week 3 Typical Motor Development Birth to 2 years old
1/59
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
60 Terms
Childhood occupations
play, feeding, dressing, grooming, communication, functional mobility
primitive reflexes
involuntary (automatic, CNS) motor responses originating in the brain stem present after birth in early childhood development that facilitates survival. eventually integrated/inhibited by 4-6 m, and replaced with voluntary motor movements
Retention
occurs when reflexes dont integrate, difficulty with volitional smooth movement
delayed milestones, poor motor coordination, poor balance and posture, learning difficulties, behavioral concerns, sensory processing
Delayed milestones
crawling, transitions, walking
poor motor coordination
fine and gross motor, writing, cutting, dressing
poor balance and posture
maintaining balance despite changes in posture
learning difficulties
difficulties with reading and writing
behavioral concerns
impacts habit and routines
sensory processing
over or under sensitivity to stimuli
Newborn primitive reflexes
rooting, sucking, moro, spinal galant, symmetrical and asymmetrical tonic neck reflex, grasp, stepping, tonic labyrinthine response
Rooting reflex
supports infant feeding
Stimulus: stroke side of cheek
Response: head rotates to the side of the stimuli, mother opens wide with tongue thrust
Integration: around 4 m
Retention: feeding difficulties, speech and articulation, movement and head control
Sucking Reflex
Stimulus: light touch to inside the mouth
Response: closes mouth, sucks and swallows, more control
Integration: around 3-5 m
Retention: poor suck, swallow, breath coordination. Under development of dissociation of tongue and jaw movements
Moro (startle) reflex
Stimulus: hold child and drop head more than 30 degrees
Response: arms extend and hands open (fear) followed by arm flex and hands closed (protect)
Integration: around 6 - 10 m
Retention: impacts development of head control, equilibrium and protective reactions
Galant reflex
Stimulus: in quadruped or supported prone, stoke along side of spine up/down
Response: lateral flexion and hip external rotation towards stimulated side
Integration: around 3-9 m
Retention: poor reciprocal movements such as crawling and walking
Asymmetrical Tonic Neck Reflex (ATNR, Bow and Arrow)
Stimulus: in supine, turn head to one side
Response: arms and legs extend on nasal (turned side). arms and legs flex on occipital side)
Integration: around 5-6 m
Retention: impacts hand eye coordination, reaching, grasping, bilateral coordination, rolling
Symmetrical Tonic Neck Reflex (STNR)
baby is prone
Stimulus: flex head, extend head
Response: arms flex and legs extend, arms extend and legs flex
Integration: around 5-6 m
Retention: crawling and walking
grasp reflex (hand and plantar)
Stimulus, Response, Integration, Retention
Stimulus: pressure on ulnar surface/palm or ball of foot
Response: fingers flex/close or toes flex/curl
Integration: around 5-6m
Retention: impacts voluntary release of objects and standing/ambulation
Spontaneous stepping reflex . Stimulus, Response, Integration, Retention
Feet responding to surface underneath, no voluntary control on gait
Stimulus: supported while bounced on feet
Response: legs extend, may hyper extend knees
Integration: around 1-2 m
Retention: impacts gait, standing, walking
Tonic Labyrinthine Response
Stimulus: arms and legs moved into flexion (supine). arms and legs moved into extension (prone)
Response: extensor tone of neck, arms, and legs increase. flexor tone of neck, arms, and legs increase
Integration: around 6-10 m
Retention: impacts turning/rolling, transitions from lying to sitting and crawling
Righting reactions
motor behavior that appear at 4-6 m and are important in developments of posture. automatic postural responses that allow the body to maintain or return to an upright orientation in space using visual, vestibular and somatosensory input to align the head and body related to gravity
Equilibrium reactions
motor behaviors that begin to emerge at 7-8 m and include protective reactions of the limbs and curvature of the spine to accommodate trunk displacement. starts to begin when a baby starts to move as they are losing balance.
Types of righting reactions
landau righting reaction, labyrinthine head on body righting, optical righting, body on body righting
Landau “airplane”
a righting reaction
Stimulus: head in prone suspension
Response: hips and legs extend, arms extend and abduct
Integration: onset: 3-6 m. integrate around 12 m
Retention: impacts development of prone extension, sitting, standing
Labyrinthine (head on body) righting reaction
Stimulus, Response, Onset, Integration, Retention
a righting reaction, replies on vestibular (understanding where head is in relation to body)
Stimulus: head vertically and tilted to the side with eyes covered
Response: maintains head in upright position. onset: 4-6m, integrate: remains in tact/present throughout lifespan
Integration: never, goes into adulthood, but can be overrided as an adult
Retention: ability to lift head and perform transfers, maintain head in position despite movement
Optical Righting
Righting reaction
Stimulus: head vertically and tilted to the side with eyes uncovered
Response: maintains head in upright position using visual information
Integration: onset: 4-6 m. integrate; remains intact throughout lifespan
Retention: maintain head in position despite movement
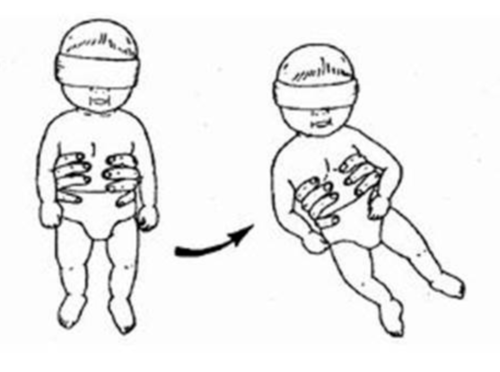
Body on Body righting
righting reaction, correcting to midline orientation
Stimulus: displace/move the body or the head
Response:body reorients itself to the surface despite change in head position
Integration: onset: 5-6m. Integrate: remains in tact/present through lifespan
Retention: impacts ability to move in rotary positions, impact learning to transitions into sitting or quadruped, rolling
Types of equilibrium reactions
Protective extension, equality reactions
