Inflammation (Slide 24-46) transfer 24–27 to features
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
23 Terms
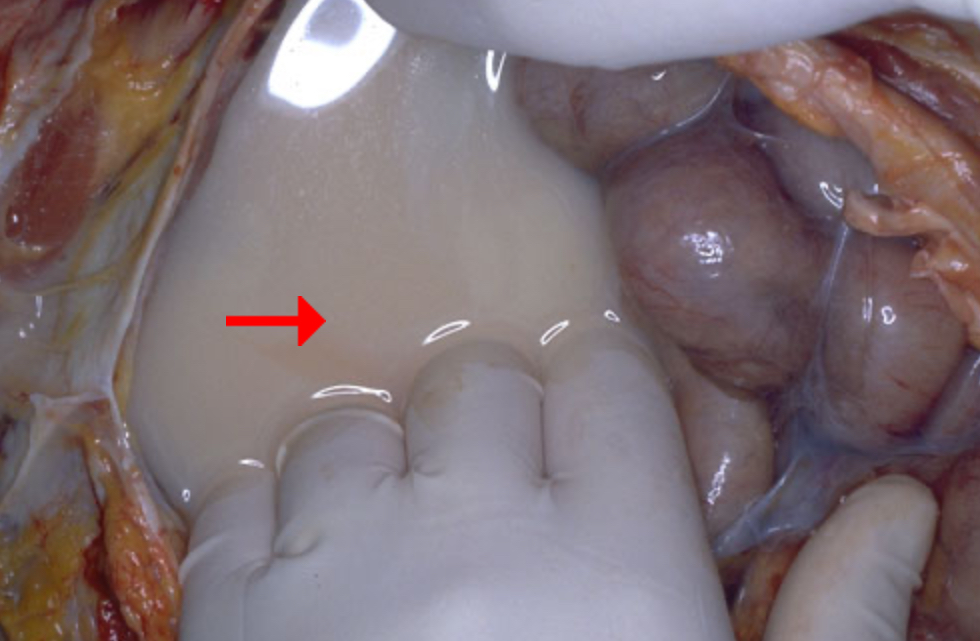
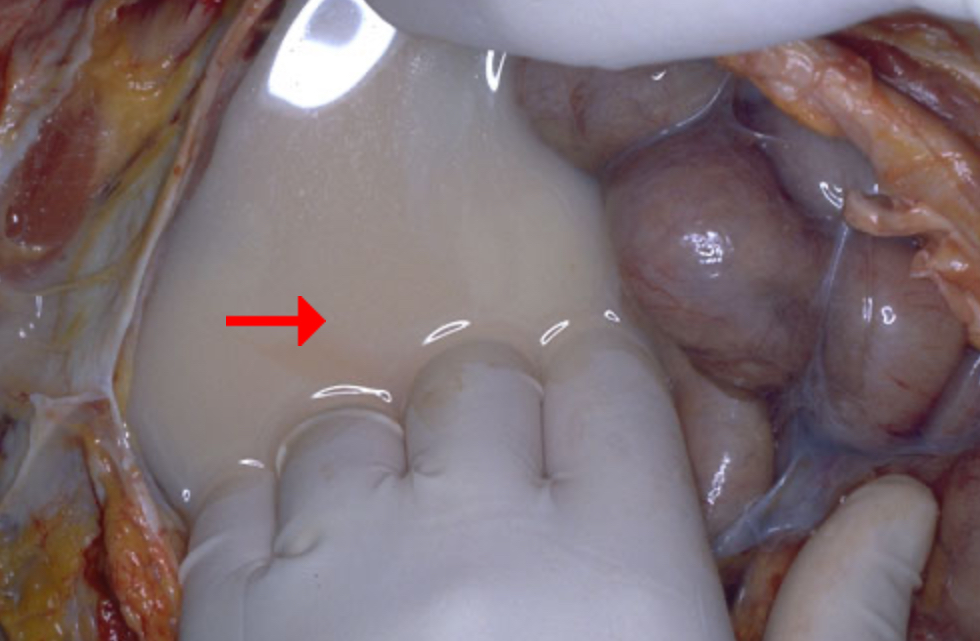
Milky white fluid in the peritoneal cavity indicates what?
Possible cause
Edema or effusion?
Chylous ascites (milky white due to presence of lipids)
Blockage of lymphatic drainage
Effusion
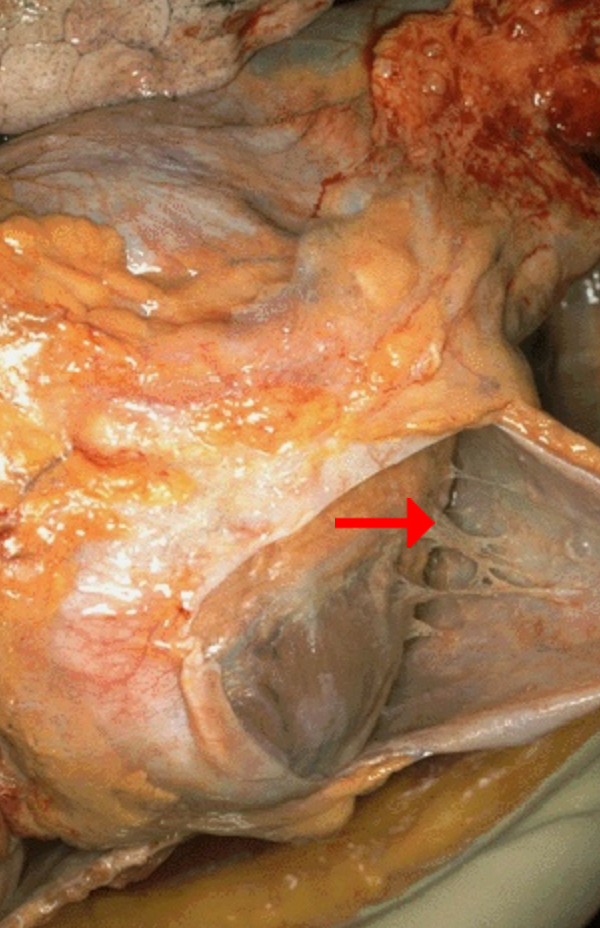
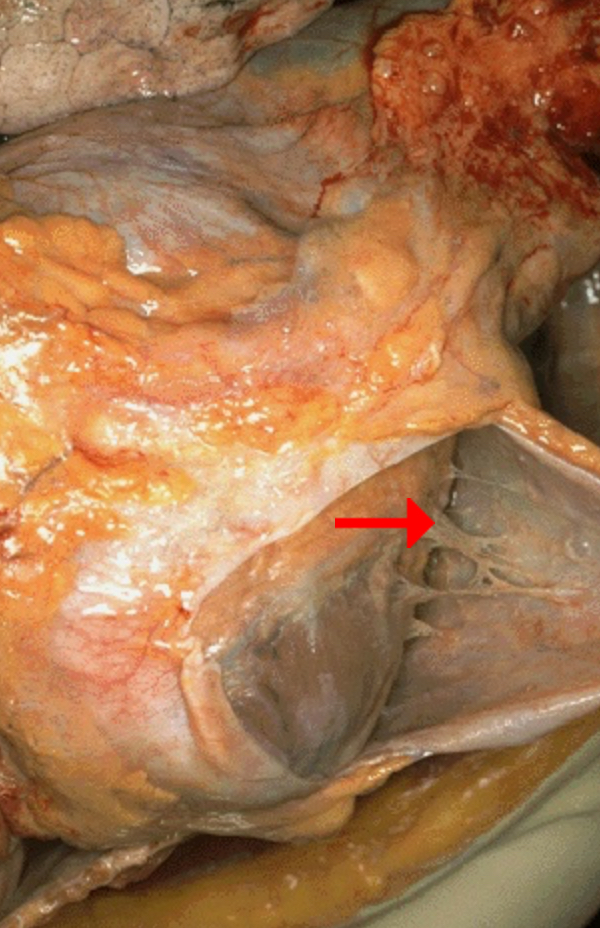
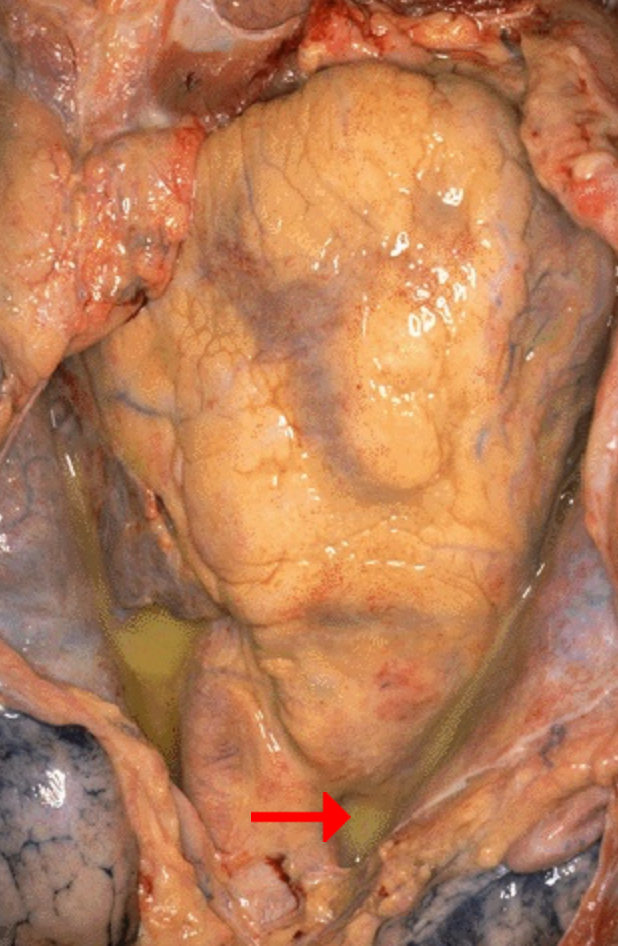
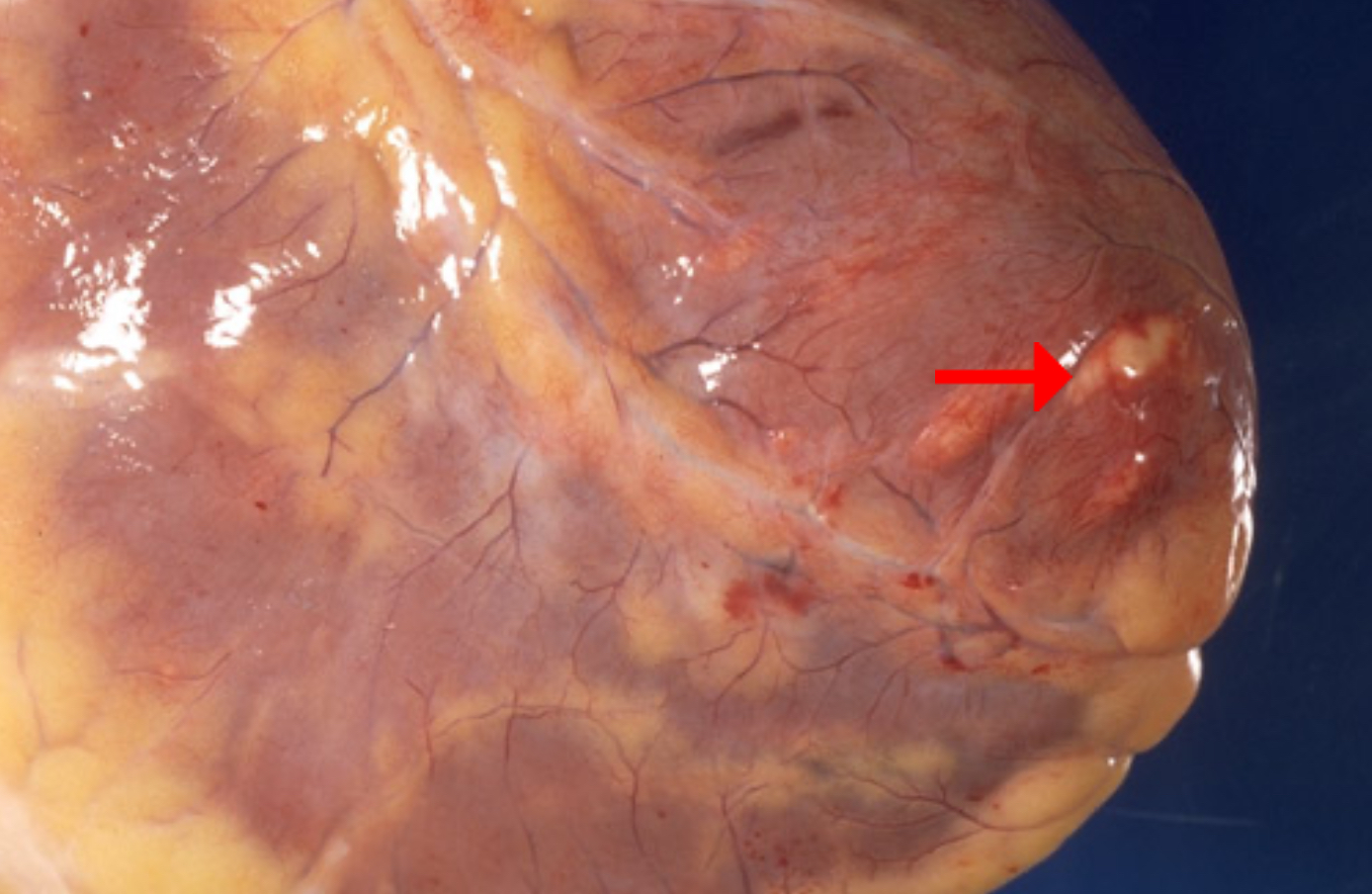
Identify morphologic pattern of acute inflammation
Identify main component of pointed structure
This is a result of edema or effusion?
Is the accumulated fluid transudate or exudate?
Fibrinous Inflammation
Fibrin
Effusion (in pericardial cavity)
Exudate (protein-rich)
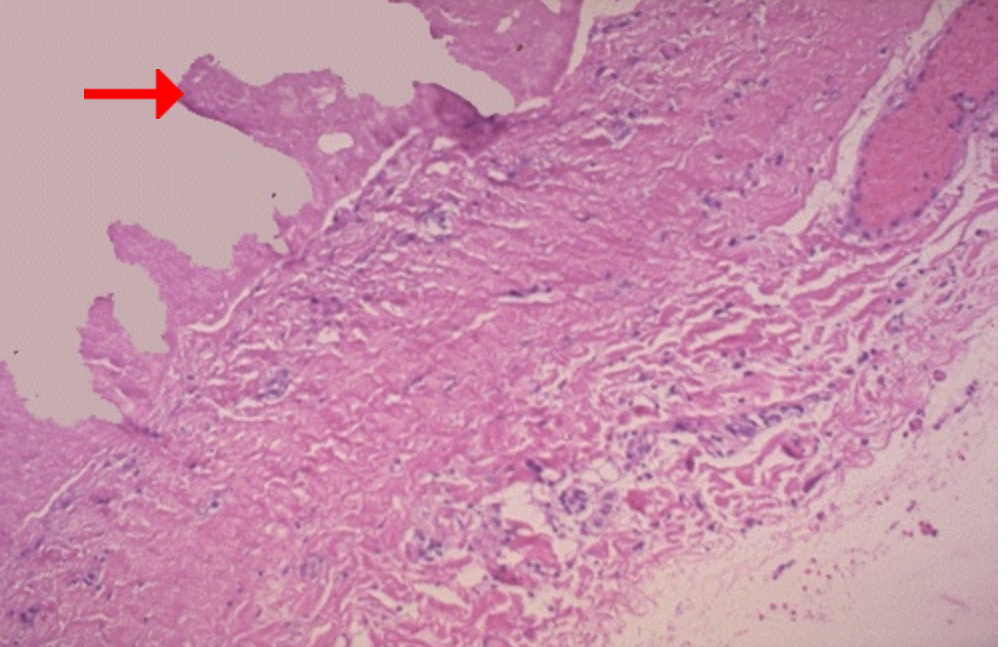
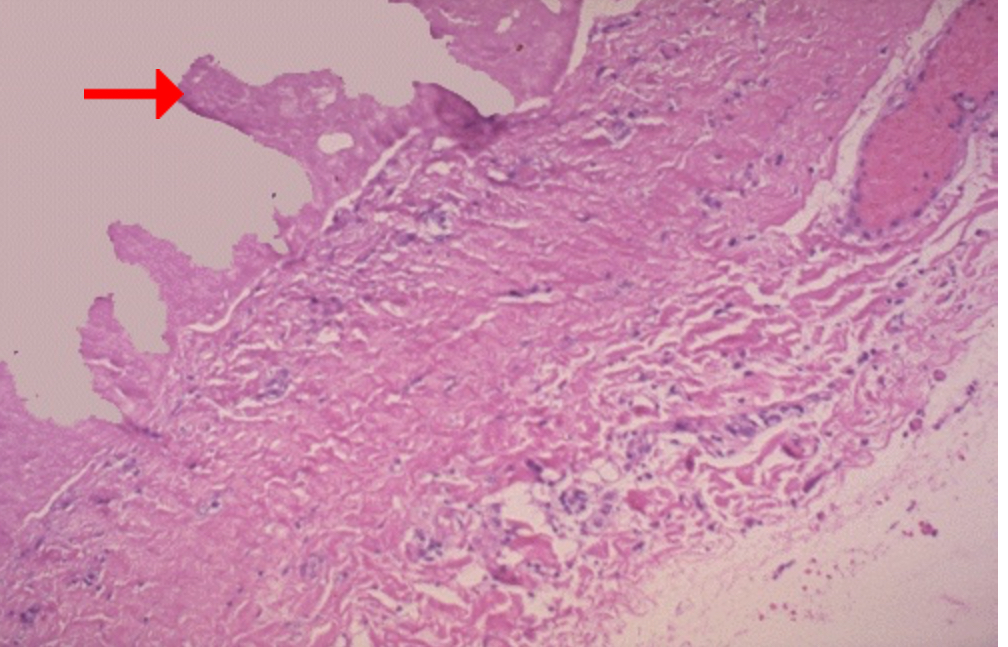
Identify pointed structure
Friction between such structures would produce what auscultatory finding?
