Ch 7 & 8 Organization and A &M text
1/13
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
14 Terms
Primary, Secondary, Tertiary levels of care-examples-which is most costly
Primary
Common health problems that account for 80- 90% visits to providers
ex. immunizations, colds, physicals, ear infections
Secondary
Problems that require more specialized clinical expertise
ex. OB/GYN, ENT, Surgery, Cancer treatment
Tertiary
Rare + complex problems
ex. Organ transplant, congenital malformations
Most costly: Tertiary
Regionalized model-dispersed model- features,
1. Regionalized model
Highly structured
Base is primary care, organization
works upward as neededGeneral physician practitioners (GPs)
practice exclusively at the primary care
levelRelies on resources coordinated in a
geographic region
2. Dispersed model
More fluid model- allows patients to go
where they wish, tertiary expertise
emphasizedPrimary care is spread among
specialists, total supply of generalists
Why dispersed model has grown in the U.S.
Biomedical Model
Flexner report 1906- Medical training was reformed with an
emphasis onAcademically oriented training
Technology and basic science
Specialist training
Financial Incentives
Medicare/Medicaid paid more for procedures
Blue Shield- Reimbursement for procedures- fees remained
high despite the physician time needed for procedures
declined
Hill Burton Hospital Construction Act 1946- hospital expansion
Professionalism
Physicians have been sovereign, American Medical
Association (AMA) has supported physician independence.System has been weighted toward hospital and specialty care
Arguments for and against a dispersed model
For
Pluralism enables providers and facilities
to be more availableAmericans value choice of providers,
access to specialists and technology
Against
It lacks coordination
Quality of care can be maintained with use of fewer
resourcesResearch shows comparable outcomes for patients treated by
General practitioners and Nurse practitioners
It is not consistent with the health needs of the
majority of the population “Common disorders
commonly occur and rare ones rarely occur”e.g. (URI, skin disorders, emotional disorders, preventive care
needs)
Is costly
Research shows that generalists in contrast to specialists
practice a less resource intensive style of medicineCosts are lower for patients treated by generalists vs.
specialists after controlling for severity of illness.
Supply of U.S. generalist physicians- why this is a problem
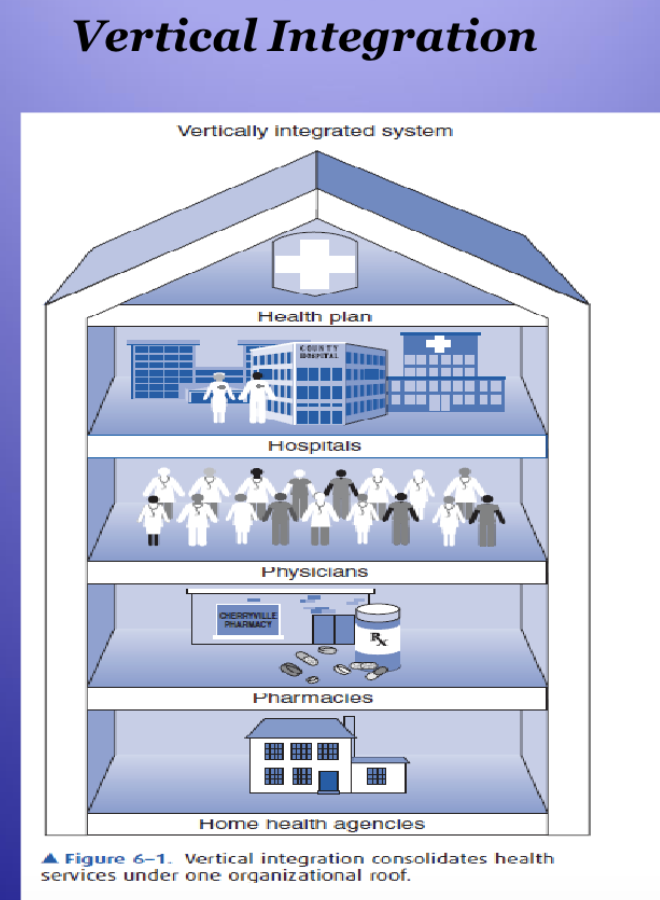
