Lecture 4: Regulation of K+ secretion, Regulation of pH
1/27
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
28 Terms
is most of the K+ in our body intracellular and extracellular
intracellular
explain effects of low extracellular K+ concentration (hypokalemia) on neuronal and skeletal muscle action potentials
bigger K+ gradient → more negative equilibrium potential for K+ (Ek) → pulls the resting potential toward K+ equilibrium potential → Vm farther from threshold → more difficult to generate action potential
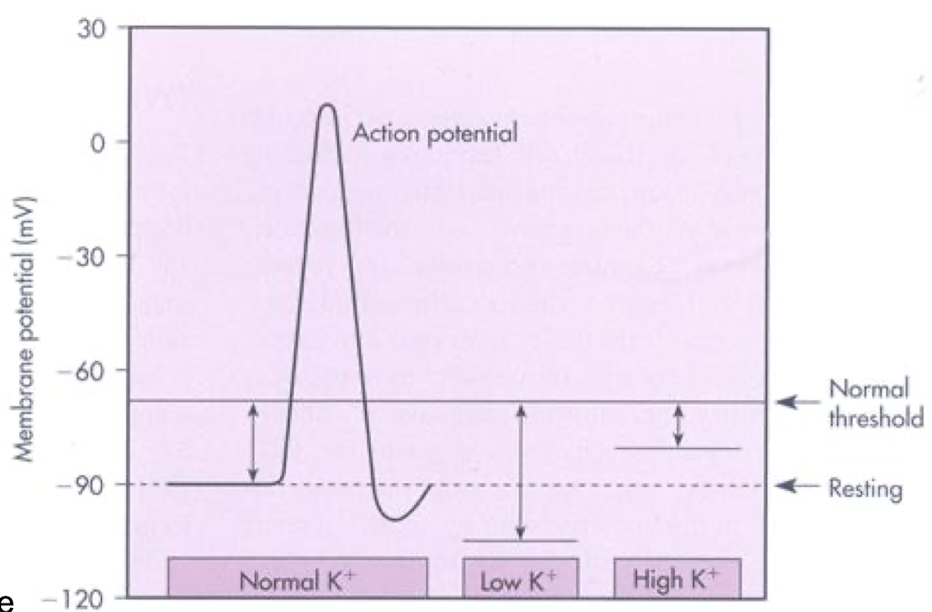
explain effects of high extracellular K+ concentration (hyperkalemia) on neuronal and skeletal muscle action potentials
smaller K+ gradient → Ek is less negative → resting Vm less negative → not as far from threshold → hyper-excitability → easier to generate AP
is K+ synthesized in the body?
no
where is K+ filtered
freely filtered at the glomerulus
55% of filtered load is reabsorbed in the proximal tubule
