Week 1_Prescriptions, Drug Approval, Pharm basics, Receptor theory, Pharmacokinetics
1/65
Earn XP
Description and Tags
Week 1 lectures
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
66 Terms
Which federal institution determines what is a prescription drug and what isn’t?
The Food and Drug Administration (FDA)
Describe an over the counter drug
can be safely self-administered by the layman
instructions are on the package must be written for lay comprehension
they have been deemed safe enough to allow consumers to make educated decisions about their own use
these are still considered drugs
Describe a prescription
mechanisms to ensure the practitioner and patient get what is desired and agreed to
it represents the end of a diagnostic process
What are the 3 types of prescriptions?
prescriber’s order for the patient’s chart or MR
written order pharmacist refers to
patient’s medication container
What is the importance of the Federal Comprehensive Drug Abuse Prevention and Control Act of 1970?
aka the Controlled Drug Act
regulates the manufacture, distribution and sale of certain chemicals identified as controlled substances and penalties for misuse
enforcement was entrusted to the Drug Enforcement Administration (DEA)
Describe a Schedule I drug and give examples
controlled substance with no accepted medical use and has a high potential for abuse
heroin, lysergic diethylamide (LSD), marijuana, peyote, methaqualone, and certain fentanyl
Describe a Schedule II drug and give examples
controlled substance with high potential for abuse with severe psychological or physical dependence, but accepted medical use
morphine, methadone, cocaine, amphetamine (Adderall), methylphenidate (Ritalin)
What are some special prescribing concerns for schedule II drugs?
valid to provide the pharmacy a script up to 14 days
provider must see patient to prescribe
no refills
street address of patient must match ID
warning label required due to abuse potential, caution on drug interactions, sedation likelihood
some states restrict who can prescribe
Describe a Schedule III drug and give examples
abuse potential is present and dependence liability is less then C1 and C2, accepted medical use
anabolic steroids, Dronabinol (synthetic THC), codeine with acetaminophen
Describe a Schedule IV (4) drug and give examples
abuse potential and dependence liability less than C3 and accepted medical use
diazepam (Valium), lorazepam (Ativan), alprazolam (Xanax), lorcaserin (Belviq)
Benzos and sleep meds
Describe a Schedule V drug and give examples
abuse potential and dependence liability less than C4 with accepted medical use
cough medications with codeine, antidiarrheal with low dose of opiates (Lomotil), pregabalin (Lyrica) and some analgesics
_______ prohibited mislabeling and adulteration of drugs
occurred because what was in the prescription bottle was different than the label
Federal Pure Food and Drug Act of 1906 (FDA)
_______ required new drugs to be safe as well as pure BUT did not require proof of efficacy
Food, Drug, and Cosmetic Act 1938
_______ required proof of drug efficacy as well as safety for new drugs and for drugs released since 1938
this established guidelines for reporting information about adverse reactions, clinical testing, and advertising new drugs with warnings at the end of the ad
Kefauver-Harris Amendent 1962
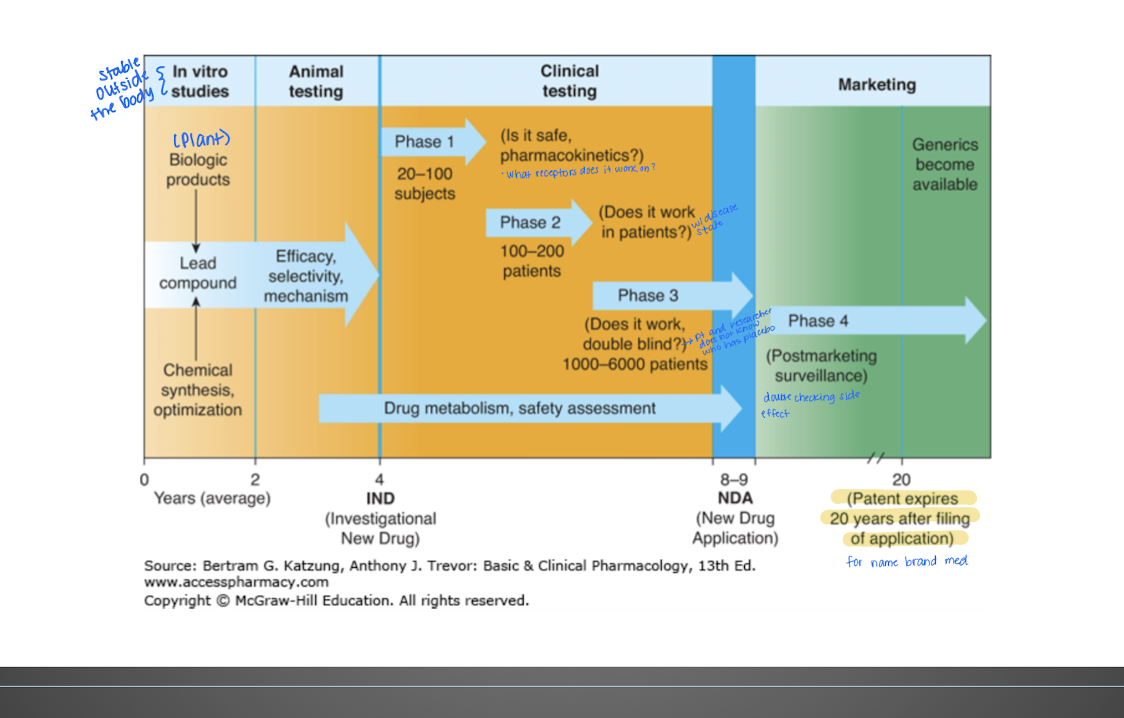
Describe each phase of approval for a new drug:
Pre-Clinical
Phase 1
Phase 2
Phase 3
Phase 4
Researchers look for the best delivery system (topical, inhaled, oral); includes animal testing (in vitro testing)
Drug is tested in small number of patients with the targeted disease )20-80 pts); first in human trials to test safety, dosage, and pharmacokinetics
Researchers look for the best delivery system (topical, inhaled, oral); testing effectiveness; dose finding (10 mg vs 20 mg); 25% move to phase 3
Get FDA approval; multisite trial; thousands of patients to confirm safety and efficacy
Companies look for additional applications for the drug beyond what is was originally used for (post marketing surveillance)
Which clinical phase was usually open label (non-blinded - for patients)?
