Fractionation and Dose-Rate Effect
1/78
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
79 Terms
Clinical advantages of dose fractionation
To help kill the cancer cells while avoiding healthy tissues
Four R's of Radiobiology
Repair, Reassortment, Repopulation, Reoxygenation
Which of the four R's is meant for protecting helping tissue?
Repair and repopulation
Which of the four R's is for damaging tumor cells?
Reoxygenation and Reassortment
Quick overview of repair
DNA damage is fixed promptly, protecting healthy tissue
Quick overview of reassortment
Cells move through the cell cycle between fractions, moving to more sensitive spots of the cell cycle
Quick overview of repopulation
Protecting healthy tissue, cell population increases due to cell division if time between fractions is long enough
Quick overview of reoxygenation
Damages tumor cells, cells are more sensitive to radiation in the presence of oxygen, helps to sensitize tumor cells
Single strand breaks are primarily caused by
Low LET
Double strand breaks are more likely with
High LET
Double strand breaks with low LET radiation are possible but more likely at
High doses
Lethal damage
Not repairable!!
-inevitably it leads to cell death
-abberations, rings, dicentric, anaphase
-caused by two double strand breaks interacting with one another
-cell is unable to divide properly in mitosis and is no longer variable
Potentially lethal damage (PLD)
Damaage that would be lethal under normal conditions
Can be repaired under SPECIAL conditions (such as a modified environment)
Sublethal (SLD)
Can be normally repaired
Sometimes becomes lethal is an additional single SLD is added
Dq on multitarget model
Conditions required for potentially lethal damage repair to occur in a cell
In order for PLD repair to occur, post-irradiation conditions must be SUBOPTIMAL for growth
What does a suboptimal environment trigger?
Triggers checkpoint mechanisms that prevent the cell from moving through the cell cycle
The resulting delay in mitosis seems to allow cells to repair radiation damage
Sublethal damage repair conditions
If a lone double strand break can be repaired before another radiation event causes a second strand break in the vicinity
DNA double strand breaks that can be repaired before that break has time to interact with another double strand break
Sublethal damage can be repaired in a matter of hours under normal cellular conditions BUT
