Applied: Local Anaesthesia
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
CNV branches
V1 - opthalmic nerve
V2 - maxillary nerve
V3 - mandibular nerve
Where does the Opthalmic Nerve V1 exit?
superior orbital fissure
Where does the Maxillary Nerve V2 exit?
Foramen rotundum
Where does the Mandibular Nerve V3 exit?
Foramen ovale
Pterygopalatine nerves of CN5 maxillary division
nasopalatine
greater palatine
lesser palatine
Infraorbital nerves of CN5 maxillary division
posterior superior alveolar
middle superior alveolar
anterior superior alveolar
What does the nasopalatine nerve supply?
palatal mucosa, gingivae, and alveolar bone anteriorly behind 2 1/1 2
What does the greater palatine nerve supply?
palatal mucosa, palatal alveolar bone and gingivae of the posterior region - 8 7 6 5 4 3/3 4 5 6 7 8
What does the lesser palatine nerve supply?
mucous membrane of the soft palate
What does the posterior superior alveolar nerve supply?
buccal mucosa, gingivae, alveolar bone, and PDL of 8 7 6/6 7 8 (may not supply MB root of 6/6)
maxillary sinus lining
What does the middle superior alveolar nerve supply?
buccal mucosa, gingivae, alveolar bone, and PDL of MB root of 6/6 and 5 4/4 5
maxillary sinus lining
What does the anterior superior alveolar nerve supply?
buccal mucosa, gingivae, alveolar bone, and PDL of 3 2 1/1 2 3
maxillary sinus lining
Anterior trunk nerves of CNV mandibular division
buccal nerve (sensory)
multiple motor nerves to muscles
Posterior trunk nerves of CNV mandibular division
auriculotemporal nerve (sensory)
lingual nerve (sensory)
inferior alveolar nerve (sensory and motor)
What does the buccal nerve supply?
cheek, mucous membrane of buccal sulcus and buccal gingivae
What does the lingual nerve supply?
lingual gingivae and lingual alveolar bone adjacent to lower teeth, floor of mouth, sensation to anterior 2/3 of tongue
What does the inferior alveolar nerve supply?
all lower teeth
incisive nerve supplies lower anterior teeth