Clinical phase
which clinical phase is usually single-blinded with a control
Phase 2
which phase is double-blind, crossover?
phase 3
T/F: compounded drugs do not go through clinical phases
true
caution is always recommended because the actual concentrated drug is regulated but not all tests are administered: potency, safety, and efficacy
The study of substances that interact with living systems through chemical processes, especially by binding to regulatory molecules and activating or inhibiting normal body processes
Pharmacology
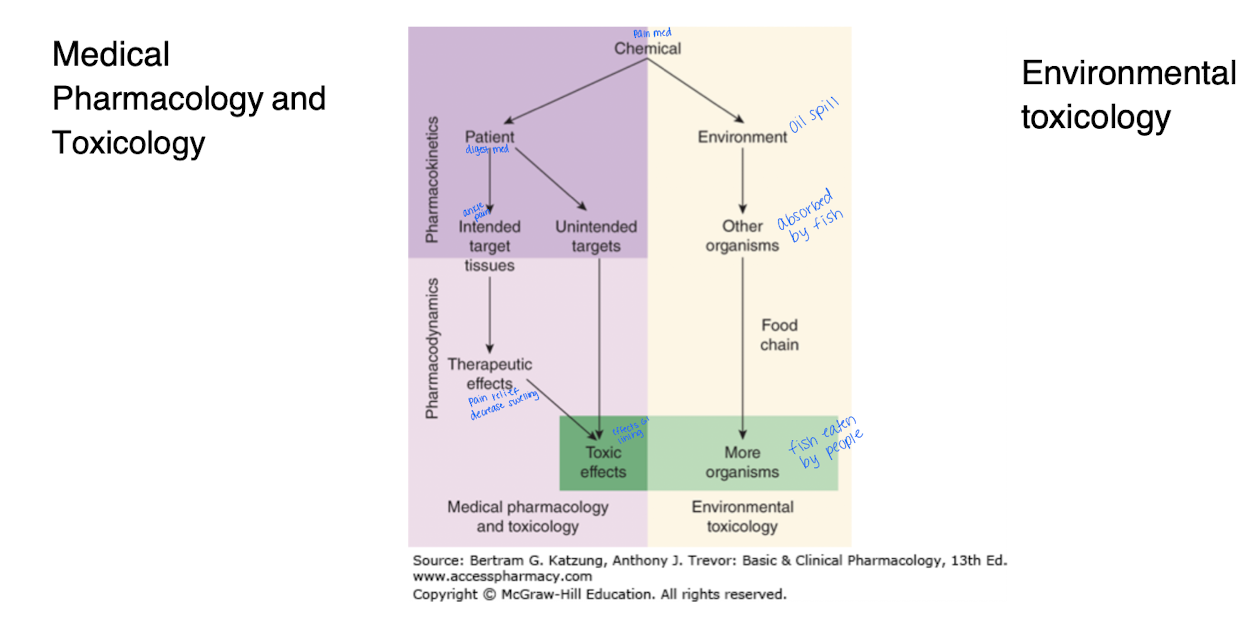
Explain the difference between Medical pharmacology and toxicology
Medical Pharm - the study of medications and their therapeutic or desired effects; science of substances used to prevent, diagnose, and treat disease
Toxicology - the undesirable effects of chemicals on living systems; toxic at certain levels or concentrations
What are the 4 categories of the nature of drugs?
Physical nature
solid, liquid, gas (inhaled)
Drug size
large drugs can’t diffuse between body compartments and may need to be injected to get to the bloodstream (ex: vancomyocin (antibiotic))
Lipophillic vs hydrophillic
a drug needs to be lipophilic to cross the blood brain barrier
Routes of administration
oral, IV, sublingual, inhalation, topical
Agonist vs Antagonist
Agonist - induces response
Antagonist - inhibits response
Pharmacokinetics vs Pharmacodynamics
Pharmacokinetics is what the body does to the drug (ADME).
Pharmacodynamics is what the drug does to the body (agonist, antagonist(.
