week 8: more labor and delivery + review
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
Factors Affecting Labor: Passenger
related factors
who is the passenger
fontanels
molding
fetal presentation
cephalic presenting part
breech presenting part
shoulder presenting part
Cephalopelvic disproportion
Passenger: Fetus
Size of the Fetal Head
Bones in the fetal skull
Fontanels: Soft spot on the top of the baby’s head
Molding: the natural, temporary reshaping of a baby's soft skull bones as they overlap to navigate the birth canal during labor
Fetal Presentation: the part of the fetus that enters the pelvic inlet first and leads through the birth canal during labor
Cephalic – presenting part is the occiput (back of the head) (called “vertex”)
Breech – presenting part is the sacrum
Shoulder – presenting part is the scapula
Cephalopelvic disproportion – head is too big to fit through the pelvis OR the pelvis is too small to accommodate the fetal head.
Factors Affecting Labor: Passenger (fetus)
fetal lie
fetal attitude
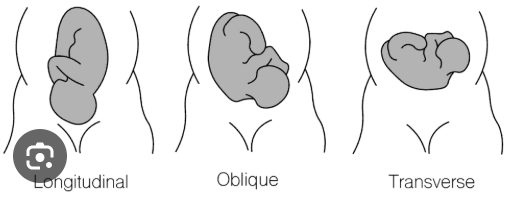
Fetal Lie: the relation of the long axis (spine) of the fetus to the long axis (spine) of the mother
Longitudinal: Ideal position
Transverse
Fetal Attitude: the relation of the fetal body parts to one another
Factors Affecting Labor: Passenger (fetus)
fetal position
position is denoted by
best position
fetal station
engagement
Fetal Position: relationship of a reference point on the
presenting part to the four quadrants of the mother’s
pelvis
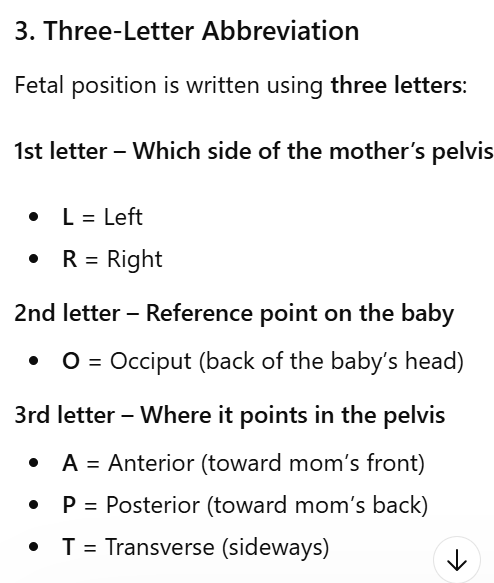
Position is denoted by a three-part letter
abbreviation
best position is LOA
Fetal Station: measure of the degree of descent of the
presenting part of the fetus through the birth canal
Engagement: usually corresponds to 0 station
Factors Affecting Labor: Powers, Position and Psychologic
powers
primary powers vs secondary powers
bearing down
Valsalva maneuver
position
psyche
Powers
• Primary powers: contractions
• Frequency, duration, intensity
• Effacement
• Dilation
• Secondary powers: bearing-down efforts: strong urge to bear down, or 'push', Valsalva maneuver: a breathing technique performed by attempting to exhale forcefully against a closed airway
Position of laboring woman
Psychologic state of laboring woman
Labor
define
signs of preceding labor
onset of labor
Labor: process of moving fetus, placenta, and membranes out of the uterus and through the birth canal
Signs preceding labor
Lightening or dropping
Bloody show
Onset of labor
Many factors involved; Cannot be ascribed to a single cause
mechanisms of labor
define
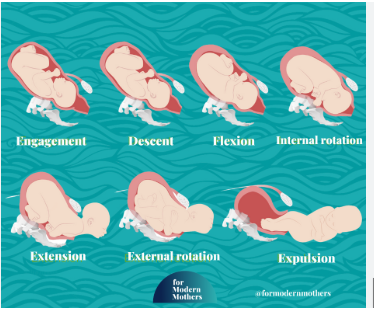
7 Cardinal Movements of Mechanism of Labor (in order)
1. Engagement
2. Descent
3. Flexion
4. Internal rotation
5. Extension
6. External rotation (also called Restitution)
7. Expulsion
Pain During Labor and Birth
pain defined
Neurologic Origins
Expression of pain
Pain: is a highly individualized phenomenon with sensory
and emotional components
Neurologic Origins
Visceral: Pain from internal organs. It is usually dull, aching, or cramping and hard to pinpoint exactly where it is.