mental nerve supplies labial gingivae and labial alveolar bone of anterior teeth, buccal gingiva and mucosa of the premolars, skin and mucosa of lower lip of chin
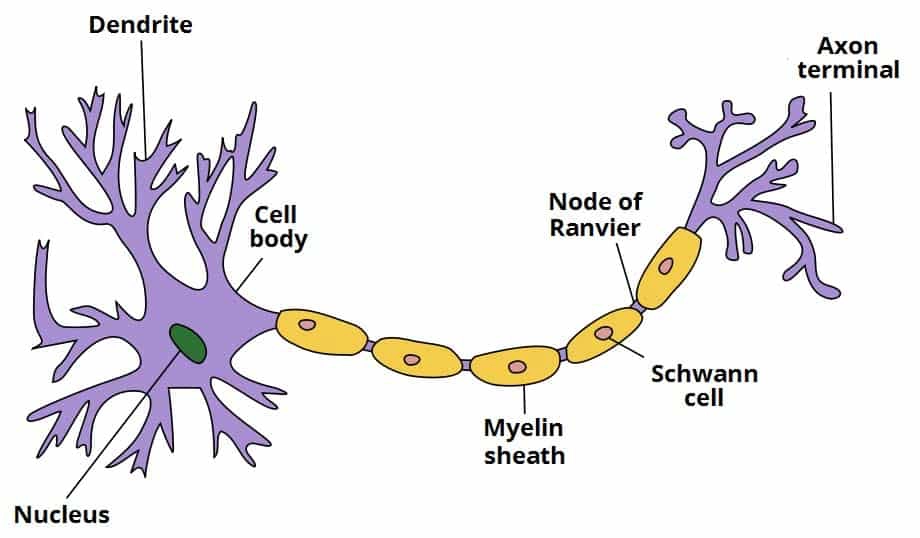
components of a nerve cell
cell body
dendrites
axon
myelin sheath
Define ‘Action Potential’
a sudden, fast, transitory, and propagatingg change of the resting membrane potential
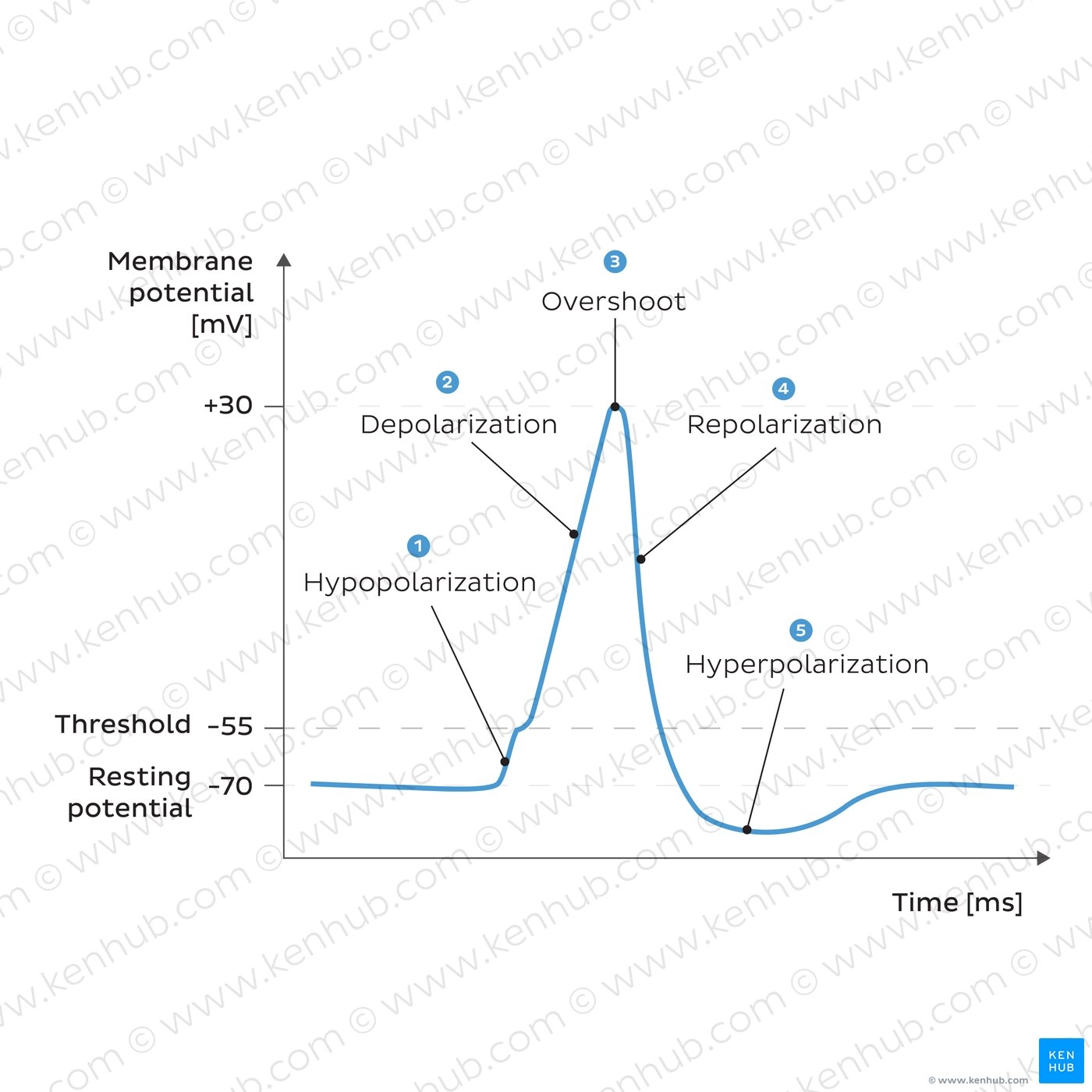
Describe the Hypopolarisation phase
initial increase of the membrane potential to the value of the threshold potential
the threshold potential opens voltage-gated Na channels and causes a large influx of Na ions
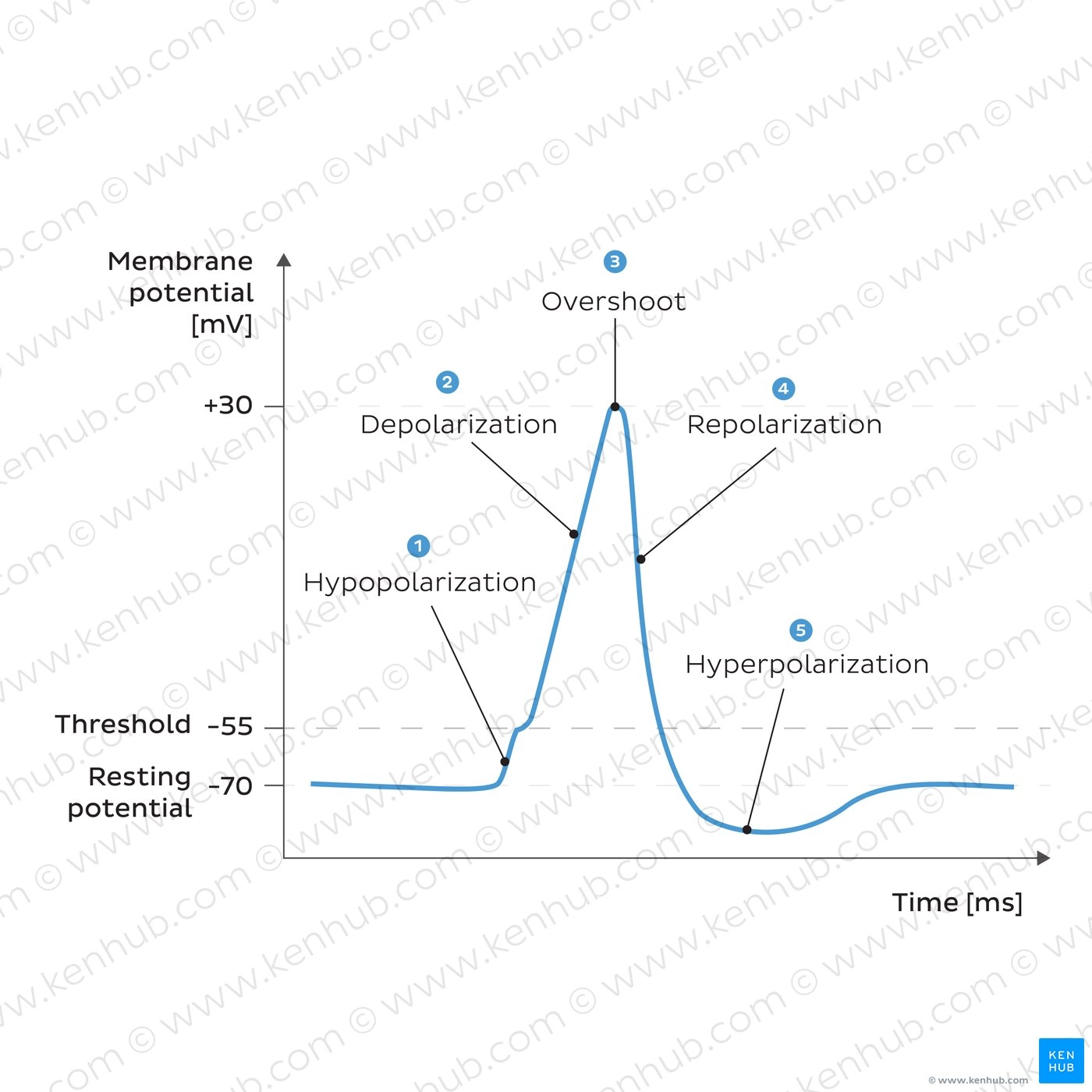
Describe the Depolarisation phase
the inside of the cell becomes more and more electropositive due to influx of Na+, until the potential gets closer to the electrochemical equilibrium for Na
this phase of extreme positivity is the overshoot phase
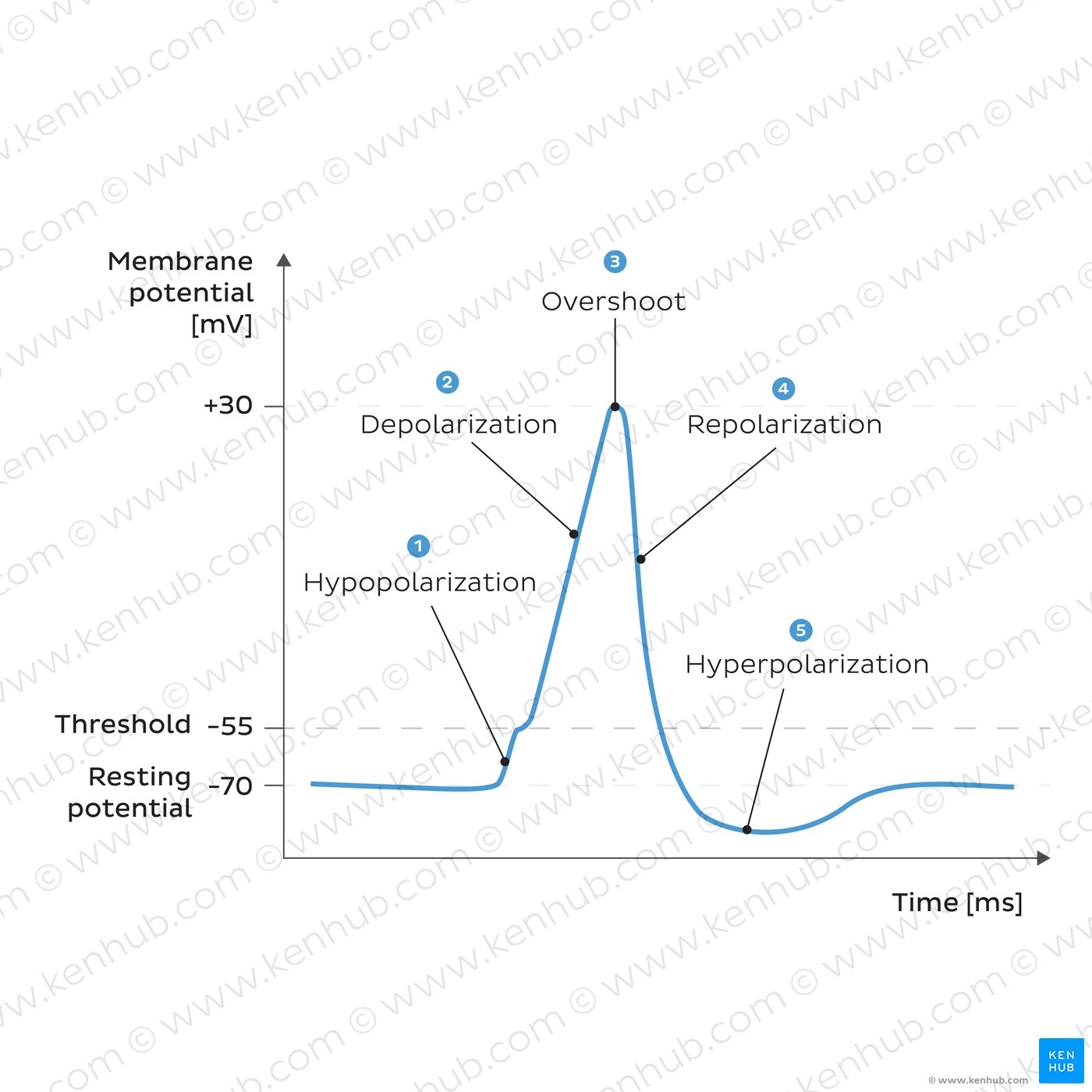
Describe the Repolarisation phase
Na permeability suddenly decreases due to the closing of its channels