If additional double strand breaks occur before the repair is complete, the damage has a higher chance of becoming a lethal aberration
If we want to harness the power of sublethal damage repair, we must
Find a way to lower the probability of a second double strand break
Dose
the amount of energy radiation deposits in any given unit mass via ionization
Two ways that a radiation dose can be manipulated to encourage sublethal damage repair
1) We can lower the total dose
OR
2) We can use the same dose but slow down the rate of interaction
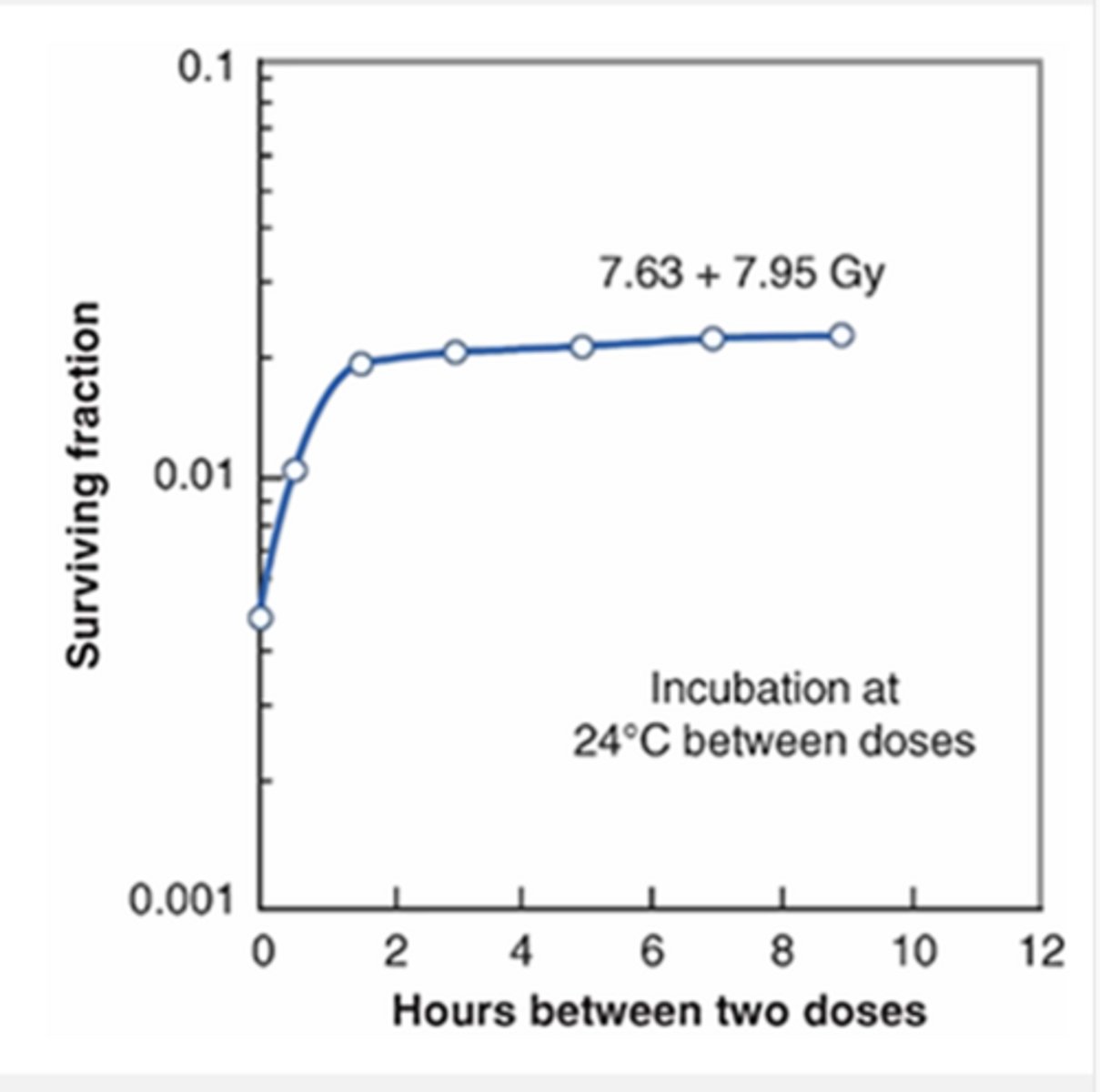
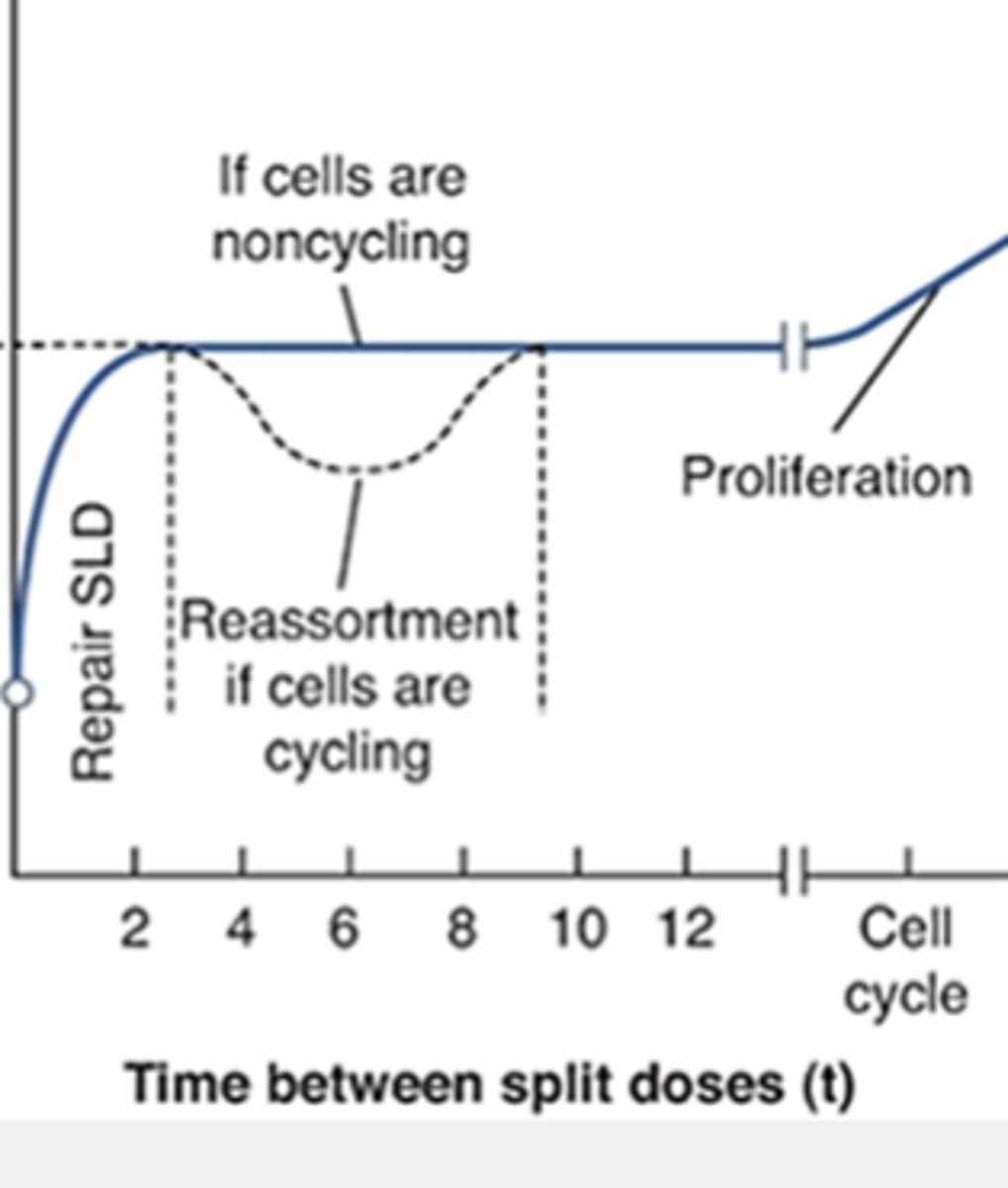
How fractionation can be used to increase the radioresistance of a cell population
By dividing a large radiation dose into several smaller doses separated by a time interval
-the plateau that occurs on the graph indicates the time interval where all sublethal damage has been repaired and there is no advantage to increasing time between fractions
-the cells in this graph were maintained at room temp between dose fractions to prevent them from moving through the cell cycle
Single vs. fractionated dose and cell survival
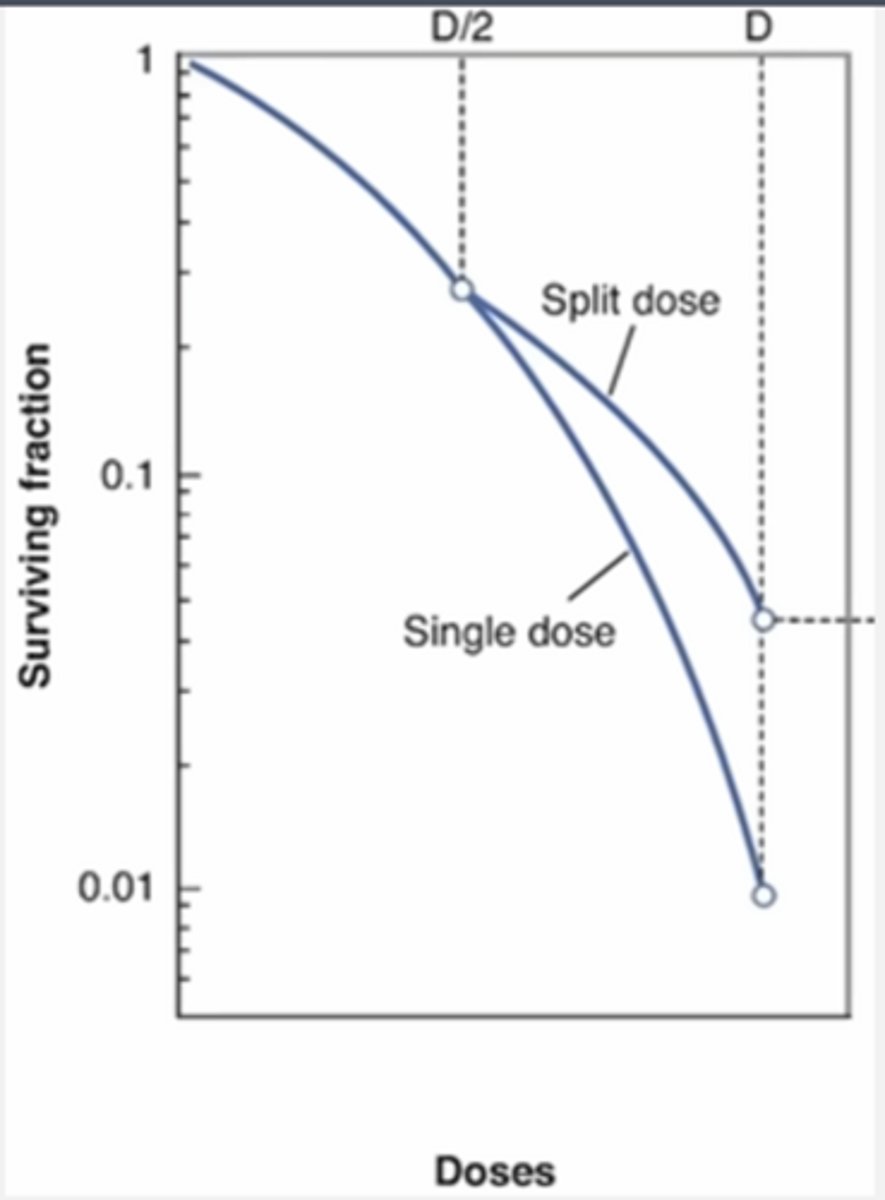
Single event killing and sublethal damage repair
Single event killing is more devastating in relation to sublethal damage repair
(if one radiation event creates both DSB's, there is no way for the cell to repair the first break before the second one occurs)
What type of DNA damage is most likely to occur at LOW doses and LOW LET?
Single strand breaks
Almost all radiation interactions under these conditions result in single strand breaks, which are easily repaired by the cell
Cell survival at low doses of low LET
Cell survival is generally high due to single strand breaks and sublethal damage repair
If cell death does occur, it is likely due to single radiation event causing both DSB, which leaves no time for repair (linear component)
Type of DNA damage that is most likely to occur at HIGH doses of LOW LET
Dominant mechanism: single strand breaks
HOWEVER, higher statistical chance of double strand breaks now compared to at low doses because there are more radiation events happening in general
The odds of different radiation event creating a second double strand break is much higher (quadratic component)
High doses of low LET overview
Dominant damage: single strand breaks
Sublethal dose repair: less common
Chances of another DSB from another radiation event: more likely
What does the shoulder of a survival curve represent?