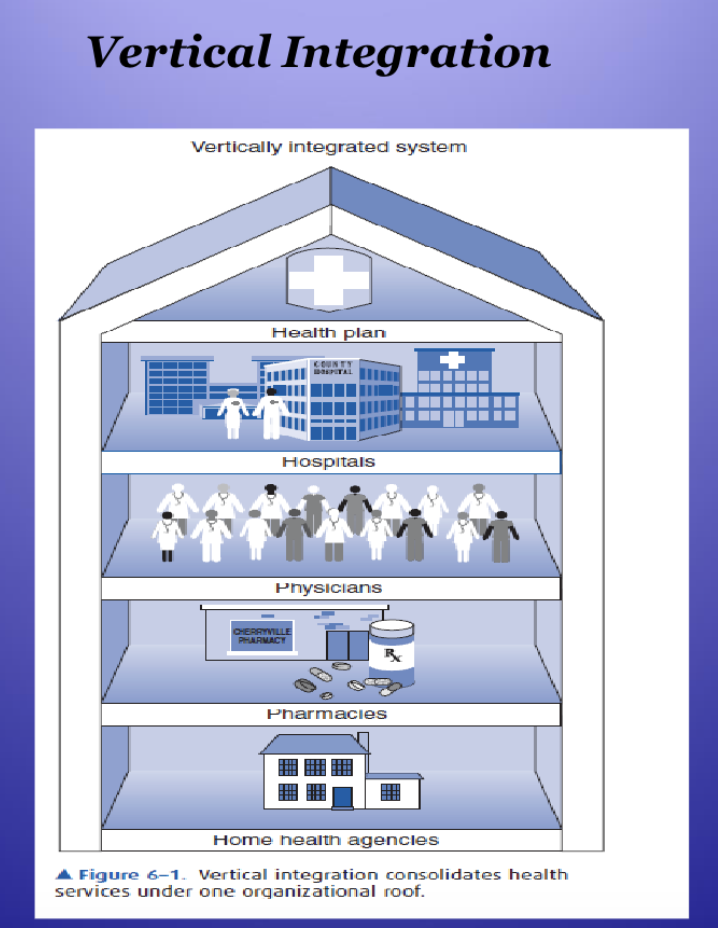
Vertical integration- First generation HMOs- Kaiser
A vertical integration model: consolidates all
levels of care, staff, and facilities under one
organizational ownershipDoes not cover an entire population but
responsible for delivering all services to a
population of enrolleesPhysician group practice provides care to
members under a capitated plan.Enables a more population based model of
health
Virtual integration- Independent Practice Associations (IPAs) and Integrated Medical Groups
Benefits of vertical/benefits of virtual integration
Virtual integration:
Hospitals and insurers recruit office
based fee for service community physicians into an IPA
creating a basis for an HMO and negotiate contracts
with the physicians to provide care.
IPA model:
Allows insurers, etc. to respond to market changes by
renegotiating contract bargains with providersHas the advantage of low capital costs because the HMO
does not have to own buildings
Integrated medical group model:
Physicians do not own their practices but the medical group
organization employs them
(IMGs)- Value of virtual integration, disadvantages
IMG Value/Disadvantages:
Encourages cooperation w/o consolidation
Limited control + potential inconsistency across independent entities
Importance of HMO act 1973
Purpose:
encouraged the development of Health Maintenance Organizations
Importance:
marked a shift towards managed care, cost containment, & preventative focus
Differences between old and new primary care models
Old Model:
solo or small-group practice; fee-for-service payment; limited coordination; reactive care
New Model:
team-based, integrated sys, use of electronic health records, pop health management, + preventive focus
Role hospitalists have in health care
Patient care medical homes
Accountable Care Organizations
Networks of physicians and other providers that are held accountable for the cost and quality of the continuum of care delivered to a group of Medicare patients.
Medical Neighborhoods
Services are functionally integrated similar to traditional HMOs. PCP coordinates care. Patients are informed and involved. Coordinated care contributes to the health of a population.
High performing health care requires excellent medical homes and medical neighborhoods.
Are based on “Patient Centered Medical Homes” where the primary care physician is in charge of care provided by all people and places where care is provided including specialists, pharmacies, hospice, home health, nutritionists, etc.