the overshoot value of the cell potential opens voltage-gated K channels - large K+ efflux decreases cell’s electropositivity
repolarisation phase has purpose of restoring resting membrane
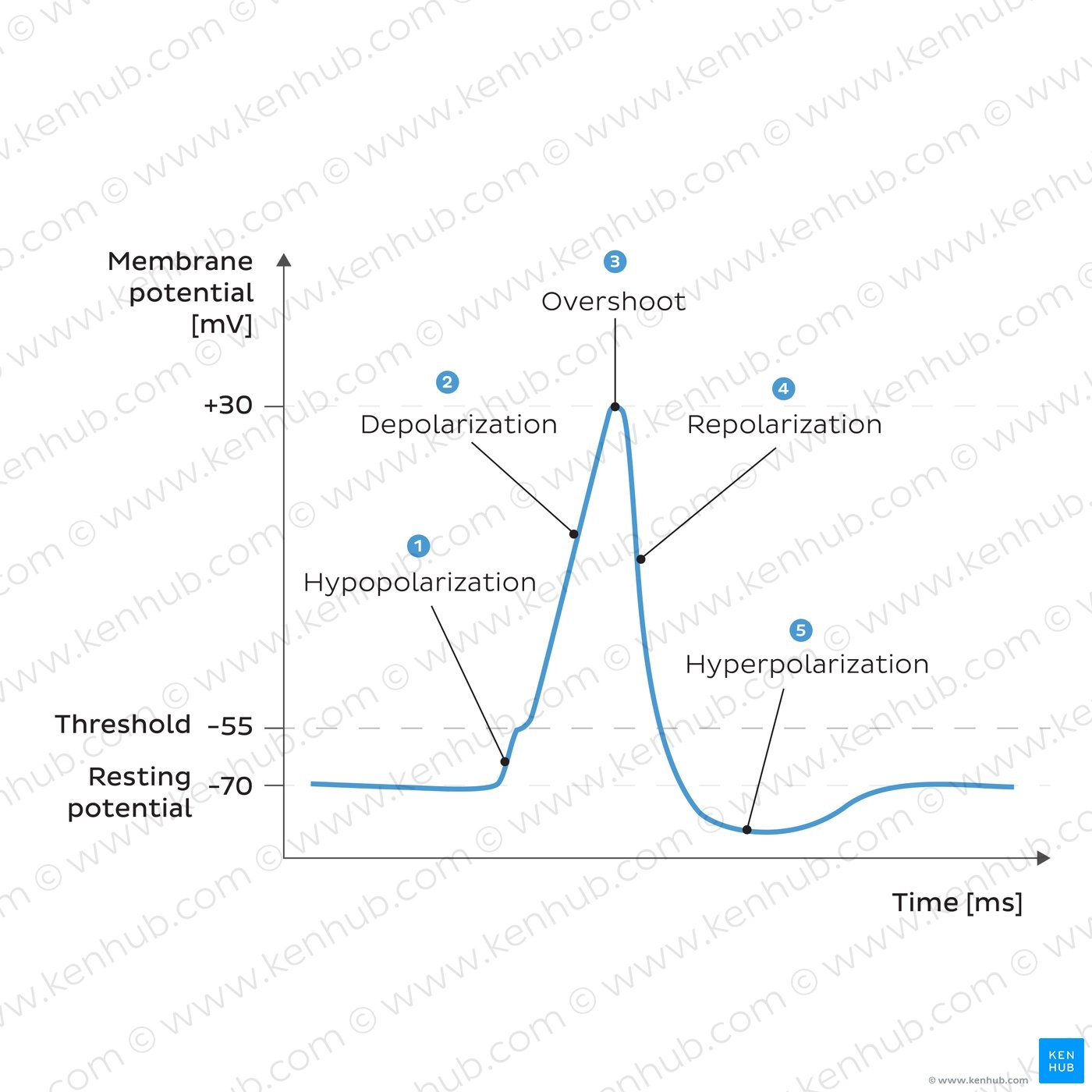
Describe the Hyperpolarisation phase
membrane potential is more negative than resting membrane potential
membrane will eventually establish again the values of membrane potential
Describe the Absolute Refractory Period
occurs once the sodium channels close after an AP
sodium channels then enter an inactive state during which they cannot be reopened, regardless of the membrane potential
Describe the Relative Refractory Period
occurs when sodium channels slowly come out of inactivation
the neurone can be excited with stronger stimuli than the one normally needed to initiate an AP
early on in the relative refractory period, the strength of the stimulus required is very high
gradually, the required stimulus strength becomes smaller as more sodium channels recover from inactivation