Somatic: Pain from skin, muscles, bones, or tissues. It is usually sharp and well localized, meaning you can point right to where it hurts.
Perception of pain
Many factors influence how one copes with pain
Expression of pain
Physiologic reactions
Sensory or emotional reactions
Factors Influencing Pain Response
Physiologic Factors
Culture
Nurse must understand how culture mediates the response to pain
Anxiety
Previous Experience
Comfort
Support
Environment
Nonpharmacologic Pain Management: Methods for preparing for labor and birth: Relaxing and Breathing Techniques
Focusing and Relaxation Techniques
Breathing Techniques:
Slow breathing
Quick breathing
Patterned breathing
Effleurage and Counterpressure
Touch and Massage
Application of Heat and Cold
Nonpharmacologic Pain Management: other
Acupressure and Acupuncture
Transcutaneous Electrical Nerve Stimulation (TENS)
Water Therapy (Hydrotherapy)
Intradermal Water Block
Aromatherapy
Music
Hypnosis
Pharmacologic Pain Management: sedatives
define
Barbiturates
Phenothiazines
Benzodiazepines
Sedatives: relieve anxiety and induce sleep; may be given to a woman experiencing a prolonged early phase of labor when there is a need to decrease anxiety and promote sleep.
Barbiturates – rarely used in obstetrics
Phenothiazines - rarely used in obstetrics
Benzodiazepines – when given with an opioid analgesic, pain relief is enhanced, and nausea and vomiting are reduced
Pharmacologic Pain Management: Anesthesia & analgesia
anesthesia
analgesia
Anesthesia encompasses analgesia, amnesia, relaxation, and reflex activity. the temporary loss of all physical sensation, including pain, often accompanied by loss of consciousness
Analgesia: the alleviation of the sensation of pain or the raising of the threshold for pain perception without loss of consciousness or total feeling
The type of analgesic or anesthetic chosen is determined in part by the stage of labor of the woman and by the method of birth planned.
Pharmacologic Pain Management:
Systemic Analgesia
Nerve Block Analgesia and Anesthesia
Systemic Analgesia: Opioids readily cross the placenta; effects on the fetus and newborn can be profound; their analgesic effect in labor is limited
Opioid (narcotic) antagonists (Narcan)
Nerve Block Analgesia and Anesthesia: used to produce sensory blockade and various degrees of motor blockade over a specific region of the body
Local Perineal Infiltration Anesthesia
Pudendal Nerve Block
Spinal Anesthesia (Block)
Post–dural puncture headaches
Epidural blood patch
Pharmacologic Pain Management: Epidural
Epidural Anesthesia or Analgesia (block):
Combined spinal-epidural (CSE) analgesia:
Epidural Anesthesia or Analgesia (block): currently the most effective pharmacologic pain relief method for labor
Effectively relieves the pain caused by uterine contractions but does not completely remove the pressure sensations
Advantages and Disadvantages
Combined spinal-epidural (CSE) analgesia: sometimes referred to as a “walking epidural,” although women often choose not to walk because of sedation and fatigue, abnormal sensations in and weakness of the legs, and a feeling of insecurity
Epidural and Intrathecal (spinal) opioids
Contraindications to subarachnoid and epidural blocks
Epidural Block Effects on Newborn
Active or anticipated serious maternal hemorrhage
Maternal hypotension
Maternal coagulopathy
Infection at the injection site
Increased intracranial pressure
Allergy to the anesthetic drug
Maternal refusal or inability to cooperate
Some types of maternal cardiac conditions
Epidural Block Effects on Newborn
No evidence that it has a significant effect on the child's later mental and neurologic development
Pharmacologic Pain Management
Nitrous oxide for analgesia
General anesthesia
Nitrous oxide for analgesia
Nitrous oxide mixed with oxygen can be inhaled in a low concentration (50% or less) to provide analgesia during labor and birth.