The ability of a cell population to repair sublethal damage quickly!
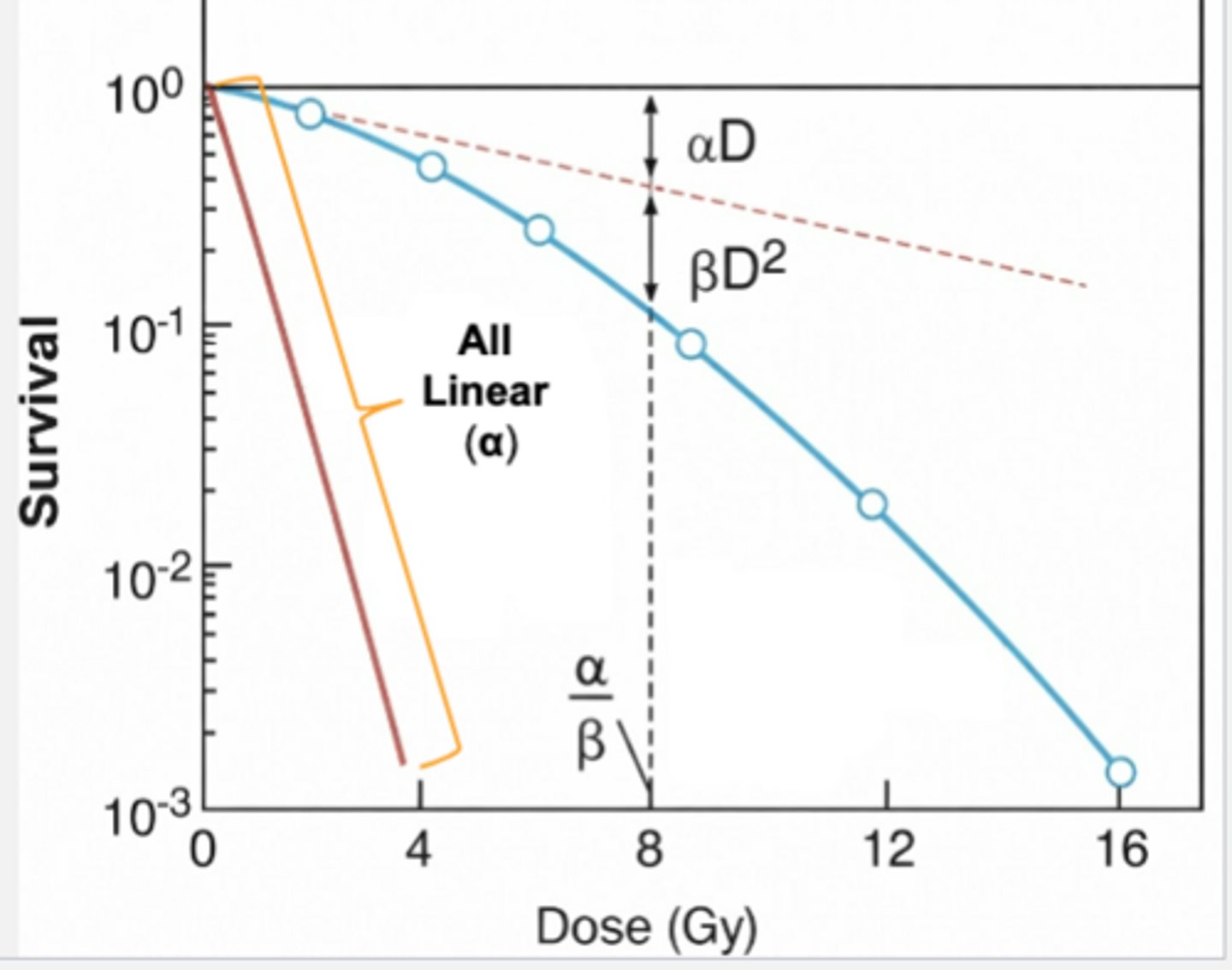
Linear component of linear-quadratic curve
Dominates in the early low-dose regions of the curve
-probability of DSB is low with low LET radiation at low doses
-if DSB occurs, it will likely represent sublethal damage
-lethal damage: predominantly the result of single events
How is the linear portion reflected?
High cell survival region of the curve, the shoulder of the curve is contaned within this region
Quadratic component of linear-quadratic curve
Dominates in high-dose regions of the curve
-there is significantly a higher number of radiation events
-more radiation events= higher number of interactions
-becomes more likely that two interactions will cause two DSB
How is the quadratic portion reflected?
Reflected in comparatively low cell survival in this region
Where does the shoulder of the cell survival curve end?
Ends at the same point where the quadratic portion of the curve takes over.
