Embryology of the Lungs
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
structures found in conduction portion
URT:
nasal cavities
nasopharynx
oropharynx
larynx
LRT:
trachea
bronchi
bronchioles
terminal bronchioles
structures found in respiratory portion
respiratory bronchioles
alveolar ducts
alveolar sacs
alveoli
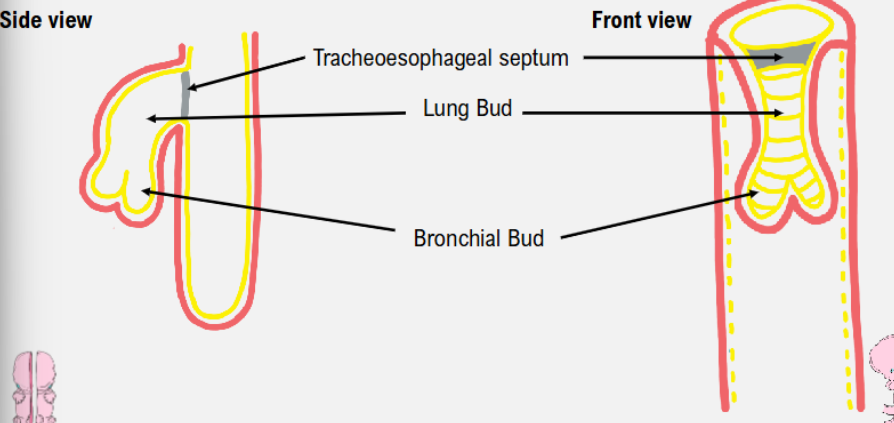
growth of lung bud
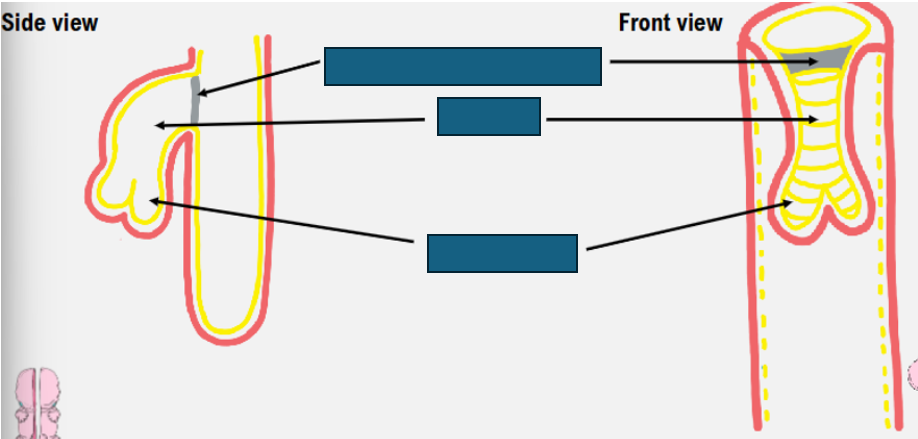
lung bud at week 4
foregut material is pulled anterioraly to form a lung bund
groove is formed→ tracheoesophageal groove
lung bud starts to pinch off, which pinches off to form tracheoesophageal septum
bifocation of primitive trachea into bronchial buds
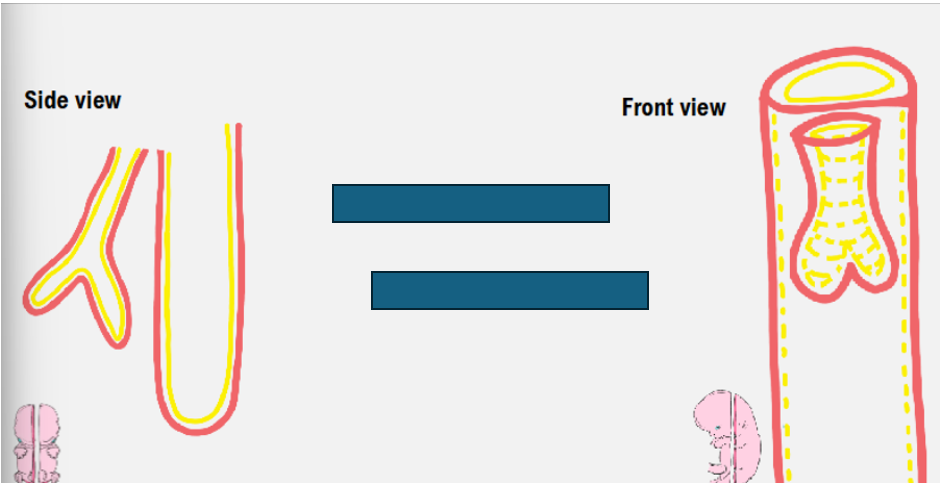
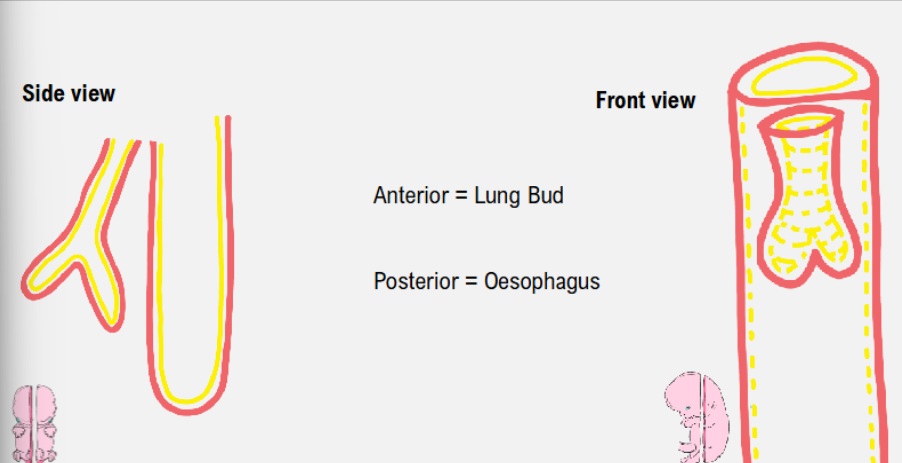
growth of lung bud- week 5
developing trachea has fully pinched off from foregut anterior to oesophagus
complete septation of the two structures→ trachea is separate to oesophagus
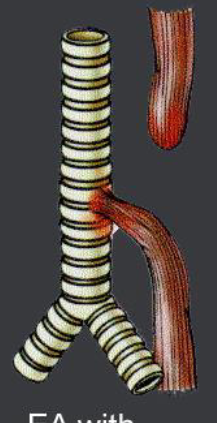
tracheoesophageal fistulas
occur when oesophagus and trachea are linked as opposed to completely separating
tracheoesophageal fistual with oesophageal atresia
difficult to detect prior to birth
stomach still able to fill with amniotic fluid via connection of oesophagus to trachea→ normal appearance on prenatal scan
upper portion of oesophagus becomes distended as also fills with amniotic fluid→ can give normal stomach appearance on scan
