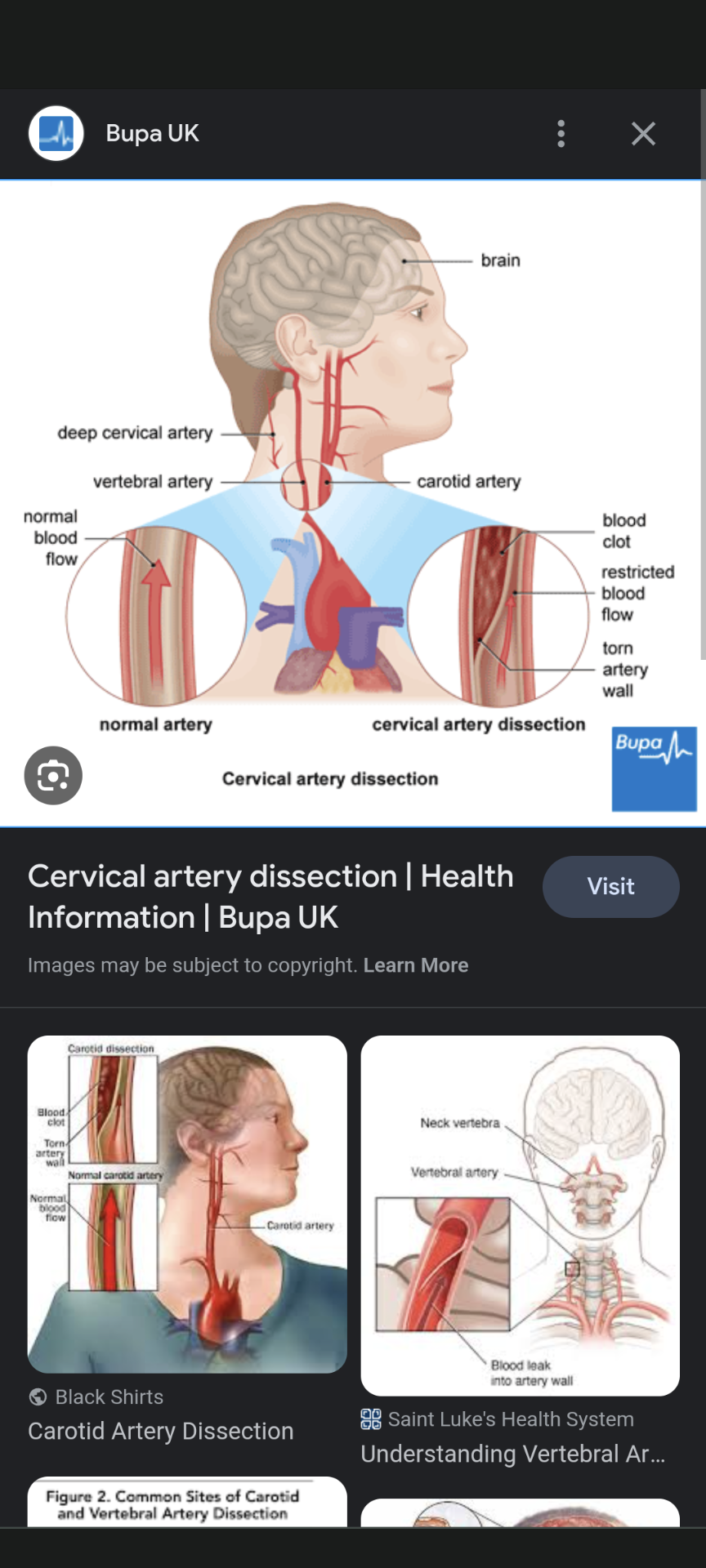
Carotid Arteries Back of card
Description: Supply blood to face, neck, and brain.
Types: External (face, neck), Internal (brain).
.Term: Vertebral Arteries
Description: Form basilar artery, supply brainstem, cerebellum.