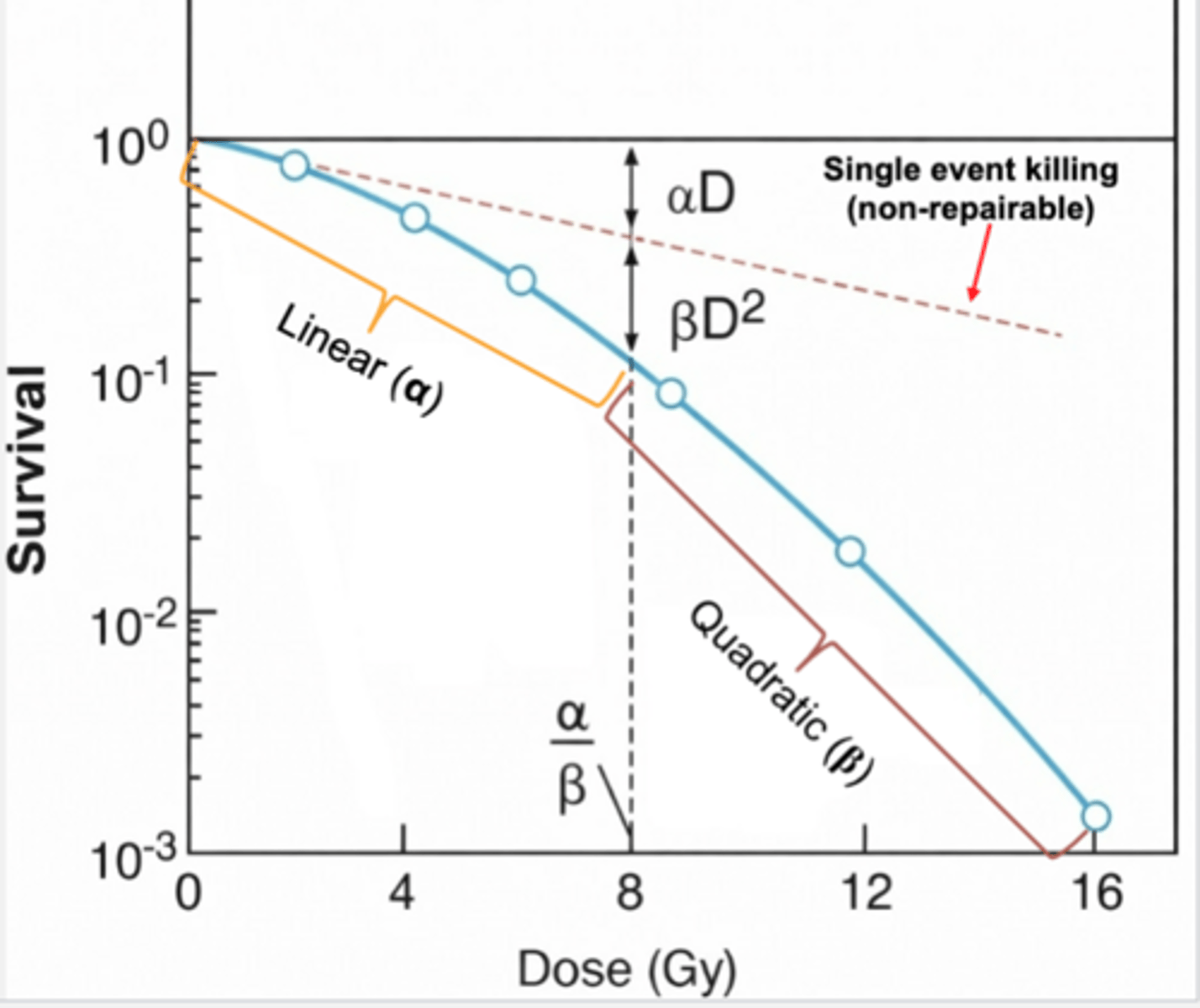
Cell-survival curve: linear quadratic model
Cell populations that are very efficient at repairing sublethal damage will have
broad shoulders
D = α/β
Represents the end of the shoulder and the beginning of the quadratic portion of the curve
The shift in where double events will dominate more of the low LET curve, making it much harder to repair sublethal damage
D = α/β in relation to sublethal damage
If we choose a dose below D = α/β point, we can harness the power of sublethal damage repair
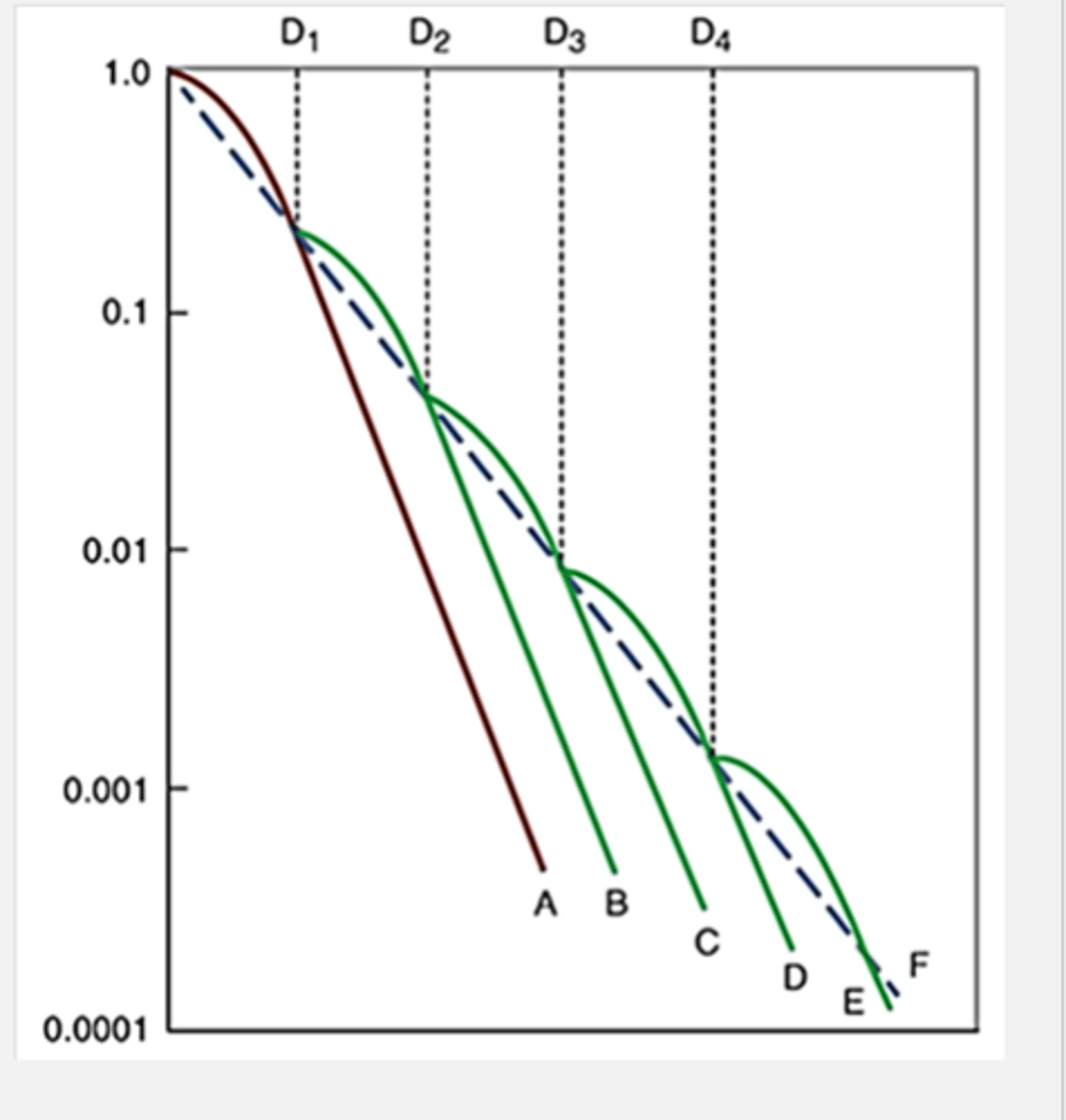
D = α/β in relation to fractionation
If we know where D = α/β point is for a given tissue, we can use that to determine the dose needed for each fraction
By breaking up the total dose into smaller doses that eliminate the quadratic portion of the curve, we can give those normal tissues a chance at sublethal repair every time we deliver a fraction
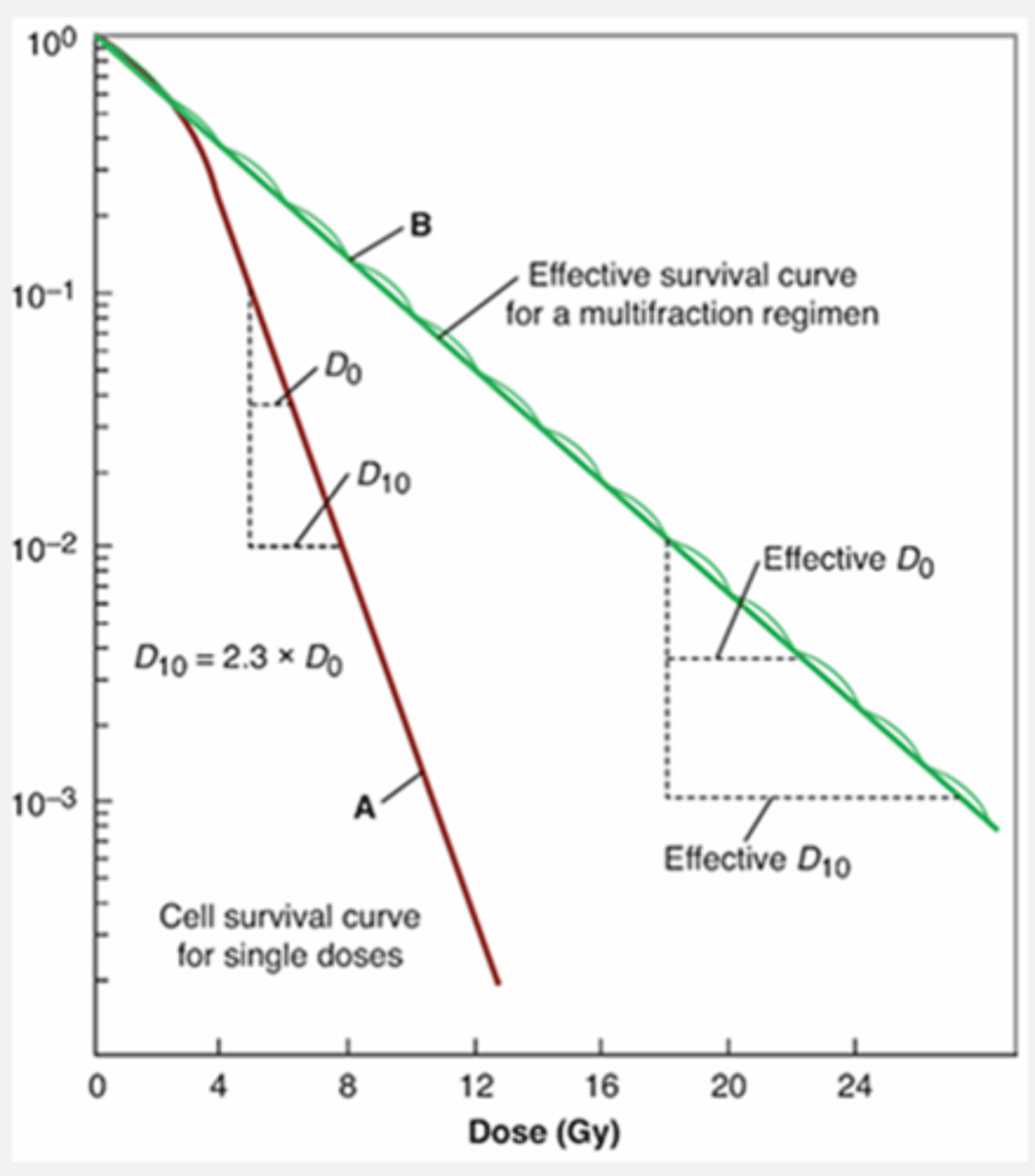
How does fractionation effectively make a cell population more radioresistant?