Fibrin strand
Friction rub (creaking or scratching sound, sometimes described as rubbing sandpaper)

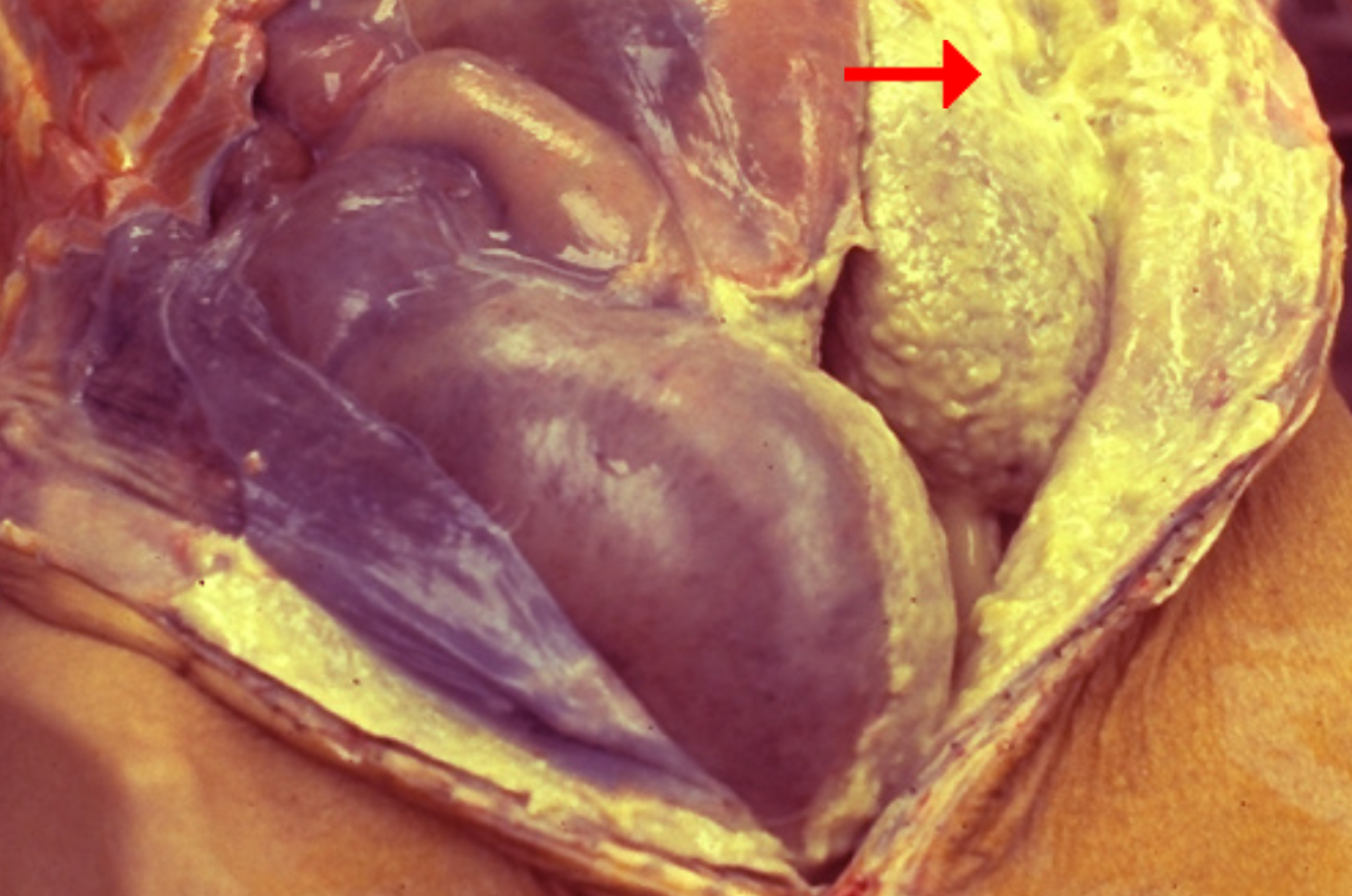
Predominant (dead) cells in the yellow-green exudate
Other components present in the exudate
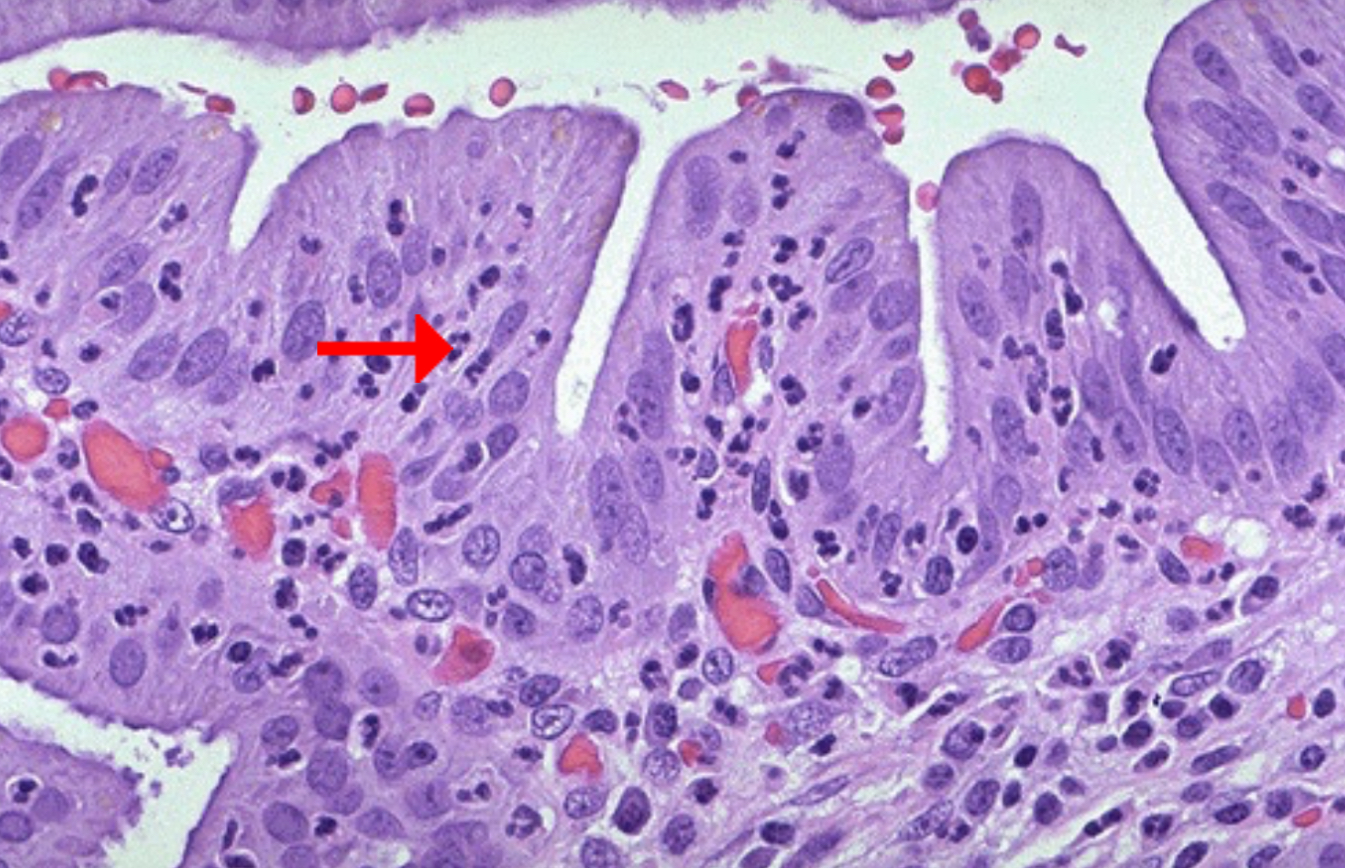
Condition: inflamed, hyperemic (erythematous) bowel mucosa
Neutrophils
Fibrin, amorphous debris of dying cells

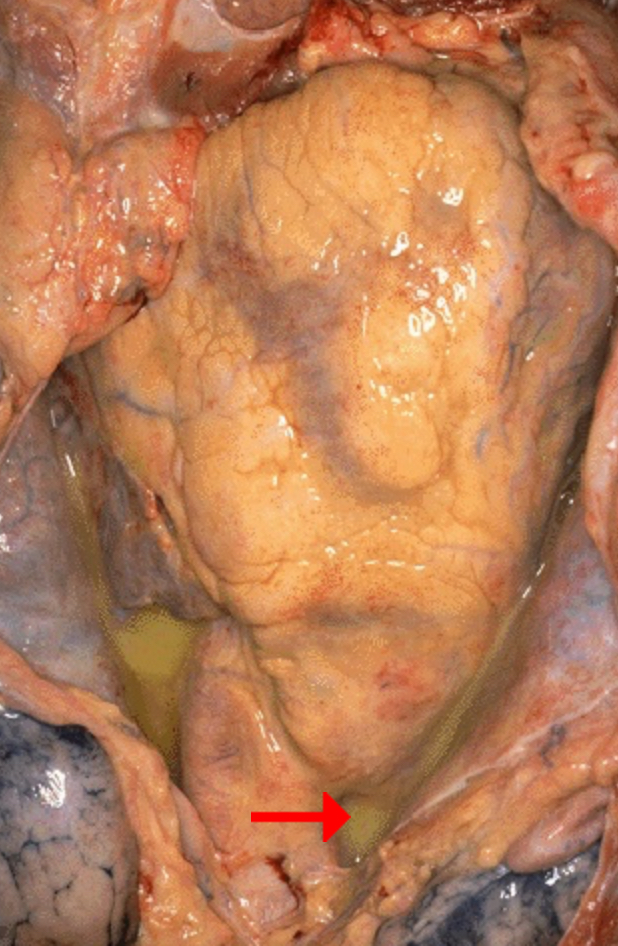
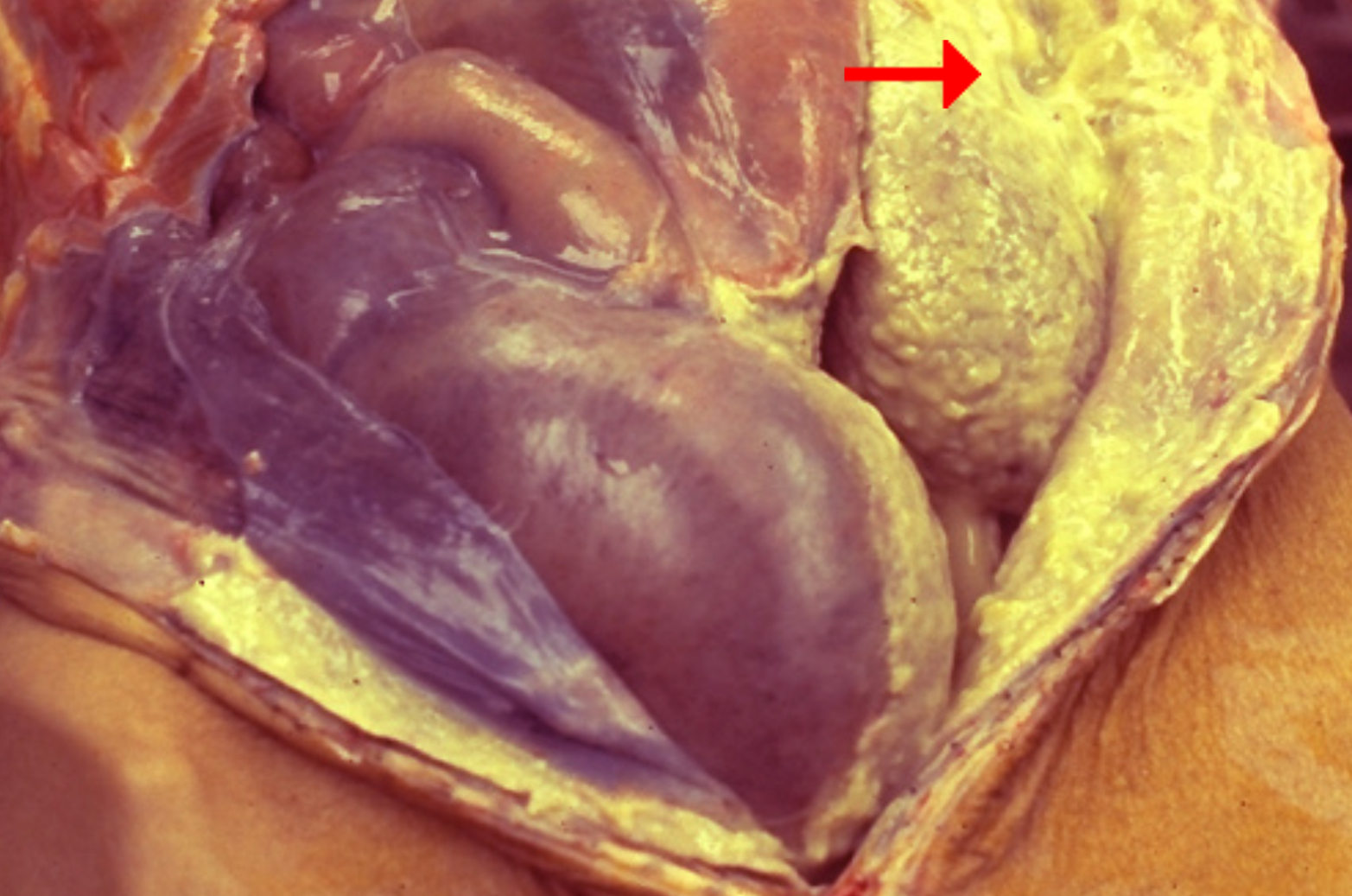
Identify morphologic pattern of acute inflammation
What could be the underlying cause of the disease leading to accumulation of the pointed yellowish fluid?
Condition: Purulent pericarditis
Purulent (Suppurative) Inflammation
Bacterial infection
Purulent pericarditis can have variable components of fibrinous exudate and serous effusion. If the inflammation is severe, it could even become hemorrhagic.
