Unipolar Depression
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
17 Terms
Unipolar Depression
An affective disorder characterised by low mood, loss of interest or enjoyment and marked by fatigue, which must be experienced for more than 2 weeks.
Features of Depression
British Psychological Society (BPS):
Nearly a fifth (19%) of British adults have reported an episode of depression
Depression is more prevalent among women (30%) than men (15%)
Depression is reported by 27% of divorced or separated people, compared to 20% of people who are single and 16% of people in stable relationships
People in lower-income households are more likely to report depression compared to wealthier households
The most at-risk age group is 50-54
APMS found that the prevalence of diagnosable depression was 3.3 people per 100.
Depression is linked to many physical illnesses like cancer and cardiovascular disease.
Symptoms of Depression
Affective symptoms: depressed mood, feelings of worthlessness and guilt, pessimism about the future and a lack of interest in things that used to be enjoyable are all reported by people with depression. This is called negative affect.
Cognitive symptoms: other symptoms include fatigue, difficulty concentrating and indecisiveness (these are mental symptoms but they're not to do with emotion).
Behavioural symptoms: people with depression often abandon hobbies and pastimes, work and study; they withdraw from relationships with friends and family, leading to diminished activity. Shown for at least 2 weeks.
Bodily symptoms: Reduced energy levels. people with depression often experience loss of appetite (or sometimes increased appetite) along with unexplained aches and pains; they move and speak slowly and there are changes in their sleep patterns (some sleep all the time, some can't sleep at all).
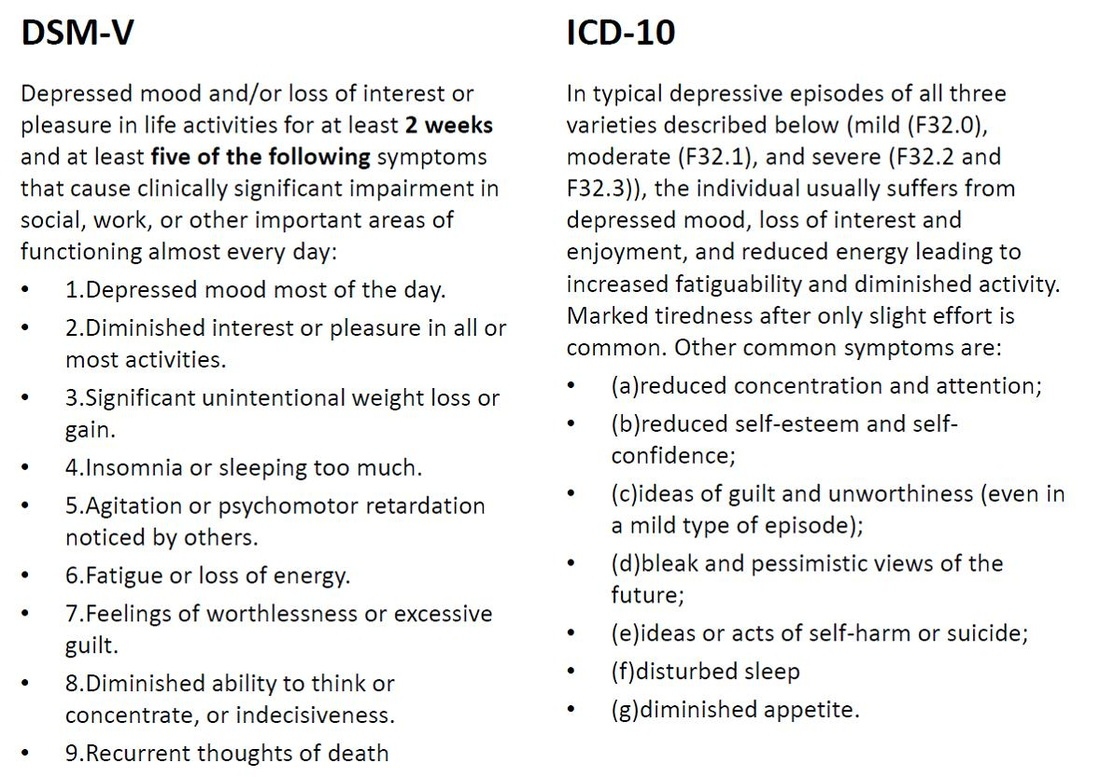
DIAGNOSIS OF DEPRESSION USING ICD-10 AND DSM-5
DSM-5 requires at least 5 of these symptoms evident for at least two weeks to diagnose a Major Depressive Disorder. There are two key symptoms in DSM: depressed mood and loss of interest. At least one must be in evidence to make a diagnosis, but the severity of the diagnosis is based on the number of extra symptoms and the degree of dysfunction they create.