By repeating the shoulder of the curver over and over
What is the dominant mechanism of DNA damage from high LET?
Double strand breaks
At which doses do double strand breaks overtake at high LET?
At all dose levels
What event also dominates at high LET?
Single-event killing due to high LET radiation being so densely ionizing
With single event killing, what is the chance of sublethal damage repair?
Zero chance
Since both DSB occur at the same time
High LET cell survivial curves do not have a
Shoulder
No D = α/β
High vs low LET cell survival curve
High LET
-no shoulder
-no D = α/β
-single event killing takes over at all dose levels
-no quadratic to calculate
Low LET
-has shoulder
-has linear and quadratic
High LET fractionation effectiveness
Ineffective at increasing the radioresistance of a cell population because there is no sublethal damage repair to take advantage of, and therefore no shoulder to repeat
Fractionating the dose almost makes no difference in cell survival for low-energy neutrons in this graph
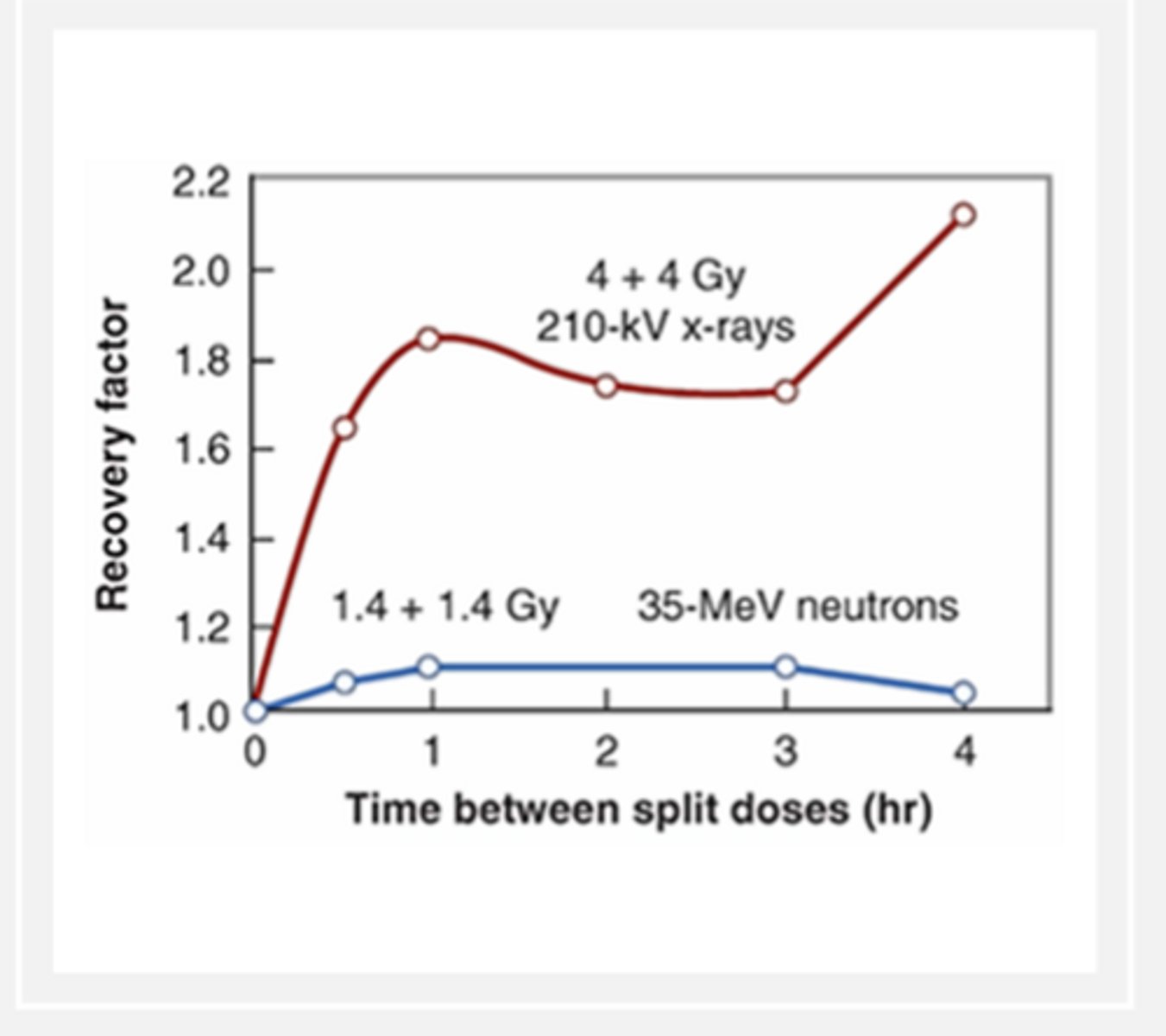
Low LET fractionation effectiveness
Effective at increasing radioresistance because there is sublethal damage repair that can be taken advantage of
Radiosensitivity changes with position in
Cell cycle
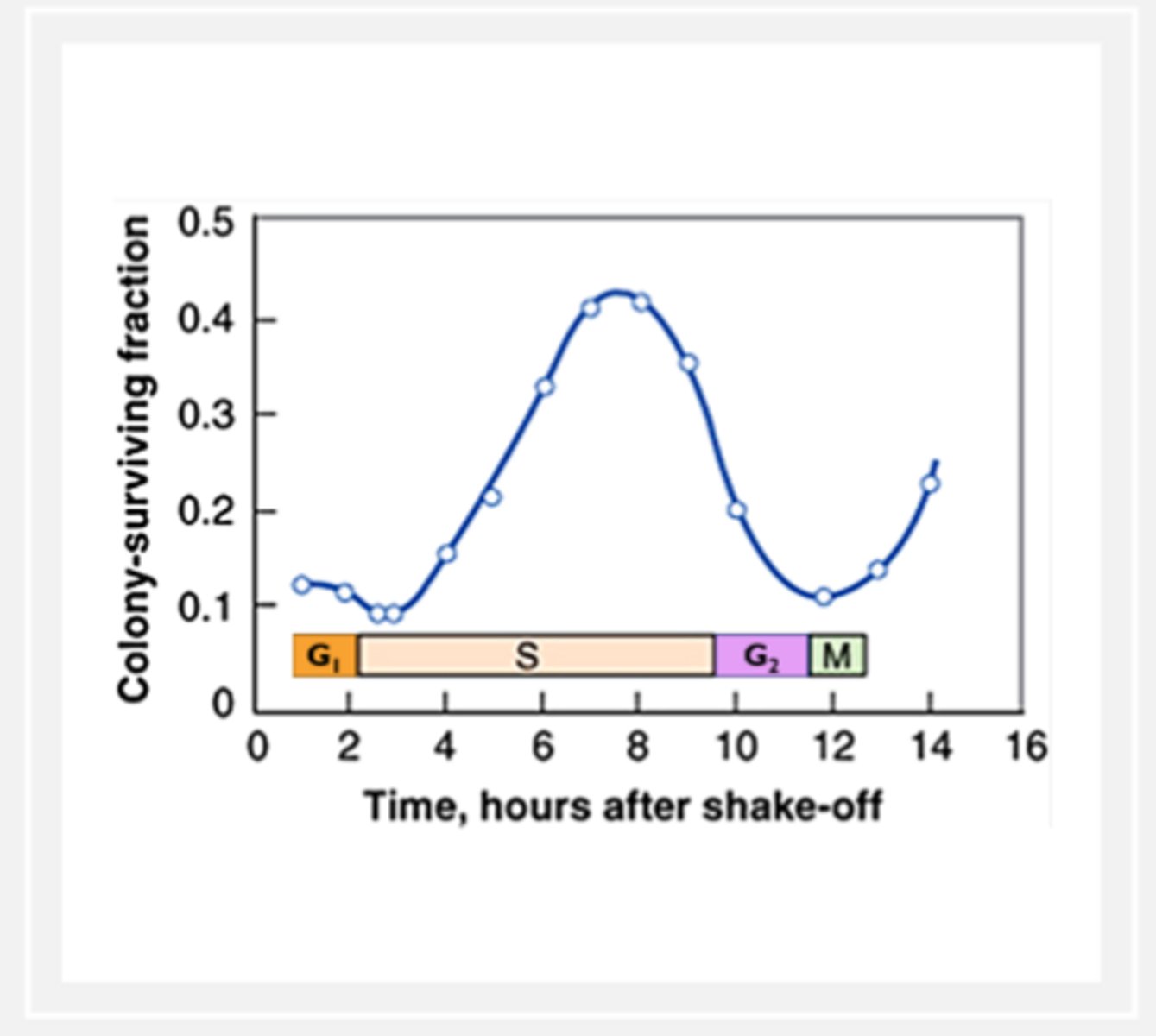
Cells are more radiosensitive in