30% of filtered load is reabsorbed in loop of Henle
how is secretion of K+ controlled
aldosterone
ECF [K+]
flow rate
what is the relationship between plasma [K+] and aldosterone
increased plasma K+ → acts on adrenal → increased aldosterone release
decreased plasma K+ → acts on adrenal → decreased aldosterone release
what is the relationship between ECF [K+] and K+ secretion
hyperkalemia (high ECF K+) → acts on Na/K ATPases on CD basolateral membrane → increases K+ secretion
hypokalemia (low ECF K+) → acts on Na/K ATPases on CD basolateral membrane → decreases K+ secretion
what is the relationship between flow rate and K+ secretion
high flow rate → acts in CCD → increases K+ secretion
low flow rate → acts in CCD → decreases K+ secretion
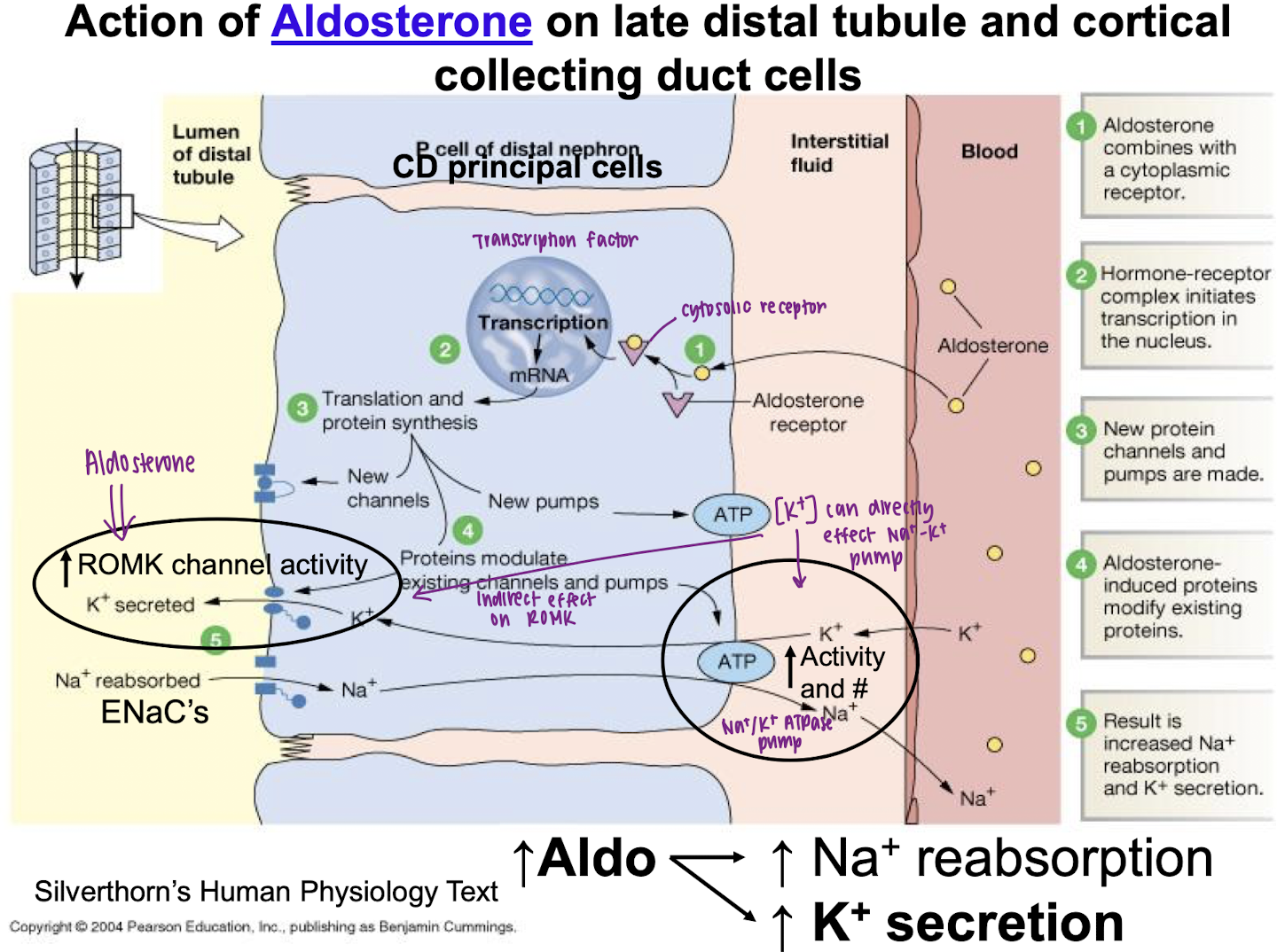
explain the action mechanism of aldosterone on K+ secretion
aldosterone combines with cytoplasmic receptor
initiates transcription, translation, and protein synthesis in nucleus