ICD-10 requires 4 symptoms for mild depression, 6 for moderate depression and 8 for severe depression. There are three key symptoms in ICD-10: depressed mood, loss of interest, and decreased energy. For mild or moderate depression two of the three must be in evidence and for severe depression all three must be evident.
EVALUATING THE DIAGNOSIS OF DEPRESSION (AO3)
Supporting Research:
The DSM-5's definition has converged with ICD-10, now that both include "feelings of unworthiness and excessive guilt". This makes diagnosis more reliable and valid because clinicians are looking for the same symptoms.
There used to be a danger of False Negatives when diagnosing depression in people who had been recently bereaved. By removing the "bereavement exclusion", DSM-5 makes it more likely that someone with depression will be diagnosed and treated, whereas in the past they might have been dismissed as "just grieving" for the recent death of a relative.
Opposing Research:
Cultural Differences - Cooper et al. (1972) asked American and British psychiatrists to diagnose patients by watching a number of filmed clinical interviews. The British psychiatrists diagnosed the patients to be suffering from depression twice as often as the American psychiatrists (who diagnosed them with schizophrenia).
Sadness and anxiety is a normal (even, a healthy) response to many life events, like bereavement, relationship break-up and work stress. False Positive diagnosis leads to a healthy person being diagnosed with depression and being prescribed anti-depressant medication. This person will believe themselves to be sick and in need of drugs, when they aren't.
Different Theories:
A short period of time means a sick person is more likely to be diagnosed (and treated) quickly. However, this increases the risk of a False Positive, because lots of things can cause people to behave abnormally for short periods (stress, grief, drugs, etc.).
Application:
In Bradshaw's case study, Carol was diagnosed using DSM-IV with undifferentiated type schizophrenia. However, many of her symptoms matched unipolar depression (negative affect, social withdrawal, cognitive symptoms) and the therapy used (CBT) is one that is traditionally used for depression. This shows that there is overlap between the two conditions.
In Rosenhan's study, 7 of the pseudopatients were admitted with diagnoses of schizophrenia; the eighth was diagnosed with "manic-depressive psychosis". This also shows the overlap between symptoms of depression and symptoms of schizophrenia and the risk of misdiagnosis of both.
Biological Explanation For Depression
Monoamine Depletion Hypothesis: Monoamines are a group of neurotransmitters that regulate mood; they include serotonin, noradrenaline and dopamine.
Criticism: Oversimplification
Schildkraut (1965): Depressed mood states can be caused by low levels of noradrenaline or dopamine, but the main culprit is the serotonin, which is controlling the other two. A particular gene called 5-HTT has been linked to regulating serotonin levels. People with variations of the 5-HTT gene that are under-active seem more likely to suffer depression after stressful life events.
When serotonin levels are low, levels of noradrenaline drop and noradrenaline provides attention and reward. Low levels of noradrenaline are linked to a lack of pleasure.
Low levels of serotonin causes dopamine levels to drop and dopamine is related to alertness and energy. Low levels of dopamine are linked to anxiety.
Receptor Sensitivity Hypothesis: Depression is caused by changes in the sensitivity of postsynaptic receptors.