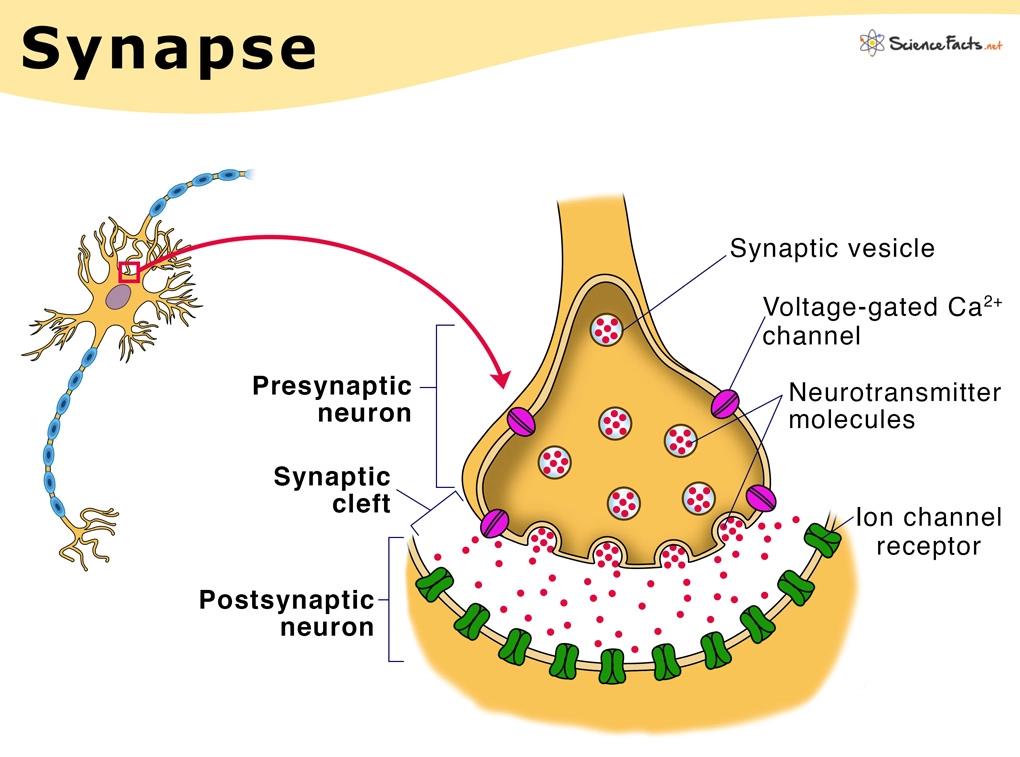
Define ‘Synapse’
gap between two neurones
Describe the process of neurotransmission across the synapse
AP arrives at synaptic knob and depolarises presynaptic membrane
voltage-gated Ca2+ channels open - influx of Ca2+ ions
influx causes vesticles containing various neurotransmitters to move and fuse with presynaptic membrane
exocytosis of neurotransmitters which diffuse across synaptic cleft
neurotransmitters bind to specific receptors on postsynaptic membrane
binding causes Na channels to open - influx of Na+ ions
depolarisation of postsynaptic membrane - AP is sent down axon once threshold for AP is reached
when the presynaptic membrane is no longer depolarised, neurotransmitters bound to receptors are broken down by a specific enzyme and the products are recycled
Draw the basic structure of an LA agent
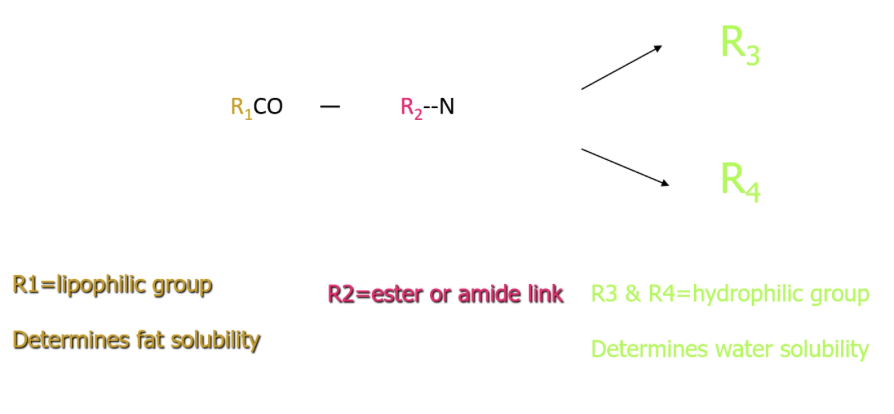
Which group in an LA agent determines its fat solubility?