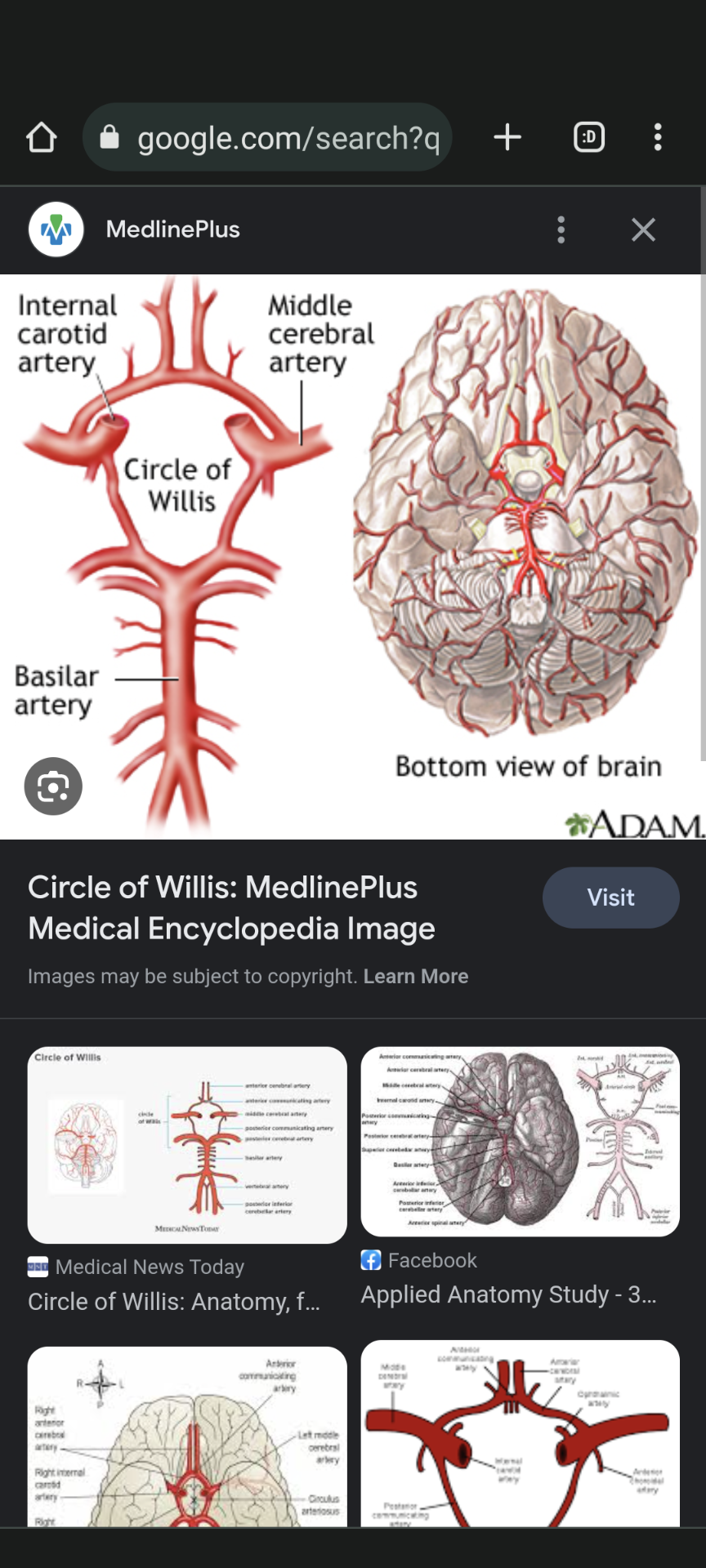
Circle of Willis
Description: Arterial network at base of brain.
Role: Provides collateral circulation, prevents severe ischemia
Term: Ischemic Stroke
Description: Clot blocks blood vessel, causes infarction.
