Encoding Pt 1 - Association Cortices
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
Key terms
Cortex vs Lobe
Sulcus (plural sulci)
Gyrus (plural gyri)
Brodmann Area
White Matter Tracks
Laterality
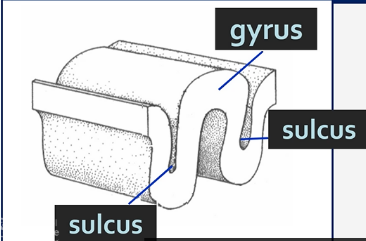
Sulci and Gyri
Gyri - Grooves
Sulci - Fissures
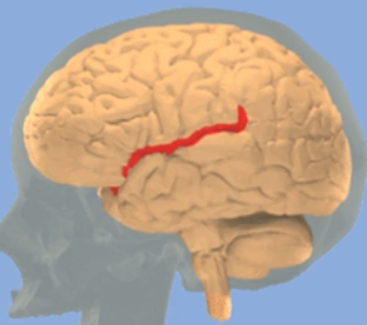
Central Sulcus
Separates Parietal and Frontal Cortices
Insula (Insular Cortex)
The insula is important for the feeling of disgust
Brodmann Areas
'Map' of the cortex
First mapped by Korbinian Brodmann in 1909
Based upon areas of similarity in histology
Still widely used today
52 regions, some subdivided
Posterior Parietal Cortex – Attending to stimuli
Broadmann area 5,7,39,40
Important for attention
Especially spatial attention
Integrates visual, auditory and somatosensory info
Damage results in 'neglect'
Neglect
A sign of posterior Parietal cortex damage
Sensory neglect – Incoming sensory information from the contralateral hemispace is ignored
Conceptual neglect – neglect of the body and the external world in the contralateral hemifield
Hemiasomatognosia – patient denies that affected side of body belongs to them
Motor neglect – fewer movements in the contralateral space
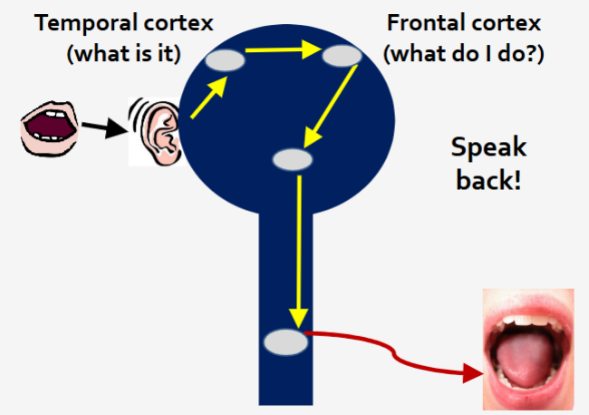
Temporal Cortex
Identifying the nature of stimuli (what is it?)
Agnosia
non-knowledge, or loss of knowledge, is an inability to recognise sensory stimuli and a sign of Temporal Cortex damage
Inferior Temporal Cortex damage
Visual agnosia (psychic blindness)
Patient can see, but no identify
Fusiform gyrus
Prosopagnosia (face blindness)
Inability to recognise individuals from their faces. Patients can describe the constituent parts of the face and can identify the subject by voice, clothes and other cues
Middle Temporal cortex damage
Movement agnosia
Cannot distinguish between moving and stationary
Integration of sensory streams
Allow us to assemble one coherent perspective on the world
The McGurk effect
It happens, even when you know its happening
In humans, vision is the dominant sense (ish)
Large variation in how people experience it
Reduced in Dyselxia, Autism
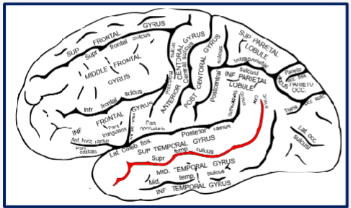
Integrating audio and visual information in speech processing
Superior Temporal Sulcus
Frontal Cortex – Selecting and planning an appropriate response (What to do about it?)
Prefrontal cortex
Rostral to Primary Motor Cortex
Very large in humans
Develops very late 20-30 – is why many mental health conditions develop late
Dorsal – thoughts, attention
Ventral – emotion
Restraint – Judgement, foresight, inhibiting appropriate actions, concentration
Initiative – drive, creativity, curiosity, personality, flexibility
Order – planning, abstract reasoning, working memory, attention
Frontal cortex damage
Difficulty planning sequence needed to complete a task (e.g., making a cup of tea) - requires working memory
Loss of spontaneous interactions
Loss of flexibility in thought
Perseveration – persistence of a single thought or action
Inability to focus on the task in hand
Emotional lability
Abulia – passivity, apathy
Socially inappropriate behaviour
Personality change
Difficulty with problem solving
Expressive aphasia
Hemiplegia
Executive function –resides in the prefrontal cortex
Long-term planning
Withholding impulsive behaviour
'Cognitive control'
Important in many pathologies
Addiction
Personality Disorders
Dementia
Important in everyday behaviours
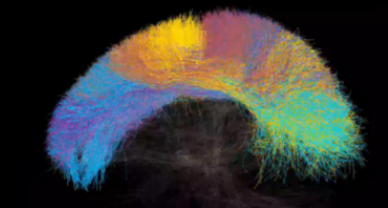
White Matter Tracts
Connect the Association Cortices
Not really visible by physical exam, CT or static MRI
Poorly understood
Use diffusion tensor imaging to map – tactography, a form of MRI
Association fibres
Connect cortical areas in the same hemisphere
Superior Longitudinal Fasciculus – An example of an Association tract

Commisural fibres
Connect across hemispheres
Corpus Callosum (connect hemispheres)
An example of a Commisural tract

Projection fibres
Connect cortex to other brain regions
Corticospinal (motor) and Corona-radiata - examples of projection tracts
Language
Cortical areas working together
Speech difficulties - How do they arise?
Dysarthria
Difficulty moving the muscles of the face + tongue that mediates speaking
Aphasia
Difficulty in naming objects, repetition of words is impaired
Wernicke’s Area - Understanding language
Wernicke's Aphasia
Unable to understand language
Fluent speech, but makes no sense (assuming Broca's area intact), little repetition, adequate syntax and grammar, contrived or inappropriate speech
Which Brodmann Area(s) is Wernicke’s Area located in?
Brodmann Area 22
Which Brodmann Area(s) is the Auditory Cortex located in?
Brodmann 41+ 42
Damage to Wernicke’s Area
Often as a result of a stroke
Also called fluent, sensory or receptive aphasia
Broca’s Area
Brodmann 44 + 45
Broca’s Aphasia
Few problems understanding language – assuming Wernicke's area intact
Difficulty constricting their own
Halting speech
Repetitive
Disordered syntax + grammar
Disordered structure of individual words
Also called non-fluent, motor, expressive or production aphasia
Damage to Broca’s Area
Often as a result of stroke
(Different) branches of the Middle Cerebral Artery
Aphasias
Recognition of 'conversation cues' seems ok
Affects other forms of language: reading, writing, sign language
Many other forms of aphasia
Arcuate Fasciculus
Connects Broca’s + Wernicke’s Areas