protective extension
understanding if limb protects from weight shifting/falling
Stimulus: holding at the pelvis, provide sudden movement of the head towards floor (threat). in sitting: push forward, to the side or backwards
Response: arms extend to catch and protect the head
Integration: onset: 6m (forward, sideways, backwards)
Retention: impacts protection when center of gravity is displaced
the order in which Protective extensions show
forward parachute reflex → slideward parachute reflex → backward parachute reflex
Equilibrium reactions
body shifts to opposite side that surface shifts
Stimulus: center of gravity is displaced
Response: head righting (non weight bearing side trunk flexes, arm and leg abducts and internally rotates, elbow wrist and fingers flex). head righting on weight bearing side (truck extend/elongates, arm and leg externally rotate, elbow wrist and fingers abduct and extend)
Integration: onset 6 m. integrates: remains in tact/present through lifespan
Retention: difficulty with transitional movements and maintaining balance
Postural Alignment
how the head, shoulder, spine, hips, knees, ankles line up with one another. can be good or bad.
proper: put decreased pressure through spine and assists with good posture and efficient movement patterns
non proper: out of alignment, puts undo pressure on another join above or below
Base of support
used to assess postural alignment. Changes based on position: sitting (long sit→ short sit→ ring sit→ W sit), standing, prone (flat → prone prop)
Center of Gravity
single pt where a persons entire wight can be considered consolidated/centralized. average location of the persons weight
Weight Shift
chnage in the base of support away from the center of gravity
transitional movements
help a person move from one position to another. children perform these movements as they learn to move. (rolling, sitting, kneeling, standing)
Supine
gives largest surface area. lying on the back, stabilizes head, truck scapula. requires anti gravity movement to engage in hand on body, hand to midline, hand to mouth
Prone
on the belly. develops strength and coordination of the trunk and head, lengths muscles of anterior neck, trunk and hip muscles, pushing up on hands develops palmas arches and proximal shoulder control/stability. explains why tummy time is very important
side laying
narrower base of support. balance is dependent on control of flexor and extensor. offers gravity lessened position of unweighted. allows for exploration of reaching, kicking, hand on hand body exploration. explore midline in various positions
sitting
becoming more independent in movement. changes in visual orientation allows for improvement in visual perceptual skills. gross motor progression between supine/prone to stand, walking, crawling. requires delicate balance of flexors and extensors
standing
more narrow than typical sitting. improve LE joint alignment, balance, LE strength + control for walking. Challenges core strength and stability
What are developmental characteristics seen in newborns?
physiological flexion. asymmetrical. gravity dependent. random extremity movements. turn head to clean airways. eat and eliminate. establish bonds with caregivers. attempt to self sooth.
One to Two months development
begins to lift head in prone (big prone age). holds head up when in supported position. hand to mouth for self soothing. shows more facial expressions. begins to start improving suck-swallow-breath coordination
3 to 4 m development
begins to show symmetry. explores different position (supine, prone, supported sitting), rolls stomach to back. begins to grasp toys. hands to midline-holds bottle. improving self soothing. experimenting with voice for expression. not strong enough for sitting (antigravity) without support causes a stacked spine.
5 to 6 m
achieves symmertry. prone prope on extended elbows. plays and weight shift in prone. rolss both directions. sits independently. maintains side lying. improving control of extremities. pull to sit. begins drinking from cup. babbling/imitating sounds.
7 to 8 m
controlled asymmetry. on the move. prone pivot. commando crawling/cruising. pull to stand. various grasp patterns. finger feeding, improving lip seal. increasing speech sounds.
9 to 10 m
creeping. variation in sitting position. pull to standing through half kneel. standing with decrease BOS. Walks with two hand held. protective reactions ( b/c BOS is becoming unsupported). greater grasp patterns to accommodate various objects.
11 to 12 m
emerging independent stand and ambulation. cruises, walks with one hand assist. refining reach and grasp with voluntary supination. eating solid foods with improved oral musculature. increasing speech with some words.
18 m
walking forward/backwards. stop and turn. pull toys. walks upstairs with hand held. squats during play. small object manipulation. construction toys.
2 yr
swings arms when moving. run. stairs with railing (2 step), jumps, emerging hand preference. thread beads on lacing string. challenging independence. tool use- crayons, markers. Dont have a hand dominance and it wont show until 5 (still work on developing skills on both sides)
When does a child start to develop grasping reflex and visual scanning skills?
birth to 3 m
4 m fine motor grasp
directed reaching, ulnar palmer grasp
5m fine motor grasp
palmer grasp.
Whats the typical age for a child to transfer between hands?
5-6m

At what age will a child have a radial palmer grasp and begin to reach with increase accuracy?
6 m
7m fine motor/grasp
radial digital grasp. raking grasp. voluntary release.

When does a child have an inferior pincer grasp and starts picking up small objects?
9 m
8 m fine motor/grasp
radial digital grasp.
9 m fine motor/grasp
inferior pincer grasp. picking up small objects.
What age will a child develop a fine pincer grasp and release into container?
10 m

12 m fine motor/grasp
pincer grasp. release objects in container and surfaces.