tracheoesophageal fistula repair
surgery required soon after birth
connection between trachea and oesophagus is closed
upper and lower parts of oesophagus are connected
if gap is large→ patient will need to wait few months for oesophagus to grow more:
until then, fed through tube directly to stomach
vacterl
describes group of anomalies- often occur together in newborn babies:
Vetebral (spinal) defects
Anorectal atresia (failure of anus and lower end of gut to form)
Cardiac (heart) defects
Tracheoesophagal fistula with or without Eoshageal atresia
Renal (kidney) anomalies
Limb defects
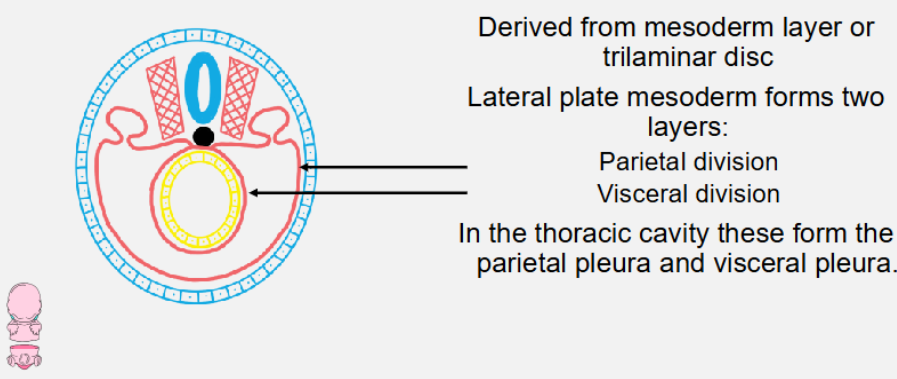
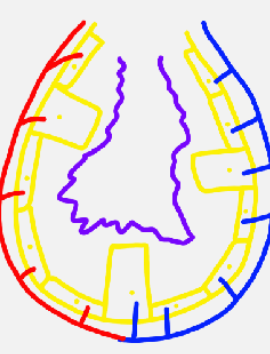
formation of the pleura
derived from mesoderm layer or trilaminar disc
lateral plate mesoderm forms two layers:
parietal division
visceral division
in thoracic cavity these form parietal and visceral pleura
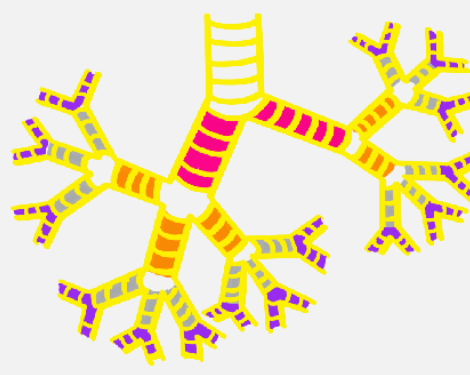
stages of lung development
pseudoglandular
canalicular
saccular
alveolar
pseudoglandular stage
week 5- week 16
right and left primary bronchi
secondary (lobar) bronchi:
3 on right
2 on left
tertiary bronchi
terminal bronchioles
canalicular stage
week 16- week 26
respiratory bronchioles
primitive alveoli→ cuboidal cells
pulmonary capillaries

saccular stage
week 26-birth
increase in number of primitive alveoli