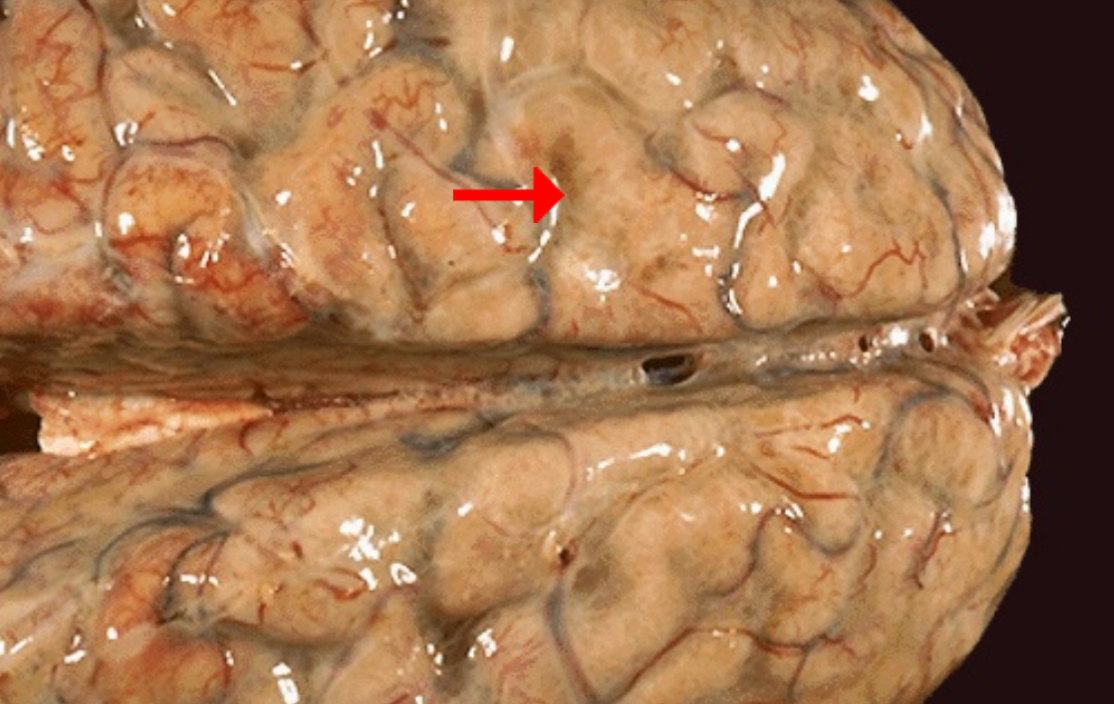
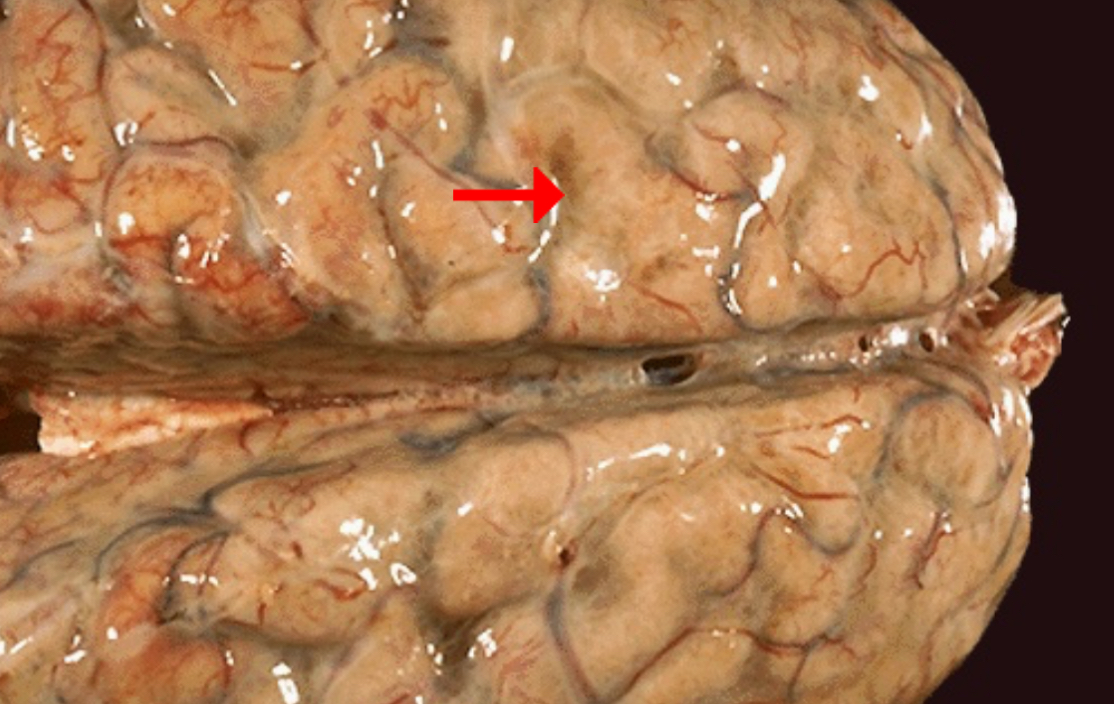
Identify morphologic pattern of acute inflammation
What could be the underlying cause of the disease leading to accumulation of the pointed fluid?
Possible effects on affected individual
Preponderant cell if CSF samples are obtained
Condition: Acute meningitis
Purulent (Suppurative) Inflammation
Bacterial infection (Streptococcus pneumoniae)
headache, nuchal rigidity, and changes in mental status
Neutrophils (with marked leukocytosis)
Identify morphologic pattern of acute inflammation
Preponderant cells in the exudate
Condition: Peritonitis
Purulent (Suppurative) Inflammation
PMNs
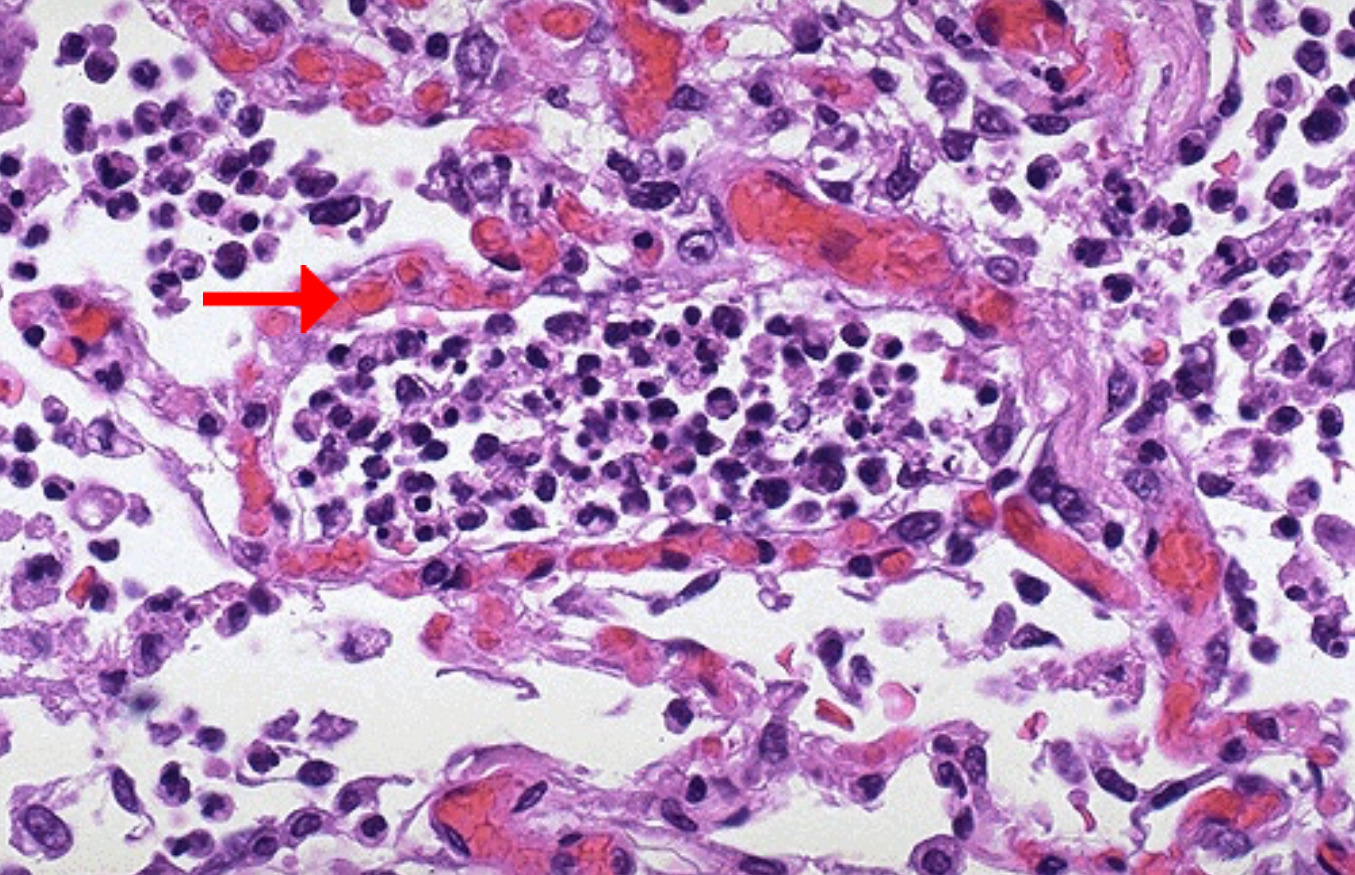
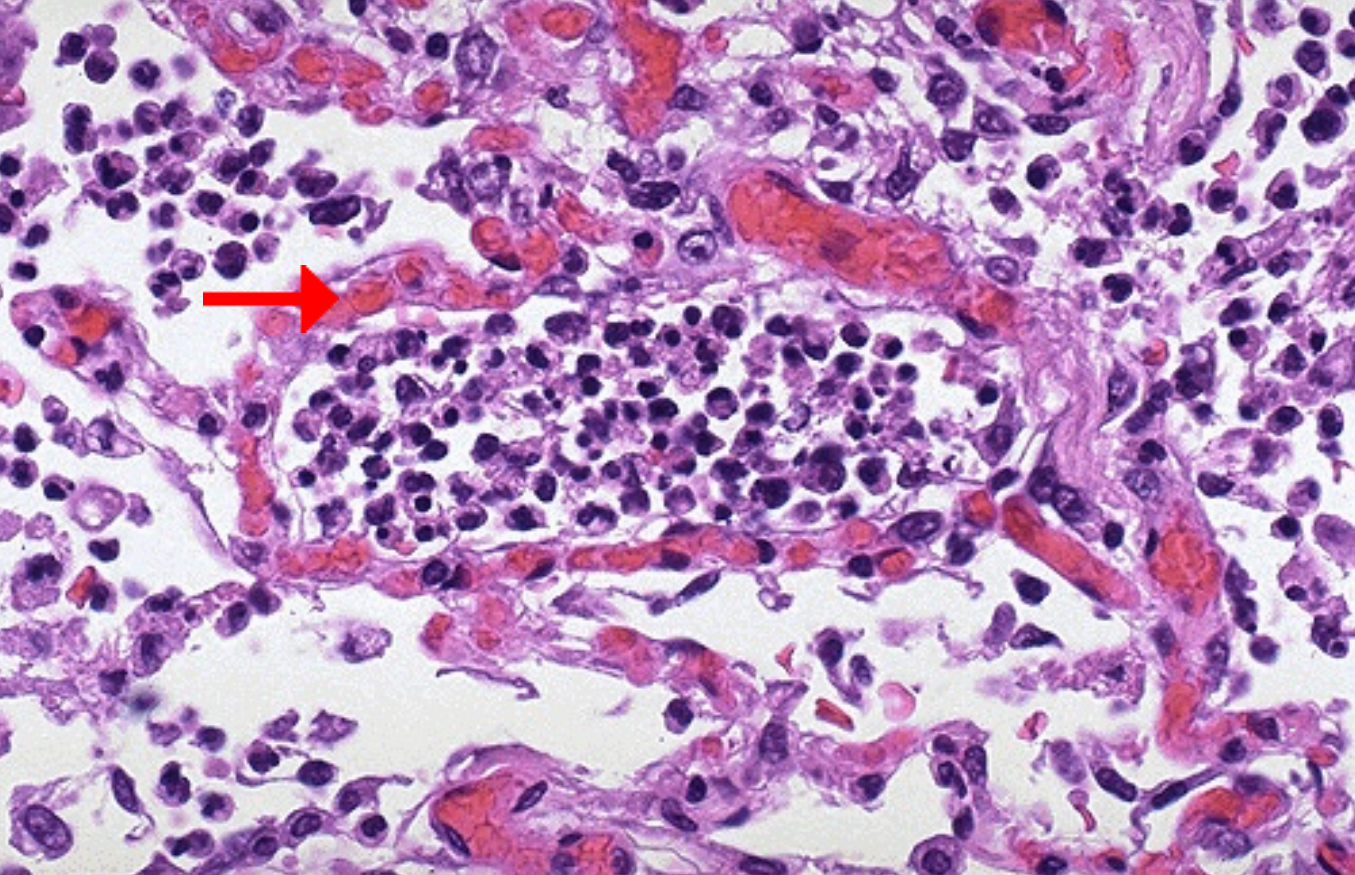
Predominant cell in the alveolar spaces
Describe the microscopic appearance of the surrounding blood vessels
Condition: Acute bronchopneumonia
Neutrophils
Dilated and congested with RBCs
This exudative process is typical for bacterial infection. The exudate gives rise to a productive cough of purulent yellow sputum. The alveolar architecture is still maintained, which is why even an extensive pneumonia often resolves with minimal residual destruction or damage to the pulmonary parenchyma.
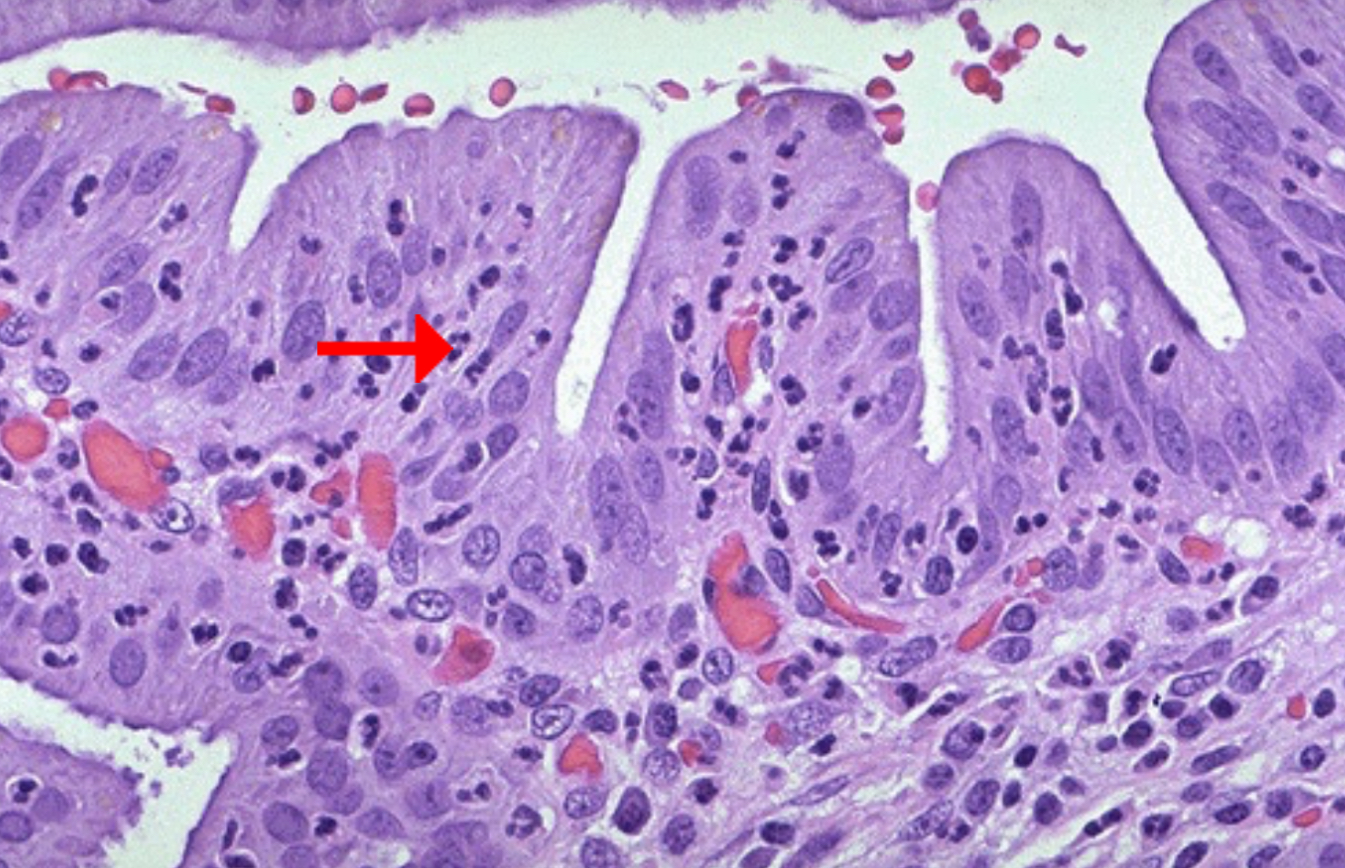
Identify pointed cell
Physical indicator of the condition on the affected individual
What may have been present within the gallbladder to elicit this inflammatory response?
