8.1 restorative dentistry for the pediatric patient
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
what three things should restorative treatment be based on?
Restorative treatment should be based upon the results of an appropriate clinical and radiographic examination, ideally be a part of a documented comprehensive treatment plan and must be prepared in conjunction with an individually-tailored preventive program
tx plan should take into account what five things?
developmental status of the tooth n stage of root resorption n caries risk assessment n caries experience of the patient n the patient's ability to cooperate for
treatment
how do primary teeth differ in anatomy compared to permanent teeth?
(size, enamel and dentin layer thickness, pulp chamber size, pulp horn location and shape, enamel rod direction)
Primary teeth are smaller in all proportions
Enamel and dentin layers are thinner
Pulp chambers are larger
Pulp horns are higher and more pointed
Enamel rods in gingival third extend in occlusal direction from dentin-enamel junction
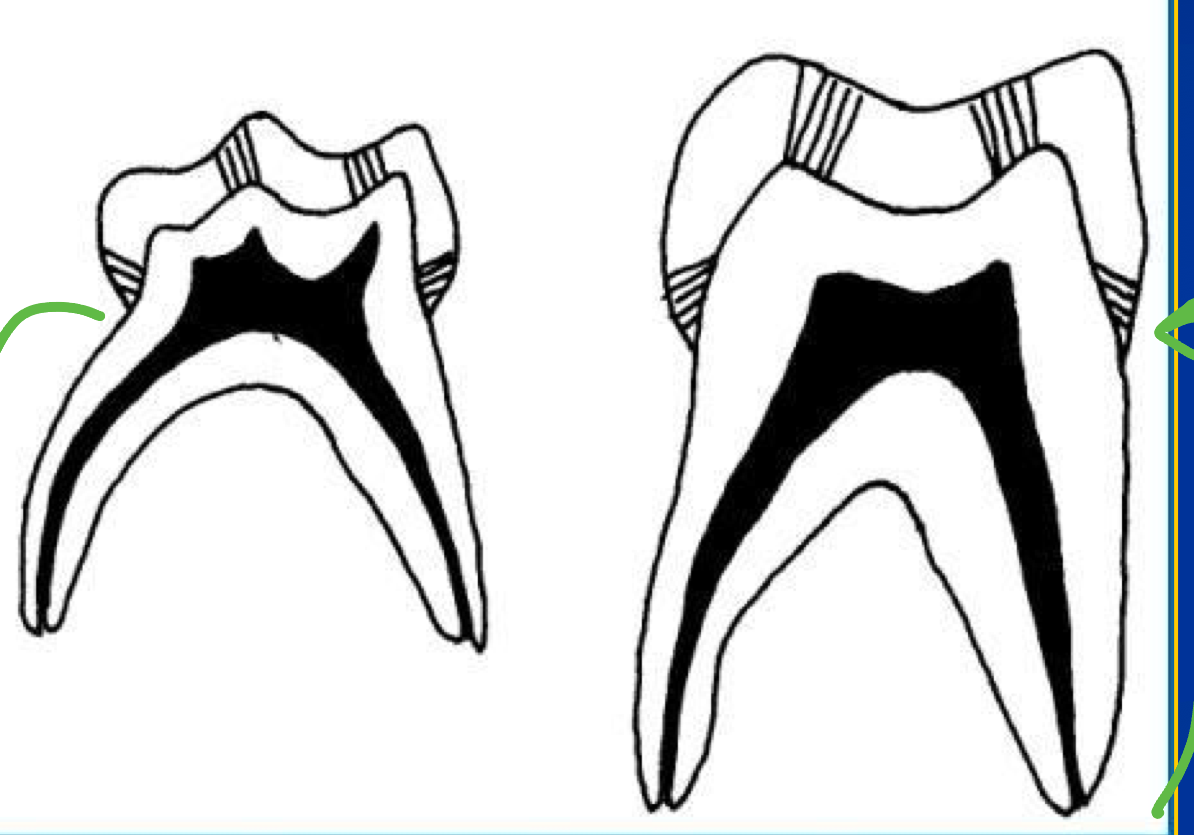
large pulp chambers
primary teeth
higher pulp chambers with higher and more pointed pulp horns
primary teeth
enamel rods in gingival third extend in occlusal direction from DEJ
primary teeth
enamel rods in gingival third extend in gingival direction from DEJ
permanent teeth
teeth A&J and K&T: which type of primary teeth? turn into which permanent teeth?