M phase and G2
Cells are more radioresistant in
S phase
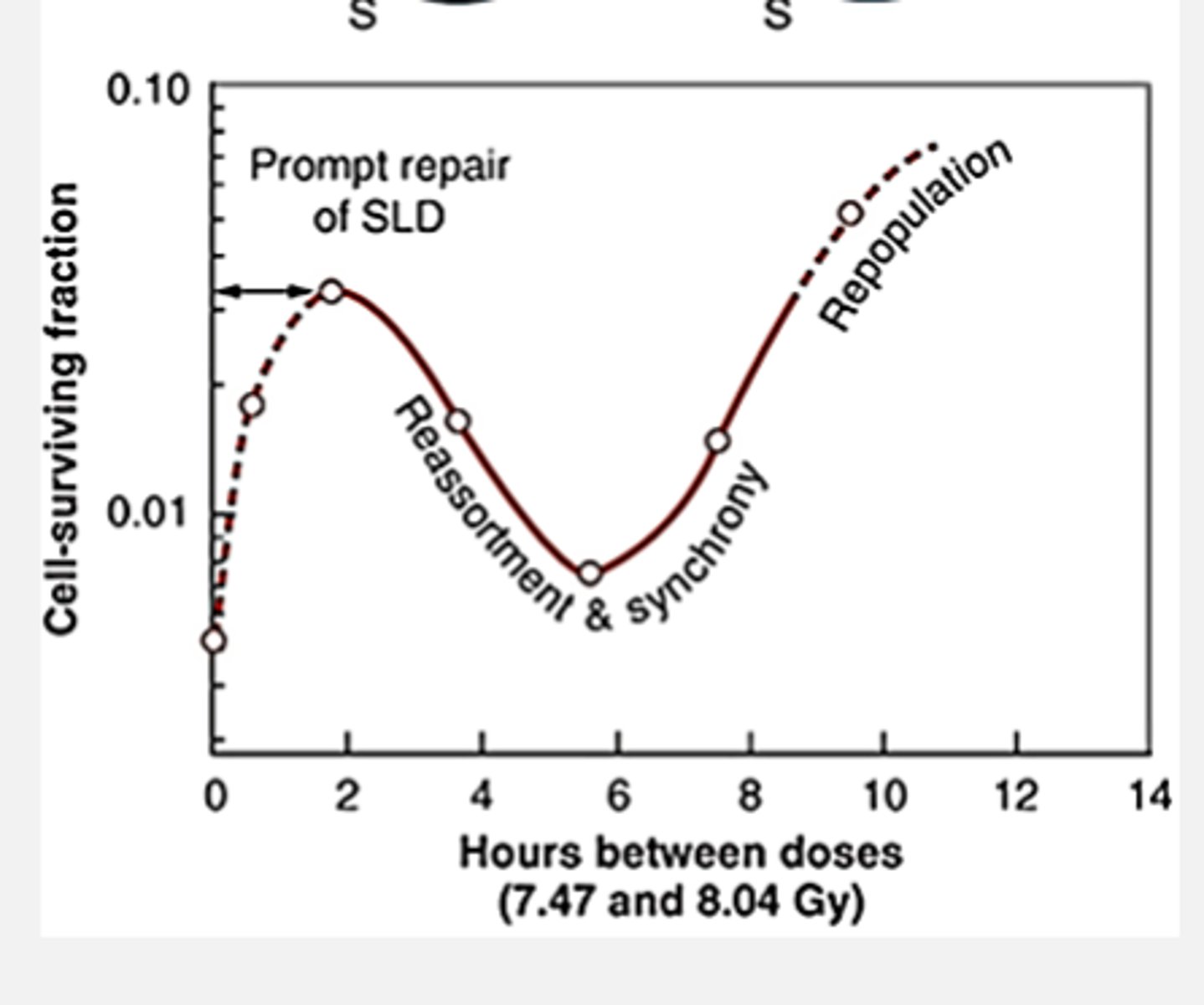
Fractionation and reassortment
radiation will naturally produce a rough synchronization of in vivo cell populations by disproportionately killing cells in sensitive phases of the cell cycle
We can purposefully plan the timing between radiation fractions to be delivered when large numbers of cells are in the sensitive cycle phases
If we allow more cells to cycle into sensitive phases like G2 and M, we can kill more of them with the same dose
Fractionation and Repopulation
Longer periods between fractions give cells more time to progress through full cell cycle, including mitosis
Everytime a group of cells progress through M, it divides and doubles the original number of cells
Given enough time between fractions: repopulation
Cell survival increases due to multiplication in the M phase
Repair overall
Lower the probability of double strand breaks, cells can repair sublethal damage in hours
Reassortment overall
If we allow cells to cycle into sensitive phases like G2 or M, we can kill more of them at the same dose
Repopulation overall
If cells are given enough time to progress through the entire cell cycle, the population will increase via normal cell division
What does the curve look like with the four R's for proliferating cell lines?