Consequences: Tissue death, neurological deficits.
Term: Hemorrhagic Stroke
Description: Caused by brain bleeding.
Types: Intracerebral (within brain), Subarachnoid (between brain layers).
.Neuroanatomy in Strokes
Importance: Predict deficits, plan rehab for specific impairments.
Knowledge: Identify functional consequences, design targeted interventions.
Occupational Therapy Frame of Reference for Acute Stroke: Neurodevelopmental Treatment (NDT) Approach
Focus: Enhance optimal movement patterns, function, and quality of life.
Application in Acute Stroke:
Motor Control: Address movement impairments, coordination, muscle tone.
Task-Specific Training: Mobilize early, practice functional tasks for recovery.
Handling Techniques: Hands-on guidance for safe movement, positioning.
Environment: Consider impact of surroundings on mobility.
Collaboration: Multidisciplinary teamwork for holistic care.
Holistic Approach: Address physical, cognitive, emotional aspects.
Individualized Care: Tailor interventions to unique needs and goals.
Goal-Oriented: Set functional goals, immediate ADLs and mobility
.Communication Challenges:
Aphasia:
.
Expressive Aphasia: Trouble expressing thoughts.
Receptive Aphasia: Difficulty understanding language.
Strategies: Boards, gestures, simple sentences.
communication challenges: Apraxia
Motor speech disorder affecting coordination.
Trouble planning and executing speech sounds.
Techniques: Therapy, slower speech.
.Fall Prevention:
Balance Exercises:
Tai Chi, heel-to-toe walking, one-leg stands.
Strengthen muscles, improve balance.
Fall prevention:
Home Modifications:
Remove clutter, secure rugs, bright lighting.
Grab bars, railings for safety.
.Fall prevention
Assistive Devices:
.
Canes: Walking stability.
Walkers: More support, some with wheels.
Orthotics: Correct foot drop.
.Cognitive Impairment
,
Cognitive Rehabilitation:
Memory exercises, problem-solving tasks.
Boost memory, mental agility.
Structured Routines:
Set schedules, use visual cues.
Enhance memory through routine.
Bathing
Grab Bars: Provide stability.
Shower Chair: Prevent falls.
Handheld Showerhead: Easy reach.
Dressing
Velcro Closures: Simplify fastening.
Dressing Stick: Manage buttons.
Zipper Pulls: Independent dressing.
.Toileting:
Raised Toilet Seat: Easier sitting/standing.
Commode Chair: Alternative option.
Handrails: Enhance stability
.Grooming:
Adaptive Handles: Brushes, combs, toothbrushes.
Electric Toothbrush/Razor: Simplify tasks.
Handheld Mirror: Assist with reach.
.Feeding:
Non-Slip Placemats: Prevent spills.
Adaptive Utensils: Larger grips.
Cups with Lids/Straws: Safety in eating/drinking.
Ischemic Stroke:
Caused by a clot blocking blood flow.
Hemorrhagic Stroke:
Result of bleeding in the brain.
.3. FAST Assessment:
"Face": Look for one-sided drooping.
"Arms": Weakness in one arm.
"Speech": Slurred or inappropriate speech.
"Time": Treatment urgency based on symptom onset.
.Thrombolytic Therapy:
tPA: Clot-dissolving drug, time-sensitive use.
Risk: Bleeding concern, especially for hemorrhagic strokes.
.. Rehabilitation Principles:
Acute: Monitor vitals, prevent complications.
Subacute: PT (motor skills) & OT (daily tasks).
Chronic: Reintegration, address residual deficits.
.7. Assessment Tools:
NIH Stroke Scale: Measures impairment severity.
Barthel Index: Rates independence in activities.
NIH Stroke Scale:
Measures impairment severity.
.Barthel Index:
Rates independence in activities.
.8. Dysphagia Management:
Risk: Aspiration pneumonia.
Speech therapy, modified diets.