second primary molars max and mand; turn into permanent second premolars
teeth B&I and S&L: which type of primary teeth? turn into which permanent teeth?
first primary molars max and mand; turn into permanent first molars (look like them too just very small)
contact areas are flat, broad, and wide
primary teeth
since contact areas are flat, broad, and wide you cannot detect what for primary teeth just by looking, you need a bw
interproximal caries
greater constriction of crown at CEJ, more prominent cervical contour
primary teeth
pros and cons of primary teeth greater constriction at the crown and more prominent cervical contour
advantage: stainless steel crown built in retention
disavd: class II prep with the box drop leads to overextension and you may lose gingival floor and expose the pulp
deeper pits and fissures
permanent teeth
roots are more flared and ribbon like due to permanent successor
primary teeth
advantages of rubber dam isolation
Better access and visualization
Moisture control n Safety of child is improved
Results in decreased operating time
Aids in the management of the children
Child becomes primarily nasal breather - good for NO
contraindications for rubber dam isolation (3)
Presence of some fixed orthodontic appliances
Recently erupted molars will not retain a clamp
Child with upper respiratory infection, congested nasal passage, or other nasal obstruction
(BLANK) must always be attached to the clamp
floss
only the tooth being restored must be isolated
Class I and V
at least one anterior and one tooth posterior to tooth being restored should be isolated
Class II
options for restoration of primary molars
amalgam, adhesive materials, stainless steel crown restorations
options for restoration of primary incisors and canines
adhesive materials, interim therapeutic restorations (ITR)
which restoration option for primary molars: Class I and II
amalgam
which restoration option for primary molars: CAR (conservative adhesive restorations), Class I, Class II
adhesive materials
which restoration option for primary incisors and canines: Class III, V
adhesive materials
Objectives: To restore form and function in primary and permanent teeth
Indications: They are indicated for the restorations of carious lesions and/or developmental defects in primary and permanent teeth
amalgam
ideal pulpal floor depth is (?)mm into dentin for class I amalgam primary molars
0.5
all internal angles should be (?) for class I amalgam primary molars
rounded
retention is given by (?) shape of 330 bur for class I amalgam primary molars
pear
leave (?) with enough dental support (do not cross bc it is is a strong tooth structure)
oblique ridges

some common mistakes with amalgam restorations
Failure to include all susceptible pits and fissures
Pulpal wall too deep
Undercutting the marginal ridges
Carving the anatomy of the amalgam too deep
Not removing the amalgam flash from the cavosurface margins
Under-carving which leads to subsequent fracture of the amalgam from hyperocclusion
isthmus width should be 1/3rd the (?) distance ± 0.5mm for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth
intercuspal
break buccal and lingual contacts with adjacent tooth Class II Cavity Preparations for Amalgam Restorations for Primary Teeth
true
break gingival wall contacts and do not bevel and stay at the gingival crest for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth
true
axial wall is past the dentin for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth
false, just into the dentin
for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth the proximal box should be (?) at the cervical portion
broader
for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth, retentive grooves should be placed
false, no retentive grooves
for Class II Cavity Preparations for Amalgam Restorations for Primary Teeth all internal angles should
rounded
common errors with class II amalgam restorations
Failure to extend occlusal outline into all susceptible pits and fissures
Failure to follow outline of cusps
Isthmus cut too wide - restoration will break
Flare of proximal wall too great
Angle formed by the axial, buccal, and lingual walls too great
Gingival contact with adjacent tooth not broken
Axial wall not conforming to the proximal contour of the tooth, and the mesiodistal width of the gingival floor is greater than 1mm
describe T-band matrix application
It is formed into circle
The extension wings are folded down to secure the band
The T- band is adapted to fit the tooth tightly, it is trimmed with scissors and the free end is bent back
Less need for contouring matrix bands
These materials do not require extensive removal of non-carious tooth structure to establish appropriate retention form and are more esthetic for anterior tooth restorations
Objectives: To restore form, function and esthetics
adhesive material
Indications:
All surfaces of anterior teeth, including those with developmental or acquired defects
Up to two surfaces of posterior primary or permanent teeth
Contraindications:
Where tooth cannot be isolated to obtain moisture control
In patients needing large multiple surface restorations in the posterior primary dentition n In high caries risk patients
adhesive materials
Advantages:
Excellent esthetic qualities - especially resin based
More conservation of tooth structure in cavity preparation
Restorative material bonds to the tooth
Elimination of mercury
Low thermal conductivity
Disadvantages:
Technique sensitive
Increased operator time
Potential marginal leakage
Possible postoperative sensitivity
adhesive materials
Technique sensitive, good occlusal wear resistance, good color stability and more esthetic
resin-based composites
Very limited life span. Chemically bond to both enamel and dentin, uptake and release fluoride, decreased moisture sensitivity
glass ionomers
More color change and occlusal wear than resin-based composites, chemically bond to both enamel and dentin, release fluoride, lower polymerization shrinkage
resin-modified glass ionomers
combines the preventive approach of sealing susceptible pits and fissures with conservative Class I cavity preparation of caries occurring on the same occlusal surface
limits cavity preparation to the discrete areas of caries
Bonding agent and an adhesive material are placed in the preparation and then a sealant is applied over the remaining susceptible pits and fissures
CAR (conservative adhesive restoration)
what can you use to ensure all caries are removed for class I and class II cavity preparations for resin-based composite restorations?
caries detecting dye
non carious pits and fissures can simply be sealed
true
retention for class I and class II cavity preparations for resin-based composite restorations is obtained micromechanically with what technique and what item?