General anesthesia
Rarely used for uncomplicated vaginal birth
The woman should be premedicated with (clear) oral antacid to neutralize the acidic contents of the stomach.
Because of this risk for neonatal narcosis, it is critical that the baby be delivered as soon as possible after inducing anesthesia, to reduce the degree of fetal exposure to the anesthetic agents and the CNS depressants administered to the mother.
Pain Assessment During Labor and Birth
when should a pain scale be done
what should it also evaluate
A pain scale is often used to evaluate a woman’s pain before and
after interventions are implemented.
Pain assessment should also evaluate her ability to cope with labor and her overall satisfaction with the labor and birth experience.
Fetal Heart Rate Patterns: baseline FHR
variability
4 possible categories of variability:
Variability
Described as irregular waves or fluctuations in the baseline FHR of two cycles per minute or greater
4 possible categories of variability:
Absent
Minimal
Moderate
Marked
Fetal Heart Rate Patterns
Tachycardia:
Bradycardia:
Periodic changes
Episodic
Accelerations
Tachycardia: >160 beats/min 10 minutes or more
Bradycardia: <110 beats/min 10 minutes or more
Periodic & Episodic Changes in FHR
Periodic changes occurring with Uterine contractions
Episodic (nonperiodic changes) not associated with uterine contractions
Accelerations: Considered an indication of fetal well-being
Periodic & Episodic Changes in FHR
Decelerations may be
Early decelerations caused by
Late decelerations caused by
Variable decelerations caused by
Prolonged decelerations defined
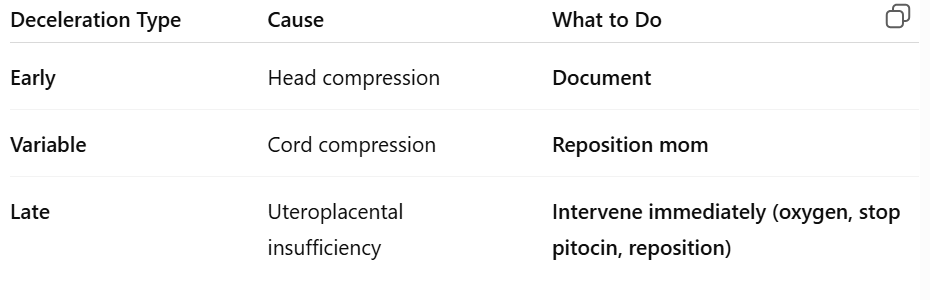
Decelerations – may be benign or abnormal
Early decelerations in response to fetal head compression
Late decelerations due to uteroplacental insufficiency
Variable decelerations due to umbilical cord compression
Prolonged decelerations - lasting more than 2 minutes but less than 10 minutes
Fetal Heart Rate Categories: Category I (normal)
baseline FHR normal range
Baseline fetal heart rate variability
late or variable decelerations
early decelerations
accelerations
Baseline FHR in the normal range of 110-160 beats/min
Baseline fetal heart rate variability: moderate
Late or variable decelerations: absent
Early decelerations: may be present or absent
Accelerations: either present or absent
Fetal Heart Rate Categories: Category II ( indeterminate)
baseline FHR
Baseline fetal heart rate variability
late or variable decelerations
accelerations
decelerations
Bradycardia not accompanied by absence of baseline variability
Tachycardia
Minimal or absence of baseline variability not accompanied by recurrent decelerations
Marked baseline variability
No accelerations in response to fetal stimulation
Periodic or episodic decelerations
Fetal Heart Rate Categories: Category III (abnormal)
baseline FHR associated with…
Baseline fetal heart rate variability
decelerations
Nonreassuring FHR patterns associated with fetal hypoxemia
Hypoxemia can deteriorate to severe fetal hypoxia
Absence of baseline variability
Recurrent or late decelerations
Bradycardia
Nursing management of abnormal patterns
The five essential components of the FHR tracing that must be evaluated regularly are