.11. Psychosocial Support:
- Depression risk, counseling referral. - Family involvement, support groups.
.15. Family Education:
- Monitor condition, manage meds. - Participate in therapy, home practice.
.19. Patient Safety:
- Pressure ulcer prevention, repositioning. - Deep breathing exercises for lungs.
20. Discharge Planning:
- Home modifications, smooth transition. - Clear instructions, follow-ups, caregiver training.
Advocating Mode:
Definition: Ensuring clients have necessary resources for participation in occupations.
Acute Stroke Example: Assisting stroke patients in obtaining adaptive equipment for safe mobility and self-care.
.. Collaborating Mode:
Definition: Facilitating autonomy and clients' ownership of the therapy process.
Acute Stroke Example: Collaborating with stroke survivors to set functional goals and plan therapy activities based on their preferences.
.3. Empathizing Mode:
Definition: Understanding and validating clients' lived experiences.
Acute Stroke Example: Expressing empathy towards stroke patients' frustrations with mobility limitations and assisting them in coping with emotional challenges.
.4. Encouraging Mode:
Definition: Fostering hope and willingness to engage in therapy.
Acute Stroke Example: Providing positive reinforcement as stroke patients make progress in regaining motor skills and self-care abilities.
.5. Instructing Mode:
Definition: Offering clear expectations and explanations about the therapy process.
Acute Stroke Example: Explaining the purpose and benefits of therapeutic exercises to stroke patients and their families.
.6. Problem-Solving Mode:
Definition: Using reasoning and strategic questions to identify solutions.
Acute Stroke Example: Collaboratively strategizing with stroke patients to overcome challenges in performing activities of daily living and suggesting adaptive techniques.
.Hypertension Management:
Definition: High blood pressure that can impact vascular health and increase stroke risk.
Relevance in Acute Stroke OT:
Monitor blood pressure during therapy sessions.
Adapt activities to prevent blood pressure spikes.
Educate patients on lifestyle modifications for hypertension control.
.Diabetes Management:
Definition: Chronic condition affecting blood sugar levels and vascular health.
Relevance in Acute Stroke OT:
Monitor blood sugar levels during therapy.
Consider glucose levels when planning activities.
Collaborate with diabetes care team for comprehensive care.
.Lifestyle Modifications:
Hypertension:
Encourage low-sodium diet, balanced nutrition.
Promote regular physical activity.
Discuss stress reduction techniques.
Lifestyle modifications: Diabetes
Educate on balanced carbohydrate intake.
Encourage consistent physical activity.
Highlight importance of blood sugar monitoring.
.Medication Management: Hypertension
Understand antihypertensive medications.
Coordinate therapy sessions around medication schedules.
medication management: .
Diabetes:
Familiarize with diabetes medications (oral/insulin).
Monitor blood sugar before and after therapy.
.Preventing Complications:
Hypertension:
Address risk factors for cardiovascular events.
Modify activities to prevent blood pressure spikes.
Preventing complications: Diabetes
Prevent hypo-/hyperglycemia during therapy.
Encourage foot care to prevent complications.
.Interdisciplinary Collaboration:
Hypertension:
Hypertension:
Communicate with medical team about blood pressure readings.
Align therapy with medical recommendations.
Diabetes:
Coordinate with diabetes care team.
Ensure therapy complements diabetes management.
.Functional Implications:
Motor Impairments:
Weakness, paralysis on one side (hemiplegia).
Challenges in fine and gross motor movements.
Functional implications: Cognitive Impairments:
Memory deficits, impaired attention, problem-solving difficulties.
Impact on participation in daily tasks.
.Sensory Changes:
Loss of Sensation:
Decreased sensation on affected side (hemianesthesia).
Impaired body awareness.
Perceptual Deficits:
Visual, spatial, and proprioceptive issues.
Difficulty with depth perception and spatial relationships.
sensory chnages
Loss of Sensation:
Decreased sensation on affected side (hemianesthesia).