David et al. (2002) - Depressed Patients had reduced serotonin receptor binding in certain areas of the brain. Many antidepressants enhance neurotransmitter availability and reduces MAOA (which removes too much monoamine).
Criticism: Unclear whether changes are a cause or effect
Brain-Derived Neurotrophic Factor (BDNF) Hypothesis: BDNF is a protein that supports the growth, survival and differentiation of neutrons; important for neuroplasticity.
Low levels of BDNF reduce the brain’s ability to regulate mood and impairs memory.
MacQueen et al. (2003) - Patients with depression had lower BDNF levels.
Criticisms: Complex relationship between BDNF and Depression and ignores influence of other biological factors.
Evaluation Of Biological Explanation For Depression
STRENGTHS:
Wender et al. (1986) - Twin and adoption studies support how depression is more common in first relatives
Supports BDNF Hypothesis - Martinowich et al. (2007) found brains of people with depression had low levels of BDNF in the PFC and hippocampus.
WEAKNESSES:
Rosenthal’s diathesis-stress model - Genes can predispose an individual to having a higher risk of getting depression but environmental triggers must be present.
Thase et al. (2002) found that depressed patients (especially those with severe depression) had increased levels of noradrenaline, which challenges the monoamine hypothesis.
Biological explanation is reductionist.
Non-Biological Explanation For Depression
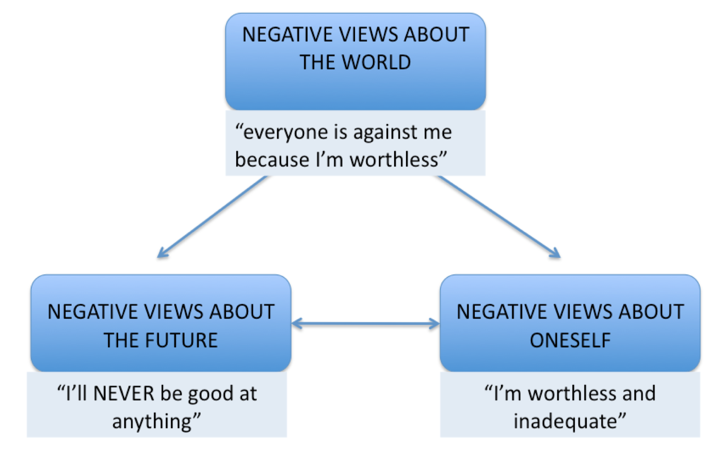
Negative Cognitive Triad
Negative view about the self
Negative view about the future
Negative view about the world
Beck's negative cognitive triad is a vicious cycle where people have negative views about the world that influence their feelings about themselves and their expectations of the future. Negative views about oneself and the future feed back into a negative worldview. People then act on these feelings, usually by giving up on projects, withdrawing from relationships and blaming themselves. This destructive behaviour causes them to fail at things and struggle in relationships, which convinces them that their core beliefs are right.
Cognitive biases
magnification: problems are exaggerated
minimisation: strengths and opportunities are under-emphasised
personalisation: the individual blames themselves for things that are actually beyond their control
Polarised thinking - setting unattainable standards like expecting to be like everybody else or something is wrong
3. Negative schemas
Develop during childhood, usually through critical relationships (like parents who are too perfectionist or school cliques that are judgmental) or traumatic events (like the death of a family member, childhood abuse or bullying at school).
According to Freud's psychodynamic approach, abnormality is caused when trauma from unresolved conflict between the id, ego, and superego is repressed into the unconscious. Freud believed that in people with depression the superego (or conscience) is over-developed. This explains the excessive guilt and the sense of worthlessness people with depression feel.
Ellis ABC Theory
Adversity (Activating Event) - Not getting selected for the school choir
Beliefs - Believing that they have a terrible voice
Consequences - Feeling sad and giving up on singing
David et al. (2010) - musterbation and catastrophising
Evaluation Of Non-Biological Explanation For Depression (AO3)
STRENGTHS:
A high level of face validity because people with depression do align with Ellis’ and Beck’s theories.