proteins modulate increased ROMK channel activity and increased Na+/K+ pump activity
result is increased K+ secretion (and Na+ reabsorption)
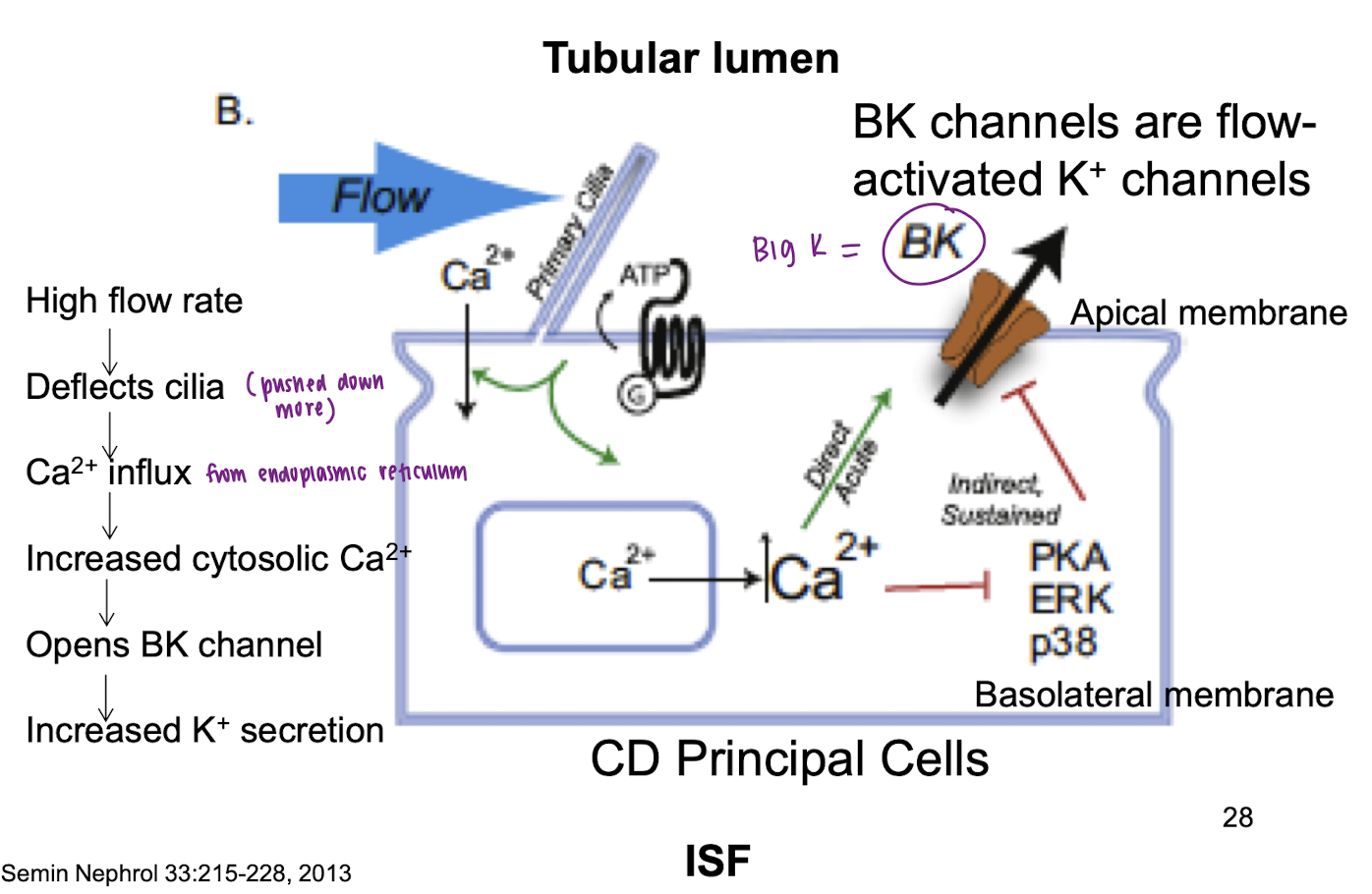
explain action mechanism of tubular flow rate on K+ secretion
high flow rate
deflects cilia
Ca+ influx
increased cytosolic Ca2+
opens BK (big K) channels
increased K+ secretion
how does flow rate also affect ROMK
increased sodium delivery typically occurs with increased tubular fluid flow → increased ENac activity → enhanced ROMK-mediated K+ secretion
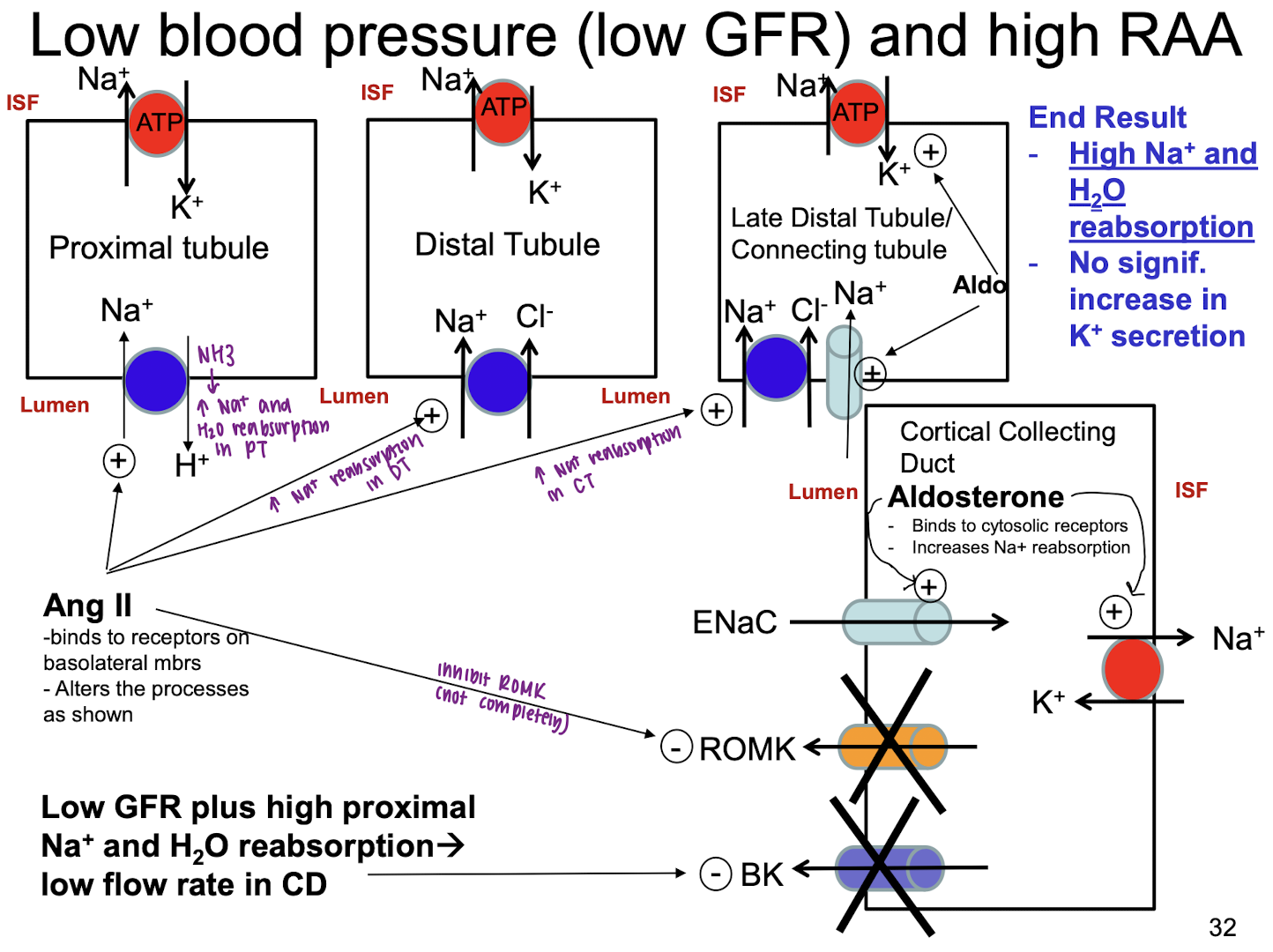
explain what happens when low MAP (low GFR) and high RAA (but K+ is normal)
Ang II stimulates Na+ reabsorption by proximal tubule → high Na+ and H2O retention
Aldo stimulates Na+ reabsorption in connecting tubule and CCD (via ENaC and Na/K ATPases) → high Na+ and H2O retention
Ang II inhibits ROMK in CCD → relatively less K+ secretion