Describe what ADME stands for and is related to
Absorption (medication is broken down and absorbed into the bloodstream
Distribution
Metabolism (half-life)
Elimination or Excretion
all define Pharmacokinetics- the body does to the drug
Describe ligand-gated ion channels and when they are used
lipid soluble chemical (drug) crosses the plasma membrane and acts on the intercellular receptor (inside cell) (1)
for lipid soluble drugs (ex: steroid molecules)
some ligand gated channels will have the drug bind extracellular but elicit activity intracellularly (2 and 3 - enzyme in the ligand family)
Hydrophilic - process occurs within the plasma membrane
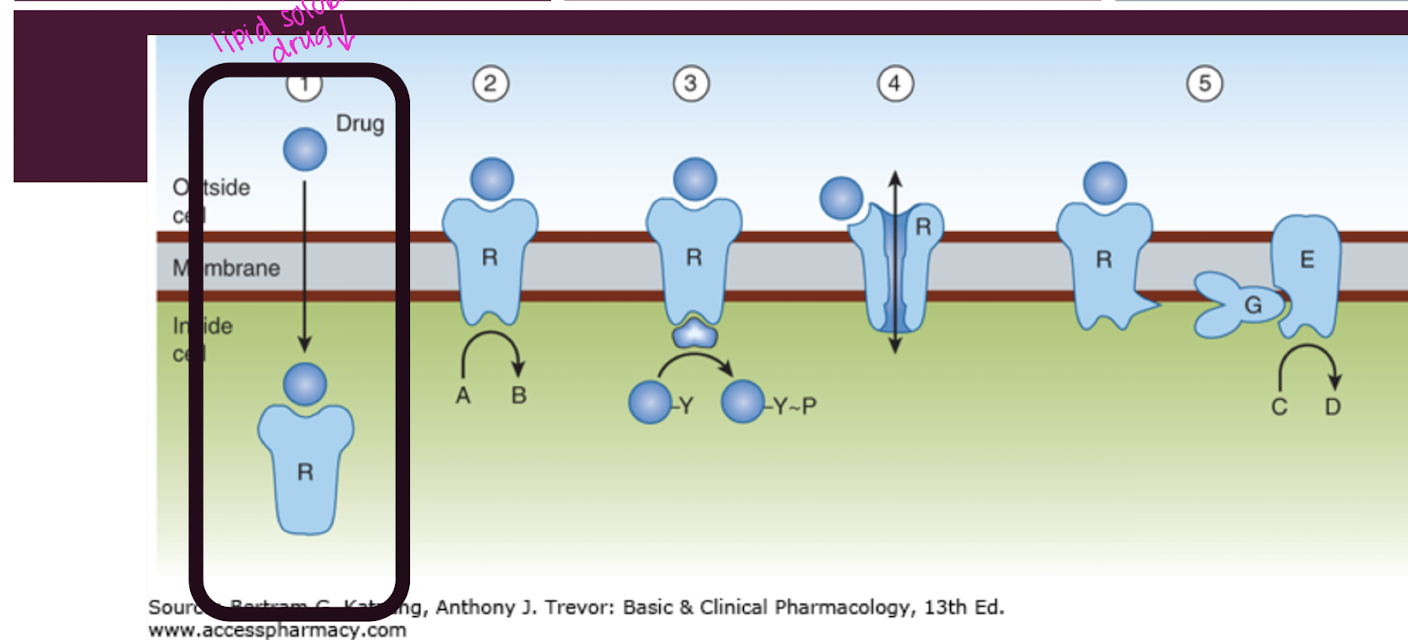
Describe Voltage gated channels
bind to allosteric site to open the VG channel. Molecules flow in and out based on the charge (4)
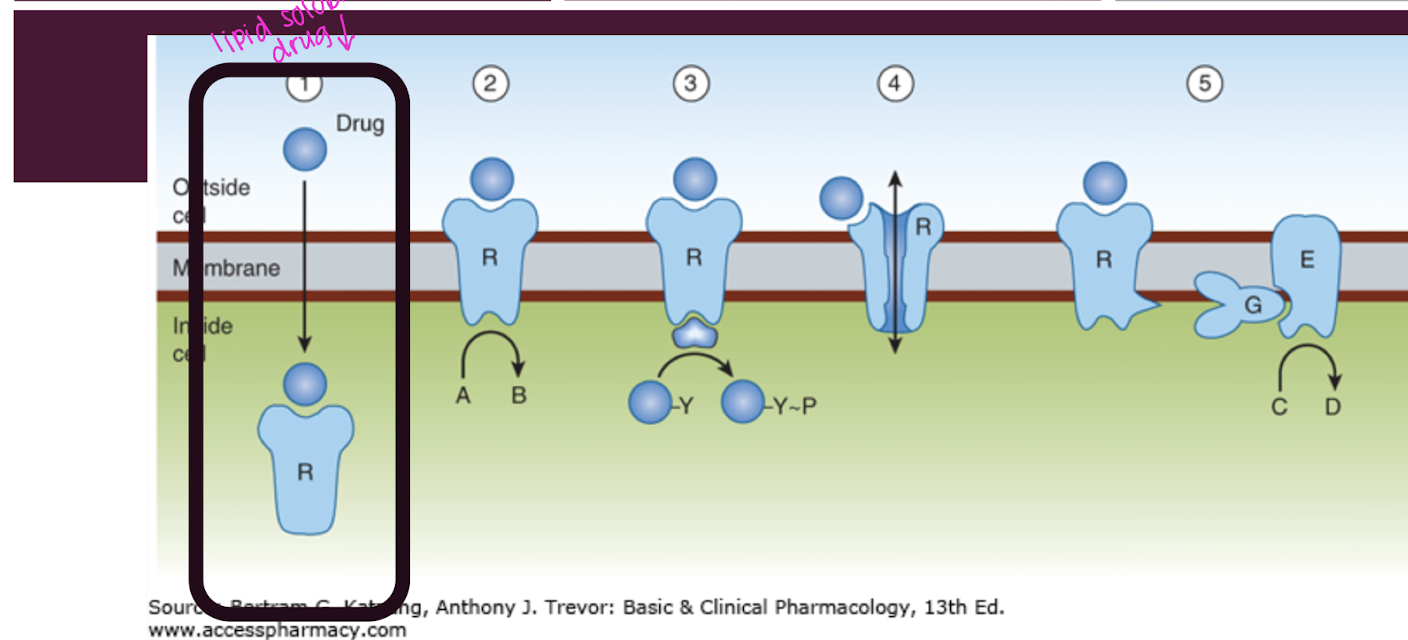