Evans et al. (2005) measured self-beliefs of 12,003 pregnant women and women who had the most negative beliefs were the most likely to become depressed.
Elliot et al. (1997) found that those with depression had an abnormal response to negative feedback which negatively affected their feedback, showing how their thought processing differs.
Challenging faulty beliefs with CBT can change negative thoughts.
WEAKNESSES:
Biological Explanation of depression & negative schemas → Hammack et al. (2011) showed that serotonin is linked to feelings of helplessness as well as activity in the amygdala. Serotonin and the amygdala are known to be linked to depression as well.
Dohr et al. (1989) - negative self-beliefs expressed during a depressive episode usually become positive later, supporting how situational factors also have an impact.
Reductionist as it ignores genetic explanations with an overemphasis on cognition.
Cultural bias and limitations to collectivist cultures.
Eysenck (1997) suggests Beck’s negative cognitive triad may be a better explanation of how depressive episodes are triggered & maintained over time.
Biological Treatment for Depression
Monoamine Oxidase Inhibitors (MAOIs): Oldest antidepressants
Mechanism: Blocks the enzyme monoamine oxidase (MO) from breaking down serotonin, dopamine and noradrenaline which improves mood.
This allows the re-uptake of excess neurotransmitters into the presynaptic neuron.
Examples: Phenelzine
Side Effects: High blood pressure, insomnia, weight gain
Effectiveness: Used as a last resort because of dietary issues
Selective Serotonin Re-uptake inhibitors (SSRIs):
Mechanism: Blocks re-uptake of serotonin in the brain which increases availability.
Example: Fluoxetine
Side Effects: Nausea, insomnia, sexual dysfunction
Effectiveness: Often the first antidepressant used
Serotonin-noradrenaline re-uptake inhibitors (SNRIs):
Mechanism: Blocks re-uptake of both serotonin and noradrenaline, increasing availability.
Example: Duloxetine
Side Effects: High blood pressure, increased heart rate, similar to SSRIs
Effectiveness: Effective for patients who do not respond to SSRIs
Noradrenergic & Specific Serotonergic Antidepressants (NaSSAs):
Mechanism: Enhances release of noradrenaline and serotonin by blocking certain serotonin receptors.
Example: Mirtazapine
Side Effects: drowsiness, weight gain
Effectiveness: beneficial for individuals who did not have success with SSRIs or SNRIs and those experiencing severe sleep or appetite issues.
Evaluation Of Biological Treatment for Depression
STRENGTHS:
Meta-Analysis → Cipriani et al. (2018) reviewed studies of 21 anti-depressants and from 522 double-blind trials, all drugs were found to be more effective than a placebo. This supports the effectiveness of antidepressants.
Quick symptom relief compared to talk therapies
Effective for moderate to severe depression
WEAKNESSES:
Limited benefits - antidepressants do not tackle causes of depression and only relieve symptoms
Varied harmful side effects
Kirsch et al (2008) who reviewed 47 trials of patients with mild or severe depression who were prescribed SSRI antidepressants or a placebo (sugar pill) that looked like an antidepressant. The patients with severe depression did show a statistically greater response to antidepressants than to placebos. This suggests that antidepressants do work - but that a lot of their effectiveness can be explained by the Placebo Effect because patients feel better if they believe in the treatment they are getting (even if it doesn't do anything).
Alternatives → In the long-term, CBT is more beneficial and does not have harmful side effects.
Hollon et al. (2005) studied patients who received treatment for 16 weeks then were observed for 12 months to see if their symptoms returned (relapse). There were 3 groups: (1) patients who received CBT; (2) patients who received drug therapy; and (3) patients received drug therapy which continued over the 12 month observation period. Only 31% of CBT patients suffered a relapse compared to 76% of those treated with drugs and 47% of the patients who carried on taking antidepressants.