primitive alveoli begin to mature
cuboidal cells become type I and type II pneumocytes:
type I→ flat cells (gaseous exchange)
type II→ cuboidal cells (surfactant)
alveolar stage
week 36- 8yrs
increased number of primitive alveoli become specialised
mature alveoli develop septa→ increases surface area
at birth→ 100mln primitive alveoli
8 years→ 300mln primitive alveoli
before birth breathing
before birth
breathing in amniotic fluid
during birth
air breathed in→ amniotic fluid ‘sucked up’ by pulmonary capillaries
all that should remain is surfactant
infant respiratory distress syndrome
child born during canalicular stage (~24 wk) have low chance of survival
alveoli not well developed
low levels of surfactant→ alveoli prone to collapse
baby unable to take in high volume of air, breathing rate increases
mechanical ventilation necessary:
causes damage to alveoli
leads to bronchopulmonary dysplasia
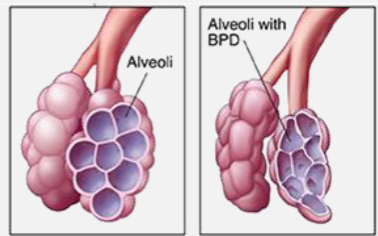
bronchopulmonary dysplasia
damaged lung tissue
slightly collapsed alveoli
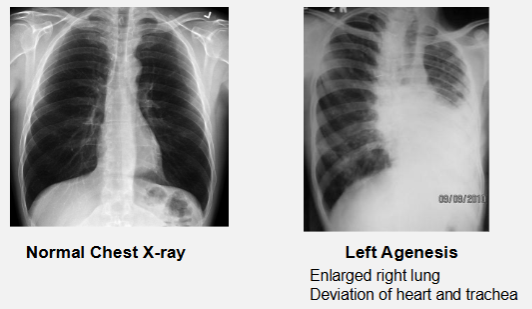
pulmonary agenesis
complete absence of one or both lungs:
can be just a lobe
disruption of lung bud during formation
pulmonary hypoplasia
either one or both lungs do not fully develop
level or respiratory distress results from degree of hypoplasia
can be found in association with congenital diaphragmatic hernia