Describe G-coupled receptors
The G coupled receptor binds extracellularly to activate the G-protein. The receptor changes shape activating the G protein. The G protein will dissociate from the subunit and which stimulates creation of the secondary messenger that relays signals within the cell, influencing various physiological processes. (5)
Subunit is within the plasma membrane
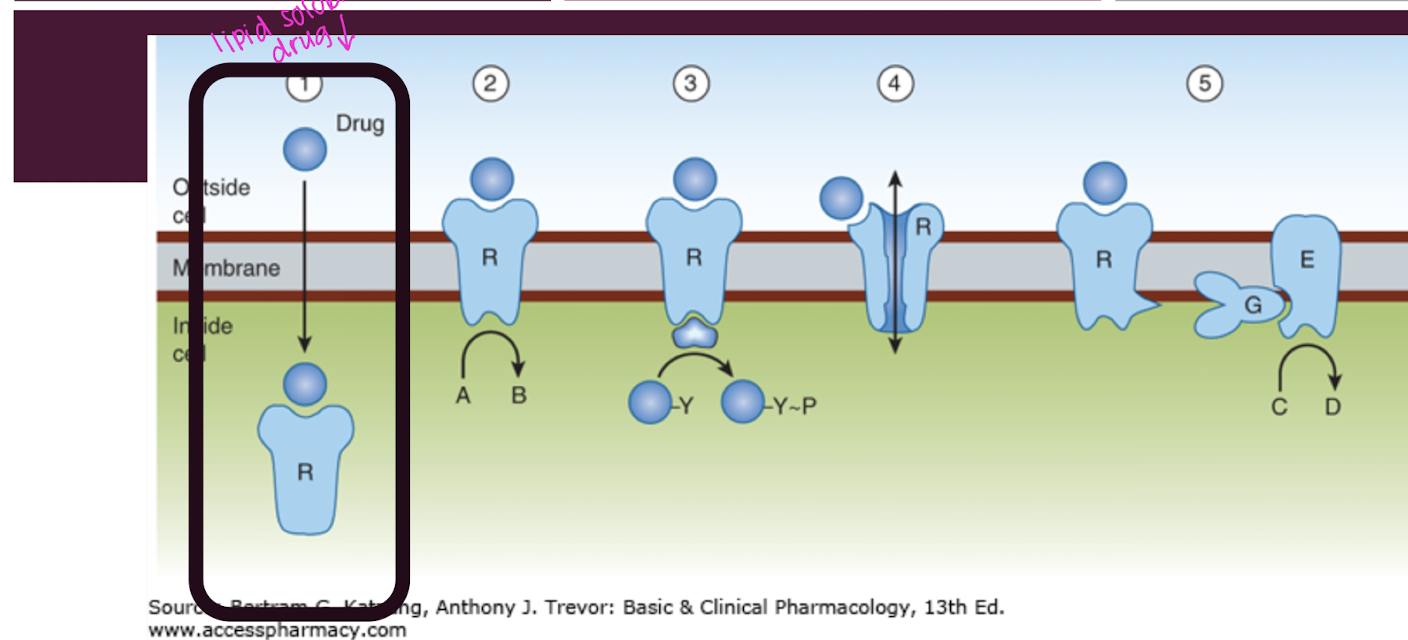
Describe enzyme linked receptors
On the cell surface (plasma membrane) and ligand are usually large and hydrophilic molecules (insulin, growth factors).
The ligand binds to the receptor’s extracellular domain and activates an intrinsic enzyme activity leading to phosphorylation cascades and signal transduction
This type of receptor, once bound by the ligand is able to reach the nucleus and alter gene expression (transcription)