Condition: Acute cholecystitis
Neutrophil
right upper quadrant abdominal pain with tenderness on palpation
Most cases of cholecystitis occur in association with cholelithiasis (gallstones).
Bacterial infection is typically absent from cases of acute and chronic cholecystitis.
Consequence of alveolar infiltration
Reduced oxygenation
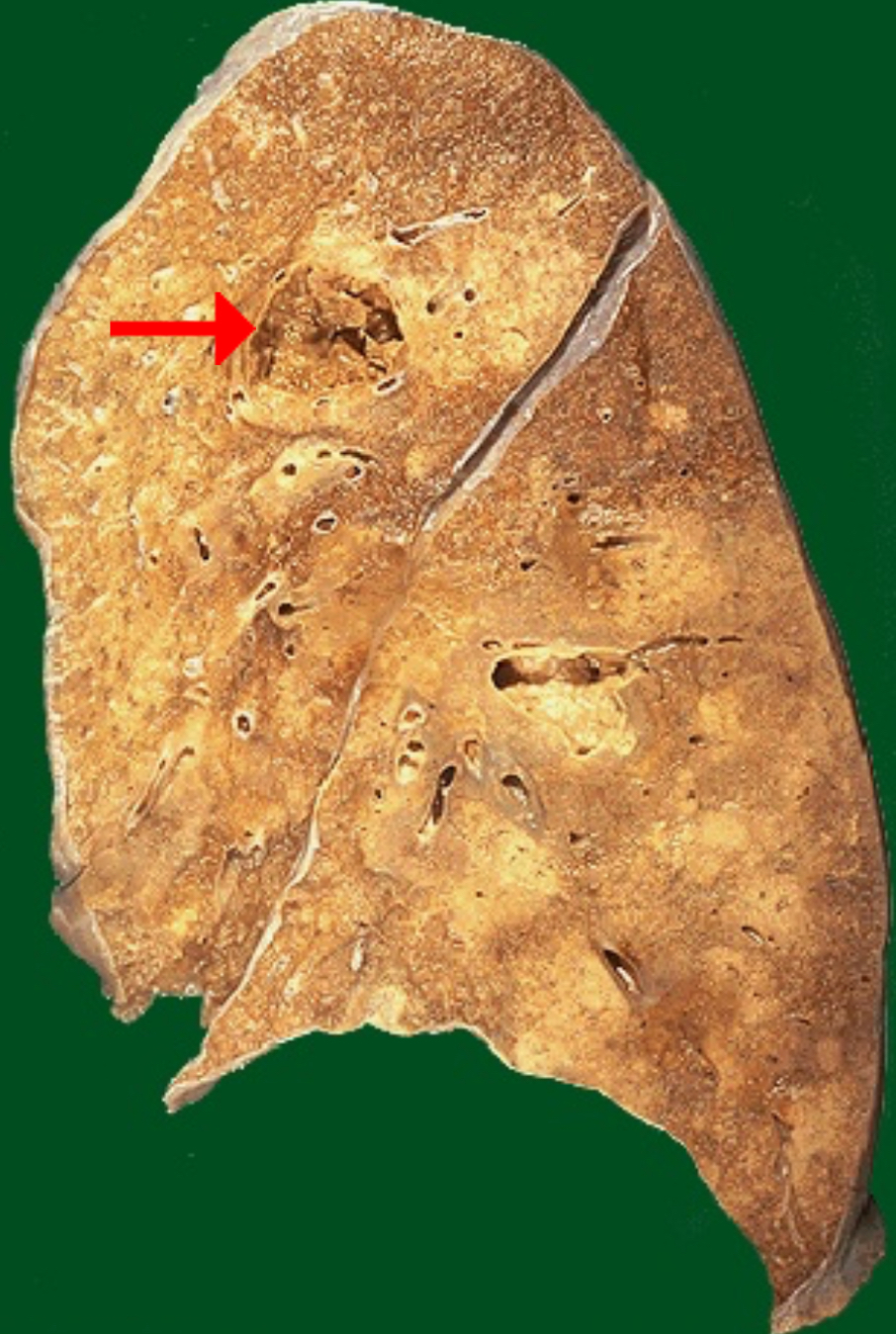
Identify morphologic pattern of acute inflammation
Abscess
Abscesses are localized collections of pus caused by suppuration buried in a tissue, an organ, or a confined space. They are produced by seeding of pyogenic bacteria into a tissue.
Which pattern of tissue necrosis is associated with abscesses?
Liquefactive necrosis
The liquefactive necrosis of an abscess is apparent, because the purulent contents are draining out to leave a cavity. On a chest radiograph, the liquefied central contents of an abscess can appear as an "air-fluid level".
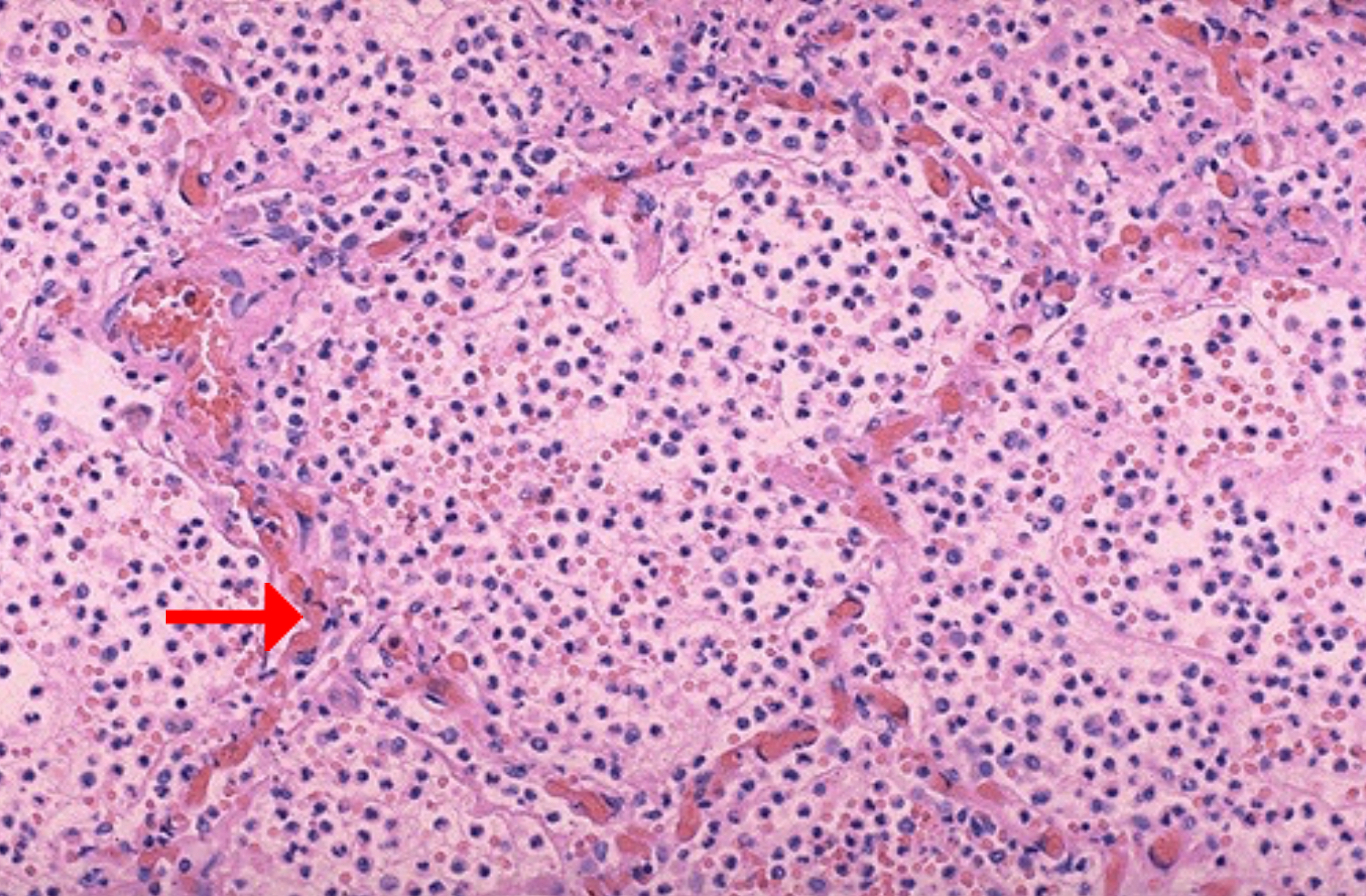