If non-proliferating cells, what does it look like on a curve
Straight line, experience some repair because repair always happens on some level with low LET
If total cell cycle time is long/ non proliferating, which R's do not apply?
Reassortment
Repopulation
Repair: Fractionation Overall
We can protect healthy tissue by harnessing the power of sublethal repair
A dose should be carefully chosen to allow for a repeaat of cell survival curve shoulder
How many hours is needed between fractons for repair to happen?
Up to 2 hours
Reassortment: Fractionation Overall
Radiosensitizes tumor cells by choosing fraction timing that allows cells to cycle into sensitive phases
Repopulation: Fractionation overall
Must choose fraction timing that allows normal tissue to repopulate, even if that means some repopulation of tumor cells
Dose rate
Dose per unit time
Examples of common dose rates in radiation science
10 Gy/min
1 mR/hr
5rem/year
Dose fractionation
Administering discrete doses of radiation
There is a beginning and an end to administration
Dose rate effect
Irradiation is continous!!!
Lowering the rate of radiation interactions in tissue is an important way to prevent too many DSB in close proximity (lethal effects)
If you lower the dose rate and extend the total exposure time
It is equivalent to delivering an infinite number of infintively small fractions
Dose rate is fractionation's
fraternal twin
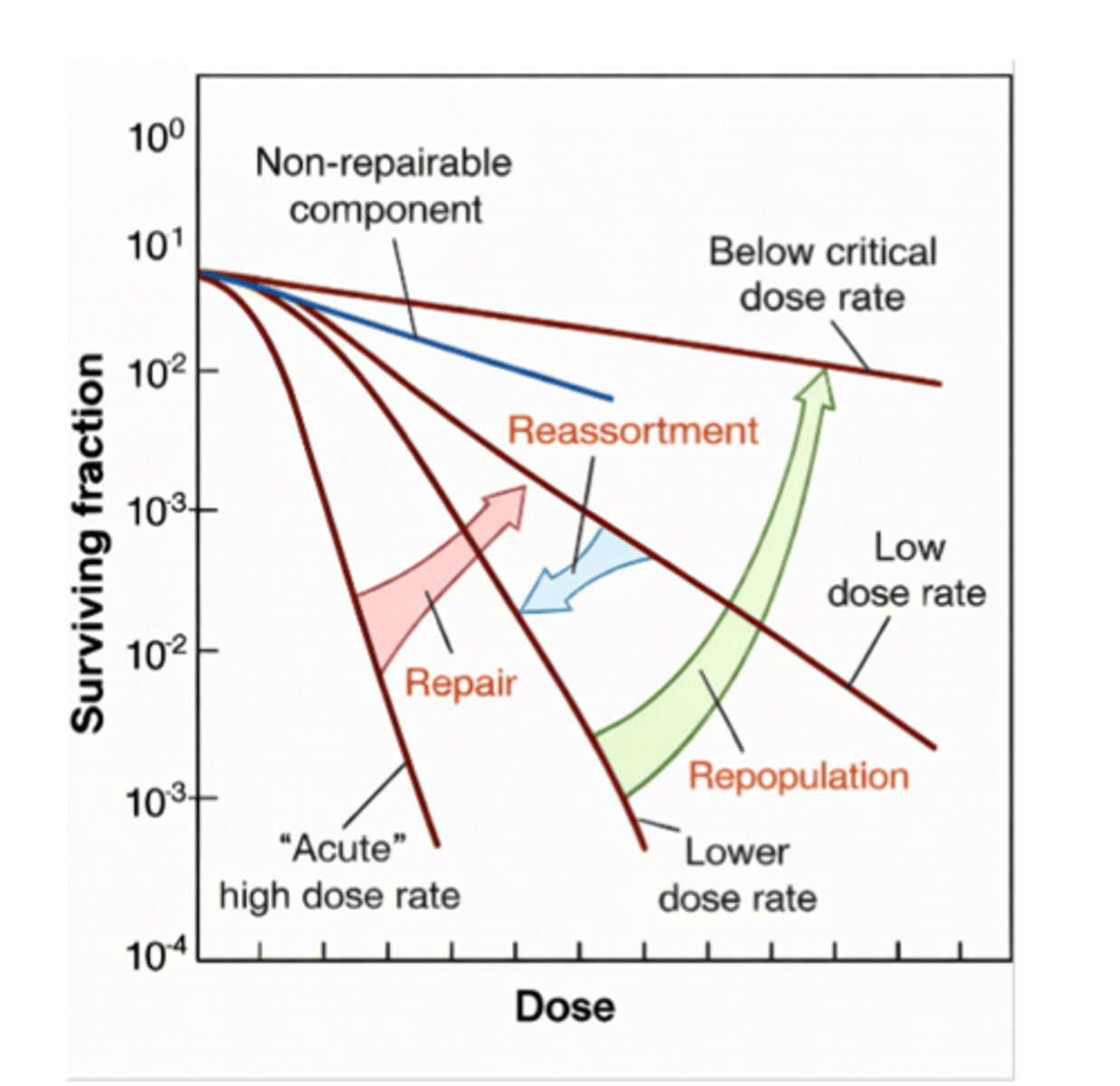
On a graph low dose rates are more
radioresistant on a graph, more to the right and transverse
more broad shoulders
On a graph high dose rates are more
radiosensitive, demonstrated to the left with less of a shoulder
Common applications influenced by principles of dose-rate effect
Occupation dose limits
Regulatory limits on device output
Shielding devices
Patient dose reduction programs (image gently/wisely)
ALARA
INVERSE SQUARE LAW (distance increases, dose decreases)
Inverse dose-rate effect
Lower dose rates trigger checkpoint genes in HELA CELLS, resulting in a blocked G2
G2 near mitosis is very sensitive
Under constant low-dose rate irradiation, many cells die here that would actually survive at higher dose rates
Which cell population is affected by inverse dose rate effect?