Intracellular receptors (steroid receptors)
Receptor is below the plasma membrane in the cytoplasm or nucleus
What do ligand gated channels, G protein coupled receptors, Enzyme linked receptors and intracellular receptors have in common?
all have intracellular effects
A nicotinic acetylcholine receptor is an example of _______
a. voltage gated channel
b. ligand gated channel
c. G protein-coupled receptors
d. enzyme-linked receptor
b. ligand gated channel
embeded in the plasma membrane
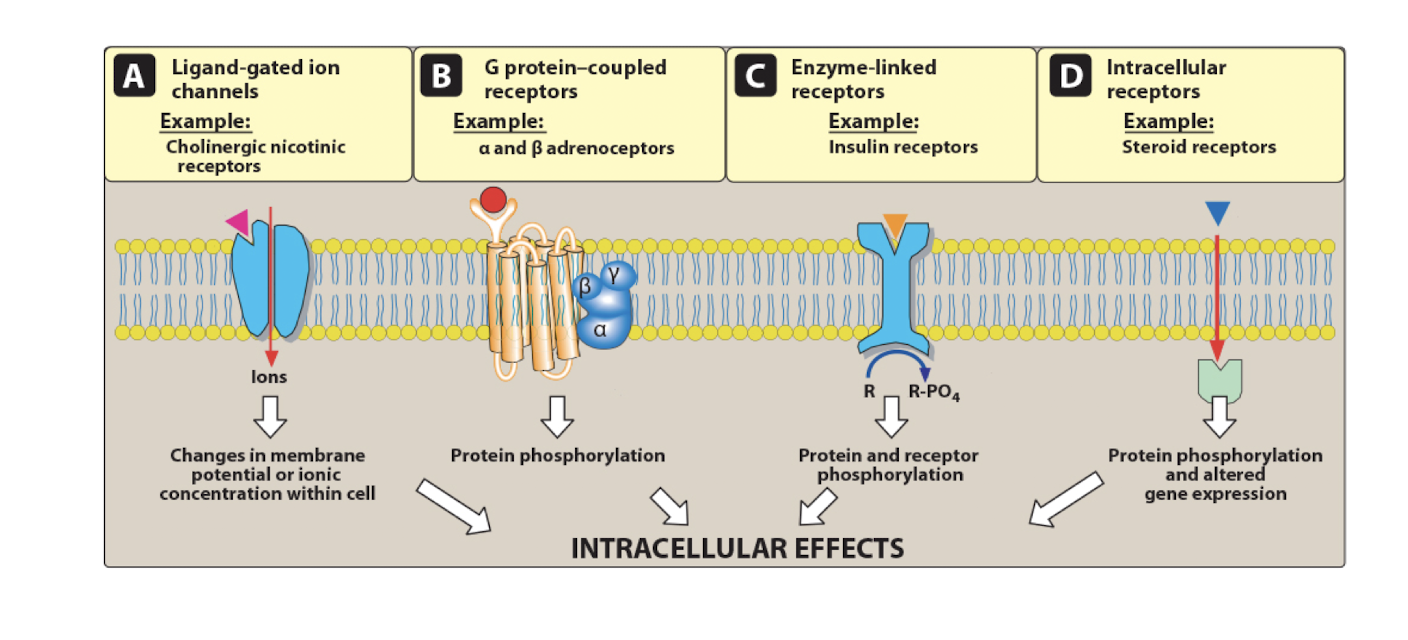
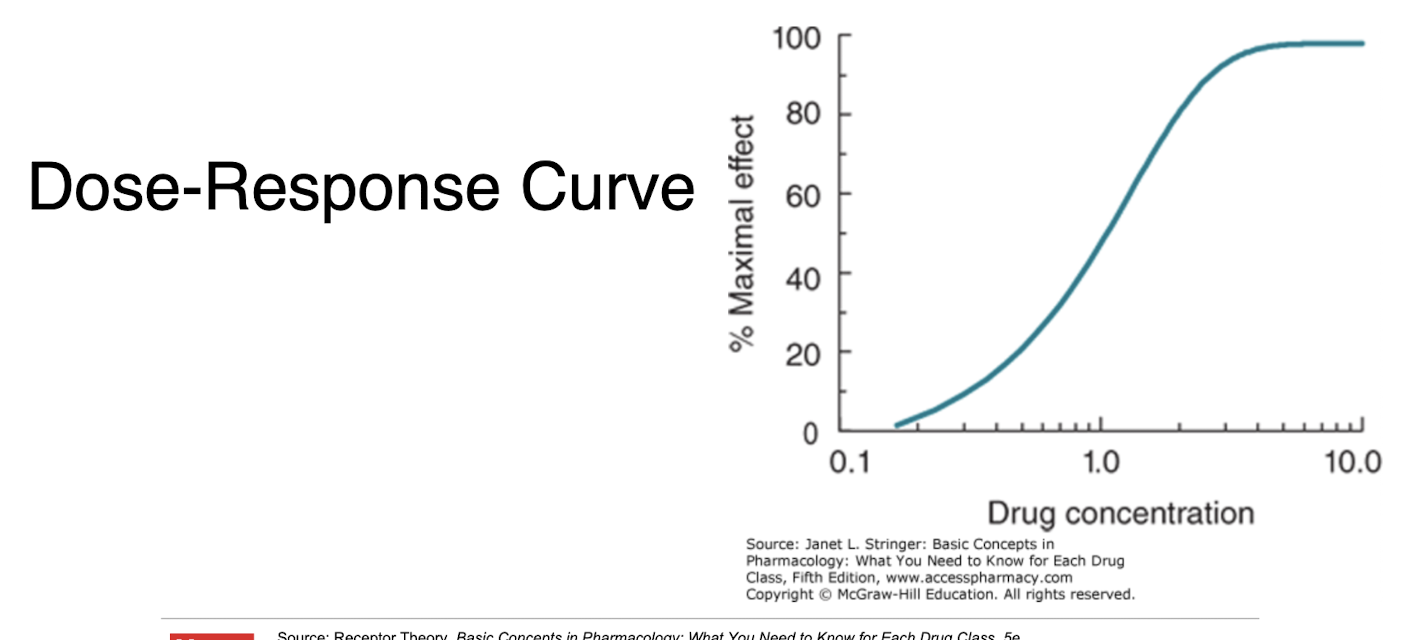
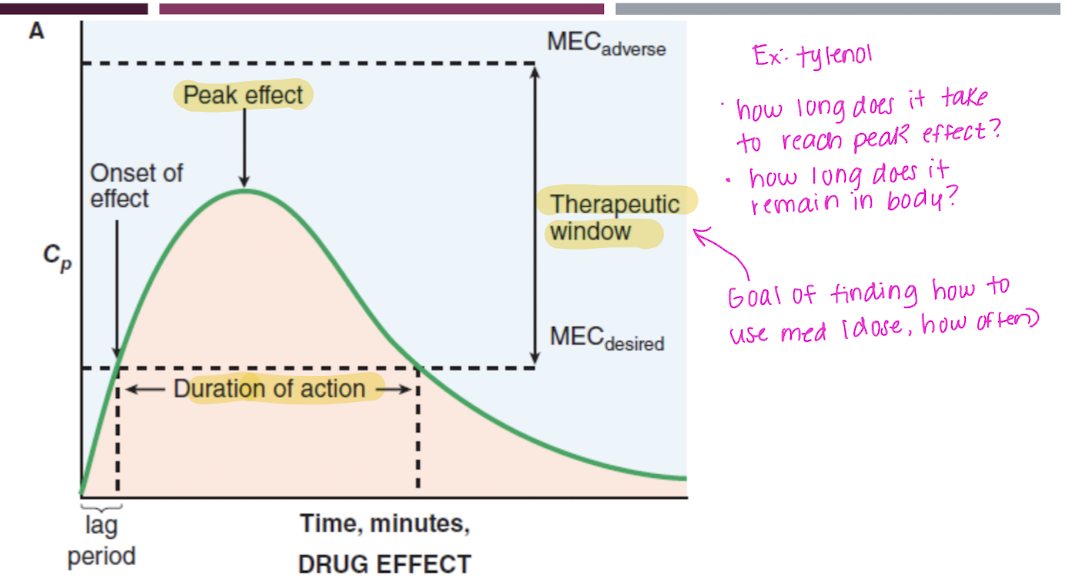
Explain the dose-response curve
A graphical representation showing the relationship between the dose of a drug and its pharmacological effect, indicating how varying doses can produce different levels of response.