These findings support the integrated approach (CBT + medication) which requires further research.
APPLYING BIOLOGICAL EXPLANATIONS OF DEPRESSION (AO2)
Understanding the link between schizophrenia and serotonin has led to the development of effective antidepressant drugs, like monoamine oxidase inhibitors (MAOIs), which inhibit monoamine oxidase A (MAO-A) and reduce depressive symptoms.
These drugs only "mask" the symptoms of depression and have unpleasant side-effects of their own. The research into the 5-HTT gene offers hope that in the future therapies could “turn up” the level of serotonin in individuals who show early symptoms of depression, which would prevent depression from developing in the first place.
APPLYING NON-BIOLOGICAL EXPLANATIONS OF DEPRESSION (AO2)
CBT - The patient (client) talks about their experiences with their therapist. Working together, the client and therapist develop a model of what’s causing the depressive episodes. These factors vary from person to person: some people need to view relationships differently, others need to be more optimistic about the future, some need adopt new ways of interacting with people around them.
Contemporary Study: Kroenke et al. (2008)
Aim:
Assess the PHQ-8 as an effective method of measuring depression in a large-population based survey. A need for a quick, reliable screening tool in clinical settings.
In particular, to see if there is a difference between diagnosis of depression using the PHQ-8 algorithm and using the PHQ-8 score of ≥ 10.
Procedure:
Monthly telephone survey conducted in all US states
Trained interviewers collected data from 198,678 adults
This was part of a regular survey called the Behavioral Risk Factor Surveillance Survey (BRFSS) in the USA. This survey is into health in general - infectious diseases, asthma, domestic violence, etc - but in 38 states questions were asked about depression using PHQ-8. Telephone numbers are produced randomly by a computer and people who answer are invited to take part.
PHQ-8 eight-item Patient Health Questionnaire rated on a 4 point Likert scale that covered 8 DSM-4 symptoms
HRQoL: Researchers analysed 3 telephone surveys and self-assessed the number of days (out of 30) where their physical and mental health was not good which impaired them from completing normal activities.
Cutpoint Method: Depression had a score of 10 or more
Diagnostic Algorithm Method: 7 or more days on 5/8 of DSM-4 symptoms
Profiling of Depressed Respondents:
Women
Non-White
Unmarried and unemployed
Below 55
Results:
9.1% of respondents were judged to have a depressive disorder based on the PHQ algorithm; 8.6% scored ≥10 on PHQ-8.
According to DSM-IV, out of the 17,040 respondents with a PHQ-8 score > 10, major depressive disorder (MDD) was present in 49.7%, other depressive disorders in 23.9% and depressed mood or anhedonia in another 22.8%. In only 3.5% was there no evidence of depressive disorder or depressive symptoms according to DSM-IV.
Mental and physical health impairments were very similar between the cutpoint and diagnostic algorithm method.
Conclusions:
PHQ-8 is valid, reliable, and practical.
The PHQ-8 is a useful depression measure for population-based studies. Its cutpoint ≥10 can be used for diagnosing depression.
Evaluation Of Contemporary Study: Kroenke et al. (2008)
STRENGTHS:
Standardised procedures - same questions asked
Simple and cost-effective
Large sample size increases generalisability
Data is confidential - protects anonymity
PHQ-8 can reduce under-diagnosis of depression
WEAKNESSES:
BRFSS was only accessible to people with telephones
May overlook less severe cases of depression
Social Desirability Bias influenced self-reported data
The study was carried out in 38 of the 50 US states, including big cities and rural areas and even Hawaii. This suggests a representative sample. The study also included a range of ethnicities and age groups (age 18 through to 75+). People that answered may have had severe mental health problems as people would not complete a health survey if there is nothing wrong with them.
Asking the questions over the telephone is a bit more unreliable because it introduces researcher effects. Respondents might want to conceal health problems from a stranger that they would write about if filling out the PHQ by themselves.