R1 - lipophilic group
Which group in an LA agent determines its water solubility?
R3 and R4 - hydrophilic group
Describe LA agents which have their lipophilic form predominating
unionised
more fat soluble
diffuse through lipid bilayer
Describe LA agents which have their hydrophilic form predominating
ionised
less fat soluble
reduced diffusion through lipid bilayer
How to determine if an LA agent is more lipophilic or hydrophilic
Local anaesthetics are weak bases, so their form depends on pKa relative to physiological pH (~7.4):
Lower pKa (closer to 7.4)
→ more non-ionised (lipophilic) form
→ crosses membranes easilyHigher pKa
→ more ionised (hydrophilic) form
→ crosses membranes less easily
2 main theories for LA action
Membrane Expansion Theory
Specific Binding Theory
Describe the Membrane Expansion Theory
1. Anaesthetic enters the membrane
Anaesthetic molecules are lipid-soluble
They insert themselves between phospholipids in the membrane
2. Membrane expands and becomes more fluid
This causes:
Increased membrane volume (expansion)
Increased fluidity
Slight thickening/disordering of the bilayer
3. Ion channel function is disrupted
Membrane proteins (like ion channels) rely on precise structure
Expansion alters their:
Shape
Conformation
Ability to open/close properly
➡ Especially affects ion movement (Na⁺, K⁺, Ca²⁺)
4. Nerve signalling is impaired
Ion channels don’t function normally
Action potentials cannot be generated or propagated effectively
➡ Leads to loss of sensation / anaesthesia
Describe the Specific Binding Theory
1. Anaesthetic binds to target proteins
The drug binds to specific sites on:
Ion channels
Neurotransmitter receptors
This binding is selective and reversible.
2. Alters ion channel/receptor function
This can happen in two main ways:
🔹 Enhance inhibition
Increase activity of inhibitory pathways
Example: potentiation of GABA_A receptor
➡ More Cl⁻ enters neurons → hyperpolarisation → reduced excitability
🔹 Reduce excitation
Inhibit excitatory receptors or channels
➡ Less depolarisation
3. Suppresses neuronal activity
Reduced ability to generate and transmit action potentials
Leads to:
Loss of consciousness (general anaesthetics)
Loss of sensation (depending on site)
Properties of an ideal local anaesthetic
have a reversible action
non-irritant and non-damaging to tissues
rapid onset and appropriate duration
effective in concentrations that are not harmful
chemically stable in solution
adequate shelf life
Examples of LA agents that are amides
articaine
bupivicaine
lidocaine
mepivicaine
prilocaine
Examples of LA agents that are esters
benzocaine
cocaine
procaine
amethocaine
Proprietary name of Lidocaine/lignocaine
lignospan
xylocaine
xylotox
lignostab
Preparation of Lidocaine
2% lidocaine with 1:80,000 epinephrine
Proprietary name of Prilocaine
citanest
When is Prilocaine popularly used?
When patients cannot have adrenaline as their vasoconstrctor
Preparation of Prilocaine
prilocaine 3% with felypressin
prilocaine 4% plain (no vasoconstrictor)
Why can Prilocaine not be administered to pregnant people?
vasoconstrictor (felypressin) is similar to a labour-inducing hormone - prilocaine plain is okay to administer
Proprietary name of Mepivicaine
Scandonest
When is Mepivicaine popularly used?
shorter duration - popularly used for short duration procedures
Preparation of Mepivicaine
Mepivicaine 2% with 1:100,000 epinephrine
Mepivicaine 3% plain
Proprietary name of Articaine
Septanest
Preparation of Articaine
4% articaine with 1:100,000 or 1:120,000 epinephrine
Constituents of an LA cartridge
active anaesthetic agent
vasoconstrictor
reducing agent - prevent oxidation of vasoconstrictor
preservative
fungicide
vehicle - sodium chloride, sodium hydrochloride, water
Why are vasoconstrictors used in local anaesthetic?