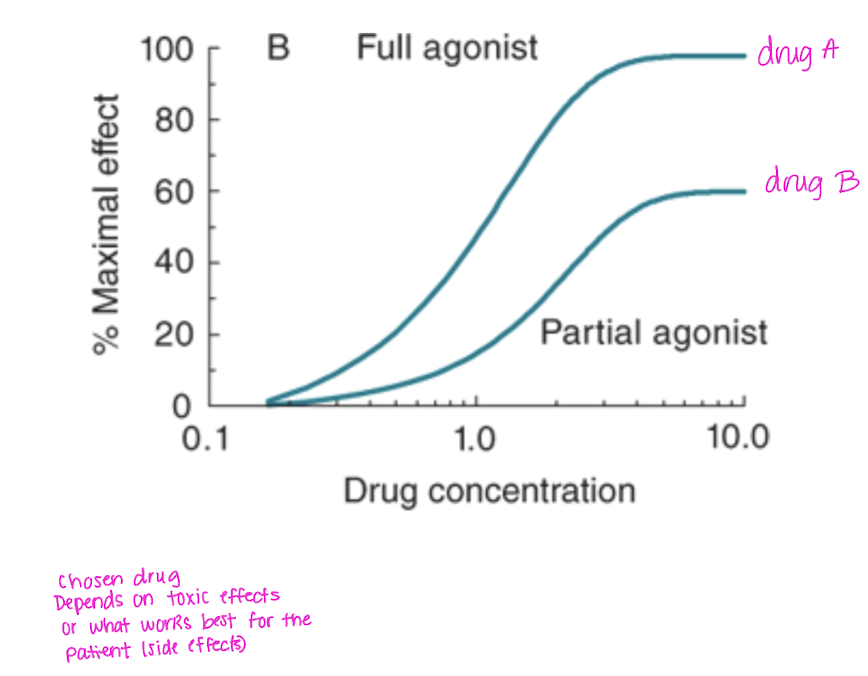
Efficacy vs potency
Efficacy - the maximum effect a drug can produce regardless of dose; activity; effectiveness
Potency - amount of drug needed to produce a given effect; affinity
Potency:
What is the Effective Concentration 50 (EC50), Effective Dose 50 (ED50)?
concentration or dose needed to elicit 50% the maximal response
it is a measure of potency
Potency:
What is Lethal concentration 50 (LC50), Lethal Dose 50 (LD50)?
Lethal in 50% of the test population; it is dose specific
Death
Potency:
What is toxic concentration 50 (TC50), Toxic Dose 50 (TD50)?
Toxic in 50% of the test population; not causing death
What is the therapeutic index?
The ratio of the toxic or lethal dose to the effective dose: LD50/ED50
A drug with a higher index is safer than one with a lower therapeutic index
It determines if a drug is worth it to administer by comparing safety to efficacy.
How does therapeutic index relate to therapeutic window?
Therapeutic index: A ratio that compares the toxic dose of a drug to its effective dose; numerical estimate of safety
Therapeutic window: the actual range of drug concentrations in the blood that gives efficacy without unacceptable toxicity; practical range used in patients
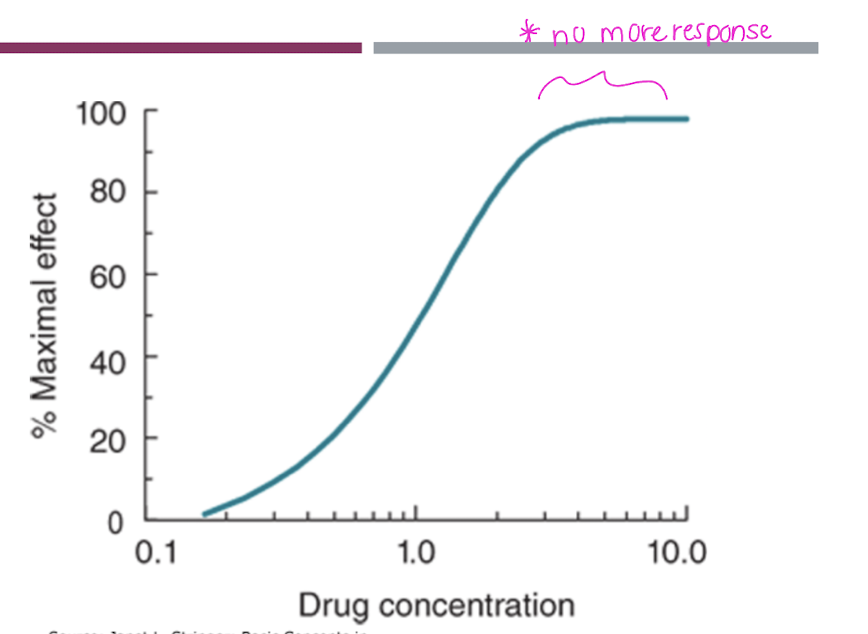
what relationship is seen between the ligand (drug molecule) and drug response in an agonist?
Increasing the concentration of the drug will increase the biologic response UNTIL no more receptors are available for the agonist to bind and or the max response is reached
what relationship is seen between the ligand (drug molecule) and drug response in a partial agonist?
Similar response as the agonist (ncreasing the concentration of the drug will increase the biologic response) BUT it will never produce 100% of the response even at very high doses
it is less efficacious than the full agonist
Explain when an agonist works alone versus an agonist and a competitive antagonist are working (ex: treating overdose)
An agonist works alone to activate receptors and produce a desired therapeutic effect, while the presence of a competitive antagonist blocks the agonist's action by occupying the same receptors (two keys fighting for a spot on the lock), reducing the overall response.