Telephone surveys are also unreliable because the respondent might not answer on the 4-point (0-3) scale as they are supposed to, but instead start describing their experiences (qualitative data), forcing the researcher to make a (subjective) decision about how to score the response.
One Non-biological treatment
Ellis’ Rational Emotive Behavioural Therapy (REBT):
The therapist gets the client to identify an "activating event" - something they believe is the trigger for their problems. For someone with unipolar depression, this might be a stressor like work, family conflicts or social interactions. The client then identifies their "beliefs" about this event.
People with depression often think that other people are critical of them or that tasks are beyond their ability. Therapist and client then explore the "consequences" of these beliefs, such as how socially withdrawing from people or challenges leads to isolation and failure.
Kendall & Hammen (1998) - CBT:
Patients’ interpretations of themselves and the world around them are different from what is actually the case.
Thoughts, behaviour and feelings are interrelated and so it is wrong to identify one of these factors (eg. behaviour) as being more important than the others.
Treatment needs to change the way people think about themselves and the world around them.
Treatment needs to change the client’s cognitive processes and behaviour; the benefits will be greater by tackling both.
Psychoanalysis:
Free association: the client says whatever comes into his or her mind and the analyst looks for connections between seemingly-unconnected ideas. According to Freud, long pauses indicate that the client is uncovering repressed ideas. Techniques like the Rorschach inkblot test can help with free association.
Dream analysis: in dreams the "censor" in our minds that keeps the repressed thoughts in the unconscious is less effective. Repressed material in dreams appears in disguised or symbolic form. Dream analysis involves interpreting the symbol and questioning clients about their dreams to work out what they mean.
Transference: The client transfers feelings they have towards their parents onto the analyst. Transference brings to the surface conflicts from the client's childhood and uncovers repressed memories.
Evaluation Of One Non-biological treatment
STRENGTHS:
Stiles et al. (2006) examined the use of cognitive and psychodynamic therapies in the NHS over a 3-year period. All the therapies showed a reduction in relapse rates (people getting depressed again) and an improvement in clients' mood according to self-reports. Psychoanalysis came out as effective as CBT, This shows that tackling cognitions is an effective treatment.
Elkin et al. (1989) - randomly allocated 239 participants diagnosed with schizophrenia to one of four treatment groups. CBT was found to be just as effective in reducing symptoms as antidepressant medication or interpersonal therapy.
Shea et al. (1992) - CBT was effective even after an 18 month follow-up.
Elkin and Shea shows how CBT is a successful treatment for mild to moderate depression in the short and long term.
WEAKNESSES:
CBT is accused of being reductionist: it places too much emphasis on cognitions. Often, a person with depression has relationships and a social environment that don't just seem bad to them, but which are objectively bad. Certain biological factors also cannot be changed just by thinking differently.
Easterbrook & Meehan (2017) - CBT practitioners have downplayed the importance of client-therapist relationships.
CBT has high dropout rates and requires commitment.
Competing argument → Both Elkin and Shea’s studies showed how CBT is not useful for treating severely depressed participants. 36% of recovered CBT patients relapsed, so antidepressants and interpersonal therapy may be more effective for these cases. Later studies like DeRubeis et al. (2005) showed how CBT is effective for all types of depression.
Alternatives:
However, in the long term, CBT might be more beneficial. Treatments can either cure the disorder or suppress the symptoms without changing the underlying problem (palliative treatments). Drug therapy for unipolar depression is palliative rather than curative, which is why there are high relapse rates when the drugs are stopped. CBT is curative instead.
Segal et al. (2006) tested patients who had recovered from depression after receiving either drug therapy or CBT. The patients were made to feel sad: they listened to a piece of dreary classical music at half-speed and were asked to think about times in their life when they had been unhappy. They then filled out a questionnaire to measure negative thoughts. Those who had received drug therapy showed more negative thinking than those who had received CBT - they were also more likely to relapse over the next 18 months.