SECONDARY LESIONS
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
secondary lesions
due to trauma or sequelae to a primary lesion (may evolve from primary lesions)
are those lesions that are characteristically brought about by modification of the primary lesion or through natural evolution of the lesion environment

erosion
only the epidermis is lost, leaving deeper layers intact
an ulceration or loss of substance that occurs on the skin or mucous membrane
clinical features of erosion
leaves no scar when healed
loss of outer layer of the mucosa
circumscribed, linear, irregular, punctuate
seen on moist surfaces which represents the necrosis & loss of the outer layer of the mucous membrane
common causes of erosion
after traumatic wounds
secondary to vesicles, blebs
external → intake of acids
internal cause → gastric content regurgitation
examples of erosion
lichen planus
desquamative gingivitis
lichen planus
autoimmune condition that causes erosions on mucosal surfaces, leading to ulceration

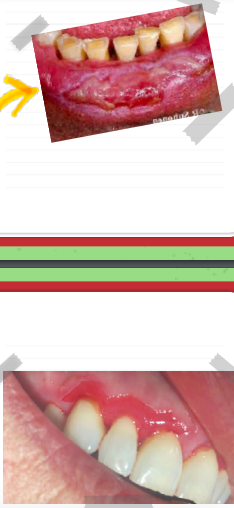
desquamative gingivitis
condition where the gingiva becomes eroded and sloughs off, often as a result of autoimmune diseases.

external causes of tooth erosions
intake of acids (e.g., citrus, soda, or acid reflux).
interrnal causes of tooth erosions
bulimia, chronic vomiting
gastric content / GERD
fissures
can be moist or dry
linear crack or break from the epidermis to the dermis
are cleft and grooves in the tissue that are pathologically present
nystatic
treatment of choice for angular cheilitis
[ why? commonly caused by candida (a fungal infection), and it kills candida, treating the underlying cause ]
clinical features of fissures
maybe inflamed
linear crack, radiating
superficial or deep (dermis)
longitudinal and transverse
occurs at the mucocutaneous junction of the mouth
examples of fissures
congenital cleft
syphilitic rhagades
athlete's foot (tinea pedis)
angular cheilitis (perleche)
scrotal tongue or fissured tongue
angular cheilitis (perleche)
cracks at the corners of the mouth
often due to decreased vertical dimension or fungal infection

scrotal tongue / fissured tongue
often linked to vitamin B deficiency or pernicious anemia
may not be inflamed unless deep grooves are present, creating a breeding ground for microorganisms

syphilitic rhagades
caused by treponema pallidum
treatment: metronidazole / penicilin
fissures that occur as a result of syphilis, typically at the mouth's corners

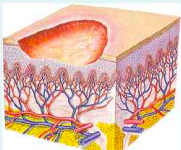
ulcers
patient feels pain, presence of lymphadenopathy due to trauma
a deeper crater that involves the full thickness of the epithelium and reaches the connective tissue
deeper defects of the skin or mucous membrane that extend beyond the epidermis into the underlying tissue
clinical features of ulcers
base is soft or indurated (hardened)
after effect resulting in vesicles / blebs
edges are rugged, punched out appearance
extends into the dermis and has a concave shape
floor is smooth, granular, glazed, pus covered or hemorrhagic
common cause of ulcer
ill fitting dentures
trauma due to accidental toothbrushing
mouth burned by hot liquids or toothache drops
common sites of ulcers
tongue, lips
gingiva & palate
mucobuccal fold
examples of conditions that manifest oral ulcerations:
ANUG
sickle cell anemia
herpetic gingivostomatitis
recurrent apthous ulcers (RAU)
orogenital sex → lingual frenum affected
sickle cell anemia
a blood dyscrasia that shows manifestation of the oral mucosa as ulceration.
herpetic gingivostomatitis
viral infection (HSV-1) leading to painful vesicles that rupture into ulcers.

ANUG
bacterial infection causing painful, necrotic ulcers with a punched-out appearance.

recurrent apthous ulcers (RAU)
non- infectious, recurring ulcers of the oral mucosa, often associated with stress or immune response.

treatment for ulcers
heals within 10 days
remove the cause
application of kenalog in orabase (hydrocortisone)
pseudomembranous
results from the response of mucous surfaces to a necrotizing agent
cause of pseudomembranous
loss of surface epithelium
plasma exudates from the vessels & spreads to the eroded surface it coagulates & encloses a necrotic epithelium
clinical feature of pseudomembranous
a white membrane is formed
examples of pseudomembranous
ANUG
diphtheria
diphtheria
affecting the nose, skin, and throat
acute infectious disease caused by corynebacterium diphtheriae
white pseudomembrane formation, which can obstruct breathing (can extend into the trachea)

eschars
masses of dead tissue caused by burns or exposure to corrosive agents
tissue necrosis leads to dry, leathery scabs (eschars), which may later slough off, leaving an ulcer.

examples of eschars
aspirin burns
phenol burns
formocresol burns
phenol & cresol burns
dull gray to brown eschar
aspirin burn
primary lesion → erythematous macule (red, flat lesion)
progression → tissue necrosis leads to ulcer formation
differential diagnosis for eschars
Erythematous macule - flat circumscribed o Eschars-ulcer (loss of necrotic tissue)
o Eschars- pseudomembrane
desquamation
color: grayish white
shedding of epithelial elements in scales or sheets

scales
results of inflammation (dry)
a clinical feature of desquamation
it is lost due to continuous wetting by saliva in the oral cavity
examples of desquamation
leukoplakia
focal hyperkeratosis
leukoplakia
white, keratotic lesion due to chronic irritation

focal hyperkeratosis
localized thickening of the epithelium due to friction or irritation
crusts
not common in oral cavity due to the moist environment from saliva
if it is removed, it leaves a bleeding surface and may form a pseudomembrane
dried pus, blood, dried serum, epithelial debris, and external matter on skin or lips

formation process
crusts (pseudomembrane) → cracks → fissures → may bleed due to trauma, speaking, or mastication
clinical features of crusts
maybe deep seated or superficial
yellowish to brown, depending on the amount of pus or blood
constant drying of coagulated blood, tissue, fluids & debris
common sites of crusts
mucocutaneous junction of the lips (ex: angular cheilitis)
associated conditions of crusts
carcinomas
vesicular lesions
traumatic ulcers
bullous disorders