When the agonist and competitive antagonist are present the same maximal effect can be achieved by the agonist but it takes a higher dose
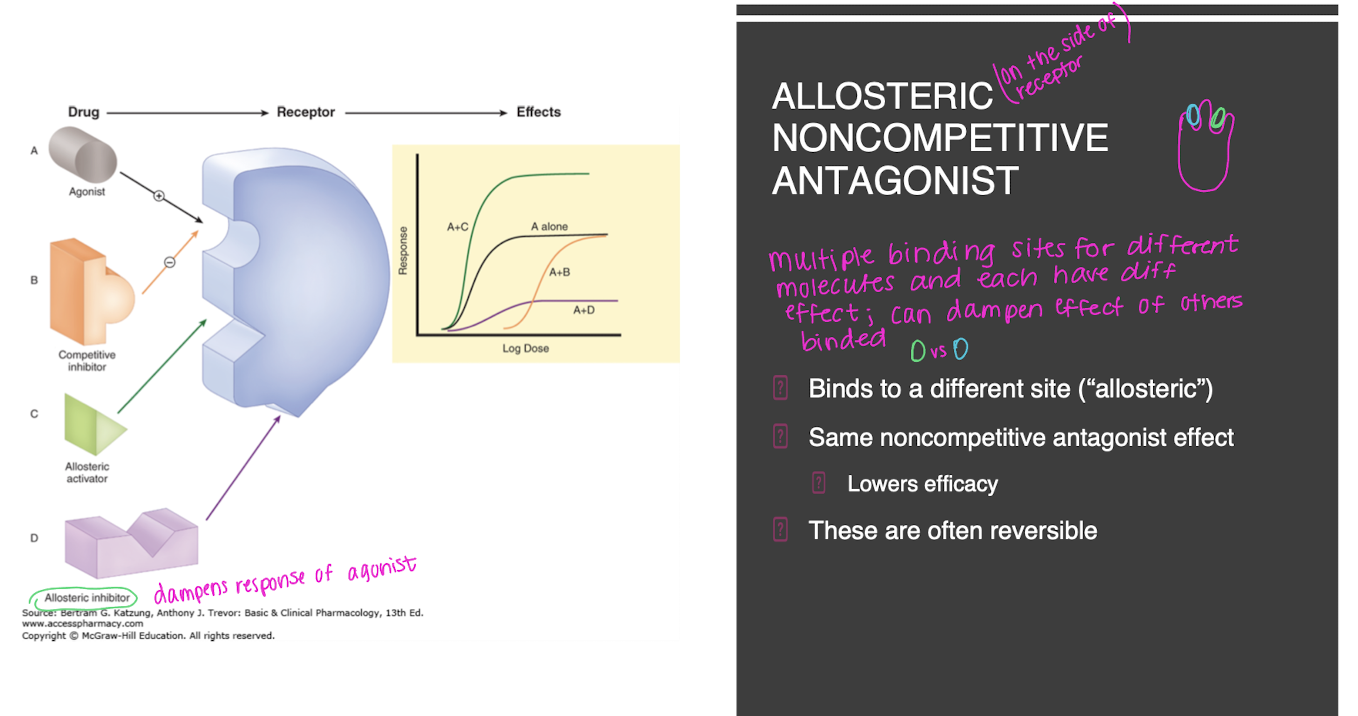
Explain a allosteric noncompetitive antagonist
allosteric means binding to a different site
it has the same noncompetitive antagonist effect (lowers efficiacy)
often reversible
multiple binding sites for different molecules and each have different effect and can dampen effect of others that are binded
Explain non-competitive antagonism
agonist and antagonist can be bound simultaneously, but antagonist binding reduces or prevents the action of the agonist
same binding site can “bump” in and out
What are spare receptors?
Spare receptors are those that exist in excess over what is necessary to elicit a maximal biological response. They are not all needed for full activation, allowing for greater sensitivity to agonists.
2 of 20 receptors can be activated and have same effect as 20 of 20 activated
the excess that are activated enhance the ability of tissue to detect and respond to low concentrations of agonists
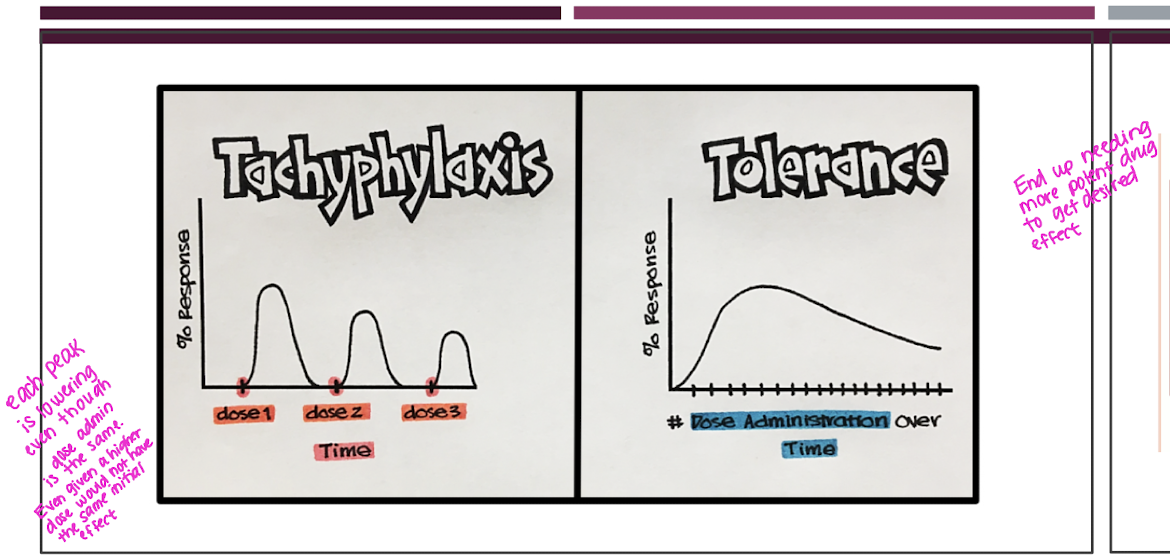
Compare Tachyphylaxis to tolerance
Tachyphylaxis - a rapid decrease in the response to a drug after repeated administration in a short period of time due to receptor desensitization, depletion or neurotransmitters or mediators, or physiological adaptation (body opposes drug effects)
develops slowly
Tolerance is when a drug had theraputic effects but over time the body needs more of the drug or greater potency to get the same desired effect
develops quickly
Name two classes of antagonists
beta blockers
narcan
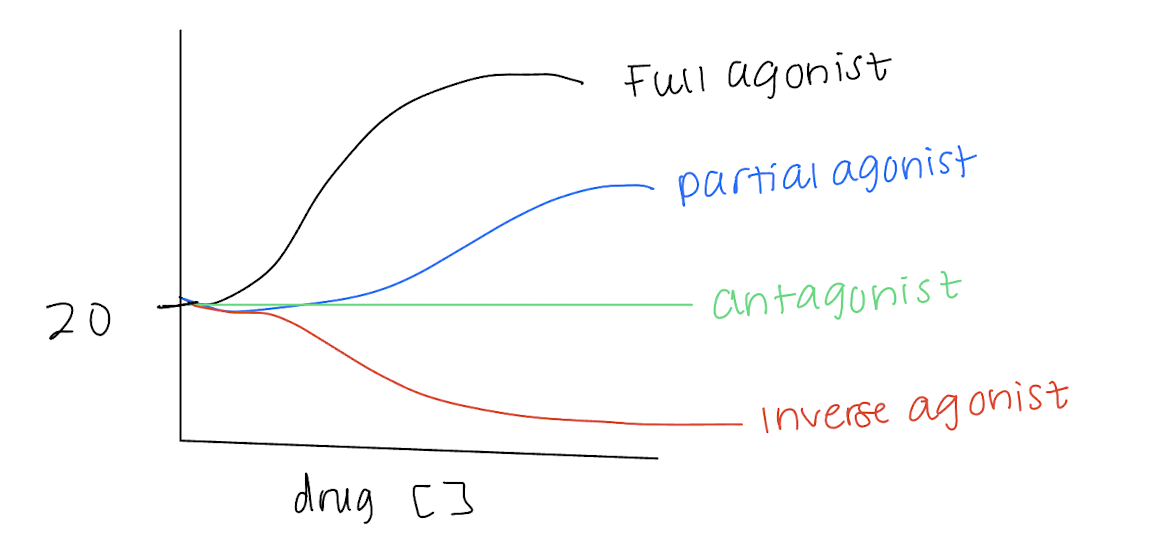
Apply each: full agonist, partial agonist, antagonist, and inverse agonist
Agonist - drug binds and causes the same action as the substance normally would
Partial agonist - agonist that cannot produce a maximal possible response as a full agonist
Antagonist - drug that binds and stops the action or effect of another substance
Inverse agonist - drug that causes an opposite effect of an agonist
Define passive diffusion vs facilitated diffusion
Passive diffusion - does not require energy and can’t become saturated. Molecules will move along a concentration gradient (electrochemical) from high to low.
Facilitated diffusion - requires no energy and can get saturated and limit the rate of absorption. They require a carrier molecule to transport the drug molecule
What are ionized versus non-ionized molecules and how do they cross the plasma membrane?
Ionized - hydrophillic and less able to move across the membranes
move across the membrane with carriers
Non-ionized - lipophillic and more able to cross the membrane
can move directly across the membrane
What is active transport?
Moving molecules AGAINST a gradient with energy. This can concentrate a molecule on one side of the membrane