LAs cause vascular dilation which would take away the agent more freely
prolongs duration of pulpal anaesthesia
allows for more profound anaesthesia
reduces local blood flow and hence bleeding
reduces toxicity; slows rate of absorption (minor effect)
Types of vasoconstrictors
epinephrine (adrenaline)
felypressin (octapressin)
Describe epinephrine as a vasoconstrictor
naturally occurring hormone
acts on adrenoceptors in blood vessels
has direct and indirect effects on the heart
increases heart rate and force of contraction, therefore C.O, pulse and potentially systolic BP
standard LA doses have little effect
affects a number of the systems
never use at extremities (ischaemia)
Describe felypressin as a vasoonstrictor
synthetic
analogue of vasopressin (labour induction)
no effect on the heart
less vasoconstrictor effect
common conc in citanest: 0.03 units per ml
When should using LA containing epinephrine be avoided?
unstable/severe hypertension or angina
unstable cardiac rhythm
Duration of action of Lidocaine 2% (with epinephrine)
Pulpal: 60 (infil) - 90 (block) mins
Soft tissue: 2.5-3hrs
Duration of action of Prilocaine 3% (with felypressin)
Pulpal: 60 (infil) - 90 (block) mins
Soft tissue: 2.5-3hrs
Duration of action of Prilocaine 4% Plain
Pulpal: 10mins (infil), 50mins (block)
Soft tissue: 2-3hrs
Duration of action of Mepivicaine 3%
Pulpal: 30 mins
Soft tissue: 2-3hrs
Duration of action of Articaine 4% (with epinephrine)
Pulpal: 60 (infil) - 90 (block) mins
Soft tissue: 2.5-3hrs
similar to Lidocaine has the ability to diffuse widely
Recommended maximum dose of Lidocaine 2%
4.4mg/kg
300mg
6.8 cartridges
Recommended maximum dose of Prilocaine 3%
6mg/kg
400mg
6 cartridges
Recommended maximum dose of Articaine 4%
7mg/kg
5 cartridges
General contraindications of using LA
uncooperative patient
hypersensitivity to LA
infection at injection site
absorption to blood stream may increase possibility of systemic side effects
altered local pH may decrease effect of LA
haemorrhagic disorders
anticoagulant therapy (depends on NR)
significantly reduced vascularity
severe liver dysfunction
severe renal dysfunction
Types of LA delivery
topical
infiltration
regional block
Systemic complications related to LA
vasovagal faint
drug interaction
adverse reaction to drug
psychogenic reaction
toxicity
Local complications related to using LA (excluding those related to ID blocks)
failure to achieve anaesthesia
prolonged anaesthesia and paraesthesia - trauma to nerve itself
bleeding at injection site
blanching at injection site - caused by intrarterial injections if blanching remains
needle and cartridge breakage
pain on injection
post-injection pain
trauma to blood vessel - haematoma
Local complications related to using LA specifically for ID blocks
restricted jaw opening (trismus)
facial palsy
visual disturbance (very rare)
blanching of skin in cheek area (rare)
What can cause pain on injection?
subperiosteal injection
injecting too quickly - liquid is being forced into area
touching nerve when giving ID block will translate to ‘electric shock’ - rapid anaesthesia
injecting large amounts into dense tissues
What can cause post-injection pain?
rapid injection
large volumes of LA
lip and cheek trauma
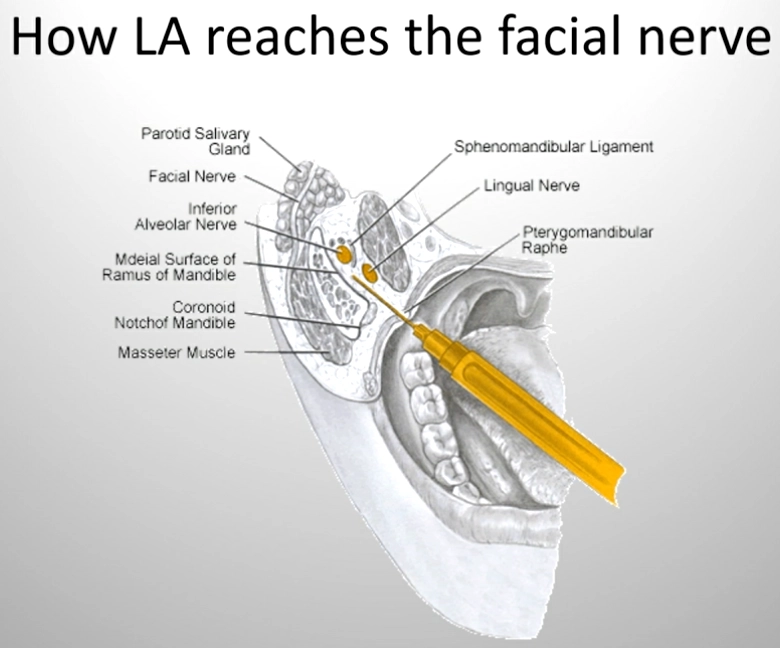
What causes temporary facial palsy after administering ID block?