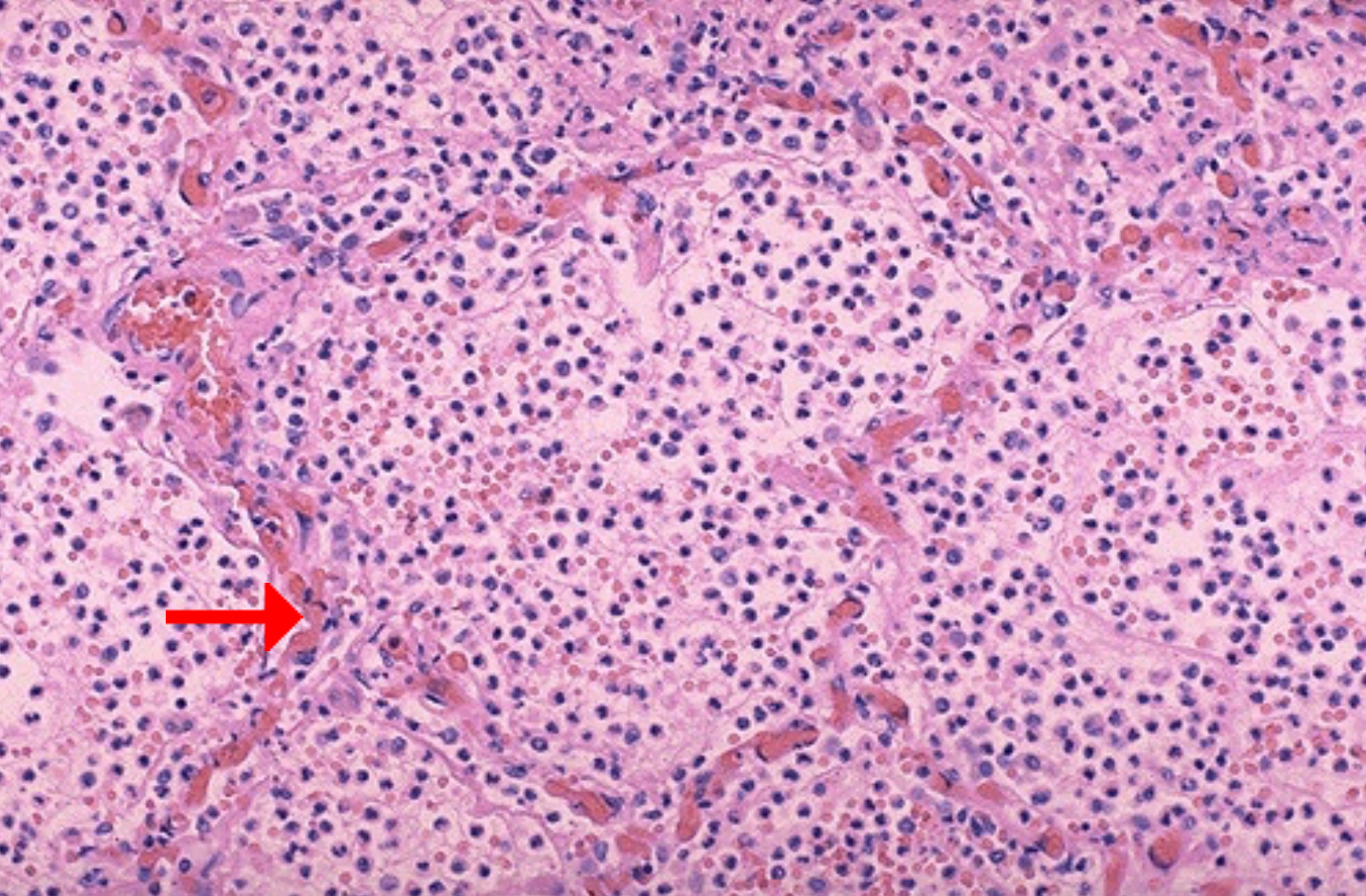
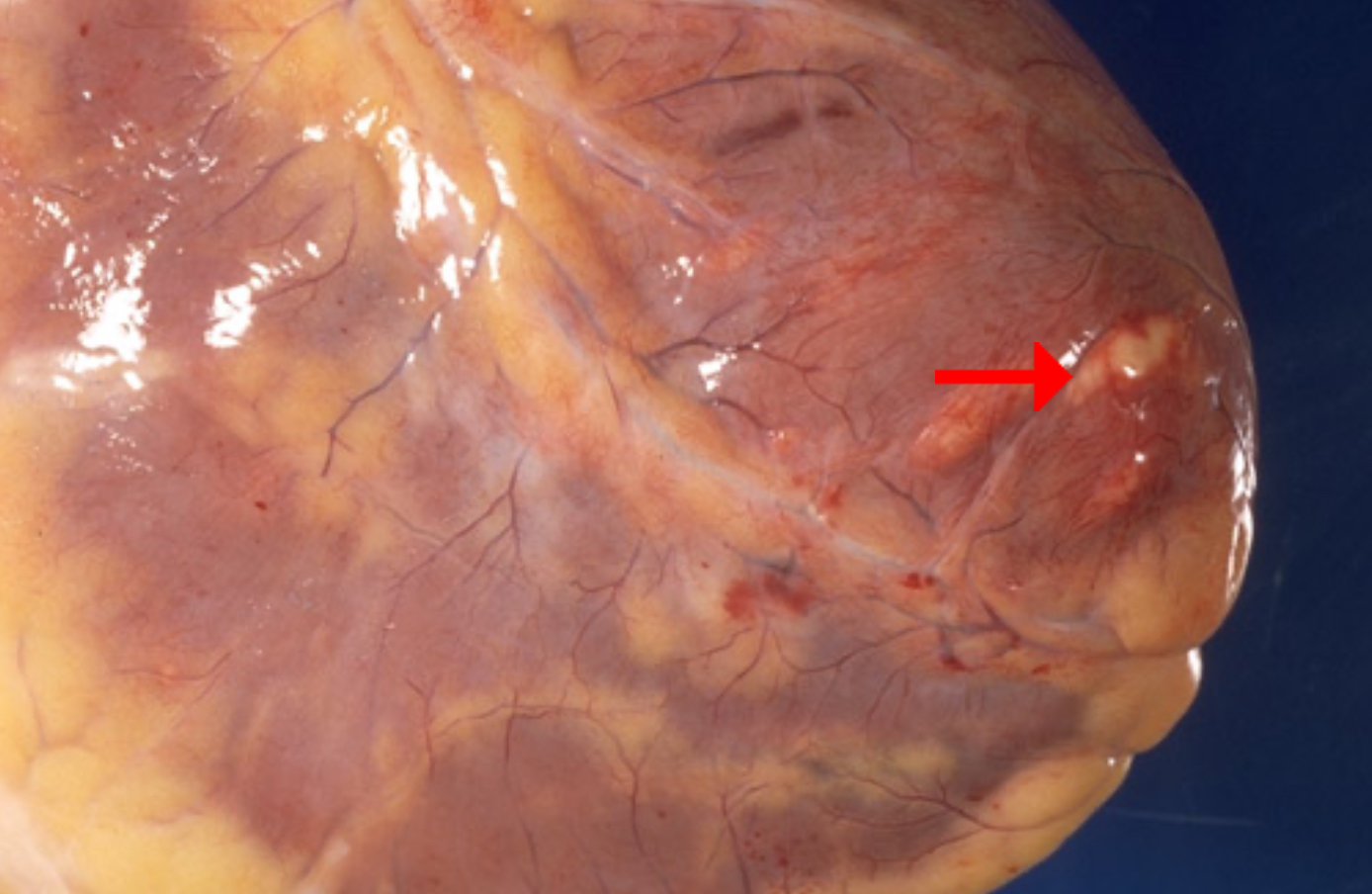
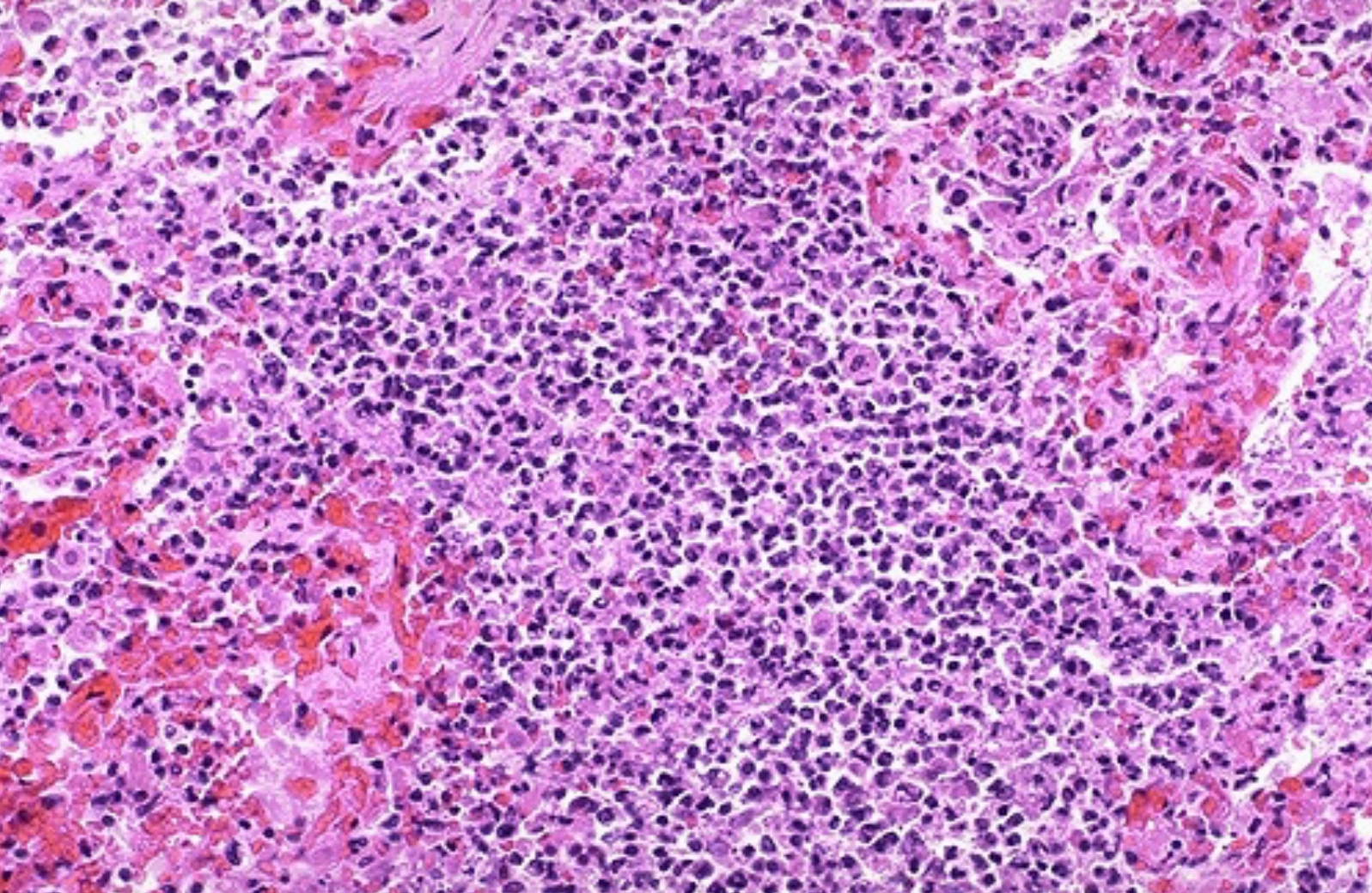
Identify morphologic pattern of acute inflammation
Possible adverse effects of myocarditis
Condition: Myocarditis
Abscess (specifically microabscess)
fever, chest pain, dyspnea from left-sided heart failure, and peripheral edema from right-sided heart failure; Arrhythmias
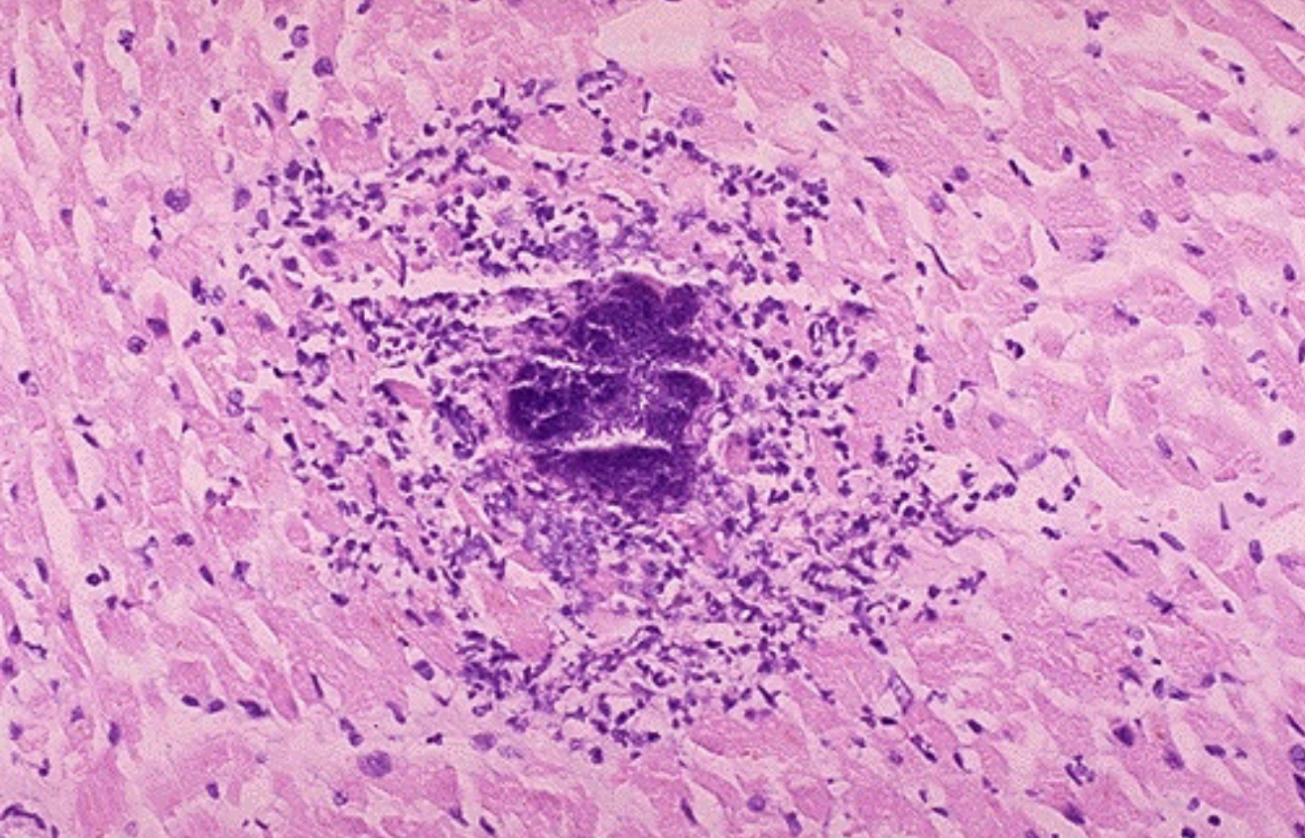
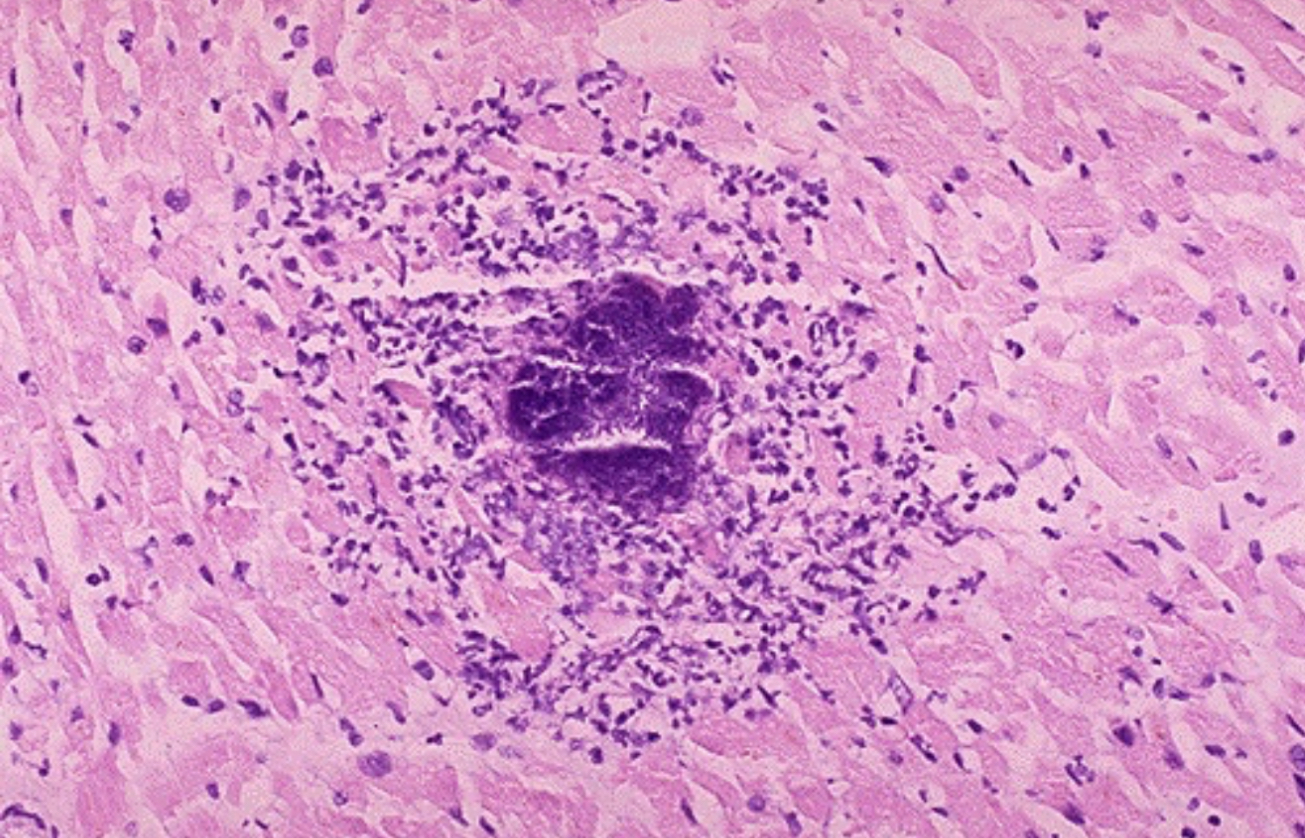
An abscess is a localized collection of what cells?
The irregular dark purple center is a collection of?
PMNs
bacterial debris

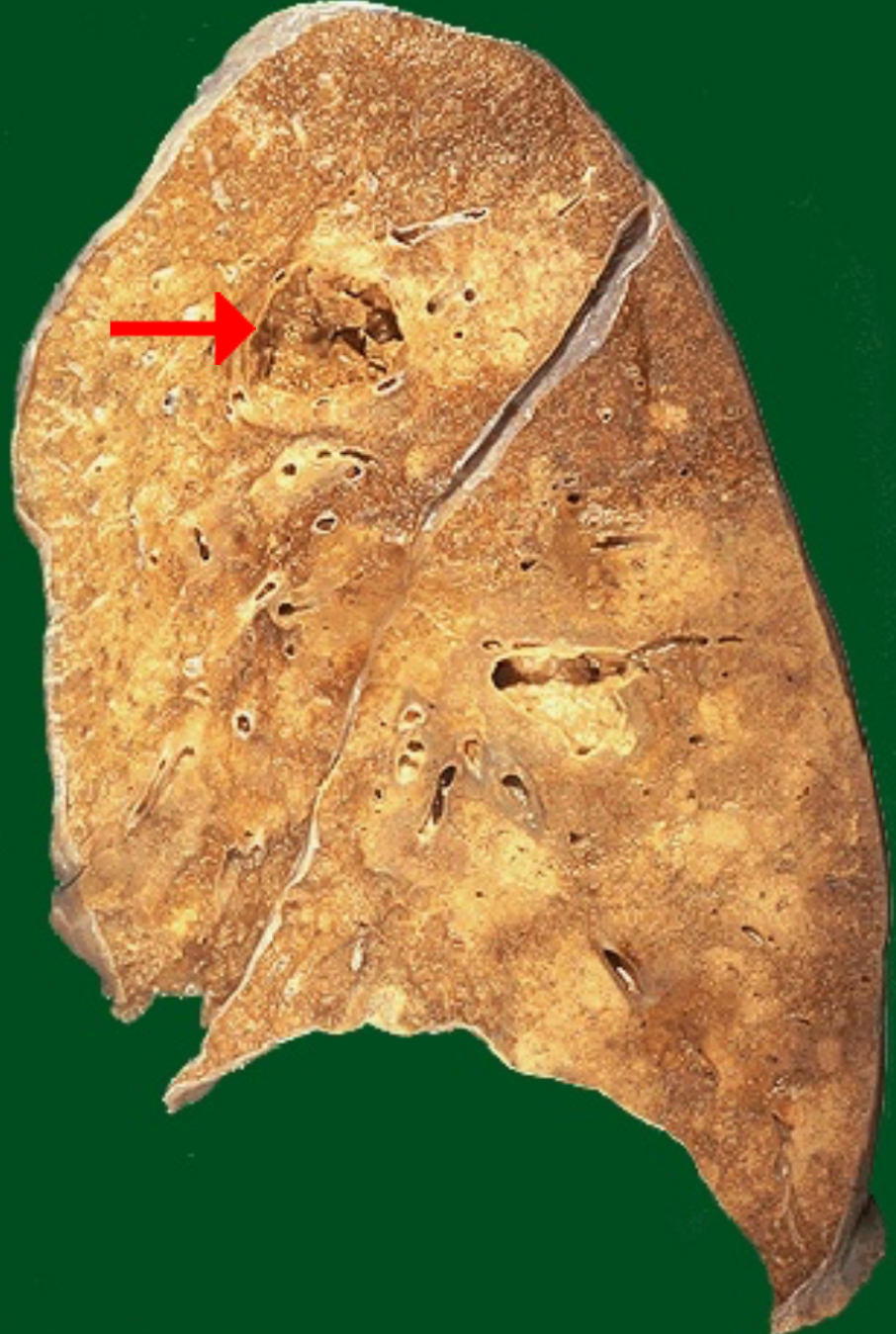
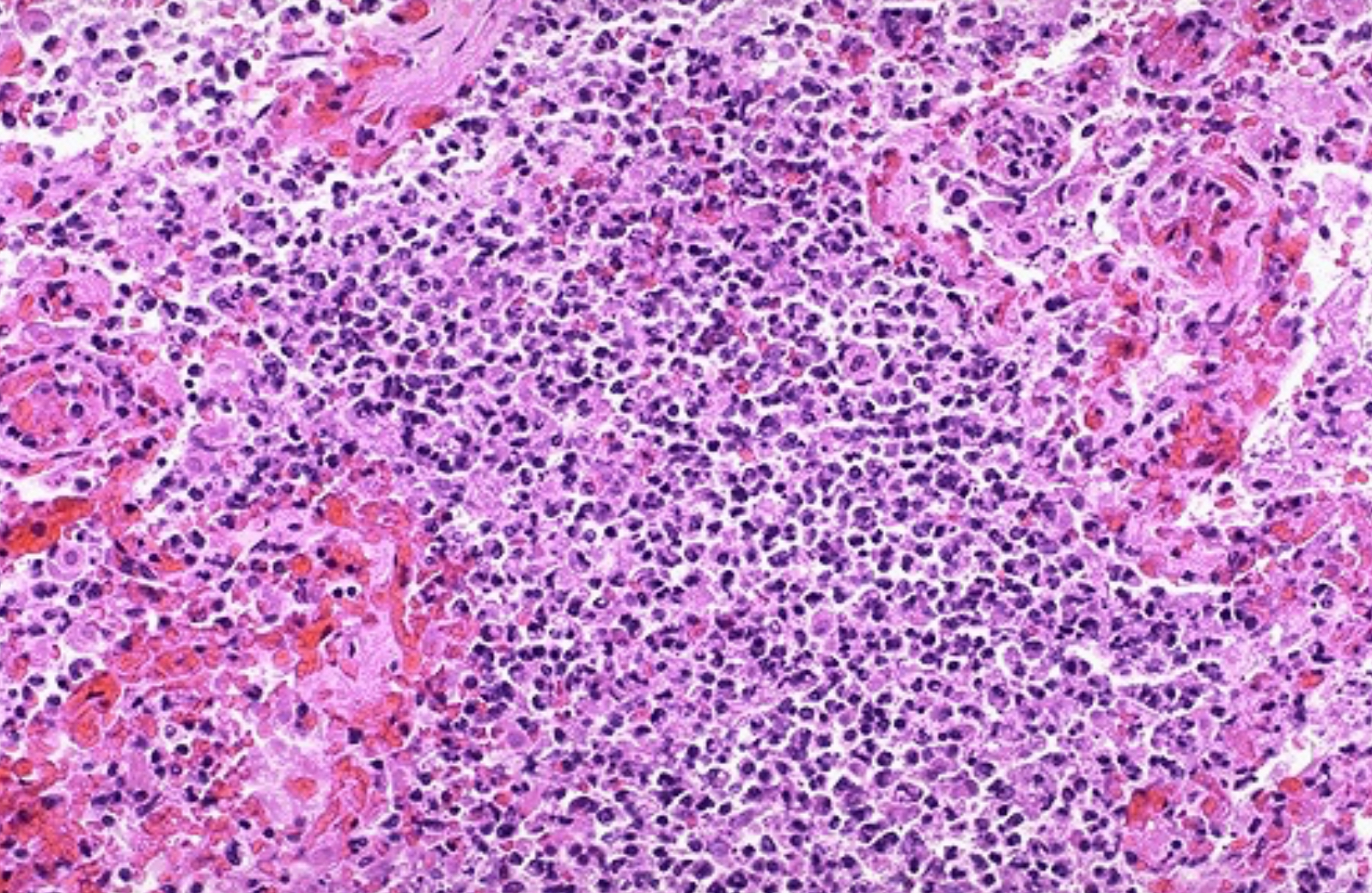
Identify morphologic pattern of acute inflammation
Preponderant cell in pointed area
Abscess
Neutrophils
A lung abscess is typically a complication of severe pneumonia, most often from virulent organisms such as Staphylococcus aureus, some pneumococci, and Klebsiella pneumoniae.