Impaired body awareness.
Perceptual Deficits:
Visual, spatial, and proprioceptive issues.
Difficulty with depth perception and spatial relationships.
.Dysarthria:
Speech difficulties due to muscle weakness.
Occupational Therapy Management:
Task-Specific Training:
Focus on functional activities for independence.
Grading activities to match patient's abilities.
Occupational Therapy management 2
.
Constraint-Induced Movement Therapy:
Encourage use of affected side by constraining unaffected side.
Enhance motor recovery.
.Assessment and Diagnosis: (RCP)
Early Identification: Rapidly identify stroke symptoms.
Imaging: Utilize brain imaging for accurate diagnosis.
Stroke Scales: Use standardized scales for severity assessment.
Acute care management (RCP)
Thrombolysis: Administer clot-dissolving treatment as appropriate.
Multidisciplinary Team: Collaborate for comprehensive care.
Brain Imaging: Monitor changes and tailor interventions.
Secondary Prevention: RCP
.
Risk Factor Management: Address hypertension, diabetes, etc.
Antiplatelet Therapy: Prescribe antiplatelet medications.
Lifestyle Changes: Promote healthy behaviors.
.Rehabilitation and Recovery:
Early Mobilization: Initiate gentle movement and therapy.
Functional Goals: Set individualized functional targets.
Patient-Centered: Focus on patient's needs, preferences.
CPR
Purpose: Emergency life-saving technique for cardiac arrest.
Steps: Check responsiveness, call for help, start compressions and rescue breaths.
Compression Rate: 100-120 compressions per minute.
Depth: 2-2.4 inches for adults; 2 inches for children; 1.5 inches for infants.
Compression-to-Breath Ratio: 30 compressions followed by 2 rescue breaths.
.Automated External Defibrillator (AED):
Purpose: Restore normal heart rhythm in cardiac arrest.
Use: Attach pads, follow AED prompts, ensure safety.
Follow-Up: Continue CPR after AED shock for 2 minutes.
.Choking:
Conscious Adult/Child: Perform abdominal thrusts (Heimlich maneuver).
Unconscious Adult/Child: Combine CPR with chest thrusts.
Infant: Perform back blows and chest thrusts.
.Using Slings and Hoists:
Assessment: Assess the client's needs and abilities.
Select Appropriate Sling: Choose a sling based on client's condition and transfer type (e.g., standing, sitting).
Position the Sling: Place the sling under the client, ensuring it's properly aligned.
Attach Hoist: Attach the hoist's hooks to the sling's attachment points.
Check Safety: Ensure hooks are secure and sling is well-fitted.
Lift Smoothly: Operate the hoist to lift the client, maintaining stability.
Transfer: Move the client to the desired location smoothly.
Lowering: Gently lower the client, then detach and remove the sling.
.Using Transfer Boards:
Assessment: Evaluate client's mobility and transfer needs.
Prepare Environment: Position the transfer board between surfaces (bed to chair).
Assist Client: Guide the client to the edge of the starting surface.
Position Transfer Board: Place one end of the board under the client's starting point.
Assist Client to Slide: Assist the client to slide across the board.
Monitor Safety: Ensure stability and comfort during the transfer.
Guide Movement: Support client's movement as they slide.
Complete Transfer: Assist the client to the desired position, ensuring safety.
.Using Assistive Devices (e.g., Walking Aids):
Assessment: Assess client's mobility needs and abilities.
Select Appropriate Device: Choose the appropriate walking aid (cane, walker, etc.).
Size and Fit: Adjust the device's height for optimal posture and support.
Educate the Client: Teach proper use and weight-bearing techniques.
Grip and Stance: Instruct the client on holding the device and maintaining balance.
Initiate Movement: Encourage the client to take small, controlled steps.
Observe and Guide: Monitor the client's movement for safety.
Gradual Progression: Assist the client in practicing and improving mobility.