intrauterine resuscitation & process
The five essential components of the FHR tracing that must be evaluated regularly are:
baseline rate, baseline variability, accelerations, decelerations, and changes or trends over time
intrauterine resuscitation: If any component is abnormal, corrective measures must be taken immediately to improve fetal oxygenation
Assist woman to a side-lying (lateral) position
Increase maternal blood volume by increasing the rate of primary IV infusion
Routine use of oxygen supplementation in individuals with normal oxygen saturation for fetal intrauterine resuscitation is not recommended
FHR Monitoring: Care Management: Other Methods of Assessment and Intervention: Assessment Techniques
Fetal scalp stimulation and vibroacoustic stimulation
Umbilical cord acid-base determination
Fetal scalp blood sampling
Amnioinfusion
Tocolytic therapy
Client and Family Teaching
Documentation
Deceleration: cause and what to do
early
variable
late
Traditionally first stage of labor dilation by phase
latent phase
active phase
transition phase
Traditionally, the first stage of labor was
considered to be composed of three
phases
Latent phase (up to 3 cm of dilation)
Active phase (4 to 7 cm of dilation)
Transition phase (8 to 10 cm of dilation)
However, these definitions have changed based on research findings
New definition of the First Stage of Labor
how many phases
define each phase
NOW, divided into only two phases:
1. Latent Phase - extends from the onset of labor,
characterized by regular, painful uterine contractions that
cause cervical change, to the beginning of the active phase,
when cervical dilation occurs more rapidly. 1-5cm
2. Active Phase - defined as the period during which the greatest rate of cervical dilation occurs, which begins at 6 cm, and ends with complete cervical dilation at 10 cm
First Stage of Labor: Care Management
how to determine if it is a true labor (3)
Obstetric triage and EMTALA
Determination of whether the woman is in true labor or false labor
Contractions
Cervix
Fetus
Obstetric triage and EMTALA
Emergency Medical Treatment and Active Labor Act
A pregnant woman presenting to an obstetric triage area is presumed to be in “true” labor until a qualified HCP certifies that she is not.
supportive care during first stage of labor
supportive care includes
labor supported by
Supportive care during labor and birth: emotional support, physical care and comfort measures, and advice/information.
Labor Support by:
• Nurse
• Father or Partner
• Doulas
• Grandparents
• Siblings during labor and birth
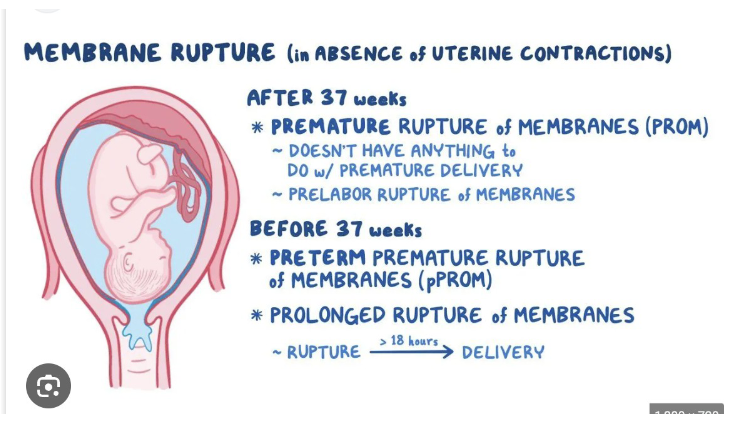
membrane Rupture in absence of uterine contractions
PROM
PPROM
prolonged rupture of membranes
Second Stage of Labor
begins with what
what happens
complete what
also called the ___ stage
end with
Infant is born
Begins with full cervical dilation (10 cm)
Complete effacement
The “pushing” stage
Ends with infant’s birth
Second Stage of Labor
how many phases
define each phase
Ferguson reflex:
Two phases
Latent: sometimes referred to as delayed pushing, laboring down, or passive descent; relatively calm with passive descent of baby through birth canal. the uterus to push the baby down naturally without active maternal pushing right away.