HELA CELLS
Repair: Dose rate effect
Low dose rates promote sublethal repair
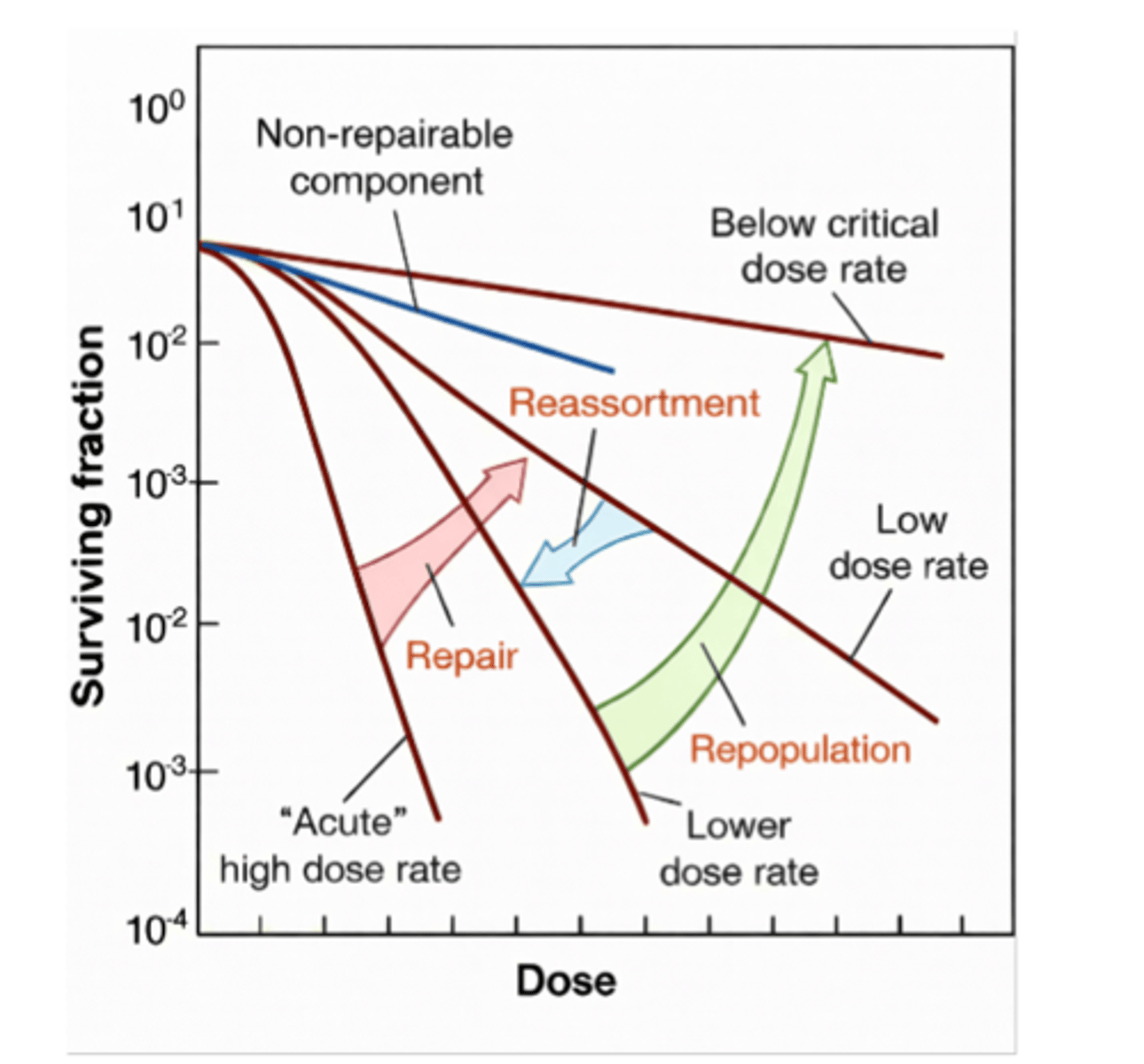
Reassortment: Dose-rate effect
Lowering the dose rate cana trrigger a reassortment sensitivity in some cells
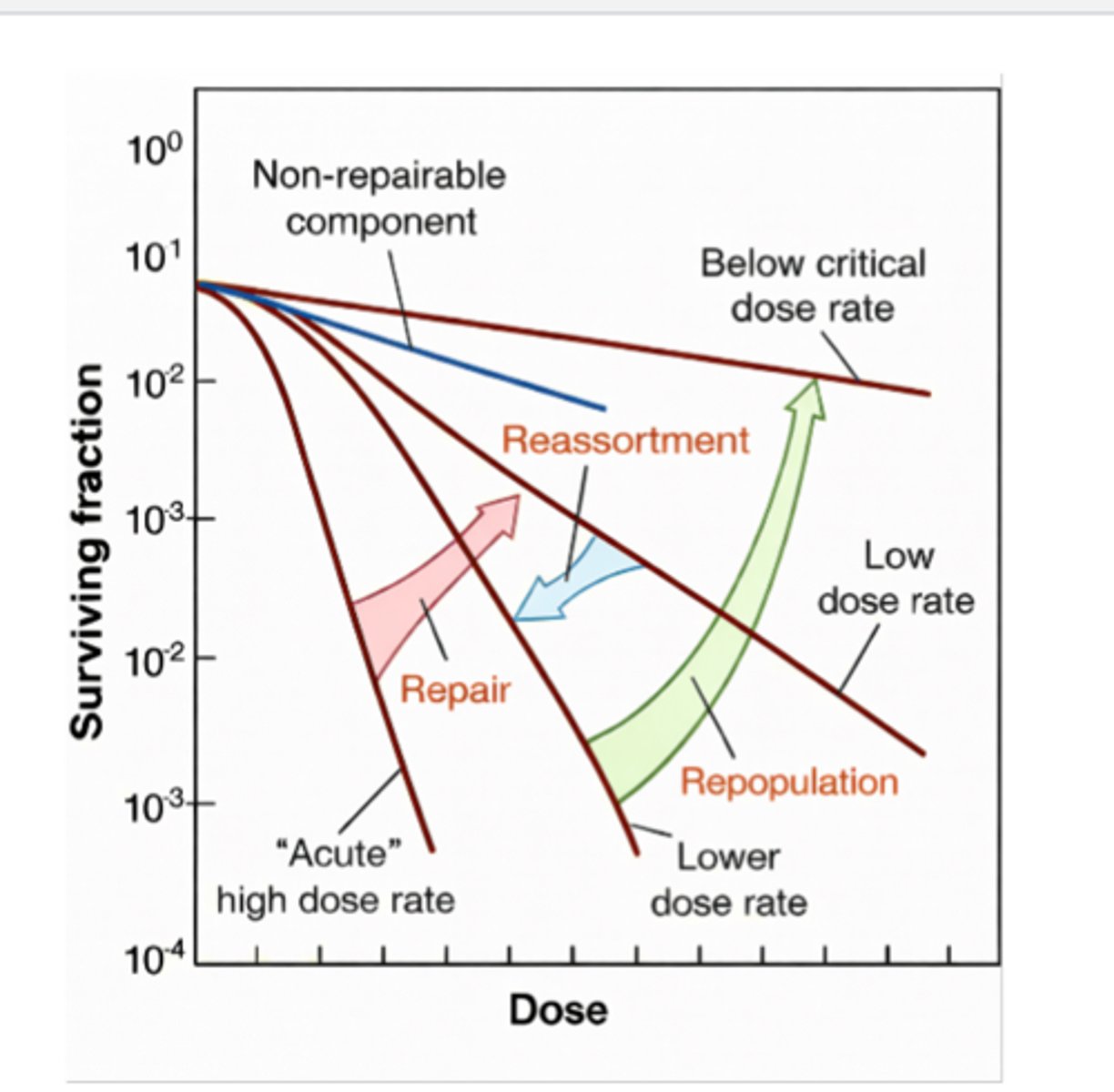
Repopulation: Dose-rate effect
Incredibly low dose rates allow depleted cells to repopulate
High LET and dose-rate
DNA damaged by single events represent a non-repairable component that is NOT AFFECTED BY DOSE RATE