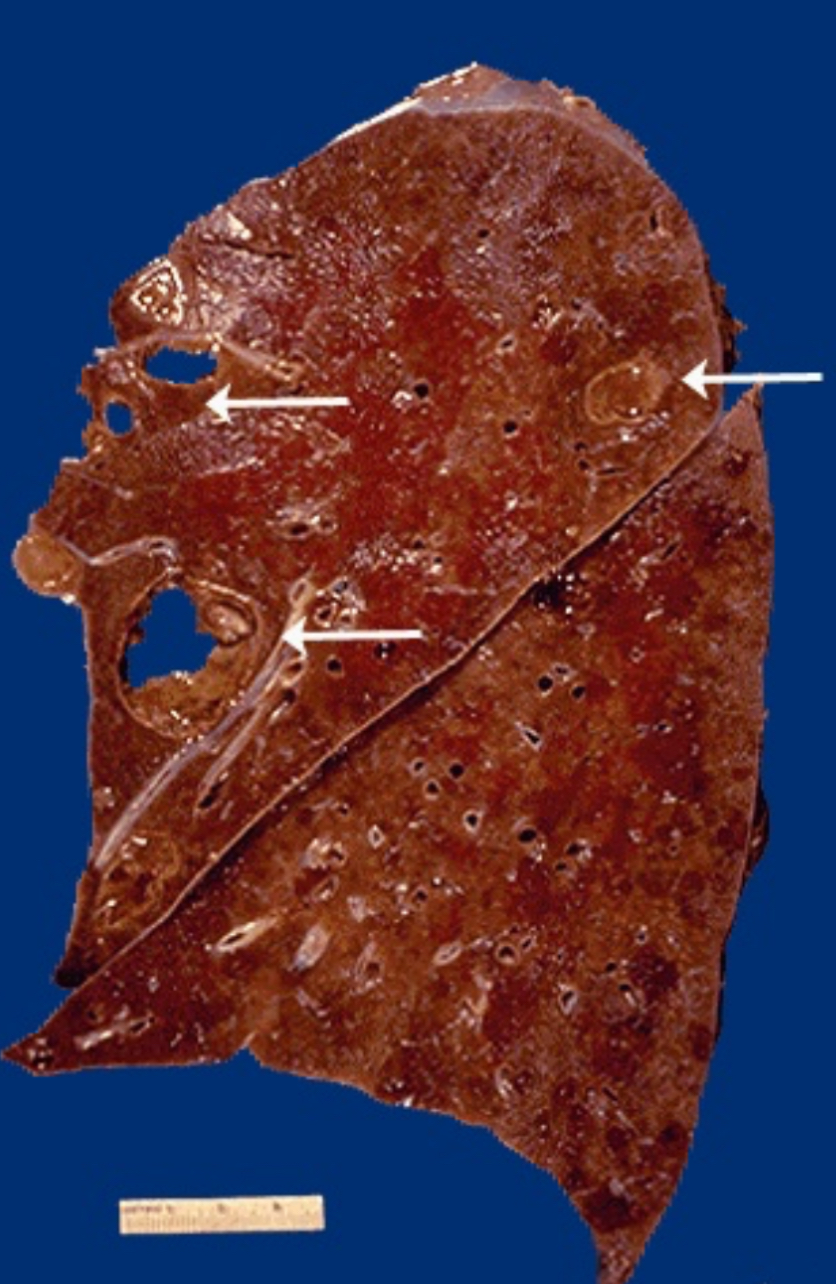
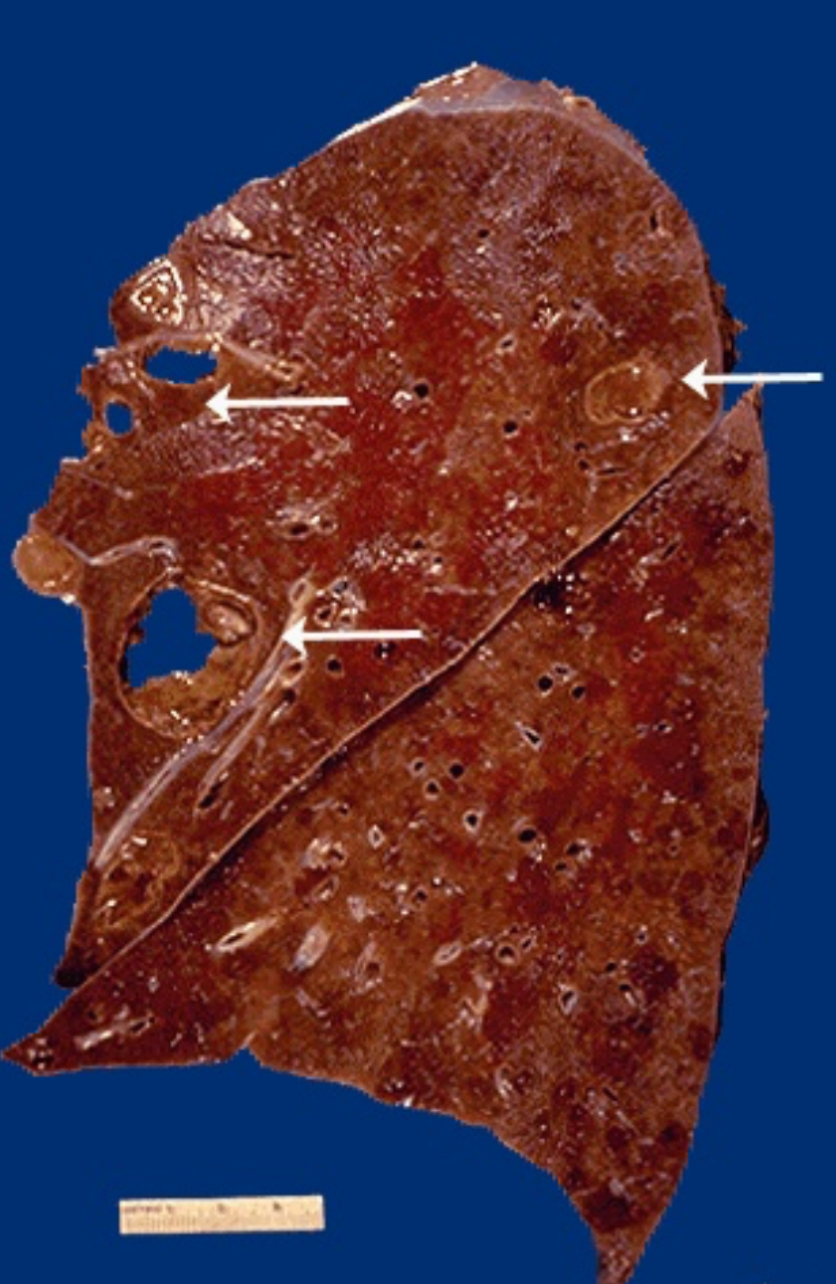
Identify morphologic pattern of acute inflammation
Describe microscopic appearance of affected region
Abscess
Alveolar walls are no longer visible; adjacent hemorrhage
More virulent bacterial organisms or more severe inflammation with pneumonia can be associated with destruction of lung tissue and hemorrhage.
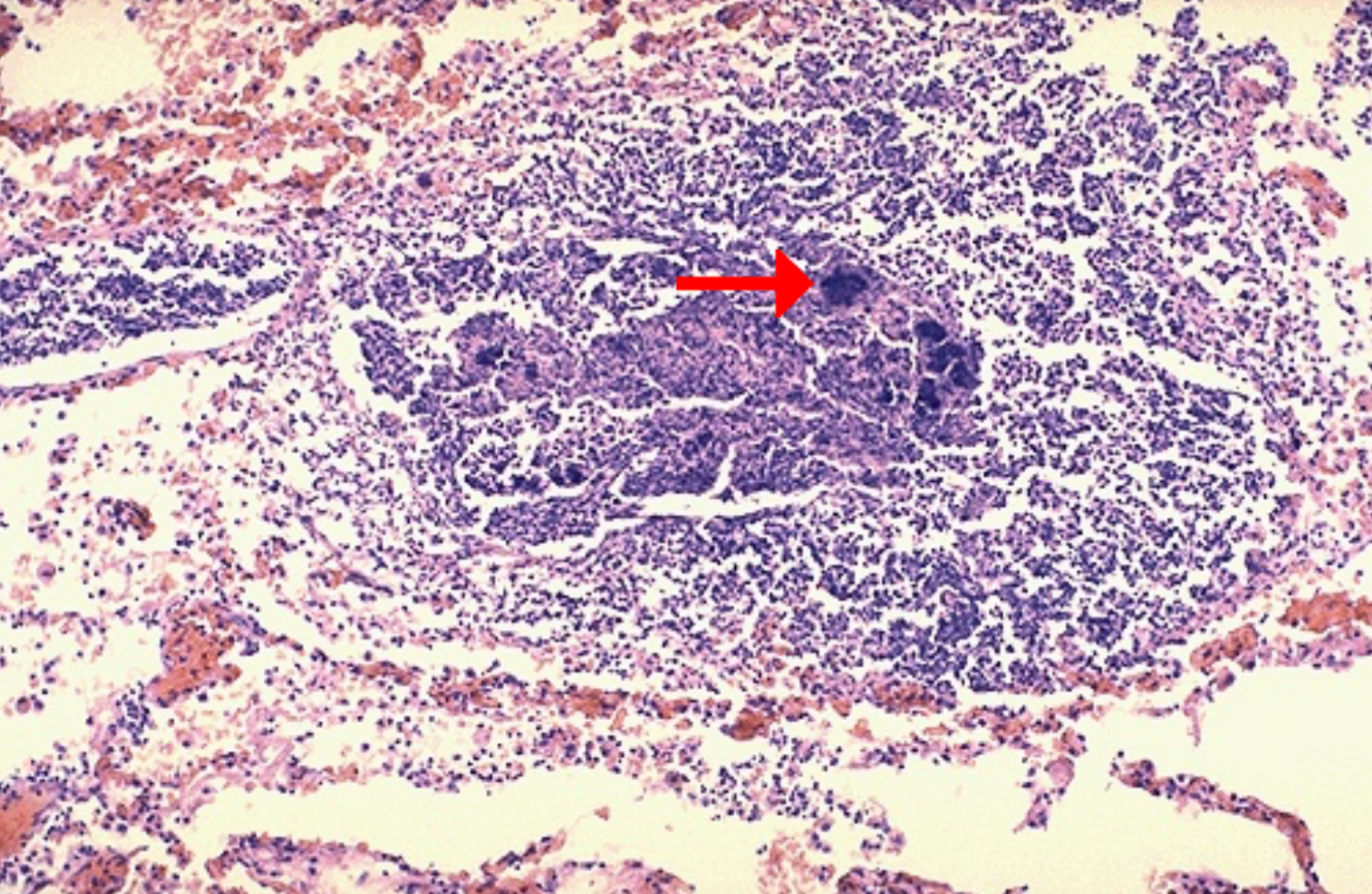
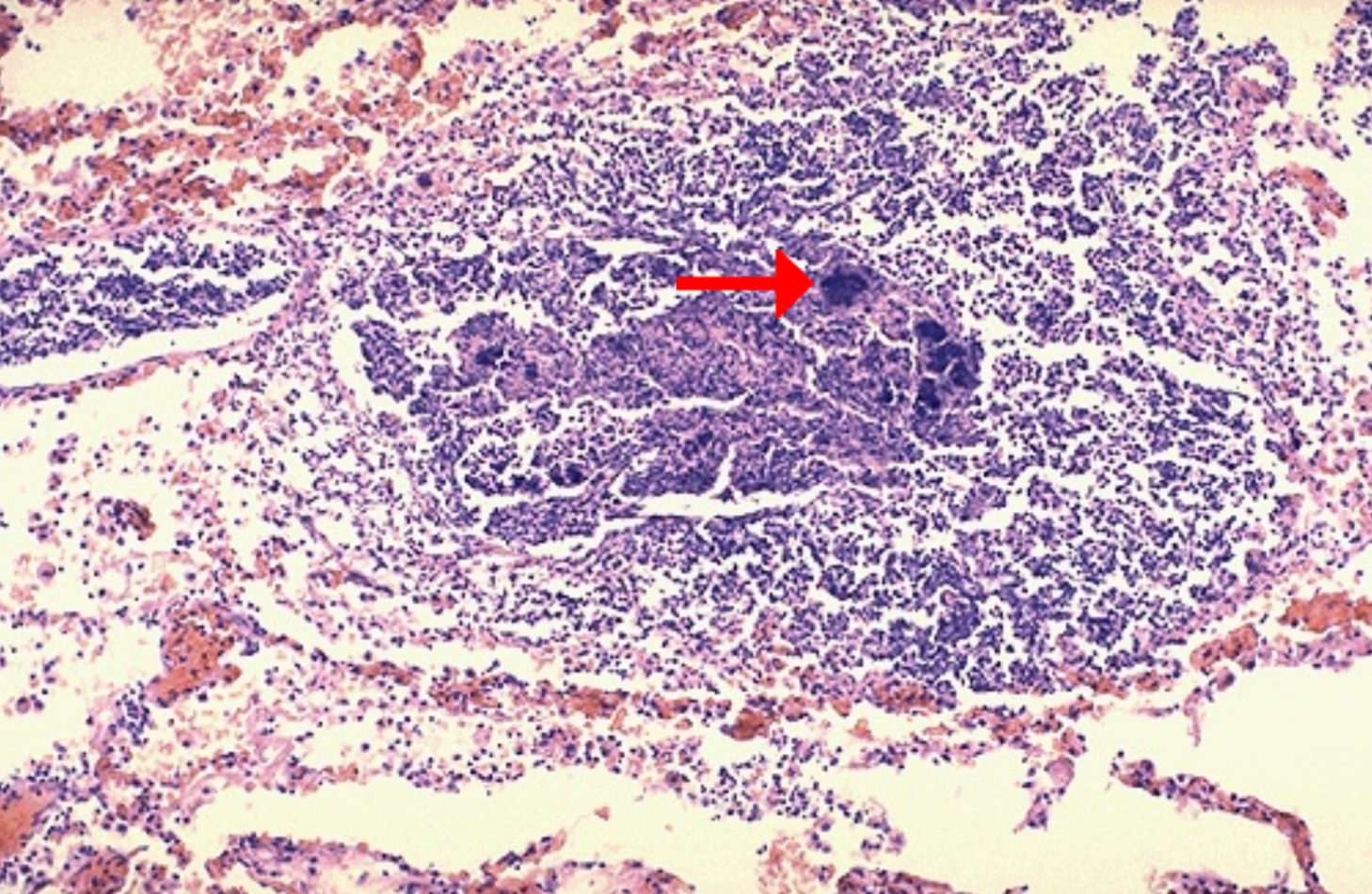
Identify morphologic pattern of acute inflammation
Pointed structure is a collection of?