with acid etching technique and with the use of bonding agents
for class I and class II cavity preparations for resin-based composite restorations break which three contacts
buccal, lingual, and gingival
for class I and class II cavity preparations for resin-based composite restorations
for class I and class II cavity preparations for resin-based composite restorations at least an equal amount of dentin that is found on the gingival floor of the box should be prepared on the (?) surface; 50-50 rule
occlusal surface
for class I and class II cavity preparations for resin-based composite restorations what materials are used?
T-band and wooden wedge
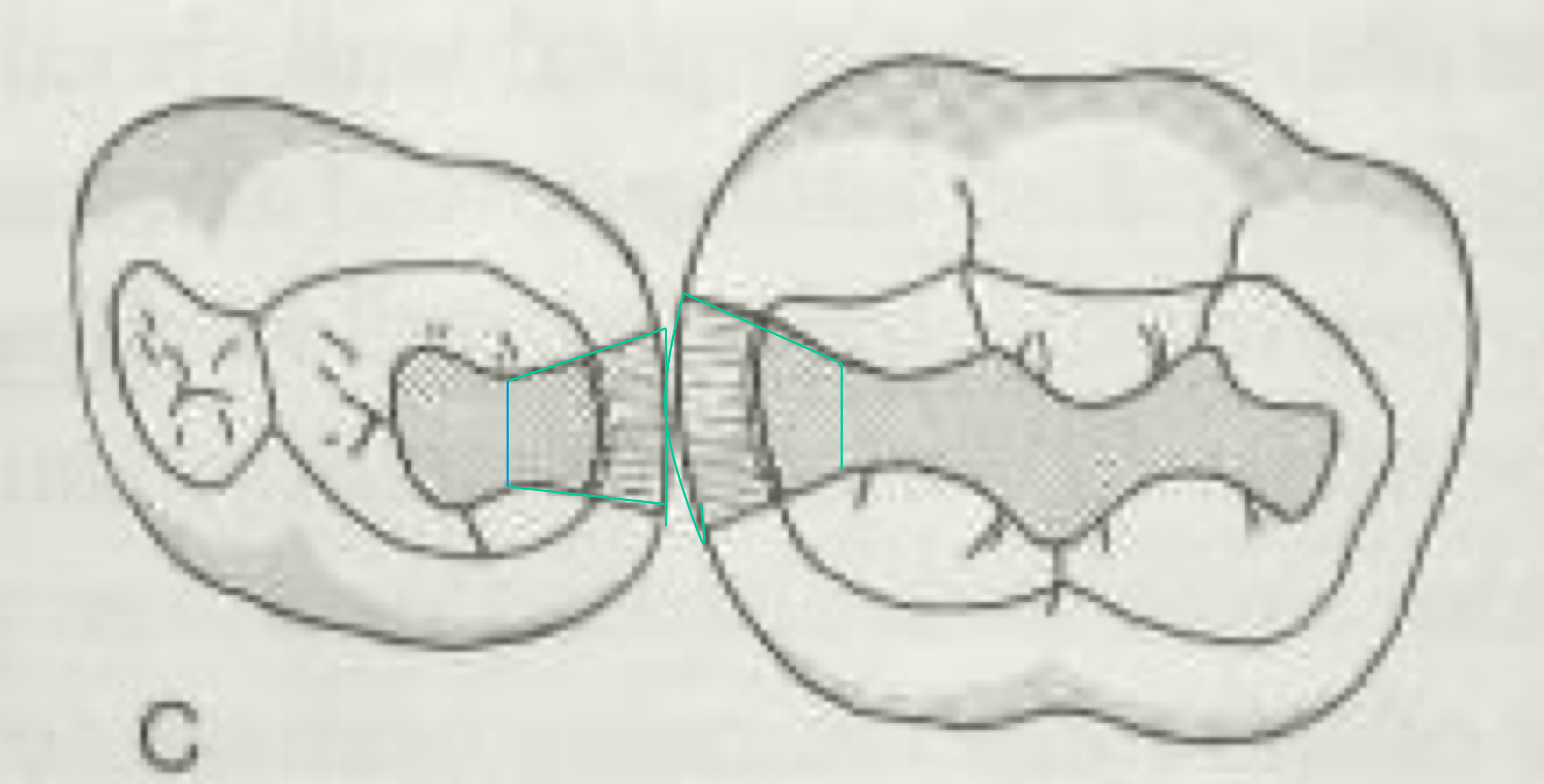
which is the amalgam surface? composite?
gray outline amalgam and green-blue is composite
prefabricated crown forms that are adapted to individual teeth and cemented with a biocompatible luting agent
stainless steel crowns
Objectives: To restore form and function in primary and permanent teeth
Advantages:
Extremely durable
Relatively inexpensive
Offer the advantage of full coronal coverage
Subject to minimal technique sensitivity during placement
stainless steel crowns
Indications:
Restoration of primary or young permanent teeth with extensive carious lesions - open apex
Restoration of primary teeth following pulpotomy or pulpectomy procedures n In patients with increased caries risk whose cooperation is affected by age, behavior, medical history or require general anesthesia for treatment
Intermediate restoration of fractured permanent posterior teeth
Restoration of primary teeth to be used as an abutment for a space maintainer
Restoration of hypoplastic or hypocalcified primary or permanent teeth n Restoration of teeth with hereditary anomalies (dentinogenesis imperfecta or amelogenesis imperfecta)
Failure of other available restorative materials
others: don’t need a completely dry field
stainless steel crowns
stainless steel crowns come in 2-7 sizes with (?) as the most common
4 (and 5)
stainless steel crowns are usually places 1mm below gingival margin, take them out and tighten with cotton pliers, tighten some more and cement
true
Very challenging restorations
Caries often extend subgingivally
Extra retention is often required - due to size
Preparations must be kept small because of the large size of the pulps
Slot preparation with a dove tail is used for both incisors and canines
Retention can be gained by beveling the cavosurface margin
class III adhesive restorations
An atraumatic minimally invasive procedure that involves removal of caries using hand or slow speed rotary instrument with caution not to expose the pulp.
The tooth is restored with an adhesive restorative material such as glass ionomer or resin-modified glass ionomer cement
ITR (interim therapeutic restorations)
ADVANTAGES
Prevention of further decalcification and caries in young patients, uncooperative patients, or patients with special health care needs
Protection of the tooth in cases that traditional cavity preparation and/or placement of traditional dental restorations are not feasible and need to be postponed.
Reduction of the levels of cariogenic oral bacteria
The need of local anesthesia is eliminated.
Glass ionomer (fluoride releasing material) helps prevent further caries.
ITR (interim therapeutic restorations)