low flow rate (due to low GFR and high Na+ and H2O reabsorption in CCD) → BK channels in CD are closed → reduced K+ secretion
explain what happens when High K+ and high aldo (but MAP is normal)
ang II is low → low reabsorption of Na+ and H2O in proximal and distal tubule → flow rate is higher
higher flow rate opens BK channels → high K+ secretion
aldo stimulates K+ secretion in CCD (ROMK and Na/K ATPases)
high K in ECF stimulates K+ secretion (ROMK and Na/K ATPases)
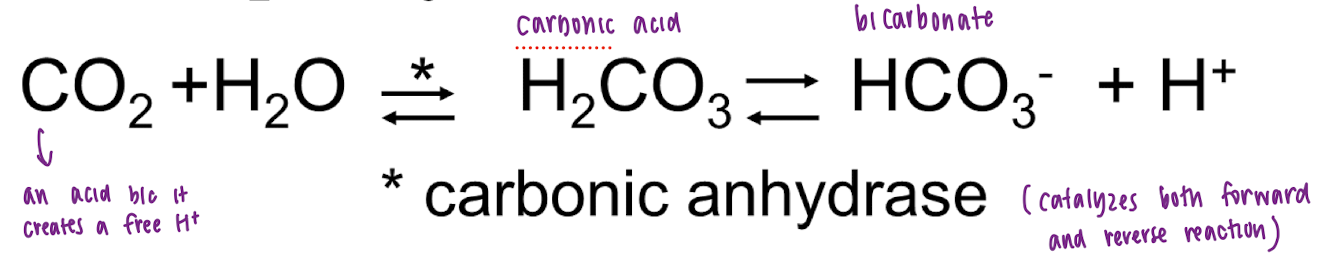
what is the CO2*HCO3- system
what is the major extracellular buffer
CO2*HCO3- system
what is the major intracellular buffer
phosphates and proteins
acidosis can develop if
H+ is added to the blood
HCO3- is removed from the blood
CO2 is added to the blood
alkalosis can develop if
H+ is removed from the blood
HCO3- is added to the blood
CO2 is removed from the blood
blood Pco2 changes have a significant impact on blood __ levels, but an insignificant impact on blood __ level
H+, HCO3-
if we get/lose 1 H+ and 1 HCO3-, then why does pH change
when Pco2 increases, [H]+ increases signficantly but [HCO3-] increases insignificant amount. so a Pco2 increase → a pH decrease
if increase HCO3-/Pco2, then _________
alkalosis
if decrease HCO3-/Pco2, then ________
acidosis
plasma Co2 is controlled by
the lungs (rapid)
plasma HCO3 is controlled by
the kidneys (slower)
what happens when HCO3 is excreted via kidney
renal excretion of HCO3- → gain of H+ → decreased ECF pH
what happens when new HCO3 is added by the kidney
renal addition of new HCO3- → lose H+ → increased ECF pH
explain the mechanism of reabsorption of filtered HCO3- at proximal tubule
H2O + CO2
carbonic anhydrase (CA)
H2CO3 splits into H+ and HCO3-
HCO3- added to ECF by facilitated diffusion and H+ is secreted by active transport into tubule lumen
secreted H+ combines with filtered bicarbonate to form H2O and CO2
H2O and CO2 diffuses back into the proximal tubule cells — so H+ not excreted