Abscess
Fuzzy dark purple areas represent clusters of bacterial colonies
The alveoli in that area have been destroyed.

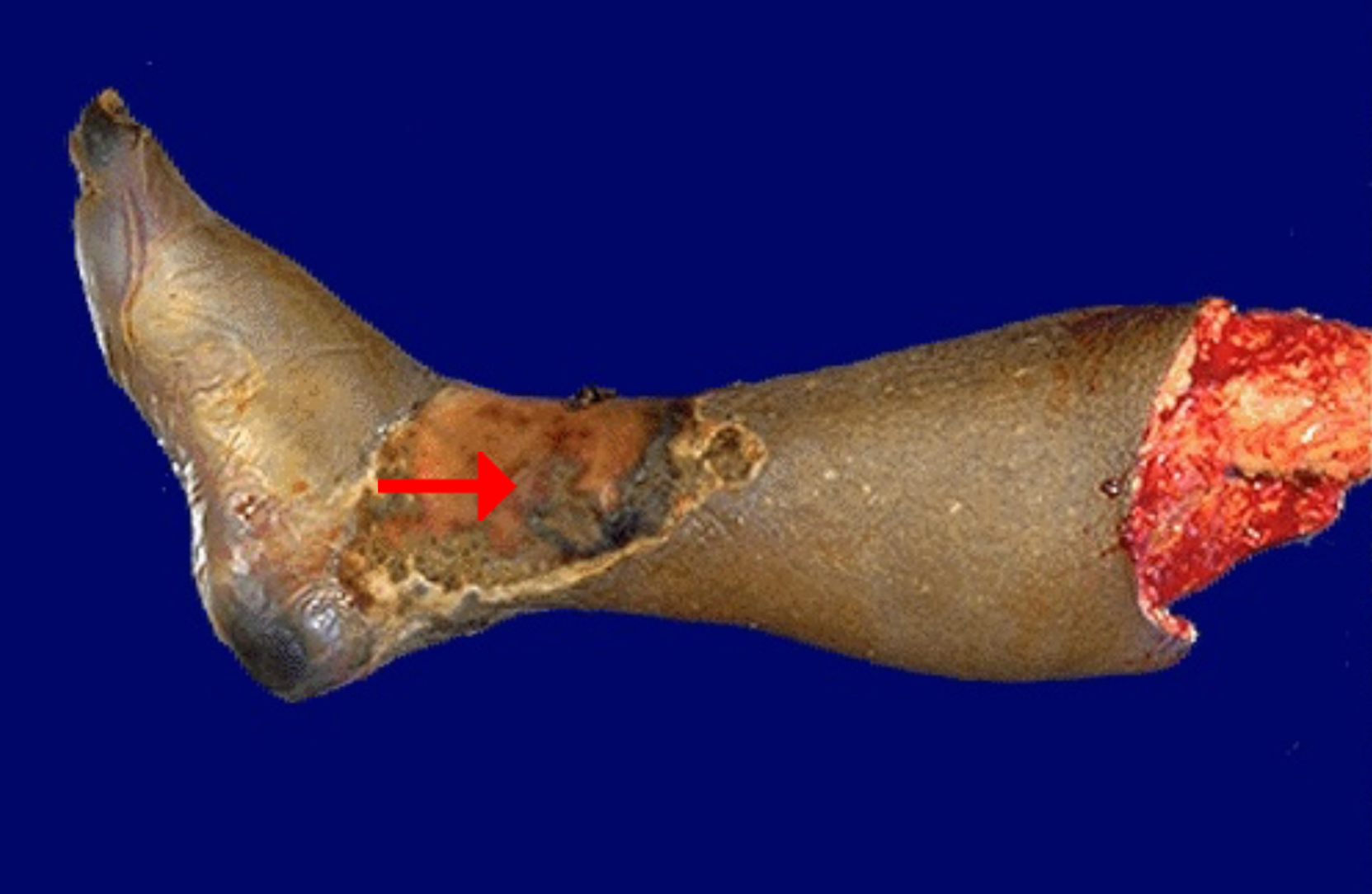
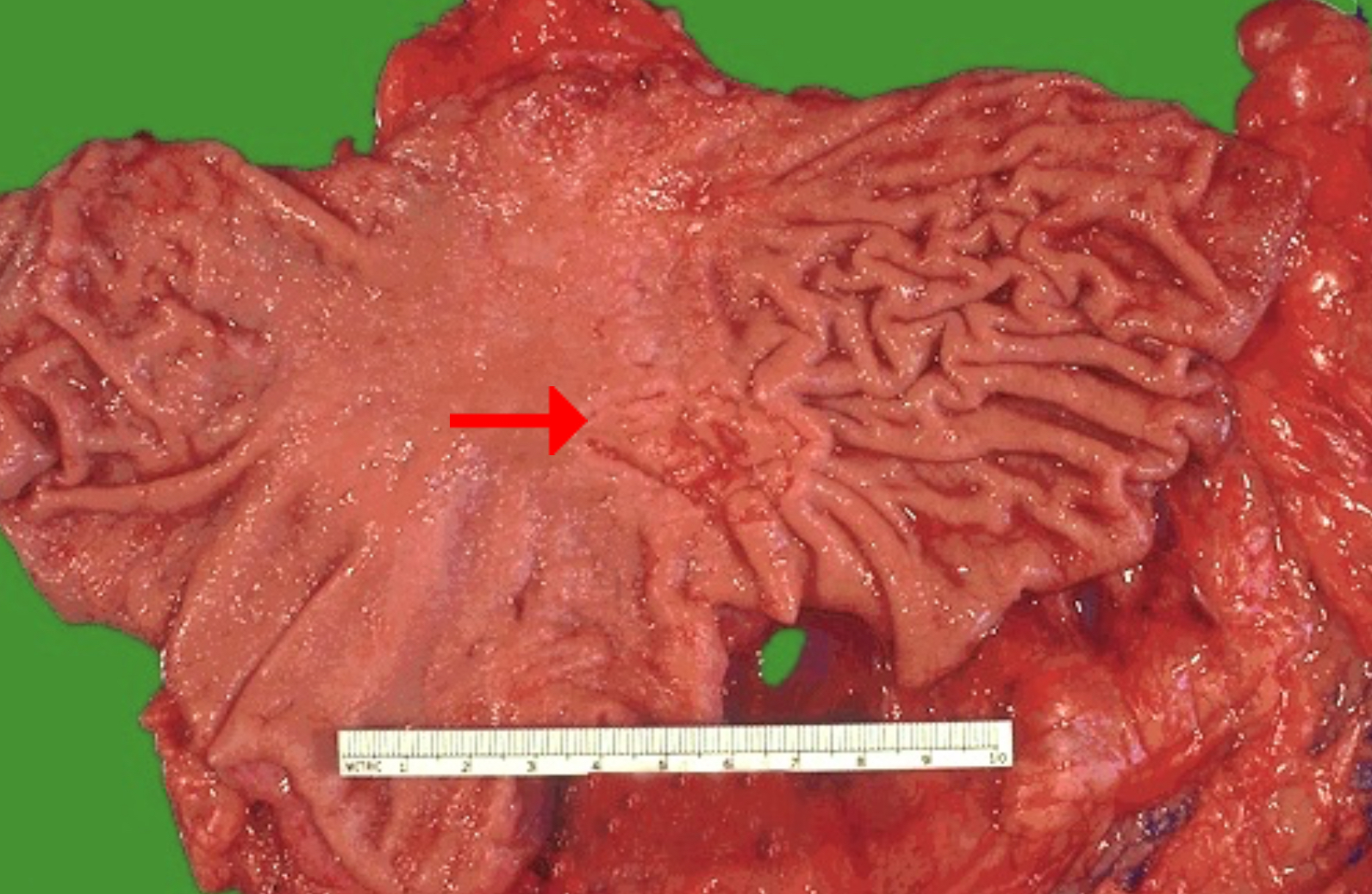
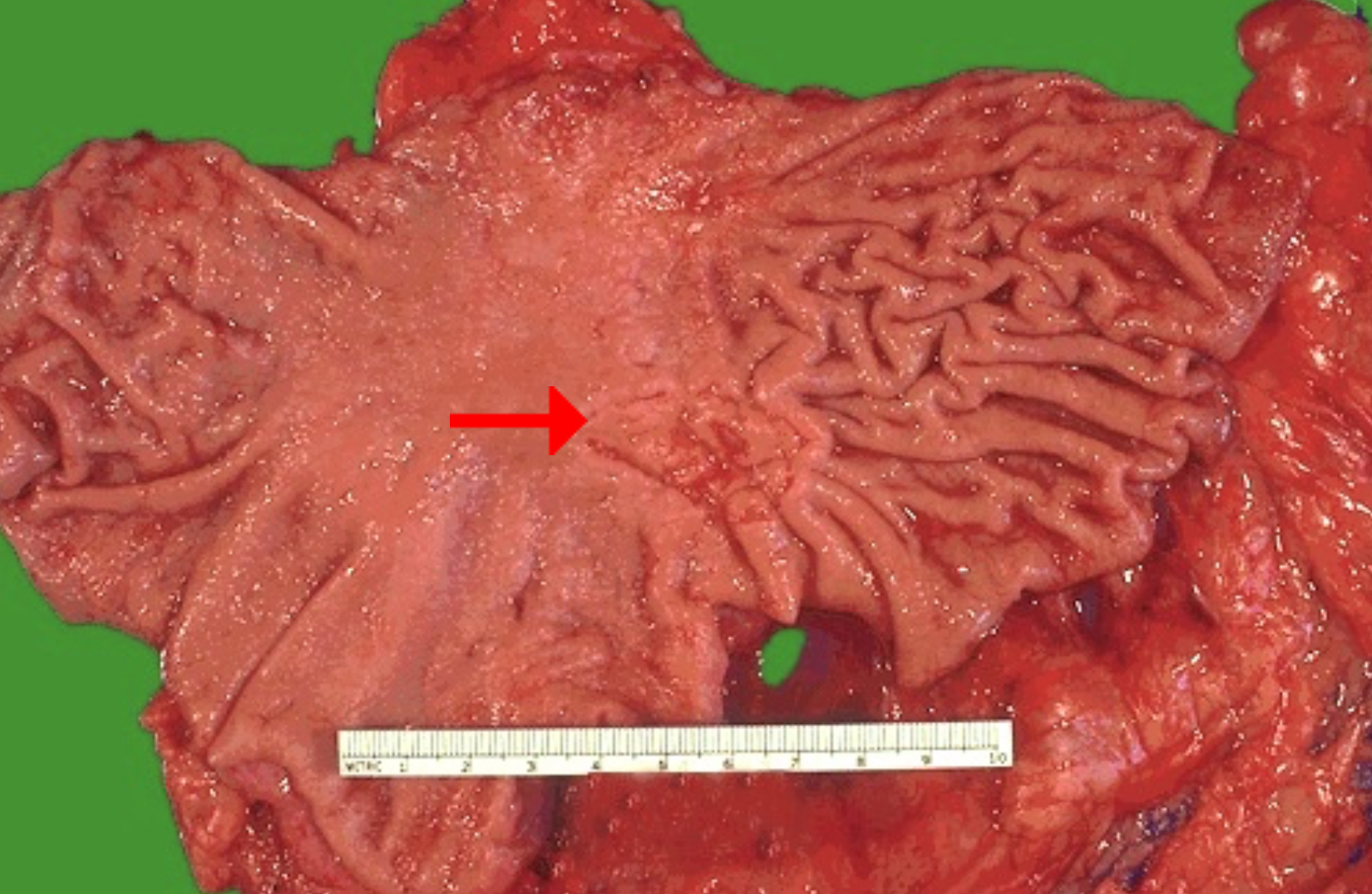
Identify morphologic pattern of acute inflammation
Possible adverse effects of the pointed defect
Possible causes
Condition: Acute gastric ulcer
Ulcer
hemorrhage, penetration (extension into an adjacent organ), perforation (communication with the peritoneal cavity), and stricture (as a result of scarring)
Helicobacter pylori infection; NSAIDs
An ulcer is an area of full-thickness loss of the mucosa (an erosion is a partial-thickness loss).

Identify morphologic pattern of acute inflammation
Most accurate procedure to determine malignancy
Ulcer
Biopsy
All gastric ulcers and all gastric masses must undergo biopsy because it is impossible to determine malignancy from their gross appearance. In contrast, virtually all duodenal peptic ulcers are benign.
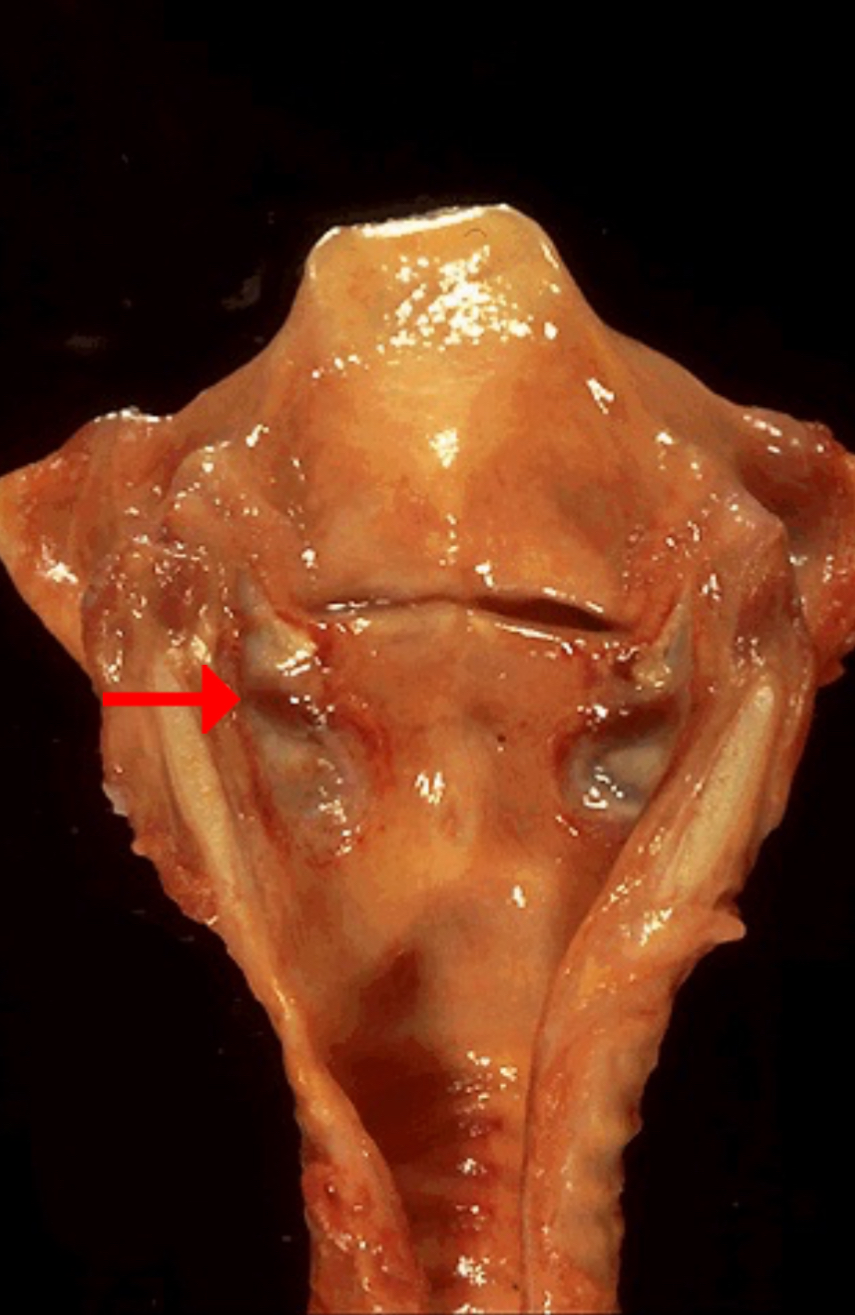
Identify morphologic pattern of acute inflammation
Term for ulcers that form on skin over bony prominences in persons who are bedridden for an extended time
Ulcer (caused by mechanical forces)
"pressure ulcers" or "decubitus ulcers"
According to webpath, this is an ulcer. But, Robbins Atlas says that this is a case of laryngeal erosion. An ulcer is an area of full-thickness loss of the mucosa (an erosion is a partial-thickness loss).