incorrect placement of needle
penetration of parotid gland capsule during injection (facial nerve)
causes short duration paralysis of face
POI after temporary facial palsy
reassure pt that palsy will subside in a few hours
if pt cannot blink, offer eye patches or eye drops
offer pt to wait in reception until anaesthesia wears off for monitoring
Causes for LA failure
pharmaceutical reasons - expired/incorrect storage
poor technique/inappropriate placement
inadequate volume of LA
anatomical variation
injection into infected or inflamed area
patient anxiety
Nerve supply for upper teeth
upper teeth - maxillary nerve
posterior superior alveolar nerve - molars (and part of first molar)
middle superior alveolar nerve - premolars (sometimes first molar)
anterior superior alveolar nerve - incisors and canines
Nerve supply for lower teeth
lower teeth - mandibular nerve
mandibular nerve - main nerve
inferior alveolar nerve - travels through mandible to supply all lower teeth then gives off branches to incisors and canines
Nerve supply for buccal/labial gingivae
buccal nerve
Nerve supply for palatal gingivae
greater palatine nerve
Nerve supply for lingual gingivae
lingual nerve
Infiltration technique
Retract tissues taut to allow good visibility
place bevel towards tooth and insert needle at point of reflection of alveolar and vestibular mucosa
ensure needle is parallel to long axes of tooth and angle needle towards bone surface
advance needle forward (3-5mm) so that the needle tip is opposite the apex of tooth
aspirate, check cartridge
deliver solution at slow and steady pace
withdraw smoothly and rub area gently
Post-operative advice
avoid smoking
avoid hot foods and drinks
avoid biting cheek and lip
assure them that their face is not swollen and the numbness will pass in a few hours
give contact number for any concerns
Which teeth and surfaces does the IDN not cover?
mandibular incisors - cross-innervation
buccal gingiva of mandibular molars - long buccal nerve
lingual gingiva - depends on lingual nerve
Where should you aim to deposit the LA in an IDB?
as close to the mandibular foramen as possible
Height of injection in IDB
adults: approx 1cm above the occlusal surfaces of the molars
children: approx 0.5cm above the occlusal plane
very young children: approx the height of the occlusal plane
Key landmarks for IDB
external oblique ridge
coronoid notch
pterygomandibular raphe
IDB Technique
position patient and position of mandibular foramen estimated using landmarks
parallel to occlusal plane, approx 1cm above occlusal surfaces of molars
place thumb of opposing hand onto external oblique ridge (at anterior aspect of ascending ramus) - do not move
roll tip of thumb forward onto coronoid notch
identify pterygomandibular raphae (attached to internal oblique ridge)
buccinator muscle and the superior constrictor muscle of the pharynx
insert needle from left side of mouth with syringe barrel lying across contralateral premolars (direct technique)
needle enters tissues at midpoint of tip of palpating finger or thumb (about 0.5cm medial to it) and lateral to pterygomandibular raphe
insert slowly until bone is contacted (about 2-2.5cm) and then withdraw ~1mm (prevents subperiosteal injection) and aspirate
slowly deposit almost a full cartridge
deposit remaining 0.5ml solution as you pull out - anaesthetise lingual nerve
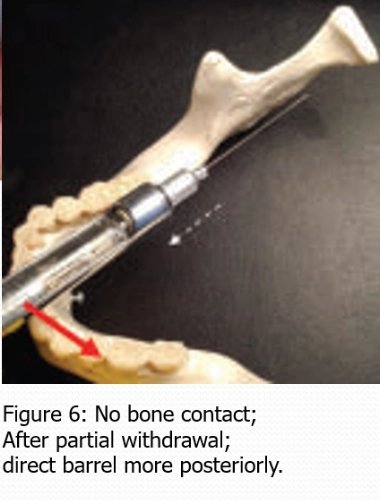
Common positioning mistakes when administering IDB
inject too posteriorly - early bone contact
inject too anteriorly - no bone contact
Importance of aspiration
prevent intravascular injection:
avoids systemic toxicity - dizziness, increased heart rate, tinnitus
prevents failed anaesthesia - LA is taken away in blood quicker
less risk of haematoma formation