It is carrier mediated and can get saturated
What is permeation?
Permeation is the process by which a substance passes through a barrier, such as a biological membrane. It encompasses various transport mechanisms including passive diffusion, facilitated diffusion, and active transport.
Drugs are ______ and plasma is the _______ (diluting and dissolving the drug)
a. solvent, solute
b. solute, solvent
b. solute, solvent
T/F: drugs move down the concentration gradient
true
______ is selectively permeable and considered a bilayer of amphiphathic lipids with hydrocarbon chains pointed inward
plasma membrane
Which proteins are embedded within the plasma membrane layer?
structural anchors
receptors
ion channels
transporters
How does pH effect passive transport?
Many drugs are weak acids or bases and at a steady state, an acidic drug will accumulate on the basic side of the membrane and vise versa for a basic drug.
Only the non-ionized (uncharged) equilibrates across the membrane
Which ionic molecule equilibrates across the membrane in terms of pH?
a. ionized
b. non-ionized
c. both
d. neither
b. non-ionized
In the case molecules are too large (for passive transport), a form of active transport, endocytosis occurs. Explain how.
Molecule attaches to the cell surface and it is engulfed (not broken down) and then released on the other side of the membrane
In the case molecules are too large (for passive transport), a form of active transport, exocytosis occurs. Explain how.
The process where substances are transported out of the cell when vesicles fuse with the plasma membrane, releasing their contents into the extracellular space. (neurotransmitters)
What is the new drug application vs the abbreviated new drug application?
NDA - FDA approval. to take a drug to market and sell (after phase 3)
ANDA - approval for a generic version of an already approved drug; core requirement is to show bioequivalence (show release mechanism)
medication(s) with the same active ingredient to a brand-name medication able to be broughto to market after ANDA approved BUT can’t start till the patent runs out on the brand is ______
generic
the generic drug must show similar PK and PD to the brand drug is _____
bioequivlence
biologic medications that show a high similarity to the original biologic drug
tend to have a biologic base
most injections
is _______
biosimilar
What is the black box warning?
Added to labeling by the FDA before a drug is approved and occurs IF:
drug has been associated with a serious side effect or death if not used properly
if patients and prescribers follow specific administration, monitoring, and/or dosing guidelines, injury risk can be avoided or reduced
extra, mandatory steps needed in prescribing
the strength of the action between two substances
a. tolerance
b. efficiacy
c. potency
d. affinity
d. affinity