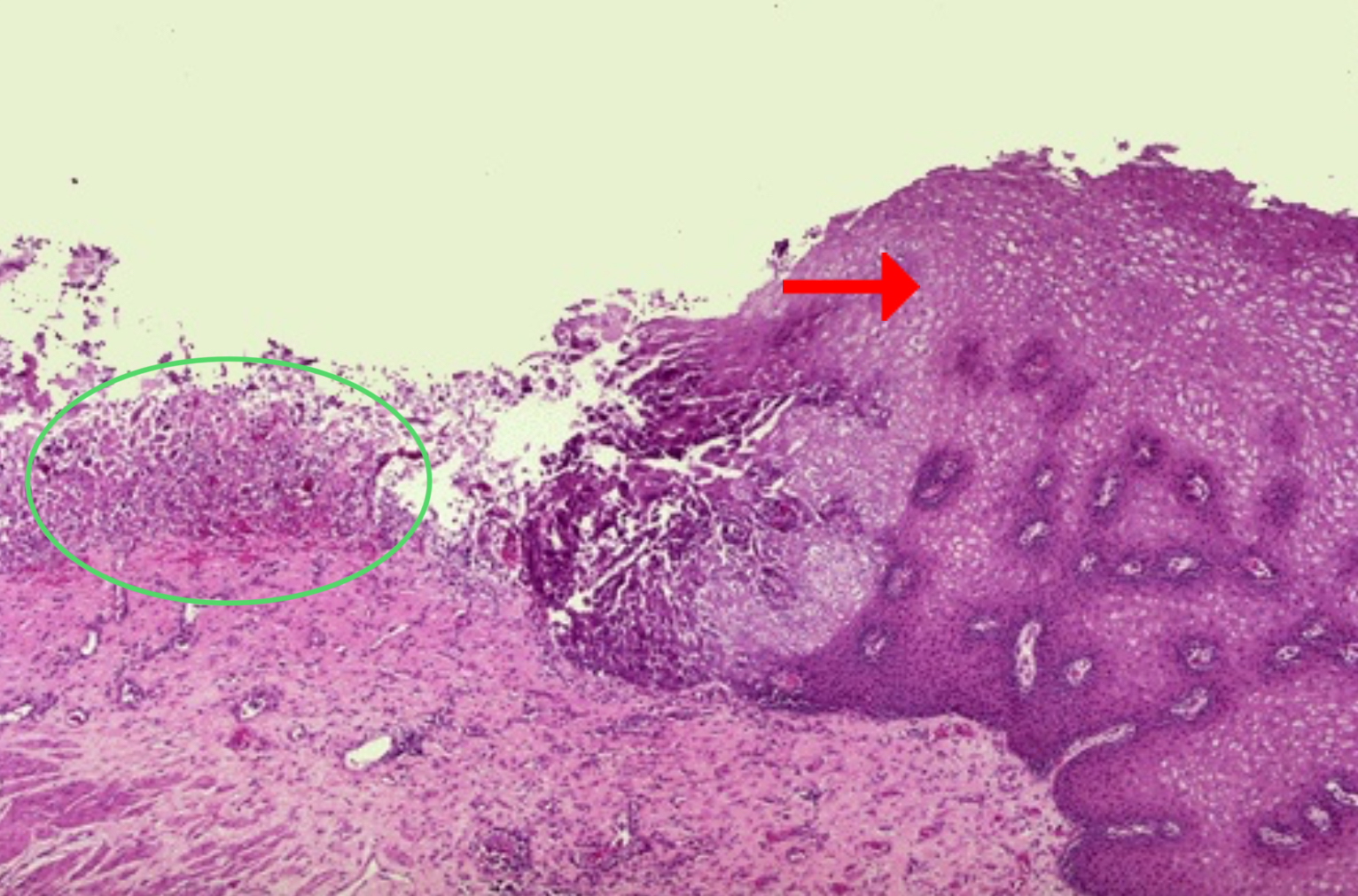
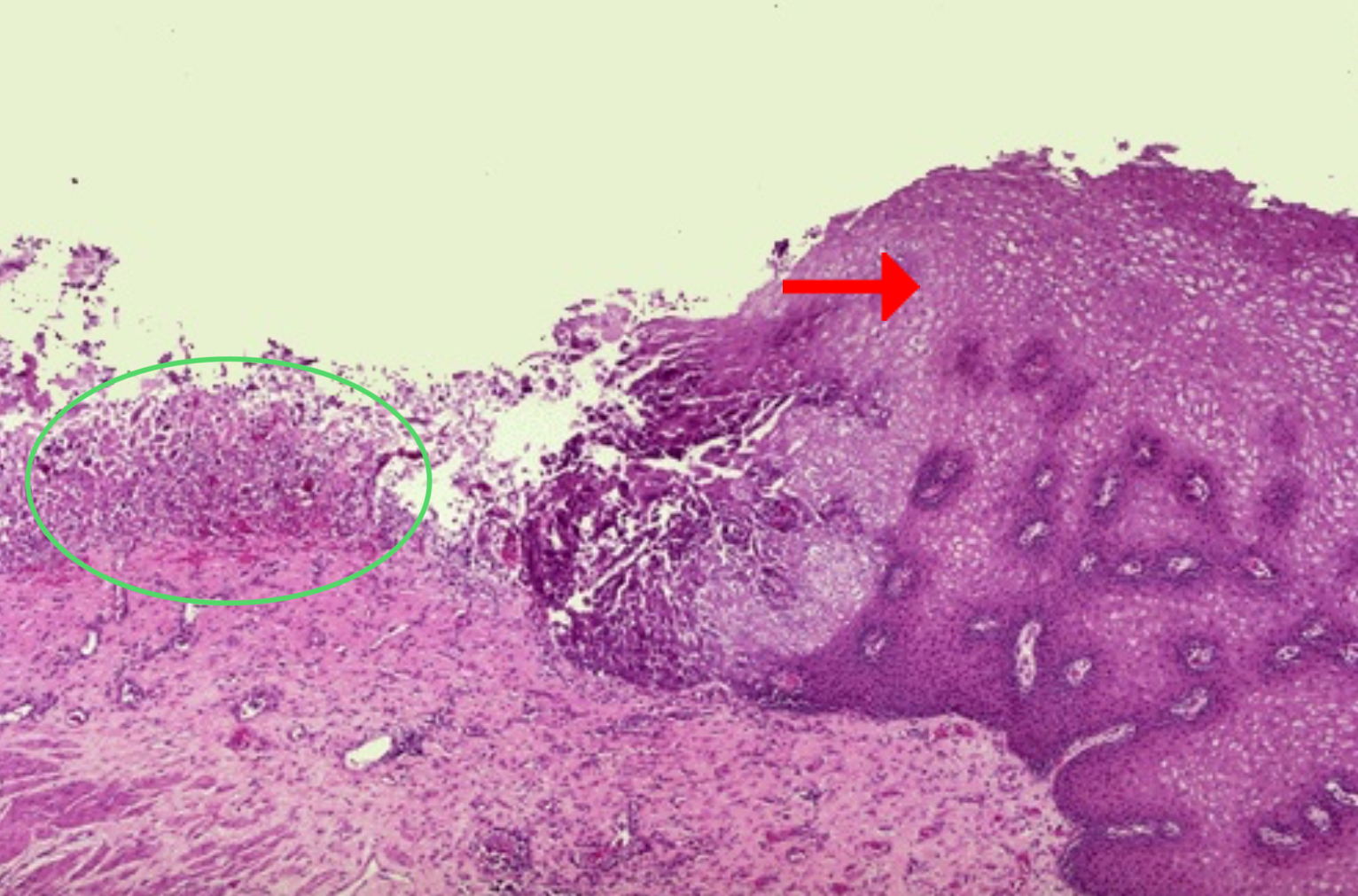
Identify pointed tissue
Identify clinical condition
Identify morphologic pattern of acute inflammation (green circle)
Preponderant cells in acute phase of inflammation
Preponderant cells in chronic phase of inflammation
Most prominent pathologic process if infection persists
Stratified squamous epithelium
Esophageal acute ulcer
Ulceration
PMNs
lymphocytes, macrophages, and plasma cells
fibroblastic proliferation, scarring
An ulcer is a local defect, or excavation, of the surface of an organ or tissue that is produced by the sloughing (shedding) of inflamed necrotic tissue. Ulceration can occur only when tissue necrosis and resultant inflammation exist on or near a surface. Ulcerations are best exemplified by peptic ulcer of the stomach or duodenum, in which acute and chronic inflammation coexist. During the acute stage there is intense polymorphonuclear infiltration and vascular dilation in the margins of the defect.
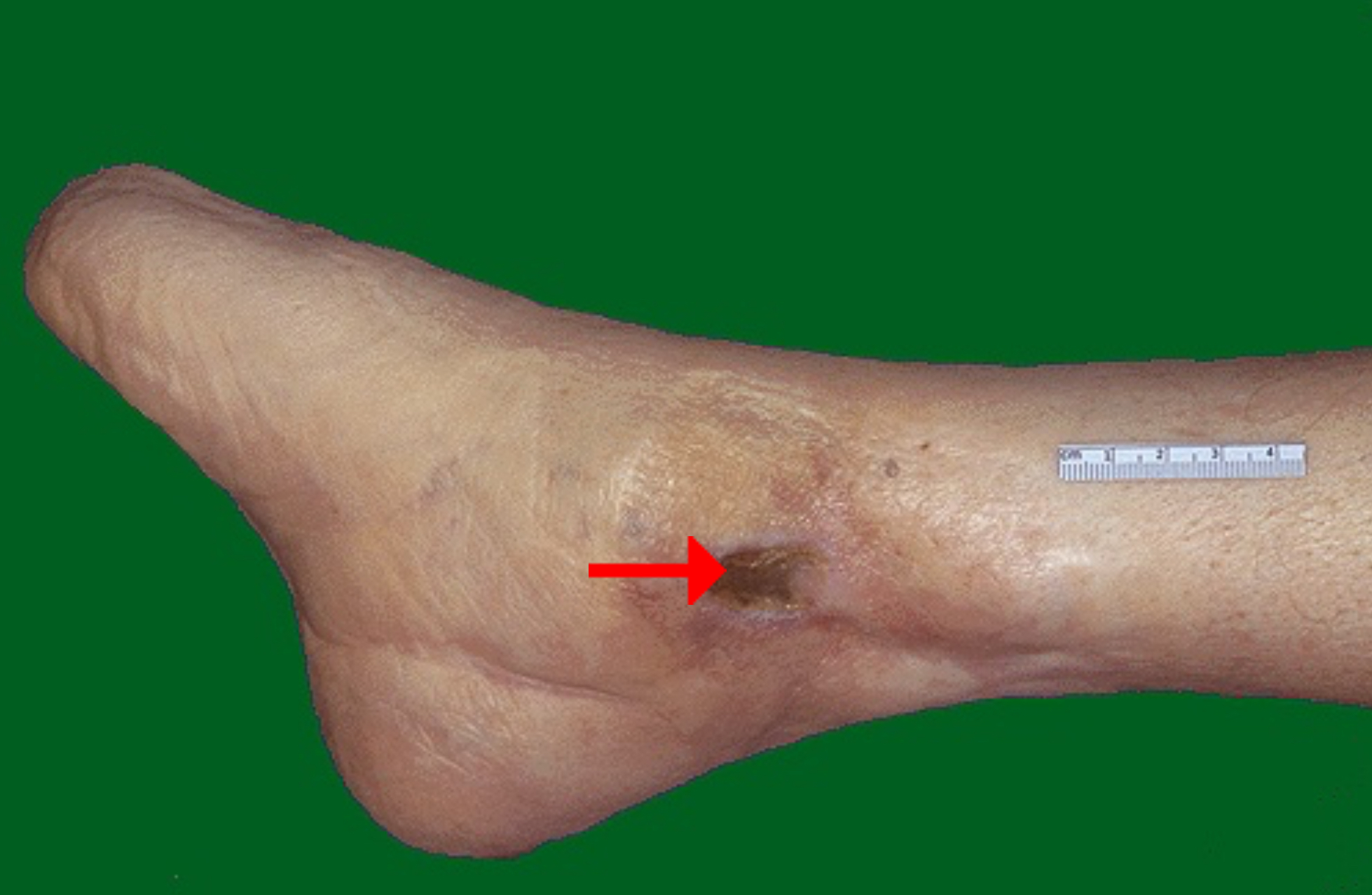
Possible underlying causes of the ulceration
Diabetes mellitus leading to marked atherosclerosis with arterial narrowing
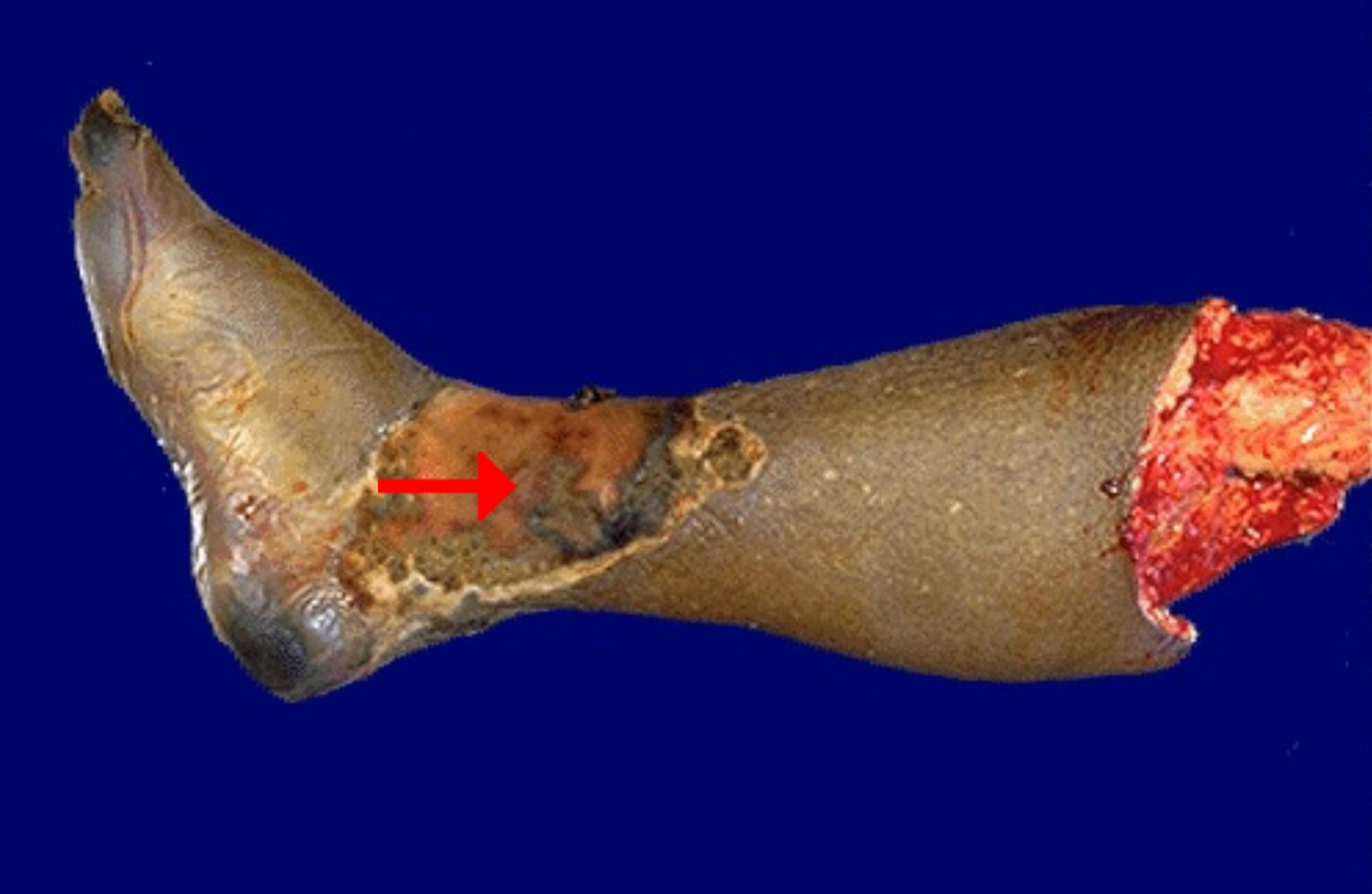
Identify pattern of cell death
Gangrenous necrosis