Active: pushing and urge to bear down
Ferguson reflex: activated when the presenting part presses on the stretch receptors of the pelvic floor. stimulates the release of oxytocin from the pituitary gland, Leading to stronger uterine contractions and an involuntary, natural urge to push (bear down)
Second Stage of Labor: Care Management: Preparing for birth
maternal position: western
what position shortens labor
bearing down
valsalva maneuver
Maternal position: supine, semi recumbent, or lithotomy positions are still widely used in Western societies despite evidence that an upright position shortens labor
Bearing-down efforts: mom is actively pushing
Valsalva maneuver: Forceful holding of breath while pushing, increase intra-abdominal pressure and help expel the baby.
Fetal heart rate and pattern
Support of Partner
Supplies, instruments, and equipment
Second Stage of Labor:
most common birthing position
Nuchal cord
Crowning
episiotomy
what is no longer recommended
skin to skin
lotus birth
most common birthing position: Lithotomy position
Nuchal cord: occurs when the umbilical cord wraps around a fetus's neck
Crowning: The moment when the baby’s head is visible at the vaginal opening and will not retract between contractions.
episiotomy: A surgical incision made in the perineum (the area between the vagina and anus) to enlarge the vaginal opening for delivery.
Routinely suctioning the newborn’s mouth and nose on the perineum is no longer recommended
skin to skin: Placing the newborn directly on the mother’s bare chest immediately after birth, often covered with a blanket.
Lotus Birth: Leaving the umbilical cord and placenta attached to the baby until it naturally falls off (usually 3–10 days).
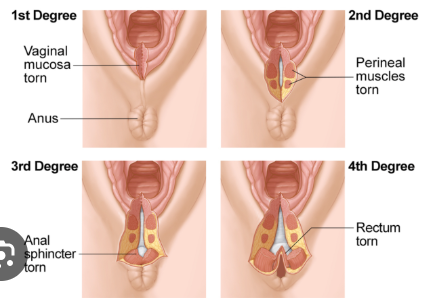
Perineal lacerations
first degree
second degree
third degree
fourth degree
First degree: laceration that is confined to the skin
Second degree: laceration that extends into the perineal body
Third degree: laceration that involves injury to the external anal sphincter muscle
Fourth degree: laceration that extends completely through the anal sphincter and the rectal mucosa
Third Stage of Labor
define
active vs passive management
passive management: the placenta is expelled within how long
signs of placental sepration
Birth of the baby until the placenta is expelled
The third stage is generally by far the shortest stage of labor
Passive versus active management:
Active management: Using medications and controlled traction to deliver the placenta quickly and prevent bleeding.
Passive (expectant) management: Waiting for the placenta to deliver naturally without interventions.
When passive management is practiced, the placenta is usually expelled within 15 minutes after the birth of the baby
Signs of placental separation include lengthening of the umbilical cord and a gush of blood from the vagina.
Vaginal fullness
Placental examination and disposal
Cultural preferences
Fourth Stage of Labor
define
care management
signs of potential problems
care of family
Begins with the expulsion of the placenta
and lasts until the woman is stable in the
immediate postpartum period, usually
within the first hour after birth
Care management
First 1 to 2 hours after birth
Assessment of maternal physical status
Physiologic changes to prepregnancy status
Signs of potential problems
Excessive blood loss
Alterations in vital signs and consciousness
Care of the new mother
Care of the family
Family-newborn relationships
Obstetric Emergencies
After an emergency birth, the nurse encourages the woman to breastfeed her newborn. The primary purpose of this activity is to:
a. Facilitate maternal-newborn interaction
b. Stimulate the uterus to contract
c. Prevent neonatal hypoglycemia
d. Initiate the lactation cycle
B